
Abstract
Study Design
Narrative review.
Objective
The spine is the most common site of metastases, associated with decreased quality of life. Increase in metastatic spine tumour surgery (MSTS) has caused us to focus on the management of blood, as blood loss is a significant morbidity in these patients. However, blood transfusion is also not without its own risks, and hence this led to blood conservation strategies and implementation of a concept of patient blood management (PBM) in clinical practise focusing on these patients.
Methods
A narrative review was conducted and all studies that were related to blood management in metastatic spine disease as well as PBM surrounding this condition were included.
Results
A total of 64 studies were included in this review. We discussed a new concept of patient blood management in patients undergoing MSTS, with stratification to pre-operative and intra-operative factors, as well as anaesthesia and surgical considerations. The studies show that PBM and reduction in blood transfusion allows for reduced readmission rates, lower risks associated with blood transfusion, and lower morbidity for patients undergoing MSTS.
Conclusion
Through this review, we highlight various pre-operative and intra-operative methods in the surgical and anaesthesia domains that can help with PBM. It is an important concept with the significant amount of blood loss expected from MSTS.
Level of Evidence
Not applicable.
Keywords
Introduction
The spine is the most common site of metastases and spinal metastases are associated with a decreased quality of life. The incidence of metastatic spinal tumours has been increasing with a growing aging population and improvements in survival rates of cancer patients. This also comes with increased patient mortality secondary to complications such as cord compression, spinal instability, pathological fractures and pain.1,2 The management of spinal metastasis continues to involve, with Patchell et al 3 demonstrating the superiority of decompressive surgery and radiotherapy compared to radiotherapy alone and henceforth leading to an increase in surgical treatment of spinal metastases. 4
The increase in metastatic spine tumour surgery (MSTS) resulted in our focus to be shifted towards the management of blood during the peri-operative period. Blood loss remains a significant concern, as it has been established that perioperative anaemia is associated with increased postoperative complications, morbidity, hospital length of stay and mortality. 1 However, with the realisation that blood transfusion is not without significant risks, the drive to adopt blood conservation strategies has led to the implementation of the concept of patient blood management (PBM) in surgical practice. In MSTS where substantial intraoperative blood loss is commonly anticipated, 2 the application of PBM will be paramount in improving postoperative outcomes.
In this review, we discuss the various advancements made in patient’s blood management from the anaesthesia and surgical perspective, as well as its effect on intraoperative surgical outcomes.
Method
