
Abstract
Study Design:
Retrospective cohort study.
Objective:
The purpose of the study was to compare early complication, morbidity and mortality risks associated with fusion surgery crossing the cervico-thoracic junction in patients aged over 80 years undergoing combined anterior and posterior approach versus a posterior-only approach.
Methods:
We retrospectively identified octogenarian patients with myelopathy who underwent fusion crossing the cervico-thoracic junction. Patient demographics, Nurick score, surgical characteristics, complications, hospital course, early outcome and 90-day mortality were collected. Comorbidities were classified using the age-adjusted Charlson Comorbidity Index (AACCI). Radiographic measurements for deformity correction included the C2-C7 sagittal Cobb angle, C2-7 sagittal vertical axis and T1 slope pre- and postoperatively.
Results:
Out of 8,521 surgically treated patients, 12 octogenarian patients had a combined anterior and posterior approach (AP group) and 14 were treated from posterior-only (P group). Mean age was 81.4 ± 1.2 and 82.5 ± 2.7 years, respectively. There was no significant difference in Nurick scores between the groups (P > 0.05). The major complication risk in the AP group was significantly higher, requiring PEG tube placement due to severe dysphagia in 4 patients (33%) compared to none in the P group. A greater improvement in cervical lordosis could be achieved through a combined approach. The 90-day mortality risk was 8% for the AP group and 0% for the P group.
Conclusions:
A combined anterior and posterior approach is associated with a significantly higher major complication rate and can result in severe dysphagia requiring PEG tube placement in one-third of patients over 80 years of age.
Introduction
Degenerative cervical spondylosis with myelopathy (CSM) is the most common cause of spinal cord dysfunction in the elderly worldwide.1-3 When symptoms occur, surgery is the most effective procedure to halt neurological deterioration and to improve neurological status and quality of life.4,5 However, there is still controversy when octogenarians are involved, who often suffer from multilevel CSM with accompanying kyphosis which may require a more complex strategy.6,7 Furthermore, elderly patients often have a diminished recovery potential due to comorbidities, less physiological reserves compared to younger patients and age-related changes of the spinal cord with decrease in numbers of myelinated nerve fibers.7-9
The presence of cervical kyphosis leads many surgeons to perform a combined anterior and posterior fusion procedure crossing the cervico-thoracic junction to achieve cervical sagittal alignment.7,10 It has been shown that a combined anterior and posterior decompression and fusion procedure is associated with substantial complications10,11 and a 178 times increased risk of acute postoperative airway emergency, compared to an isolated posterior-only approach. 12
A recently published U.S. national database study analyzed the association between complication and mortality risk and age after cervical spine surgery for degenerative disease. 13 The authors found that patients older than 74 years with a primary diagnosis of CSM who had a combined anterior and posterior or posterior-only approach have a 4.1 times higher risk of having a complication and a 19 times higher risk for in-hospital mortality compared to patients aged 20-34 years. 13
Although many articles exist concerning complications and mortality in cervical spine surgery in elderly patients13-17, no data analyzing patients over 80 years who underwent surgical fusion for multilevel cervical stenosis crossing the cervico-thoracic junction is currently available. The purpose of this current study was to compare complications, morbidity and early outcome in patients over 80 years of age between those who had a combined anterior and posterior or posterior-only approach for treatment of cervical kyphosis with myelopathy.
We further hypothesized that complications, especially dysphagia and reintubation are more common after a combined anterior and posterior approach in an elderly cohort.
Materials and Methods
This retrospective cohort study was approved by the institutional review board (ID: STUDY2018000489) and is in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. 18
Patients
We performed a review of the electronic medical records of 8,521 consecutive patients who underwent surgical treatment at our institution from January 2014 to June 2018. All patients 80 years of age and older with the diagnosis of cervical deformity with degenerative CSM and/or radiculopathy who underwent either a combined single-stage anterior and posterior or a posterior-only decompression and fusion procedure crossing the cervico-thoracic junction were included. Cervical deformity was defined as presence of one of the following criteria: C2-C7 sagittal cobb angle (C2-C7 SCA) ≥ 10° or C2-C7 sagittal vertical axis (C2-C7 SVA) > 4 cm or chin-brow vertical angle (CBVA) ≥ 25°. 19 Patients were not excluded if they had a previous cervical spine surgery. Patients with tumor, infection, cervical fracture and ankylosing spondylitis were excluded. All patients included had a minimum follow-up period of 3 months.
