
Abstract
Study Design:
Retrospective cohort review.
Objective:
To determine whether higher levels of social support are associated with improved surgical outcomes after elective spine surgery.
Methods:
The medical records of 430 patients (married, n = 313; divorced/separated/widowed, n = 71; single, n = 46) undergoing elective spine surgery at a major academic medical center were reviewed. Patients were categorized by their marital status at the time of surgery. Patient demographics, comorbidities, and postoperative complication rates were collected. All patients had prospectively collected outcomes measures and a minimum of 1-year follow-up. Patient reported outcomes instruments (Oswestry Disability Index, Short Form–36, and visual analog scale–back pain/leg pain) were completed before surgery, then at 1 year after surgery.
Results:
Baseline characteristics were similar in all cohorts. There was no statistically significant difference in the length of hospital stay across all 3 cohorts, although “single patients” had longer duration of in-hospital stays that trended toward significance (single 6.24 days vs married 4.53 days vs divorced/separated/widowed 4.55 days, P = .05). Thirty-day readmission rates were similar across all cohorts (married 7.03% vs divorced/separated/widowed 7.04% vs single 6.52%, P = .99). Additionally, there were no significant differences in baseline and 1-year patient reported outcomes measures between all groups.
Conclusions:
Increased social support did not appear to be associated with superior short and long-term clinical outcomes after spine surgery; however, it was associated with a shorter duration of in-hospital stay with no increase in 30-day readmission rates.
Introduction
Patient-reported outcomes (PROs) and 30-day readmission rates are increasingly used as proxies for quality of health care received. 1,2 An important factor to higher PROs and lower 30-day readmission rates after surgery is how well the patient recovers postoperatively. Recovery from spine surgery is a complex process that involves a multitude of elements such as physical recuperation, social support, and psychological improvement. In an era of increased diversity of patients undergoing surgery, varying levels of social support adds to the complexity of the postoperative recovery process. Components of social support such as community participation, religious beliefs, and close relationships have all been associated with positive short- and long-term recovery and surgical outcomes. 3 –5
In particular, marital support has been identified as a potential contributor to superior clinical outcomes in both medical and surgical patients. In a study of 40 820 adult medical and surgical patients, Gordon et al 6 demonstrated that married patients had a significantly lower mortality rate, length of hospital stay, and discharges to a nursing home. Furthermore, the authors found that marital status was an independent risk factor for inpatient outcomes. 6 While there have been a few studies in spine surgery assessing the influence of spousal support and surgical outcomes, the impact of social support (ie, marital status) on postoperative recovery remains unknown.
The aim of this study is to assess whether higher levels of social support are associated with superior clinical outcomes (decreased 30-day readmission rates and higher PROs) after elective spine surgery.
Methods
This was a retrospective analysis of a prospectively collected database. A total of 430 medical records were retrospectively reviewed of adult patients undergoing elective spine surgery at a major academic medical center from 2008 to 2010. All patients enrolled in the study had symptomatic lumbar degenerative disc disease or spondylolisthesis. Institutional review board approval was obtained prior to study’s initiation. All patients in this study had baseline, 6-month, and 12-month PRO data. The patients were divided into 3 cohorts by marital status at time of surgery (Married cohort, n = 313; Divorced/Separated/Widowed cohort, n = 71; Single cohort, n = 46). We identified all unplanned readmissions within 30 days of discharge after indexed spine surgery.
Demographic variables evaluated included patient age, gender, and body mass index (BMI). Comorbidities included diabetes, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), congestive heart failure (CHF), hyperlipidemia (HLD), peripheral vascular disease (PVD), hypertension (HTN), and atrial fibrillation (AFib). Another preoperative variable collected was patient smoking status. Operative variables included length of surgery, number of vertebral levels involved, estimated blood loss (EBL), and urinary output (UOP). Postoperative complications included length of hospital stay (LOS), urinary tract infection (UTI), pneumonia, superficial surgical site infection (SSI), other infections, deep venous thrombosis (DVT), pulmonary embolism (PE), and 30-day readmission rate. Ambulation at discharge was also collected from physical therapy documentation.
PRO metrics were collected and compared between cohorts before surgery, and then 6 and 12 months after surgery. Functional status was determined by the Oswestry Disability Index (ODI). 7 Back and leg pain were assessed using the back/leg-pain visual analog scale (VAS-BP, VAS-LP). 8 Short Form–36 (SF-36) physical component score (PCS) and mental component score (MCS) was used for the assessment of physical and mental health status, respectively. 9 These questionnaires have been validated, widely used and accepted in spine research.