This narrative review was conducted using PubMed, Medical Literature Analysis and Retrieval System Online (MEDLINE), The Cochrane Library and Scopus databases through 10 October 2022. The keywords used were “spine” and “metastasis” and “blood”.
Inclusion and exclusion criteria of the studies were decided by the senior authors of the paper. The articles were selected in two stages (Figure 1). Firstly, the abstracts identified by the above searches were downloaded and the list was screened using the inclusion and exclusion criteria. Secondly, the full texts of this shortlisted list were downloaded and assessed for eligibility. The reference lists of the publications were then hand-searched for additional relevant studies. This process was repeated twice by our senior authors independently. Flow diagram of the review and selection of cases.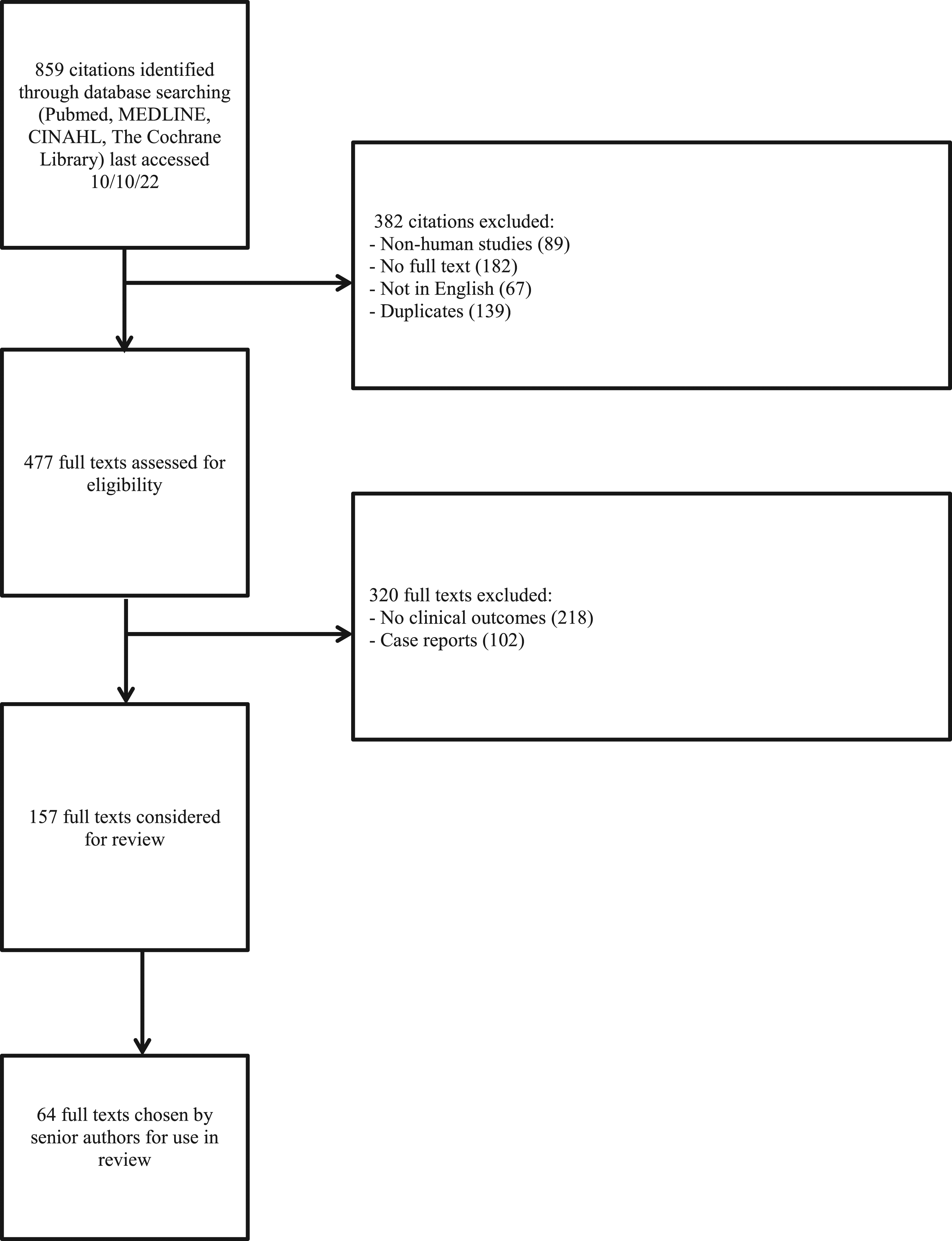
Discussion
MSTS patients can present with multiple symptomatic vertebrae requiring different types of surgery with different magnitude of invasiveness. The need for decompression, corpectomy and or fusion can lead to increased blood loss and need for blood transfusion. Kumar et al 5 described the spinal metastasis invasiveness index (SMII), comprised of surgical factors, tumour vascularity, and embolization status, which strongly predicted increased operative time (R2 = .28,P < .001) and intraoperative blood loss (R2 = .18,P < .001). For every unit increase in score, there was a 42 mL increase in mean blood loss (P < .001) and 5-minute increase in mean operative time (P < .001). This predictive system is of use to both the surgeon and anaesthetist to predict expected blood loss and the need for PBM measures to mitigate this and reduce the need for transfusion.
The Effect of Blood Transfusion
Blood loss is a significant concern in MSTS. In a meta-analysis of MSTS, the pooled mean blood loss in MSTS patients was found to be 2180 mL 6 while in a review of cases done in our institution, mean blood loss was 911 mLs. 7 While allogenic blood transfusion remains the mainstay of treatment, the demand for allogenic blood often exceeds its supply and allogenic blood transfusion is not without its complications.8–10 The role of allogenic blood transfusion in patient morbidity and mortality has been extensively investigated.
In a multicentre prospective review of 1601 patients in the American College of Surgeons National Quality Improvement Program database, 623 patients (38.9%) received a RBC transfusion, patients who received a transfusion had a significantly higher complication rate when compared to non-transfused patients, (22.3% vs 15.0%, P < .001). These complications included sepsis (3.5% vs 1.9%, P = .050), deep vein thrombosis (6.1% vs 3.3%, P = .007), and prolonged ventilation (3.9% vs 1.3%, P = .001). 11 Vinas-Rios et al 12 also found blood transfusions to be an independent risk factor for higher risk of complications while Purvis et al 13 also found that a liberal transfusion policy, transfusion of patients with Hb of 8-10 g/dL, was associated with an independently higher risk of perioperative morbidity and increased perioperative costs.