Procedures
Anterior procedures included single- or multi-level discectomies and/or corpectomies using cages filled with morselized autograft or fibular allograft. The posterior instrumentation included 3.5 mm lateral mass and pedicle screws with 3.0 mm rods. Correction of kyphosis was achieved by loading a compressive force between the inserted screws and facet release. The cranial extent of fusion varied from C1 to C2 and the caudal extent from T1-T3 depending on the surgeon’s preference and experience
Pre-Operative Baseline Characteristics
Patient demographics, body mass index (BMI), comorbidities, American Society of Anesthesiologists (ASA) score, and pre-operative neurological status. Comorbidities were preoperatively assessed based on the age-adjusted Charlson Comorbidity Index (AACCI).20,21 The AACCI score was calculated for each patient to classify comorbidity and grouped as having either no comorbidity (AACCI = 0), minimal comorbidity (AACCI = 1-2), moderate comorbidity (AACCI = 3-5), or severe comorbidity (AACCI > 6).
Outcomes
Outcomes were divided into perioperative (surgical time, intra- and perioperative complications, blood loss) hospital course (hospital stay, ICU stay), post-operative complications (reoperation, 90-day readmission, and 90-day mortality), and radiographic assessments. Surgical time was calculated from first incision through closure of the second wound, including repositioning of the patient. Perioperative complications were categorized as major or minor. Major complications included percutaneous endoscopic gastrostomy (PEG) tube placement, post-operative myocardial infarction, vocal cord paralysis, and pulmonary embolism.
Minor complications included delirium, dysphagia, pneumonia, urinary retention, urinary tract infection, deep vein thrombosis, ileus and superficial wound infection.
Preoperative and postoperative Nurick score at 3-months follow-up was documented.
Statistical Analysis
Bivariable analysis was performed to compare those who underwent an AP procedure versus those who underwent a posterior-only procedure. For categorical variables, frequency counts were computed and presented along with their percentages. For continuous variables, means were computed and presented along with their standard deviation. To compare categorical variables, the Fisher’s exact test was used. For continuous outcomes, a t-test was used. Because these procedures are so rare in octagenarians, and our sample size was small, we were unable to perform a multivariable analysis to adjust for potential confounding. All analysis were performed using Stata 13.1.
Results
Baseline Characteristics
A total of 26 consecutive octogenarian patients met study criteria and were included in this study. All patients presented with myelopathic symptoms with or without radiculopathy. 12 patients had a combined single-stage anterior and posterior approach (AP group) (Figure 1) and 14 patients were treated from posterior-only (P group) (Figure 2).

Preoperative lateral X-ray (A), sagittal MRI (B) and sagittal CT-scan (C) of a 83-year old patient with post-laminectomy kyphosis and persistent myelopathy. Postoperative sagittal CT-scan after single stage anterior discectomy and fusion at C6/7, anterior corpectomy of C5, and posterior fusion from C2 to T2 (D).

Lateral X-ray (A), sagittal MRI (B) and sagittal CT-scan (C) of a 80-year old patient with severe cervical kyphosis preoperatively. Spinal fusion from C2 to T3 (posterior-only) was performed to achieve adequate deformity correction seen on postop sagittal CT-scan (D).
The AP group included 8 males and 4 females with a mean age of 81.4 ± 1.2 years (range 80-84 years) and a mean BMI of 25.9 ± 4.9 kg/m2. The P group included 7 males and 7 females with a mean age of 82.5 ± 2.7 years (range 80-87 years) and a mean BMI of 24.5 ± 2.2 kg/m2. No significant difference in age, sex and BMI were noted between both groups (P > 0.05) (Table 1).
