
Abstract
Study Design
Prospective cohort study.
Objectives
Diabetes mellitus (DM) is associated with unfavourable patient-reported outcomes after spine surgery. Chronic low back pain (CLBP) with Modic Changes (MCs) in the lumbar vertebrae, as observed on MRI, forms a specific subgroup. This study aims to investigate the potential influence of DM on CLBP with MCs.
Methods
This study involved 259 patients with CLBP accompanied MCs. We recorded the patient-reported outcomes (visual analogue scale (VAS), Oswestry Disability Index (ODI), and Roland-Morris Disability Questionnaire (RMDQ)) at baseline, 3, 6, and 12 months. Multivariable linear regression analyses were performed to determine predictors of patient-reported outcomes.
Results
103 patients had DM. Patients with DM exhibited higher VAS (P < .05), ODI (P < .001), and RMDQ (P < .001) scores at 3, 6, and 12 months, while patients without DM experienced more significant improvements in the scores over time (P < .001). Patients with DM reported longer durations of physical exercise (P = .007). Additionally, patients without DM had a significantly higher patient satisfaction index (P < .001) and a lower prevalence of hypertension (P < .001). Notably, significant differences were observed in the distribution of MCs of lumbar vertebrae (P = .034) and Pfirrmann grades of intervertebral disc degeneration between two groups (P < .001).
Conclusion
Patients with DM demonstrated poorer patient-reported outcomes compared to those without DM in 1-year. DM emerged as an independent predictor of adverse patient-reported outcomes. It can be utilized to enhance the management and treatment of CLBP in patients with MCs.
Introduction
Chronic low back pain (CLBP) is defined as pain lasting for more than three months in the lower region of the back. As a prominent contributor to disability, CLBP poses a significant social and economic burden in contemporary society. 1 Numerous risk factors have been linked to CLBP, age, genetic predisposition, psychosocial factors, excessive lifting, obesity, decreased trunk strength, sleep disorders, intravenous drug abuse, smoking, and spinal pathologies. 2
Modic et al categorized Modic changes (MCs) into three types based on the signal intensity alterations observed in the vertebrae through magnetic resonance imaging (MRI) in 1988. 3 In their study, MCs type 1 indicated an inflammatory reaction in the subchondral bone marrow of the vertebrae, MCs type 2 represented steatosis in the subchondral bone, and MCs type 3 was characterized by sclerosis in the subchondral bone.3,4 The presence of MCs in the lumbar vertebrae, as revealed in MRI findings, serves as a warning sign for low back pain. 5 Several studies have identified lumbar vertebral MCs as a significant pathological feature of CLBP.6,7 The mechanism behind chronic low back pain with MCs may involve the chemical and mechanical stimulation of nociceptors near injured end-plates. It should be noted that CLBP with MCs is a subgroup of patients exhibiting signal changes in the vertebral bone marrow that extend from the end-plate on MRI. 8
Diabetes mellitus (DM) is one of the most serious and prevalent chronic diseases, causing disabling and costly complications, as well as posing life-threatening risks and reducing life expectancy. It is projected that by 2045, the global population will reach 783.2 million individuals with DM, representing 12.5% of the total population. 9 Additionally, it is noteworthy that approximately 34.8% of 2095 individuals with DM are known to experience low back pain. 10 Furthermore, DM serves as a critical risk factor for MCs. 11 However, the relationship and underlying mechanism between DM and CLBP with MCs remain poorly understood. Therefore, the objective of this study is to investigate whether DM influences the development of CLBP with MCs.
Methods
In this study, we gathered data from patients who were treated at the General Hospital of Central Theater Command of the People's Liberation Army of China (PLA). This data was collected from an electronic inpatient database, and a 1-year follow-up was conducted. At 3, 6, and 12 months after the surgery, patient-reported outcome measures questionnaires were distributed to the patients. The research was carried out in compliance with the principles outlined in the Declaration of Helsinki. The Ethics Committee of the General Hospital of Central Theater Command of PLA approved all study protocols (number: [2014]003-02).
Patients
We recruited patients from the orthopedics department of our hospital between January 2014 and December 2020. The inclusion criteria for patient selection were as follows: i) Age greater than 20 years, ii) Experiencing low back pain for more than three months after conservative treatments, iii) Diagnosis of type 2 diabetes, iv) Presence of all types of MCs on imaging, v) Blood test results for fasting blood glucose [FBG], glycated hemoglobin [HbA1c], total cholesterol [TC], triglycerides [TG], low-density lipoprotein [LDL], and high-density lipoprotein [HDL]. On the other hand, the patients who met any of the following exclusion criteria were not included in the study: i) History of vertebral fracture or spinal surgery, ii) Lumbar vertebra infective lesions, iii) Lumbar spine tumor, iv) Diagnosis of type 1 diabetes or gestational diabetes mellitus.