In our centre, Zaw et al 14 found that in patients receiving blood transfusions after spinal metastases surgery, the adjusted odds of developing any postoperative complication blood transfusion was 2.27 times higher in patients with transfusion (95% confidence interval [CI], 1.17-4.38; P = .01) and 1.24 times higher odds per every unit increase in blood transfusion (95% CI, 1.05-1.46; P < .01). Exposure to blood transfusion also increased the odds of having overall postoperative infections (odds ratio, 3.58; 95% CI, 1.15-11.11; P = .02) and there were 1.24 times higher odds per every unit increase in transfusion (95% CI, 1.01-1.54; P = .04).
The effect of allogenic blood transfusion on patient survival and progression free survival is controversial. Zaw et al 15 found that neither blood transfusion exposure nor quantities of transfusion were associated with overall survival or progression-free survival, only the primary tumor type consistently affected patient survival and progression free survival. Other authors have also not found blood transfusion or quantity of blood transfusion to have a significant effect on patient survival.
Although perioperative blood transfusion does not significantly decrease patient survival in patients undergoing MSTS, it does lead to an increase in complication rates and perioperative costs.16,17 For this reason, PBM is crucial in improving overall outcomes and reducing the overall need for blood transfusion.
3 Pillars of Patient Blood Management
Musallam et al previously established that perioperative anaemia is associated with increased postoperative complications, morbidity, hospital length of stay and mortality. 18 However, with the realisation that blood transfusion is not without significant risks, the drive to adopt blood conservation strategies has led to the implementation of the concept of PBM in surgical practice. In MSTS where substantial intraoperative blood loss is commonly anticipated, 6 the application of PBM will be paramount in improving postoperative outcomes.
The 3 pillars of PBM in MSTS.
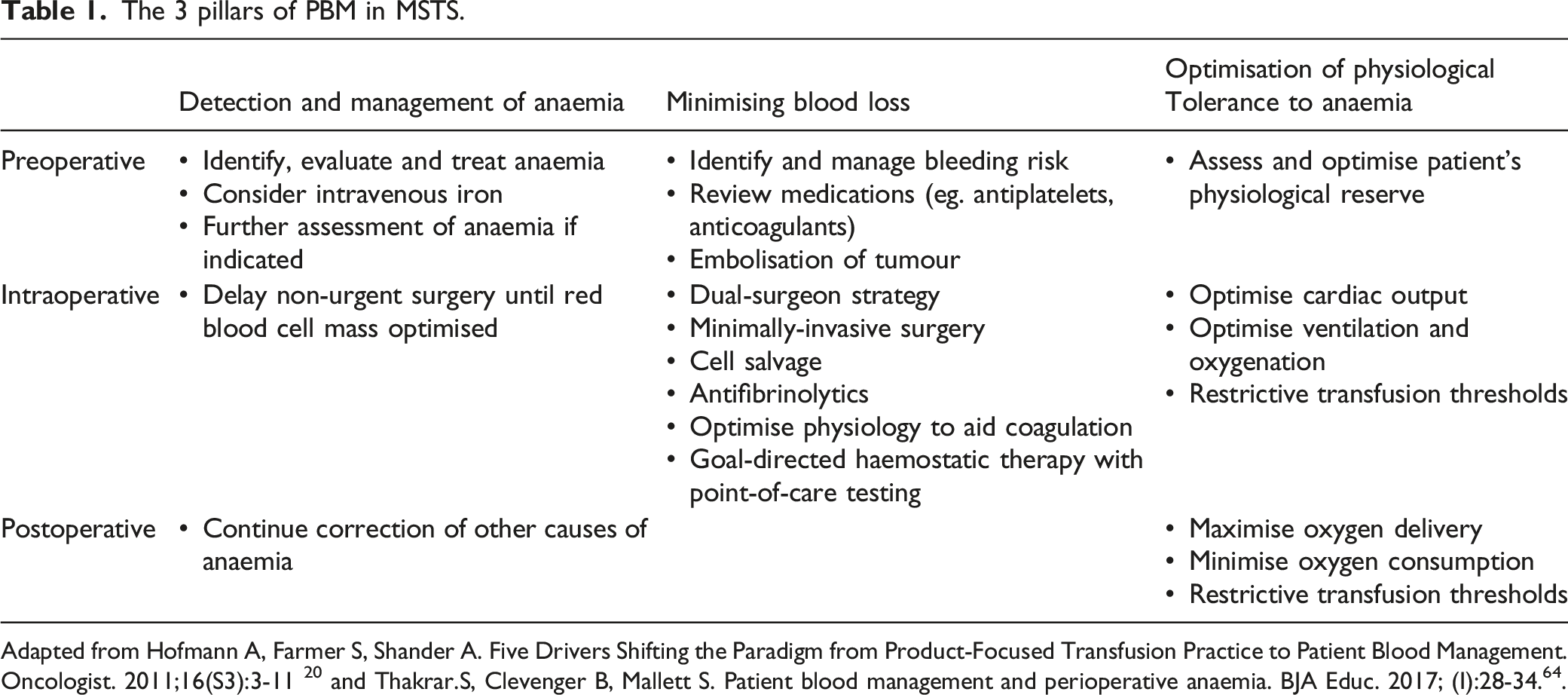
Adapted from Hofmann A, Farmer S, Shander A. Five Drivers Shifting the Paradigm from Product-Focused Transfusion Practice to Patient Blood Management. Oncologist. 2011;16(S3):3-11 20 and Thakrar.S, Clevenger B, Mallett S. Patient blood management and perioperative anaemia. BJA Educ. 2017; (I):28-34. 64 .
Pre-Operative Management of Blood Loss
Preoperative Management of Anaemia
The Association of Anaesthetists of Great Britain and Ireland has developed a consensus statement which recommends that all patients presenting with anaemia and undergoing surgical procedures with expected blood loss of more than 500 mL should be investigated with a diagnostic and treatment algorithm. 21