Comparison of Demographic and Surgical Parameters.a
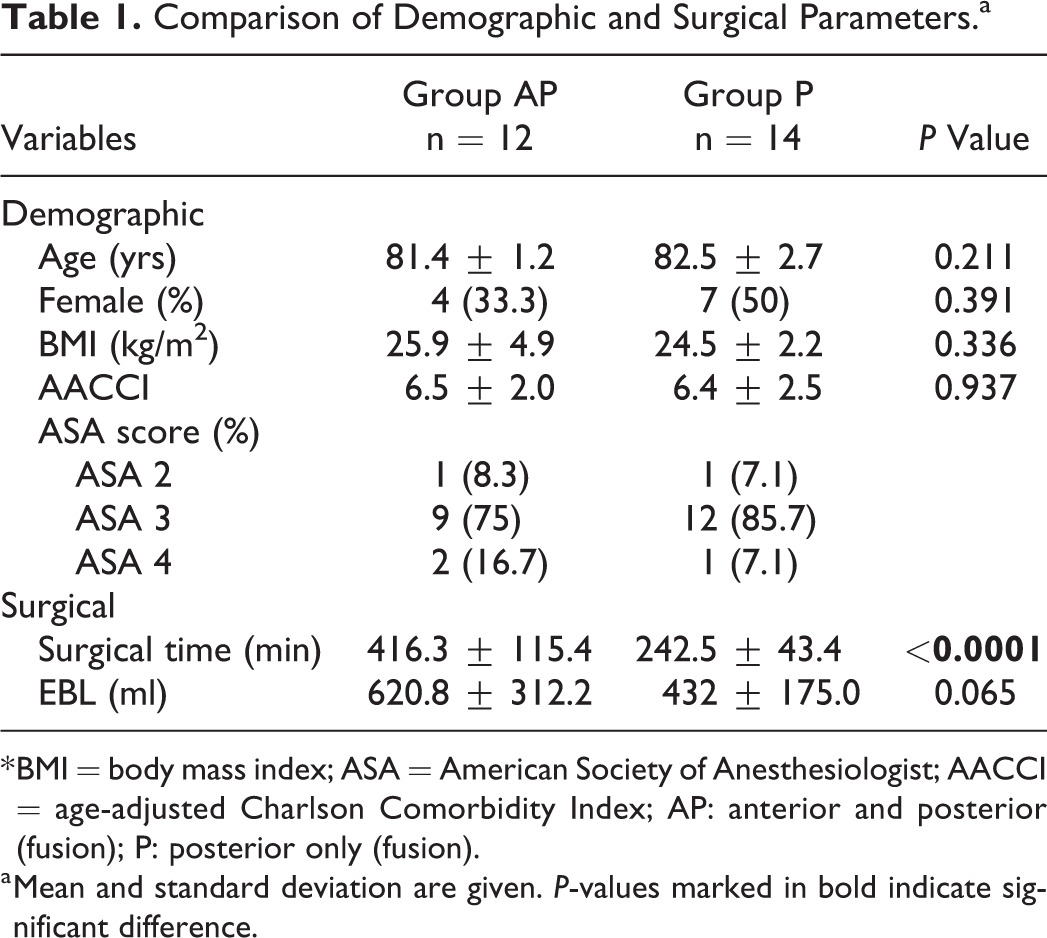
* BMI = body mass index; ASA = American Society of Anesthesiologist; AACCI = age-adjusted Charlson Comorbidity Index; AP: anterior and posterior (fusion); P: posterior only (fusion).
a Mean and standard deviation are given. P-values marked in bold indicate significant difference.
The mean AACCI was 6.5 ± 2.0 for the AP group and 6.4 ± 2.5 for the P group which did not reveal a significant difference between the groups (P < 0.05). Preoperative narcotic-relevant ASA scoring revealed1 patient (8%) with an ASA 2 score, 9 patients (75%) with an ASA 3 score and 2 patients (17%) with an ASA 4 score in the AP group. In the P group 1 patients (7%) was classified as ASA 2 and 1 patient (7%) as ASA 4, whereas 12 patients (86%) revealed an ASA 3 score. No significant difference in terms of preoperative anesthetic risk was found between the groups (P > 0.05) (Table 1). Preoperative C2-C7 SCA, C2-C7 SVA and T1 slope did not show a significant difference between the groups (P > 0.05).