Parametric data was expressed as means ± standard deviations (SD) and compared via analysis of variance. Nominal data was compared with the chi-square test. All tests were 2-sided and were statistically significant if the P value was less than .05.
Results
A total of 430 adult patients (Married cohort, n = 313; Divorced/Separated/Widowed cohort, n = 71; Single cohort, n = 46) were included in this study. There was no significant difference in age between both groups (Married cohort: 53.13 ± 10.04 years vs Divorced/Separated/Widowed cohort: 53.39 ± 8.83 years vs Single cohort: 49.83 ± 10.63 years; P = .09; Table 1). No significant differences in BMI between both groups were observed (Married cohort: 30.68 ± 7.49 kg/m2 vs Divorced/Separated/Widowed cohort: 31.63 ± 8.74 kg/m2 vs Single cohort: 32.46 ± 8.71 kg/m2; P = .27; Table 1). More men were included in the Married cohort (47.28%) compared with the Divorced/Separated/Widowed cohort (26.76%) and Single cohort (32.61%; Table 1). There were no significant differences between both groups in the prevalence of other comorbidities such diabetes, COPD, CAD, CHF, HLD, HTN, PVD, AFib, and smoking status (Table 1).
Baseline Preoperative Variables.
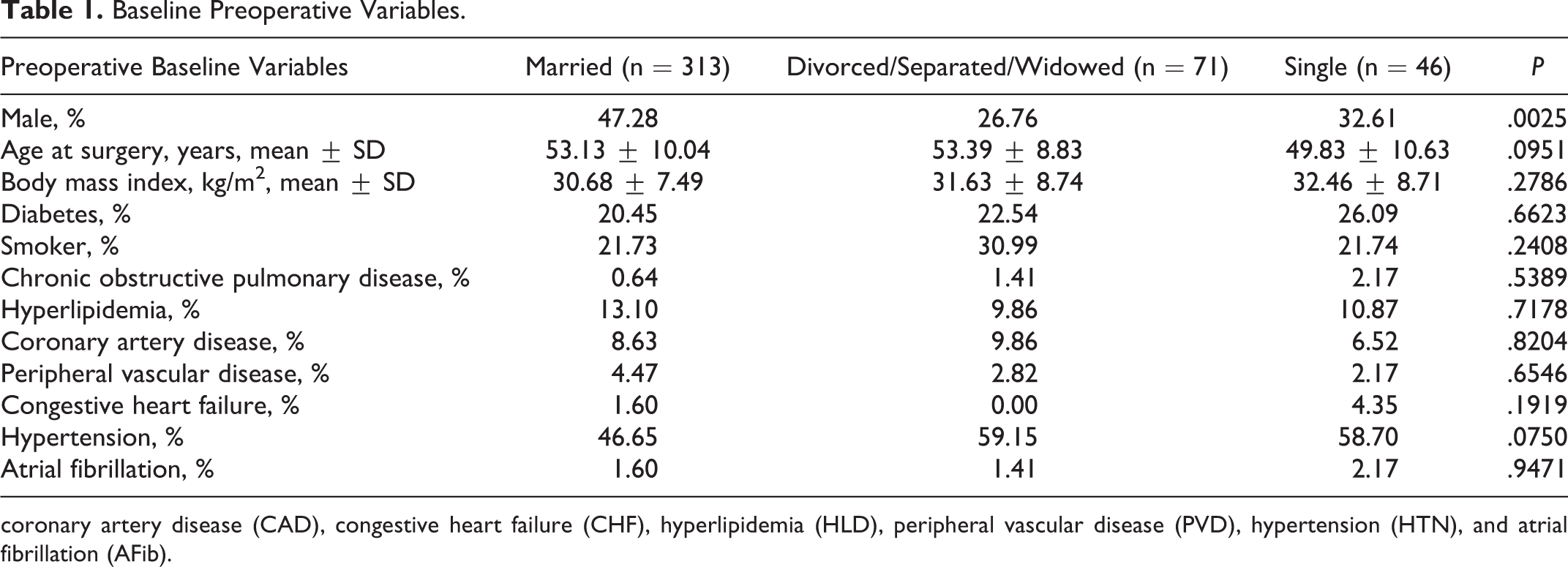
coronary artery disease (CAD), congestive heart failure (CHF), hyperlipidemia (HLD), peripheral vascular disease (PVD), hypertension (HTN), and atrial fibrillation (AFib).