Patient-Reported Outcomes Measures
The primary outcome in this study was assessed using the Roland-Morris Disability Questionnaire (RMDQ). The RMDQ measures the level of dysfunction caused by back pain and assigns scores ranging from zero to 24. Higher scores on the RMDQ indicate greater pain and disability. 12 The secondary outcomes included the visual analogue scale (VAS) and the Oswestry Disability Index (ODI). Pain intensity was evaluated using the VAS, which involves asking patients to rate their pain on a scale of zero to 10. A score of zero indicates no pain, while a score of 10 indicates the most severe pain. 13 The ODI is a back-specific questionnaire used to assess the level of disability associated with low back pain. Scores on the ODI range from zero to 100, with scores higher than 40 indicating severe disability. 14
Additional Covariates
All patient demographic characteristics, examination results, and treatments were retrieved from the electronic medical record system. This included data such as age, gender, presence of hypertension, physical exercise habits, tobacco use, body mass index (BMI), duration from symptom onset to hospital admission, laboratory test results (HbA1c, FBG, TC, TG, LDL, and HDL), as well as the type and level of MCs. Regarding the classification of intervertebral disc degeneration (IVDD), we categorized it into mild and moderate degeneration (Pfirrmann grades I, II, III), as well as severe degeneration (Pfirrmann grades IV, V). 15 Patient satisfaction index (PSI) was identified with ratings of 1 and 2 considered as satisfactory, while ratings of 3 and 4 were considered as unsatisfactory. 16 The surgical procedures were divided into four categories: microdiscectomy, lumbar laminectomy, lumbar fusion of a single level, and others (deformity or combined anterior and posterior lumbar procedures).
Statistical Analyses