Perioperative Outcomes
Five patients in each group had previous cervical spine surgery; 4 anterior and 1 posterior in each group. Details regarding surgical characteristics are presented in Table 1. Mean surgical time in the AP group was 416.3 ± 115.4 min and 242.5 ± 43.4 min in the P group, P < .0001. The intra-operative blood loss in the AP group ranged from 250 cc to 1250 cc with a mean blood loss of 620.8 ± 312.2 cc. In the P group intra-operative blood loss ranged between 250 cc and 800 cc with a mean blood loss of 432 ± 175 cc. No significant difference was found between both groups (P > 0.05) (Table 1). The mean preoperative Nurick score (±SD) in the AP group was 3.2 ± 1.3 compared to 2.9 ± 1.3 in the P group. A slight improvement in Nurick score (±SD) was seen at 3-months follow-up (2.4 ± 0.9 in the AP group and 2.3 ± 1.0 in the P group) that was statistically nonsignificant across the time. There was also no significant difference between both groups (P > 0.05).
Hospital Course Outcomes
No patient experienced deterioration in neurological status after surgery. Patients in the AP group had a slightly longer hospital and shorter ICU stay, compared to the P group (9.3 ± 4.4 days and 2.6 ± 1.6 days vs. 8.9 ± 6.9 days and 2.9 ± 4.1 days), but without significant difference between both group (P > 0.05). One patient of the AP group died within a few days after surgery due to a fulminant pulmonary embolism with respiratory failure. No in-hospital mortality was noted in the P group. Therefore, the overall in-hospital mortality was 8% for the AP group and 0% for the P group. Four patients in the AP group could be discharged home, compared to 3 patients of the P group. The remaining patients went to a skilled nursing facility. At 3-months follow-up no further mortality occurred.
Post-Operative Complications