Iron deficiency is the commonest cause of anaemia globally 22 and is prevalent amongst 39-60% of oncological patients.23,24 It can be readily diagnosed in the outpatient setting and ideally as soon as the patient is considered for surgical intervention to allow implementation of therapy. First-line recommendation by the British Society for Haematology for iron deficiency anaemia (IDA) is oral iron supplementation. 25 However, absorption of oral iron is variable and correction of haemoglobin typically requires 2 to 3 months, 26 making this route of administration unsuitable for urgent surgeries. Intravenous iron is a safe and efficacious alternative with desired effects usually achieved within 1 to 2 weeks. 27
In Europe, the multicentre PREPARE study on patients undergoing elective orthopaedic (hip, knee or spine) surgery demonstrated preoperative anaemia was less frequent (8.0% vs 18.5%; P < .001) and iron status assessed more frequently (11% vs 2.6%; P < .001) in institutions with PBM vs non-PBM centres. 28 A recent systematic review of patients undergoing major orthopaedic, cardiac, gynaecological, colorectal and abdominal surgery showed the use of preoperative parenteral iron was associated with a 16% decrease in allogeneic blood transfusion (ABT) (RR: .84, CI: .71 to .99). 29
Preoperative Angioembolization
Pre-operative angioembolization is increasingly applied to decreases the risk of haemorrhage in highly vascularized metastases such as renal cell carcinoma. 30 There is clear evidence of the utility of preoperative embolization in decreasing blood loss and transfusions. In a recent meta-analysis of 12 studies with 744 patients by Gao et al, 31 angioembolisation in angiographically demonstrated hypervascular tumours was associated with significantly less intraoperative blood loss, fewer blood transfusions and shorter operative times. A metanalysis of 839 patients in 11 studies (one RCT and 10 retrospective studies) by Gong et al 32 published in the same year also demonstrated decreased intraoperative blood loss in patients with hypervascular tumours undergoing spinal surgery. The role of perioperative angioembolisation in patients with non-hypervascular tumours is unclear. In a retrospective propensity-score matched, case-control study of patients with non-hypervascular spinal metastases undergoing surgery by Groot et al, 33 pre-operative embolisation did not lead to a significant decrease in intraoperative blood loss. Clausen et al 34 demonstrated decreased operating time in all patients both hypervascular and non-hypervascular undergoing angioembolisation but did not show any significant decreased blood loss in the non-hypervascular group. Yoo et al 35 demonstrated that in patients with non-hypervascular tumours undergoing corpectomy, pre-operative embolization significantly reduced intraoperative bleeding and total transfusion. Zhang et al 36 showed that hypervascularity on MRI and routine angiographic interrogation and embolization of additional levels above and below the involved segment was associated with significant decrease in perioperative blood loss. Thus while preoperative angioembolisation is indicated in potentially hypervascular tumours, there is no clear indication for its use in non-hypervascular tumour types. However, in non-hypervascular tumour types which show signs of hypervascularity on MRI or for which corpectomy is indicated, preoperative angioembolisation may be indicated to reduce blood loss and operative time.