Descriptive data were presented using mean and standard deviation (SD), as well as 95% confidence intervals (CI). Numbers and percentages were also utilized. Parametric analysis was employed to test patient-reported continuous outcome variables. For normally distributed continuous variables, the t-test was used, while the Mann-Whitney U-test was utilized for non-normally distributed continuous variables. Categorical variables were tested using Pearson's chi-squared test. To determine the significance of differences in VAS, ODI, and RMDQ scores over time for the entire group, as well as preoperative and postoperative outcome scores between groups, the student t-tests were employed. Univariate linear regression analyses were conducted to assess the association between patient characteristics at baseline and self-reported outcome scores at 3, 6, and 12 months. Initially, univariate linear regression analysis was performed, and factors with a P-value of less than .10 were included. These variables were then subjected to multiple linear regression. Multivariable analyses were adjusted for hypertension, history of diabetes, PSI, duration of MCs, type of MCs, level of MCs, and Pfirrmann grades of IVDD. Post-regression assessment for multicollinearity was conducted using the variance inflation factor. Statistical significance was determined using a two-tailed P-value of less than .05. All statistical analyses were performed using the Statistical Package for Social Sciences version 23.0 (SPSS Inc.).
Results
Cohort Characteristics
Two hundred and fifty-nine patients undergoing spine surgery met inclusion criteria and were included in this prospective cohort study. Complete follow-up data were available for 237 patients (91.5%) at three months, 227 patients (87.6%) at six months, and 215 patients (83.0%) at twelve months (Figure 1). The baseline characteristics are shown in Table 1. There were no significant differences (P > .05) in the patient characteristics of age, gender, BMI, smoking status, duration of symptom onset to hospital admission, surgery category, and type of MCs between patients with DM and those without DM. The patients with DM reported a significantly longer (P = .007) duration of physical exercise (6.7 ± 3.3 hours/week) compared to patients without DM (5.6 ± 2.3 hours/week). Additionally, patients without DM (92.5%, 123/133) had a significantly higher (P < .001) PSI than those with DM (81.7%, 103/126). The prevalence of hypertension in patients with DM (64.3%, 81/126) was significantly higher (P < .001) than those without DM (22.6%, 30/133). All laboratory blood test results showed significant differences between the two groups. Caption: Flow diagram of included patients. Characteristics of the Patients at Baseline. Abbrevation: BMI, body mass index; MCs, Modic changes; IVDD, intervertebral disc degeneration; PSI, patient satisfaction index; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; TC, total cholesterol; TG, triglycerides; LDL, low-density lipoprotein; HDL, high-density lipoprotein; SD, standard deviation.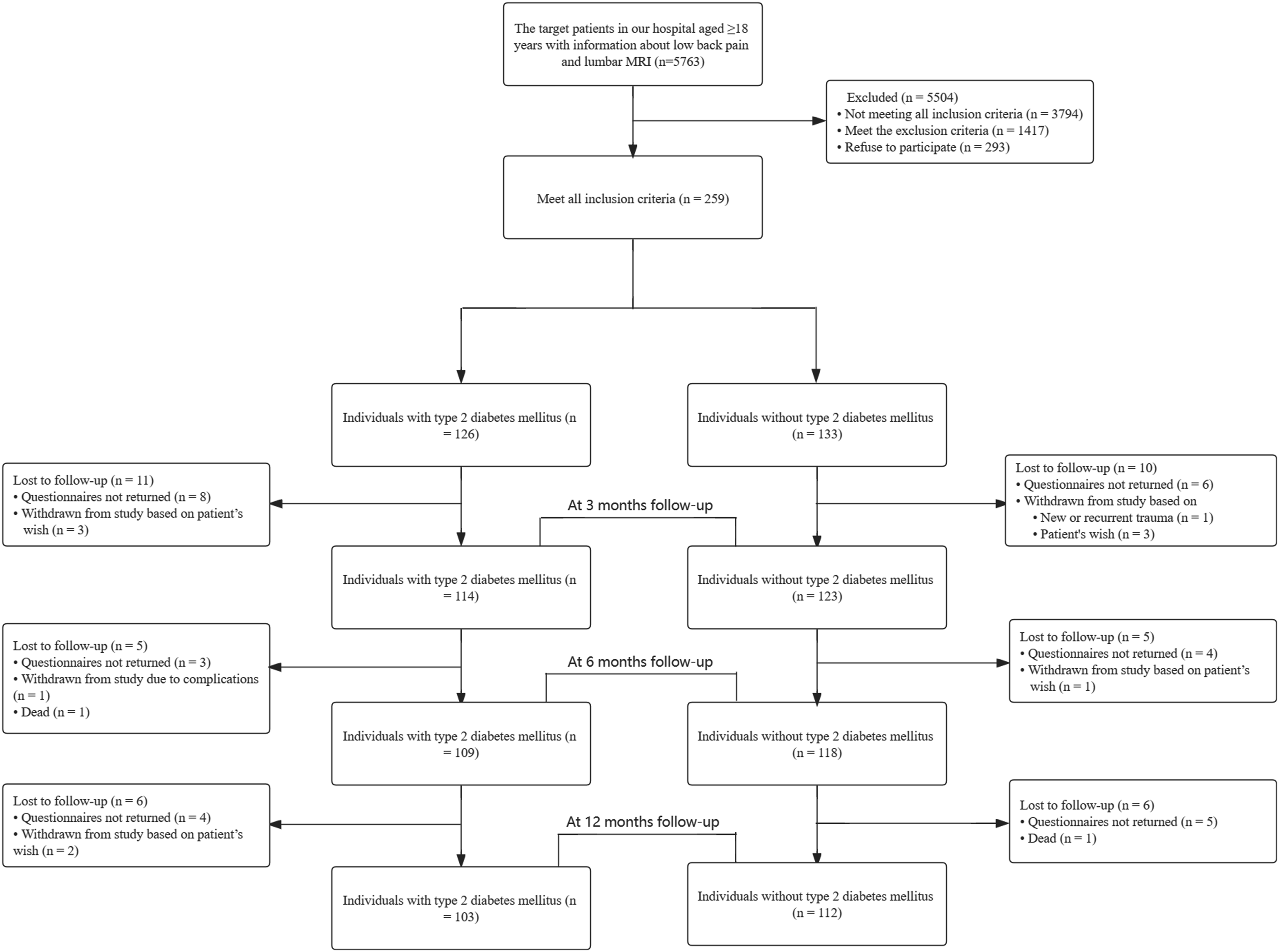
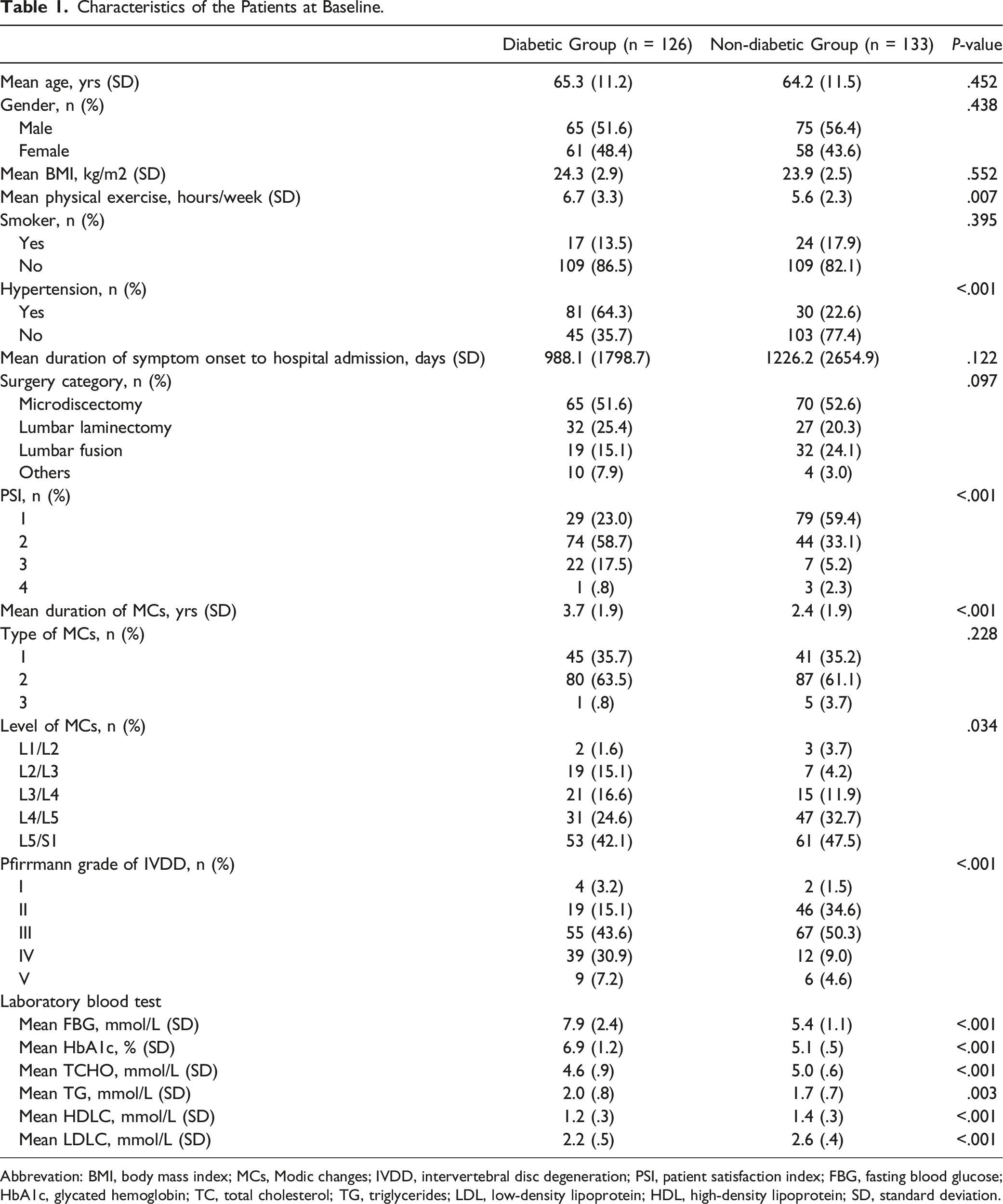
The duration of MCs was significantly longer (P < .001) in patients with DM (3.7 ± 1.9 years) compared to those without DM (2.4 ± 1.9 years). Significant differences (P = .034) were observed in the distribution of MCs in lumbar vertebrae between two groups, although the most frequent location was L4-S1 in both groups. There was a significant difference (P < .001) in the distribution of Pfirrmann grades of IVDD between the two groups. Grades IV and V accounted for 38.1% (48/126) of Pfirrmann grades in patients with DM, while only 13.6% (19/133) in patients without DM.
Patient-Reported Outcomes
Comparison of Preoperative and Postoperative Scores in Diabetic and Non-diabetic Patients.