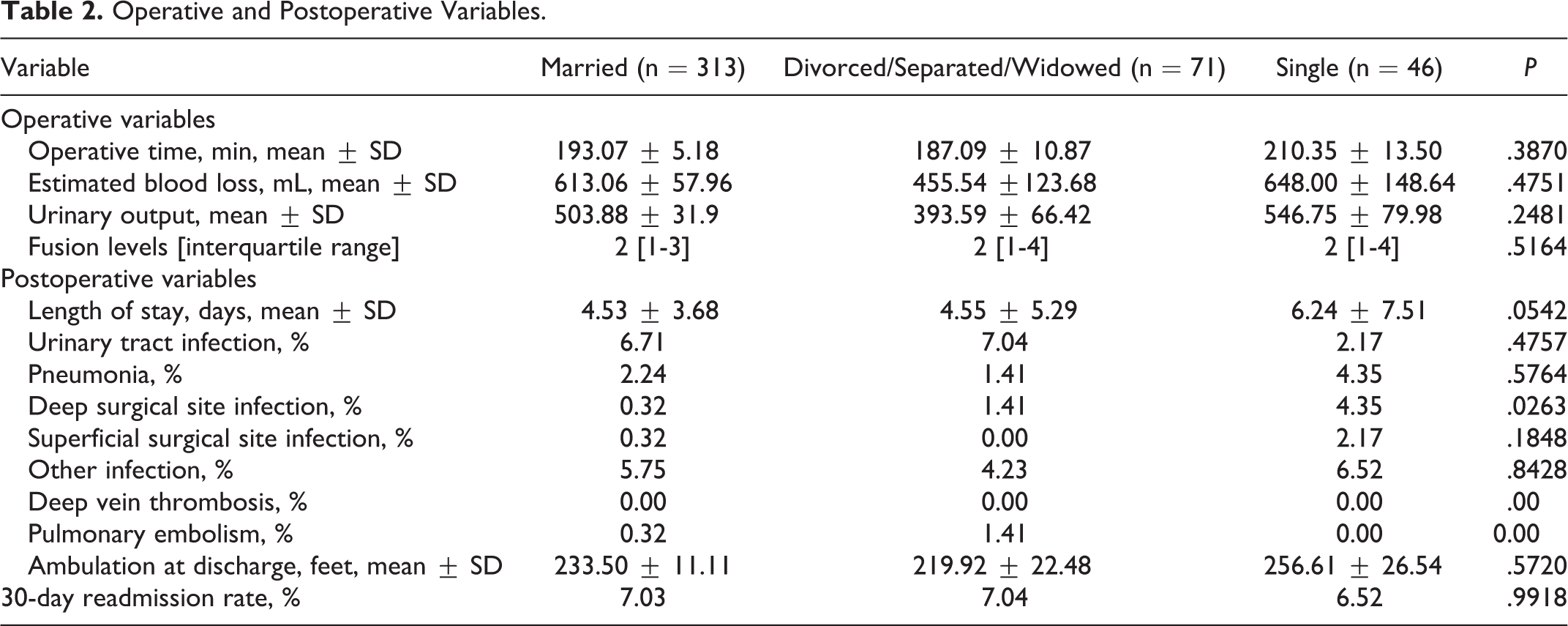
The mean ± SD operative times (minutes) for the Married, Divorced/Separated/Widowed, and Single cohorts were 193.07 ± 5.18, 187.09 ± 10.87, and 210.35 ± 13.50 minutes, respectively (Table 2). The mean ± SD estimated blood losses (mL) for the Married, Divorced/Separated/Widowed, and Single cohorts were 613.06 ± 57.96, 455.54 ± 123.68, and 648.00 ± 148.64 mL (P = .47), respectively (Table 2). There was no significant difference in the median number of levels operated between patient cohorts (P = .51, Table 2).
Operative and Postoperative Variables.