Complications occurred in 10 patients (83%) of the AP group compared to 13 patients (93%) of the P group. There was a significant difference in having major complications between both group (P < 0.05) (Table 2). Due to severe dysphagia, 4 patients (33%) of the AP group required a PEG tube placement compared to none in the P group which was also statistically significant. Myocardial infarction and vocal cord paralysis occurred in one patient each of the AP group. The only major complication that had occurred in the P group was myocardial infarction. More than one minor complication occurred in 6 patients (50%) of the AP group, compared to 4 patients of the P group (29%). The most frequent minor complication in the AP group and P group were dysphagia (58% vs. 57%), followed by urinary retention (33% vs. 21%) and delirium (17% vs. 21%) (Table 2).
Major and Minor Complications Occurred in Both Groups.
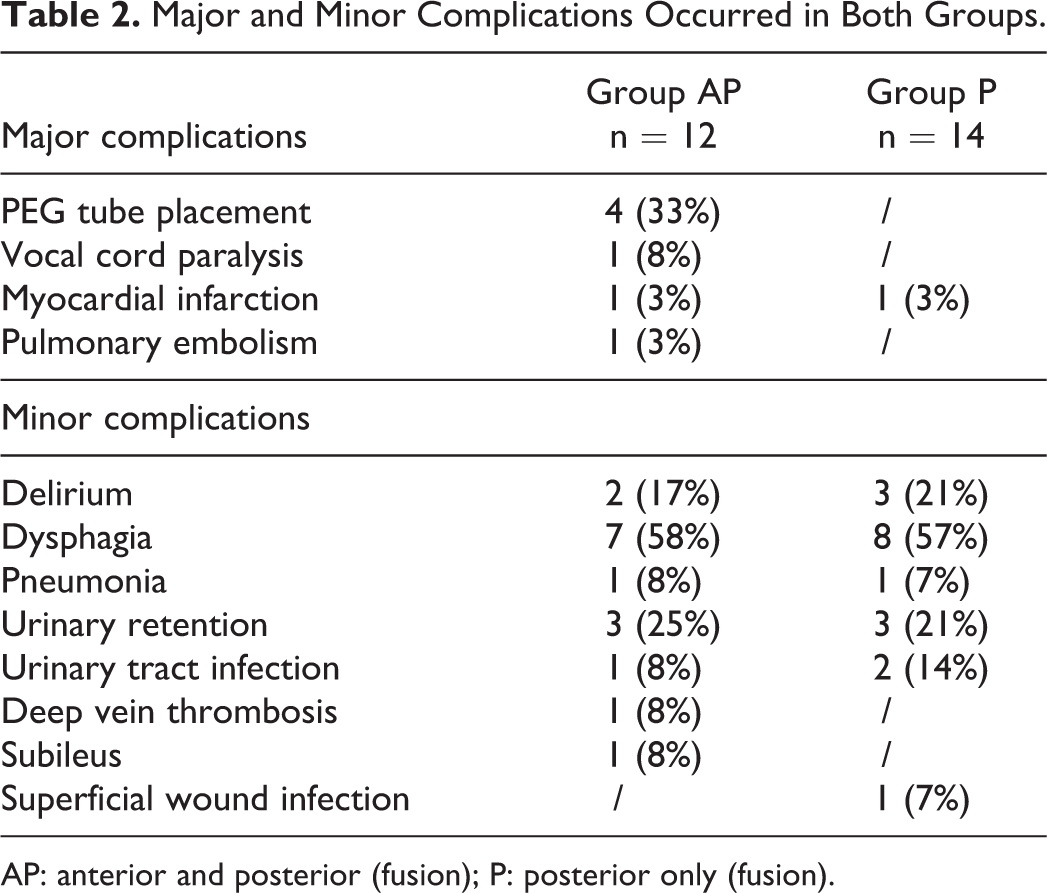
AP: anterior and posterior (fusion); P: posterior only (fusion).
One patient in the AP group developed a distal junction failure after 3 months with a T2 burst fracture (Figure 3A and B), which required surgical revision (Figure 3C-E). Two patients of the P group were readmitted within 3 months, one with dehydration and one with superficial wound infection requiring revision surgery. Another patient of the P group presented with a disengaged T2 screw at 2-year follow-up, which has not been revised.
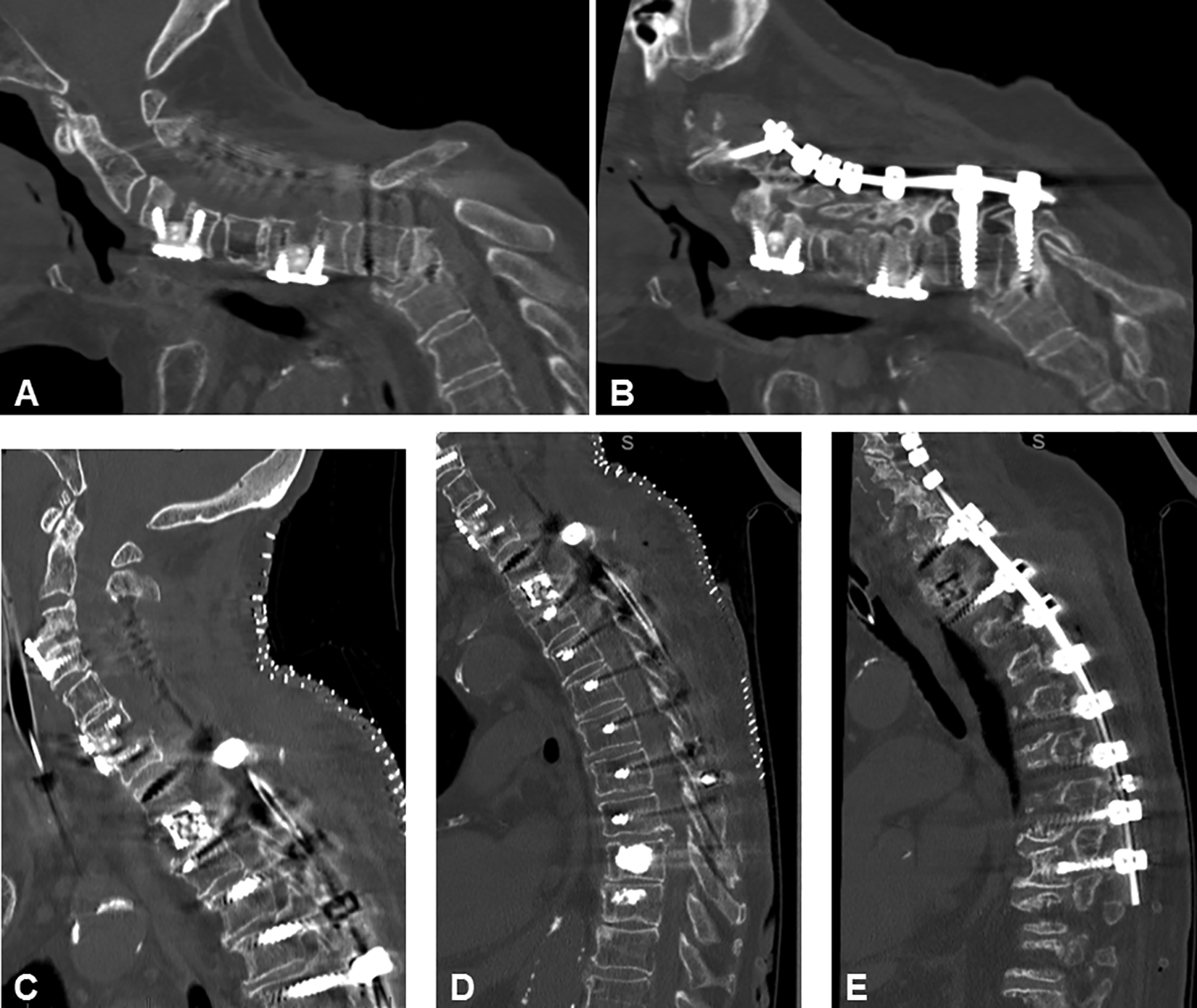
Sagittal CT-scans of a 83-year old patient who developed a distal junction failure after 3 months with a T2 burst fracture after a combined anterior and posterior approach (A, B). Surgical revision with T2 corpectomy, C2-T9 fusion and cement injection into T9 and T10 was obtained (C, D, E).
Radiographic Assessments