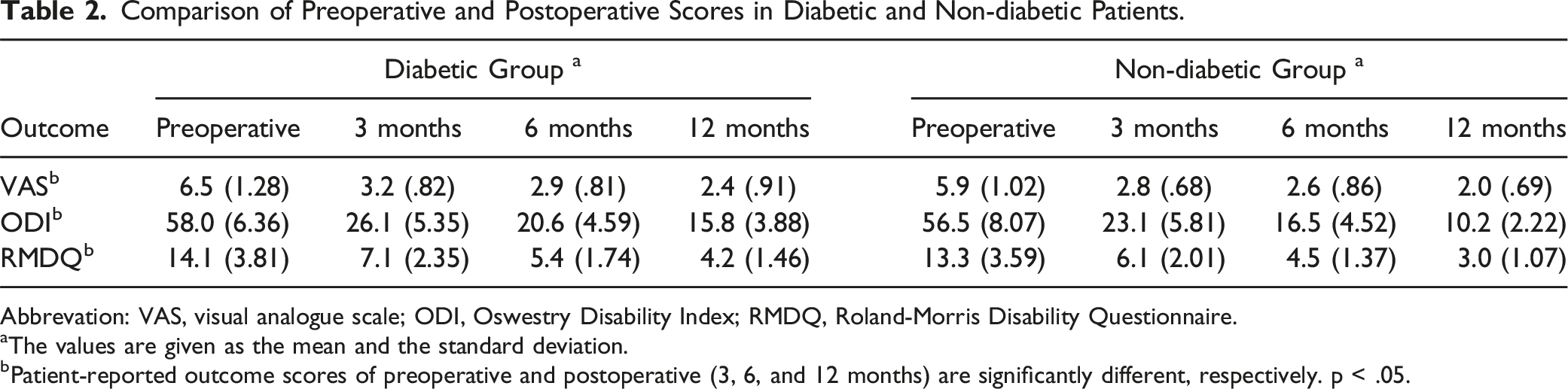
Abbrevation: VAS, visual analogue scale; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire.
aThe values are given as the mean and the standard deviation.
bPatient-reported outcome scores of preoperative and postoperative (3, 6, and 12 months) are significantly different, respectively. p < .05.
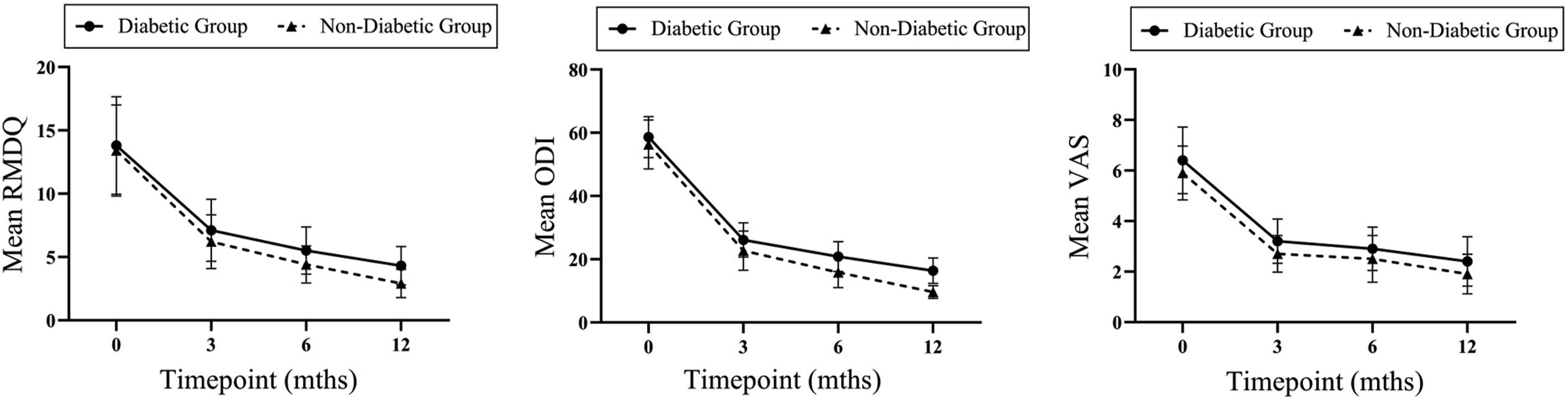
Caption: Temporal trends from Preoperative to one year after surgery in the diabetic and nondiabetic groups. Legend: (A) Mean Roland-Morris Disability Questionnaire (RMDQ). (B) Mean Oswestry Disability Index (ODI). (C) Mean visual analogue scale (VAS).
Multiple Linear Regression Analysis of Patient-Reported Outcomes at Three Months a .