Eighty percent of patients enrolled in the study underwent a posterior lumbar decompression with fusion while 20% underwent decompression alone. In the fusion cohort, 73% were married, 16% divorced/separated, and 11% single. Thirty-day readmission rates were similar between patient cohorts (P = .91). Duration of in-hospital stay appeared to shorter in the married cohort compared to single cohort (Married cohort: 4.51 ± 5.10 days vs Divorced/Separated/Widowed cohort: 4.57 ± 5.26 days vs Single cohort: 6.25 ± 6.20 days, P = .45). At 1-year postoperatively, there was no significant differences in all patient reported outcome metrics between cohorts.
In the decompression alone cohort, 70% were married, 20% divorced/separated/widowed, and 10% were single. Thirty-day readmission rates were similar between patient cohorts (P = .98). Duration of in-hospital stay was shorter in the married cohort compared with single cohort (Married cohort: 4.58 ± 5.70 days vs Divorced/Separated/Widowed cohort: 4.52 ± 5.26 days vs Single cohort: 6.22 ± 6.90 days, P = .45). Similar to the fusion cohort, there was no observed difference in all patient reported outcome metrics 1-year postoperatively.
Thirty-Day Readmission Rates and Postoperative Complication Profile
There was no significant difference in 30-day readmission rates between patient cohorts (Married cohort: 7.03% vs Divorced/Separated/Widowed cohort: 7.04% vs Single cohort: 6.52%, P = .99), Table 2. Patients in the “married cohort” had a slightly shorter length of in-hospital stay when compared to Divorced/Separated/Widowed cohort, but a significantly shorter stay when compared with the “Single cohort” (Married cohort: 4.55 ± 5.29 days vs Divorced/Separated/Widowed cohort: 4.55 ± 5.29 days vs Single cohort: 6.24 ± 7.51 days; P = .05; Table 2).
The prevalences of postoperative complications were similar between all cohorts (Married vs Divorced/Separated/Widowed vs Single, respectively)—UTI (6.71% vs 7.04% vs 2.17, P = .47), pneumonia (2.24% vs 1.41% vs 4.35%, P = .57), superficial SSI (0.32% vs 0.00% vs 2.17%, P = .18), and other infections (5.75% vs 4.23% vs 6.52%, P = .84) (Table 2). No patient had a DVT or PE (Table 2).
Preoperative Baseline Pain, Functional Disability, and Quality of Life in Patients Undergoing Elective Spine Surgery With and Without Depression
At baseline, there was no significant difference in baseline pain, functional status, and quality of life between all cohorts. The mean ± SD ODI scores for Married, Divorced/Separated/Widowed, and Single cohorts were 44.28 ± 20.9, 48.68 ± 15.33, and 44.67±20.72, respectively (P = .47, Table 3). The preoperative mean ± SD VAS-LP scores for Married, Divorced/Separated/Widowed, and Single cohort were 3.41 ± 3.86, 2.58 ± 3.92, and 3.00 ± 4.20, respectively (P = .60, Table 3). The preoperative mean ± SD VAS-BP scores for Married, Divorced/Separated/Widowed, and Single cohorts were 4.16 ± 0.38, 4.12 ± 0.79, and 3.50 ± 1.16, respectively (P = .86, Table 3). The preoperative mean ± SD SF-36 PCS scores for Married, Divorced/Separated/Widowed, and Single cohorts were 28.98 ± 8.84, 28.31 ± 7.12, and 31.72 ± 12.83, respectively (P = .39, Table 3). The preoperative mean ± SD SF-36 MCS scores for Married, Divorced/Separated/Widowed, and Single cohorts were 44.15 ± 1.09, 38.92 ± 2.23, and 38.75 ± 3.29, respectively (P = .05, Table 3).