Postoperative cervical lordosis measured with the C2-C7 Cobb angle showed a significantly higher mean increase in cervical lordosis in the AP group (−13.2 ± 6.9°) compared to the P group (10.3 ± 5.0°) (P < 0.05). The postoperative C2-C7 SVA did not show a significant difference between the groups (P > 0.05). A significantly higher improvement in the T1 slope was seen in the AP group (35.4 ± 6.8 mm) compared to the P group (42.2 ± 7.7 mm) (P < 0.05). The radiographic data is depicted in Table 3.
Mean Values of Preop, Postop and Postop Minus Pre-p Cervical Parameters.a
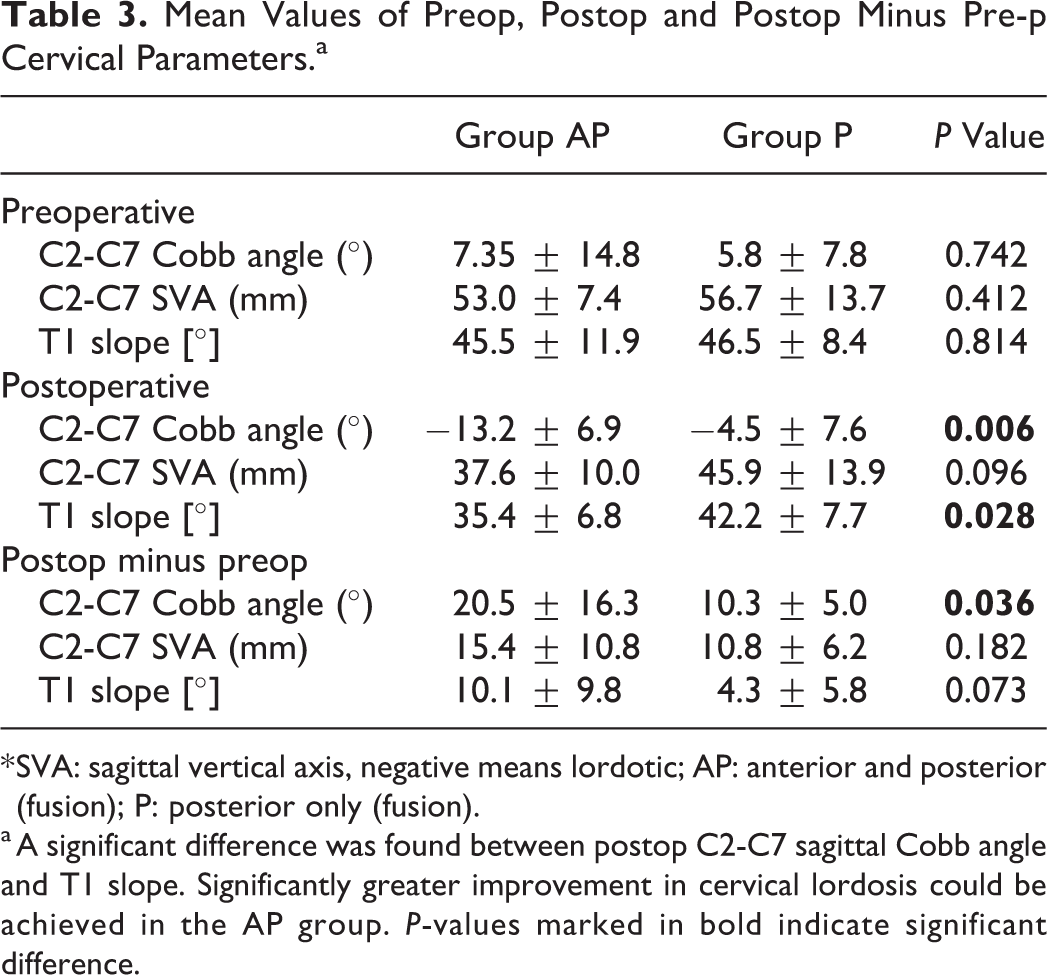
* SVA: sagittal vertical axis, negative means lordotic; AP: anterior and posterior (fusion); P: posterior only (fusion).
a A significant difference was found between postop C2-C7 sagittal Cobb angle and T1 slope. Significantly greater improvement in cervical lordosis could be achieved in the AP group. P-values marked in bold indicate significant difference.
Discussion
Surgical treatment of multi-level CSM in octogenarians remains challenging, especially in the presence of cervical deformity. Variables such as progressive degeneration, multiple comorbidities and limited physiological reserves all contribute to increased level of surgical complexity. With an increased life expectancy, the incidence of CSM in the elderly requiring cervical reconstruction may continue to increase over the next decades.1,2,22 In addition, it is well known that elderly patients who had surgical treatment of their CSM are at greater risk of encountering complications such as urinary retention, acute delirium, dysphagia, cardiovascular and respiratory complications.13,23,24 As a result, these complications may result in longer hospital and ICU stays, greater inpatient mortality rate, higher costs and increased readmission rate.23,25,26