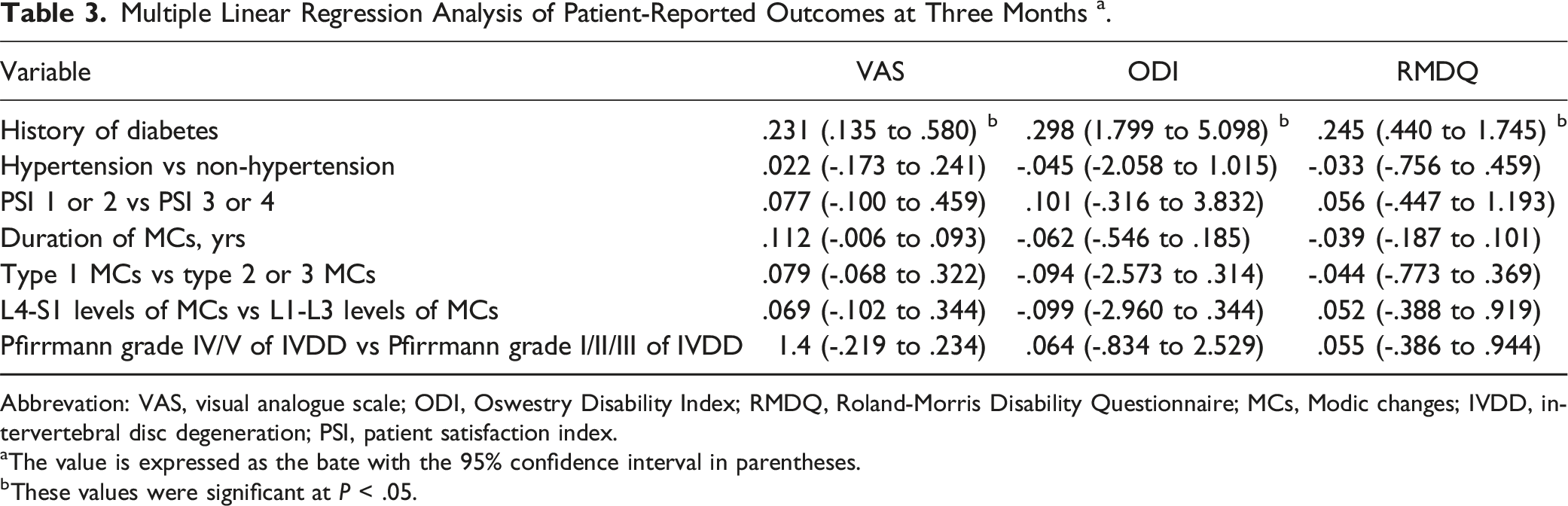
Abbrevation: VAS, visual analogue scale; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire; MCs, Modic changes; IVDD, intervertebral disc degeneration; PSI, patient satisfaction index.
aThe value is expressed as the bate with the 95% confidence interval in parentheses.
bThese values were significant at P < .05.
Multiple Linear Regression Analysis of Patient-Reported Outcomes at Six Months a .
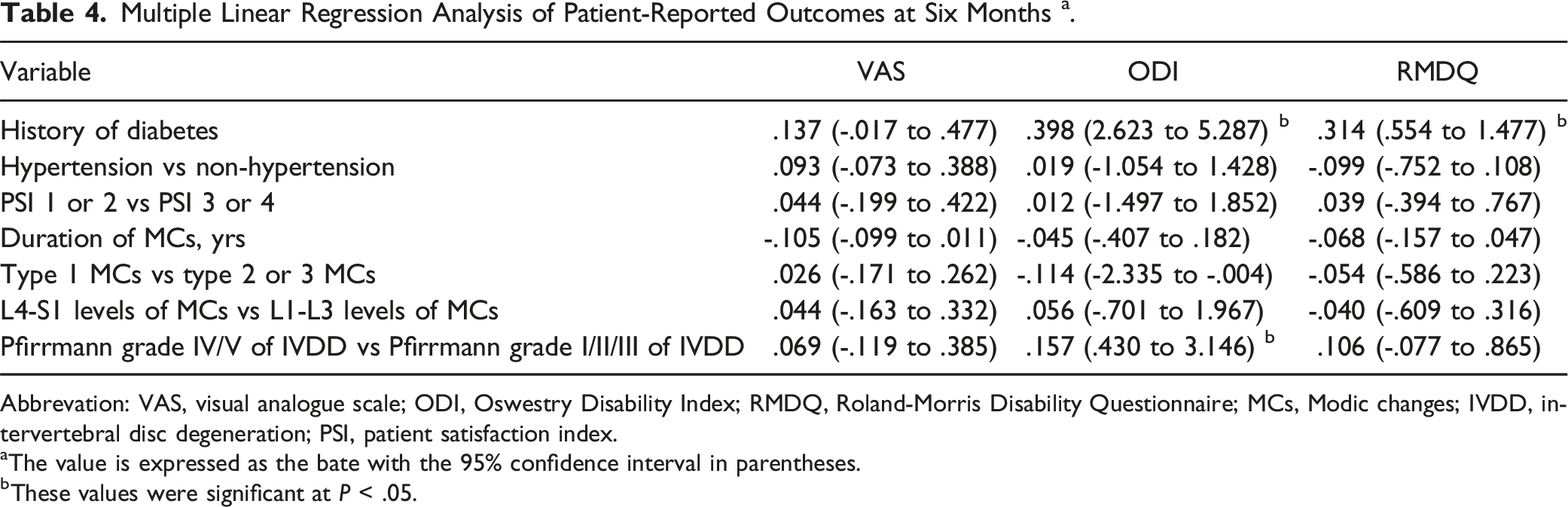
Abbrevation: VAS, visual analogue scale; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire; MCs, Modic changes; IVDD, intervertebral disc degeneration; PSI, patient satisfaction index.
aThe value is expressed as the bate with the 95% confidence interval in parentheses.
bThese values were significant at P < .05.