Baseline and 1-Year Patient-Reported Outcomes.a
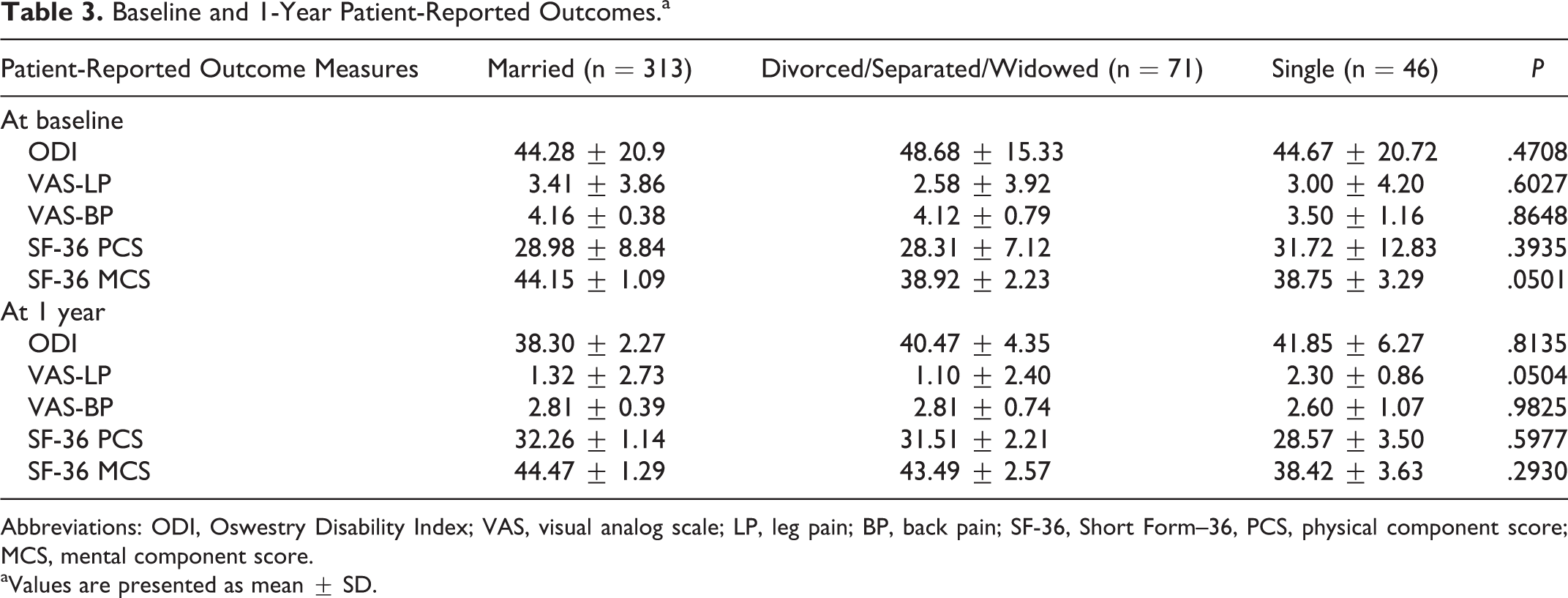
Abbreviations: ODI, Oswestry Disability Index; VAS, visual analog scale; LP, leg pain; BP, back pain; SF-36, Short Form–36, PCS, physical component score; MCS, mental component score.
aValues are presented as mean ± SD.
One-Year Postoperative Pain, Functional Disability, and Quality of Life in Patients Undergoing Elective Spine Surgery With and Without Depression
At 1 year postoperatively, there was no significant differences in all patient reported outcome metrics between cohorts. The mean ± SD ODI scores for Married, Divorced/Separated/Widowed, and Single-cohorts were 38.30 ± 2.27, 40.47 ± 4.35, and 41.85 ± 6.27, respectively (P = .81, Table 3). The preoperative mean ± SD VAS-LP scores for Married, Divorced/Separated/Widowed, and Single cohorts were 1.32 ± 2.73, 1.10 ± 2.40, and 2.30 ± 0.86, respectively (P = .05, Table 3). The preoperative mean ± SD VAS-BP scores for Married, Divorced/Separated/Widowed, and Single cohorts were 2.81 ± 0.39, 2.81 ± 0.74, and 2.60 ± 1.07, respectively (P = .98, Table 3). The preoperative mean ± SD SF-36 PCS scores for Married, Divorced/Separated/Widowed, and Single cohorts were 32.26 ± 1.14, 31.51 ± 2.21, and 28.57 ± 3.50, respectively (P = .59, Table 3). The preoperative mean ± SD SF-36 MCS scores for Married, Divorced/Separated/Widowed, and Single cohorts were 44.47 ± 1.29, 43.49 ± 2.57, and 38.42 ± 3.63, respectively (P = .29, Table 3).
Discussion
In this 1-year retrospective cohort study, we demonstrated that increased social support does not appear to be associated with superior short- and long-term clinical outcomes after elective spine surgery; however, it was associated with a shorter duration of in-hospital stay with no increase in 30-day readmission rates.