The best surgical treatment for multilevel CSM with kyphotic deformity still remains a matter of debate.2,11,27,28 On one hand, authors state that sufficient correction can be achieved from posterior-only.11,29 On the other hand, a combined anterior and posterior approach allows for anterior and posterior release and osteotomies which can achieve better correction compared to posterior-only.2,30 Recent articles have highlighted an increasing emphasis on the importance of sagittal alignment of the cervical spine.31-33 For example, it has been shown that cervical malalignment may be associated with worse clinical outcome and less neurologic recovery in degenerative CSM.30,32 Therefore, most studies suggest a combined anterior and posterior approach in degenerative CSM with kyphotic deformity to obtain adequate correction. Surprisingly, studies analyzing the octogenarian population are lacking30-32,34
Our results demonstrate that fusion surgery crossing the cervico-thoracic junction performed in octogenarians from a combined anterior and posterior approach bears a higher major complication rate compared to a posterior-only approach. As expected, a high postoperative minor complication rate was observed in both groups, of which the major complication rate, which was significantly higher in the AP group, was relatively low compared to previously published studies assessing complex spinal surgery in an elderly cohort.8,10,13 Interestingly, although no significant difference was found with regard to general risks of postoperative dysphagia, its severity was higher in patients who had undergone a combined anterior and posterior approach, making a PEG tube placement necessary in 4 patients (33%). In addition, there were no significant differences in terms of hospital and ICU stay, in-hospital mortality, readmission and reoperation rates.