Multiple Linear Regression Analysis of Patient-Reported Outcomes at Twelve Months a .
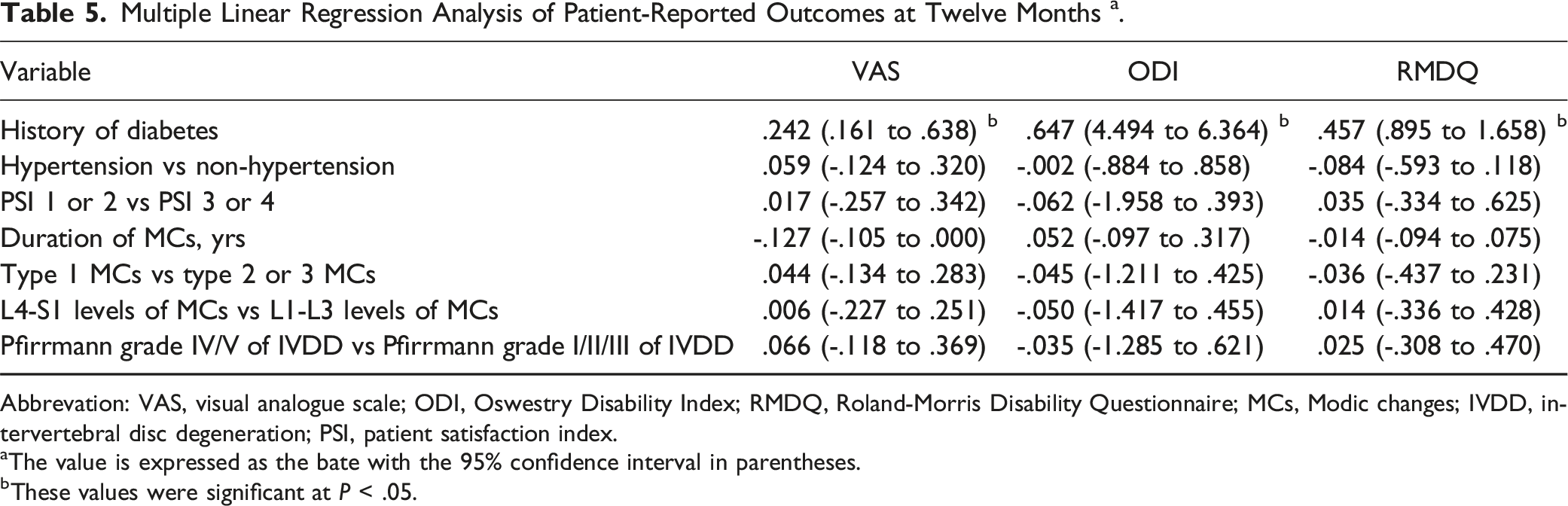
Abbrevation: VAS, visual analogue scale; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire; MCs, Modic changes; IVDD, intervertebral disc degeneration; PSI, patient satisfaction index.
aThe value is expressed as the bate with the 95% confidence interval in parentheses.
bThese values were significant at P < .05.
Discussion
This study is a prospective cohort study designed to examine the relationship between DM and CLBP with MCs. Our findings indicate that DM was associated with poorer patient-reported outcomes. Despite observing improvements in clinical outcomes from preoperative to postoperative stages in patients with DM, their scores remained worse compared to patients without DM in 1-year. Additionally, our research revealed that patients with DM had lower PSI, more severe disc degeneration, and a longer duration of MCs compared to patients without DM.
Studies have shown that hypertension is more prevalent in patients with DM compared to patients without DM.17,18 Multiple pathological mechanisms contribute to this association, including chronic activation of the renin-angiotensin-aldosterone system (RAAS), the sympathetic nervous system, and oxidative stress. 19 Although several clinical studies have investigated the association between hypertension and low back pain, the results remain controversial. In our study, we found no significant association between hypertension and low back pain. However, a recent study conducted in Saudi Arabia involving community-dwelling adults suggested that hypertension can cause low back pain. 20 On the other hand, two other studies indicated that hypertension may alleviate low back pain through hypertension-associated hypalgesia.21,22 To obtain a clearer understanding of the relationship between hypertension and CLBP, further prospective studies are needed.