The effect of marital status and social support on surgical outcomes remains an area of ongoing debate and controversy. Previous studies observed an association between increased social support and superior surgical outcomes. In a study of 283 patients, Greenfield et al 10 observed that married patients had significantly higher instrumental activity of daily living scores, 1 year after surgery compared with single patients. Similarly, in a multicenter prospective study of 463 patients who underwent coronary artery bypass graft surgery, Jenkins et al 11 demonstrated that social support was a predictor of postoperative cardiac symptom relief. In another study of 56 male patients who underwent coronary bypass surgery, Kulik et al 12 found that married patients required less pain medications and recovery time compared with the single patients. Hurme and Alaranta, 13 in a study of 357 consecutive patients, found that patients’ marital status was highly correlated with operative results. Similarly, in a prospective controlled trial of 46 patients undergoing lumbar discectomy, Schade et al 14 demonstrated that support from the patient’s spouse was an independent predictor of long-term postoperative pain relief. In the Spine Patient Outcomes Research Trial (SPORT) evaluating PROs after discectomy, Koerner et al 15 demonstrated from a 4-year multivariate analysis that being married resulted in greater treatment effect with surgery. Finally, in another study of 19 patients who had undergone spinal decompression surgery, Laxton and Perrin 16 found a significant correlation between patients’ social support scores and health-/nonhealth-related quality of life scores. While this study did not find an association between higher levels of social support and superior PRO metrics, there was an association between higher levels of social support and shorter duration on in-hospital stays.
In contrast, few studies have demonstrated no association between marital status and surgical outcomes. Gatchel et al, 17 in a study of 1679 patients, observed no significant association between marital status and surgical outcomes. Furthermore, the authors conclude that marital status does not play a significant role in health and socioeconomic treatment outcomes for these patients. 17 Similarly, in study of 170 consecutive patients, Rasmussen et al 18 demonstrated no association between marital status and superior surgical outcomes. In a prospective study of 57 patients who underwent surgery for a herniated lumbar disc, Sorensen et al 19 did not find marital status or amount of social support as predictors of postoperative outcomes. Analogous to the aforementioned studies, this study did not find an association between social support and superior postoperative PRO scores; nor did we find any differences in 30-day readmission rates.
Despite these conflicting viewpoints on the effect of social support on surgical outcomes, it is a variable that should be considered. Several studies have shown that lack of social support is associated with prolonged hospital stays an increased overall health care expenditure. In a study of 161 patients who underwent elective colorectal surgery, Ngui et al 20 found that patients who were widowed or divorced had a 3- and 1.5-fold increase, respectively, in length of hospital stay due to discharge placement delay when compared to married patients. In a study of 712 patients who underwent elective hip and knee replacement surgery, Husted et al 21 demonstrated patients living alone had a significantly greater probability of staying in the hospital more than 3 days when compared with patients who had a spouse. In another study of 808 patients after hip and knee arthroplasty, Lin et al 22 found that patients with unmarried marital status was an independent for predictor of length of hospital stay after surgery. These studies corroborate our findings and suggest that lower levels of social support may result in prolonged in-hospital stay and higher healthcare costs. In a cost-conscious health care climate, early identification of these risk factors could result in shorter in-hospitals stays, improvement in patient experience and facilitate postdischarge care coordination.
Not surprisingly, higher levels of social support may be associated with lower rates of affective disorders. Several studies have shown lower rates of depression and anxiety in middle-aged women with higher levels of social support have. 23 In a study of 1072 patients who underwent coronary artery bypass grafting (CABG), Barry et al 24 demonstrated that married patients had significantly high perceived emotional and instrumental support. Similarly, in a study of 214 patients who underwent CABG, Lindsay et al 25 found that increased levels of social support improved mental component scores 1 year after CABG.
This study has limitations, ensuing possible implications for its interpretation. The breadth of the social support network was not available for the study, which could contribute to the perceived state of well-being. The failure to quantify psychological distress in patients’ social environment could have biased the observed results. The duration and quality of social support was also not known, which precludes us from making firm conclusions based on the observed results. While pre- and perioperative variables were prospectively collected, data was retrospectively analyzed for the purposes of this study, therefore are subject to the weaknesses of a retrospective analysis. Despite these limitations, this study suggests that higher levels of social support did not appear to results in superior clinical outcome; however, it was associated with shorter in-patient hospital stays.
Conclusion
Increased social support did not appear to be associated with superior short- and long-term clinical outcomes after spine surgery; however, it was associated with a shorter duration of in-hospital stay with no increase in 30-day readmission rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.