To the best of our knowledge, this study represents the first study comparing complication and morbidity risks in octogenarians undergoing either combined anterior and posterior or posterior-only fusion surgery crossing the cervico-thoracic junction for multi-level CSM with cervical kyphosis.
Literature
Using the National Inpatient Sample (NIS), Wang et al. evaluated complications and mortality associated with age, diagnosis and procedure in the context of cervical spine surgery for degenerative disease. 13 The authors also included patients older than 74 years receiving a combined anterior and posterior or posterior-only approach for degenerative CSM. They concluded that complications rate is significantly increased in elderly patients with the diagnosis of CSM who underwent a combined anterior and posterior or posterior-only approach. National database studies in general have several limitations. In addition to the general limitations of national database analysis of potentially having underreported coding, 35 specific limitations of that study was that it did not address the cervico-thoracic junction.
In 2008, Hart et al. 10 published so far the only study which has assessed perioperative complications and outcome of patients who have undergone a combined anterior and posterior decompression and fusion for treatment of multi-level CSM with kyphosis. 13 patients with a mean age 56 years (range 39-74 years) were included. The authors demonstrated a high incidence of perioperative complications using a combined anterior and posterior procedure. However, most complications were minor and resolved without intervention or significant effect. 10 The most common minor complication was dysphagia (46%), the most common major complication was airway edema requiring prolonged intubation or reintubation, which was required in 38% of patients. 10
In a more recently published study, Hart et al. 36 conducted a study in patients with the above mentioned diagnosis and procedure to evaluate the intraoperative fluid management and its role in the development of airway edema after a combined anterior and posterior approach. After adoption of a standardized protocol with reducing intraoperative volume of fluid replacement, the incidence of airway edema was significantly reduced, albeit this did not influence the development of dysphagia postoperatively. 36 However, a specific analysis of elderly patients and a comparison of a combined versus posterior-only approaches were lacking in both studies.
Combined Anterior and Posterior or Posterior Only
This study shows that adequate deformity correction can be achieved by using a posterior-only approach but the correction of lordosis is significantly higher when a combined anterior and posterior approach is performed. Recent literature pointed out that greater improvement of cervical alignment also correlates with a superior clinical outcome.32,37 On the other hand, a combined anterior and posterior approach is associated with a significantly longer surgical time and can result in severe dysphagia requiring PEG tube placement in one-third of octogenarian patients.
The decision of surgical approach eventually depends on the surgeon’s experience and preference. Other variables which also may have influenced the surgical approach were location of stenosis, degree of cervical kyphosis and medical condition preoperatively. Although a general consensus exists that all stenotic levels should be decompressed and included in the fusion construct, there is no literature available which approach is recommended.
Limitations
This study has several major limitations. The retrospective nature of this study can introduce selection and observer bias which have to be taken into account. We have a small sample size in each group which makes comparisons less effective especially if there are potential factors that we are not accounting for; however, this is a rare population and therefore a larger sample size would not be possible without a national database. The follow-up period is short and long-term data gathering may reveal other relevant findings not captured in the current study. Furthermore, the surgical procedure was not standardized. Additional radiographic parameters which include compensatory mechanisms such as thoracic hypokyphosis, lumbar hyperlordosis or pelvis retroversion were not evaluated.
Conclusion
Currently, no guidelines exist for the optimal management of multilevel CSM with kyphotic deformity in elderly patients and the best surgical treatment strategy remains unclear. Perioperative complications following either a combined anterior and posterior or posterior-only approach are relatively frequent in octogenarians but most of them resolve without further sequelae. Although a high rate of dysphagia occurs in both groups there is a probability of 33% that a PEG tube needs to be placed when using a combined anterior and posterior approach. When performing decompressive surgery for CSM, consideration to correct cervical kyphosis and cervical sagittal imbalance should be taken into account and weighed against the possible associated major complications.
Footnotes
Authors’ Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.