Intraoperative Management of Blood Loss
Use of Tranexamic Acid
Antifibrinolytic drugs such as tranexamic acid (TXA) inhibit fibrinolysis by binding to active sites on plasminogen thus preventing formation of plasmin and subsequent degradation of fibrin. It has become a mainstay of perioperative clinical management in reducing blood loss and transfusion requirements since the introduction of TXA to clinical practice in the 1960s. 37
The benefits of TXA have led to its popularity in spine surgery with multiple studies demonstrating its efficacy and safety profile in patients with metastatic spinal disease. It is typically administered as a bolus dose of 10 to 20 mg/kg followed by an infusion of 1 to 2 mg/kg/h intraoperatively.38,39 A prospective comparative study by Damade et al 40 showed that intraoperative TXA was associated with reduced blood transfusion requirements post-operatively and Zhang et al 40 showed that TXA helped with reducing intra-operative blood loss with no significant change in coagulation markers.
The use of TXA has been measured due to potential risks of thromboembolism but various reviews40–42 have found that TXA was not associated with increased VTE risk, although high-dose TXA 42 (≥ 20 mg/kg) was associated with increased odds of DVT or PE. The role of Topical TXA is unclear, and in randomised control trial by Maethungkul et al 43 there was no difference in postoperative blood loss or transfusion requirements in patients receiving topical TXA or placebo.
As established through literature, IV TXA appears to be effective and safe and should be routinely applied in patients undergoing surgery for spinal metastases.
Point-of-Care Testing
Perioperative management of coagulopathy guided by point-of-care (POC) testing has been shown to reduce allogeneic blood transfusion requirements. 44 Traditional tests of coagulopathy require long processing times with an incomplete representation of the haemostatic deficiency. Comparatively, viscoelastic tests of haemostasis such as thromboelastography (TEG) and rotational thromboelastometry (ROTEM) provide measurement of global clot formation and dissolution in real time. 45 Furthermore, the development of this technology has enabled meaningful results to be produced in as quickly as 5 minutes, whilst promoting goal-directed haemostatic therapy thus facilitating rapid response with blood component-specific transfusion. Point-of-care testing helps to identify the need for supplementation of clotting factors, platelets and institution of pharmacotherapy to enhance haemostasis and clot formation. Use of fibrinogen and prothrombin complex concentrate guided by point of care testing has revolutionised perioperative blood management strategies. In a case-control study of patients undergoing posterior thoracolumbar fusion surgery, Guan et al showed that the use of ROTEM perioperatively was associated with a lower total amount of blood product transfusion. 46 Hence, we feel that POC testing can be extrapolated to MSTS, to allow for better PBM.
Improving Tolerance to Anaemia
The third pillar of PBM involves optimisation of a patient’s physiological tolerance to anaemia to achieve adequate tissue oxygen delivery. 47 In essence, the underlying principles involve maximising oxygen delivery and minimising oxygen consumption. Delivery of oxygen can be enhanced via increasing fractional inspired oxygen, while improving cardiac output aids organ perfusion. Ensuring sufficient analgesia and prompt treatment of infections help to prevent increase in oxygen consumption. 48
With the landmark Transfusion Requirements in Critical Care (TRICC) trial demonstrating that a restrictive transfusion strategy (haemoglobin target of 7 to 9 g/dL) was as effective as a liberal strategy (haemoglobin target 10-12 g/dL), 49 this has been supported by NICE advocating a similar transfusion threshold in patients without underlying cardiovascular disease. 50 Overall, the decision for transfusion should consider physiological and laboratory parameters and further transfusion guided by regular clinical reassessment.