Määttä et al 23 conducted a study to evaluate the relationship between MCs and IVDD. Their findings revealed that disc signal loss was associated with MCs. Additionally, mechanical stress not only accelerated disc degeneration but also caused microfractures. Moreover, the contact between the nucleus pulposus and the circulatory system led to the induction of an autoimmune response and subsequent development of MCs.24-26 In a previous study, we investigated the behavior of cartilage end-plate stem cells in a high-glucose environment, which demonstrated a tendency for osteogenic differentiation. This alteration in behavior affected the cartilage tissue of the end-plate, ultimately contributing to disc degeneration. 27 Furthermore, our research corroborated earlier findings by revealing that patients with DM experience more severe disc degeneration compared to those without DM. However, despite the significant difference in disc degeneration between the two groups, it did not affect the postoperative clinical outcome of the patients.
A study indicated that patients with DM engage in less physical activity compared to individuals without diabetes. 28 However, in our research, we discovered that patients with DM engage in longer durations of physical activity than those without DM, which may be attributed to the fact that patients with DM are often advised to incorporate more exercise into their routine. 29 Furthermore, it is worth noting that hospitalized patients with DM typically receive guidance to engage in more physical activity as part of their overall care plan aimed at facilitating a better recovery. 30
MCs in the lumbar vertebrae have been strongly associated with CLBP.8,31,32 Previous studies have demonstrated higher levels of tumor necrosis factor (TNF) in the cartilage end-plates of patients with MCs, specifically type 1 or type 2 endplates, compared to those without MCs. This elevation in TNF can induce inflammation, which stimulates sensory nerve fibers and consequently leads to low back pain 33 TNF is capable of axial transportation from the inflammatory site to dorsal root ganglion (DRG) neurons and the dorsal horn of the spinal cord. 34 This transportation, along with the activation of cytokines, can initiate the development of nociceptive neuropathy. 35 Furthermore, a systematic review has indicated that DM enhances the excitability of nociceptive afferents, resulting in painful diabetic neuropathy and mechanical ectopic pain in both patients with DM and animal models. 36 Moreover, it is important to note that DM can also impact the blood supply to the cartilage end-plate, thereby contributing to the development of MCs and IVDD. 11
The patient-reported outcomes of CLBP with MCs in patients with DM were found to be more severe compared to those without DM. Firstly, several factors such as the duration of DM, insulin resistance, diabetic neuropathy, and malnutrition may contribute to amyotrophy, leading to an accelerated loss of muscle and a slower recovery rate in patients with DM.37,38 Secondly, DM is known to cause microvascular complications, diabetic neuropathy, and nerve damage, which further impede the recovery process. 39 Consequently, patients with DM often exhibit lower PSI and experience worsened clinical outcomes with a slower recovery rate.
Armaghani et al 40 conducted a study that revealed patients with DM experienced more severe preoperative disability and worse postoperative patient-reported outcomes. Additionally, DM was identified as a high-risk factor for surgical infections in the spine. 41 However, this study did not find any significant difference in surgical procedures between patients with and without DM. This suggests that DM may not specifically influence surgical decision-making, but further investigation is necessary to explore this aspect. In patients with DM, their blood glucose levels, glycosylated hemoglobin, and lipid profiles were found to be higher compared to those without DM. The abnormalities associated with hyperglycemia affect insulin secretion, leading to disorders in lipid metabolism and resulting in metabolic disturbances in individuals with DM.42,43
Limitations of the Study
This study has a few limitations that should be acknowledged. Firstly, the glycemic control of post-discharge patients was unclear, and considering that glycemic control is known to influence clinical outcomes, the lack of this information presents a limitation. Secondly, in order to enhance the generalizability of our results, we enrolled participants who underwent various types of spine procedures. Although this approach aimed to increase the diversity of our sample, it may introduce bias in assessing the effects of these procedures on the relationship between DM and CLBP with MCs. Thirdly, it is important to note that this study was conducted at a single center, which may impact the generalizability of the findings. Additionally, the relatively short follow-up period limits our ability to extrapolate and make long-term conclusions based on our results. Fourthly, we collected and analyzed the covariates available in the medical records. Additional covariates were not collected for this study.
Conclusion
Patients with DM exhibited worse patient-reported outcomes compared to those without DM during the 1-year follow-up. The presence of microangiopathy in DM patients may directly impact CLBP or indirectly influence CLBP by affecting the development and severity of MCs. To further understand the underlying reasons for the poorer clinical outcomes observed in this particular patient population, additional laboratory studies and longer follow-up durations are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nature Science Foundation of Hubei Province (grant no. 2022CFB878) and General Hospital of Central Theatre Command of PLA Postdoctoral Foundation (grant no. 20220224KY29).