Minimally Invasive Spinal Surgery
Open spinal surgery (OSS) with stabilisation and decompression is the current gold standard of surgical treatment in MSD. However, OSS is associated with extensive soft tissue dissection leading to excessive blood loss and increased hospital stay and complication rates. In recent years, advancements in surgical techniques and technology have led to the advent of minimally invasive spinal surgery (MISS). The aim of MISS is to achieve the same surgical goal with the minimisation of surgical approach related morbidity, leading to less blood loss, operative time and post-operative morbidity. MISS includes the use of percutaneous pedicle screw fixation as well as mini-open techniques to perform tumour decompression and corpectomy. Kumar et al 7 demonstrated the utility of MISS techniques in treating patients with spinal instability secondary to spinal metastases and MSCC, with significantly decreased blood loss and length of stay. In a meta-analysis by Pranata et al, 51 comparing minimally invasive surgery with instrumented fusion vs conventional open surgical Instrumented Fusion for the Treatment of Spinal Metastases, MISS was associated with decreased blood loss and lower blood transfusion rates as well as lower rate of complications and duration of stay. There was also comparable rates of neurological improvement and duration of surgery. Similar findings of decreased blood loss, transfusion rates, complication rates and duration of hospital stay have been found in meta-analysis by Lu et al, 52 Perna et al 53 and Pennington et al. 54 MISS techniques in well selected patients are likely to have a significant role in reducing blood loss and transfusion.
Two Surgeon Operation
Dual surgeon strategies to decrease operative time and blood loss are increasing applied in scoliosis and adult deformity surgery. Lubelski et al 55 showed that a dual surgeon strategy in treating patients with spinal metastases is associated with a significantly lower total operative time (601 vs 683 minutes), estimated blood loss (956 vs 1780 mL), and decreased intraoperative blood transfusion rates (41.7% vs 75.0%). A dual surgeon strategy may be employed in patient whom a high estimated blood loss and long surgical time is expected.
Intraoperative Cell Salvage
The role of intraoperative cell salvage and autogenic blood transfusion is controversial due to the theoretical risk of tumour seeding and systemic spread of disease. 56 Its use in non-spinal metastases oncological surgery is widely established and there does not appear to be evidence to suggest that its use affects survival or subsequent spread of disease. 56
Kumar et al57,58 has previously shown that after passage through an intraoperative cell salvage machine and leukocyte depletion filter, there are minimal to no tumour cells present in the salvaged blood, and these cells are no longer viable. These studies provide the biological basis for autogenic salvaged blood transfusion in patients undergoing surgery for spinal metastases.
In the largest case series published to date, Elmalky et al 59 showed that salvaged blood transfusion in MSTS was significantly associated with a lower likelihood of allogenic blood transfusion (OR = .407, P = .03) and not associated with increased costs (P = .88). A smaller case series by Gakhar et al 60 also showed that salvaged blood transfusion did not result in dissemination of metastatic disease.
Outcomes
As discussed above, MSTS does indeed come with risks of increased blood loss intra-operatively. This makes PBM ever so important, in order to reduce the amount of allogenic blood transfusions, in turn reducing the risks of transfusion related complications. 14 As shown by Clausen 16 and Paulino et al, 17 reduction in blood transfusions do not affect survival, and hence the reduction in transfusion rates in patients is important to reduce the risks as mentioned previously.12,13,16,17 Important factors that affect patients blood management and hence outcomes can be split to anaesthetic and surgical considerations, which can be tackled pre-operatively and intra-operatively.
It is also previously established that unplanned hospital readmissions in patients undergoing MSTS is common, with reported rates of 30 day readmission of 16-18%.61,62 Madhu et al 63 reported the significant association of haemoglobin ≥12 g/dL and decreased readmission rates. PBM and reducing excess blood loss may play a role in reducing unplanned readmissions.
Conclusion
PBM is important in patients undergoing MSTS. Proper pre and intra-operative management can help to reduce blood loss and the requirement for blood transfusions, in turn reducing risks of transfusion related complications. PBM can be split into anaesthesia and surgical considerations, and it is hence important for both anaesthetists and surgeons to work in tandem in managing blood loss in patients undergoing MSTS.
Footnotes
Acknowledgements
Mr Karthigesh Palanichami and Ms Pradnya Nishant Mohite for both assisting in manuscript editing and other secretarial work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.