
Abstract
Study Design
Biomechanical Basic Research.
Objectives
Type II Fractures of the dens axis (DFTII) are common fractures of the cervical spine in geriatric patients. A surgical approach is the anterior screw fixation (ASF). However, a disadvantage is the high post-operative rate of non-union. This study aimed to develop and biomechanically test an osteosynthesis plate (OSP) for the anterior treatment of DFTII in comparison to ASF.
Methods
A novel OSP was developed and manufactured. The OSP was biomechanically tested in comparison to ASF in synthetic bone models and geriatric human cadaveric bone. An analysis of the bone microstructure of the human C2 vertebrae was performed utilizing high-resolution quantitative computed tomography to exclude differences in bone quality among the experimental groups. Biomechanical testing was performed by cyclic loading of compression and tensile forces until failure.
Results
In the comparative biomechanical analysis of ASF and OSP in synthetic bone, significant differences were observed regarding the load to failure, favoring the OSP (P = 0.040). The comparative biomechanical analysis of ASF and OSP in the cadaveric specimens also revealed a significantly lower load to failure of the ASF (P = 0.046). The experimental groups did not show significant differences regarding age, sex or bone microstructure.
Conclusions
The current study demonstrated that the OSP is biomechanically superior to the ASF, indicating higher stability. This study provides the basis for an alternative anterior treatment option for DFTII.
Introduction
Fractures of the dens axis (DAX) are the most common fractures of the cervical spine in geriatric patients. Among them, DAX type II fractures according to Anderson and D'Alonzo 1 (DFTII) are particularly frequent.2,3 The incidence is increasing, especially due to the aging population. 4 Geriatric patients often suffer from multiple medical conditions, making their management a significant challenge. Mortality rates are high, ranging from 18-44% at 1 year post trauma.3,5,6 Both conservative and surgical treatment options aim to achieve the following therapeutic goals: restoration of previous mobility, preservation of functionality, pain relief and avoidance of complications. The most appropriate therapeutic approach for these patients is frequently discussed. 7 A comparison of 165 surgically and 157 conservatively treated patients with DFTII, showed a significantly better 30-day survival rate in the surgical group, along with a positive trend towards long-term superiority. 5 Moreover, patients who underwent surgical treatment demonstrated significantly better functional outcomes, as measured by the Neck Disability Index (NDI), compared to conservatively treated patients, and showed lower rates of non-unions. 6
When opting for surgical therapy, various procedures are available. Posterior fusion of C1/C2 yields high fusion rates and can be performed using a screw and rod system according to Goel and Harms et al,8,9 or through a transarticular screw fixation as described by Magerl et al 10 combined with simultaneous fusion according to Gallie. 11 However, both techniques require posterior approaches, which may be associated with increased morbidity due to the extent of the surgical approach harming posterior structures like ligaments and muscles. Minimally invasive procedures without direct osseous fusion between C1 and C2, though, appear to be inferior in terms of fusion rates. 12 Furthermore, all these procedures restrict the rotational capability between C1 and C2, thus impairing functionality.
An alternative to the posterior approach for DFTII and of subtype A or B, according to Eysel and Roosen, 13 is the anterior screw fixation (ASF), according to Böhler et al. 14 The advantages lie in the lower surgical approach morbidity, shorter length of operation, lower blood loss and theoretical preservation of rotation between C1 and C2.15,16 However, a disadvantage is the remaining rate of non-union and implant loosening in geriatric patients.17-19
In the past, several osteosynthesis plates (OSP) have been developed to treat upper cervical spine fractures to achieve more stable osteosyntheses.20-23 However, to our knowledge, none of these OSP has yet been established in clinical practice. We believe that the following features should be considered in the development of a new OSP to facilitate its use: avoiding excessive sagittal profile thickness and the involvement of multiple vertebral bodies, ensuring secure ventral anchoring of the OSP in the corpus axis (CAX), and achieving angular stability. The aim of this study was to develop and biomechanically test a new OSP for the treatment of DFTII, which can be implanted anteriorly via the access for ASF while preserving rotation between C1 and C2, and provide increased stability compared to ASF. The design of the new OSP focused on addressing the afore mentioned plate design problems.
Methods
The present study is a biomechanical study. A novel OSP was developed and manufactured for the treatment of DFTII. Subsequently, the OSP was biomechanically tested in comparison to the conventional ASF using both synthetic bone models as proof of concept (Sawbones USA, Pacific Research Laboratories Inc, Vashon, WA, USA) and geriatric human cadaveric bone. Consent for specimen collection was obtained from the deceased individuals’ relatives. The cadaveric human C2 vertebrae (n = 14) were obtained postmortem during autopsies. The age and sex of the individuals were documented. Only anatomically normal and unaltered C2 vertebrae were included, while exclusion criteria were a history of fractures or surgeries in the cervical spine or tumor diseases. Prior to further analysis, all specimens were anonymized. This study was reported to the ethics committee of the Hamburg Medical Association (2021-300002-WF). Informed consent was waived due to the anonymous character of the study.
Development and Manufacture of the Novel OSP
The new anatomical osteosynthesis plate is instrumented ventrally on the CAX and has a slim design to prevent soft tissue irritation. For increased stability it is anchored with 2 fixed angle screws. A guide cannula for screw insertion is enabling osteosynthesis of a DFTII (Figure 1). 3D model of the novel osteosynthesis plate. The bilateral wings of the plate are depicted, which are instrumented with fixed angle screws. Additionally, the screw guide sleeve for conducting the osteosynthesis is shown.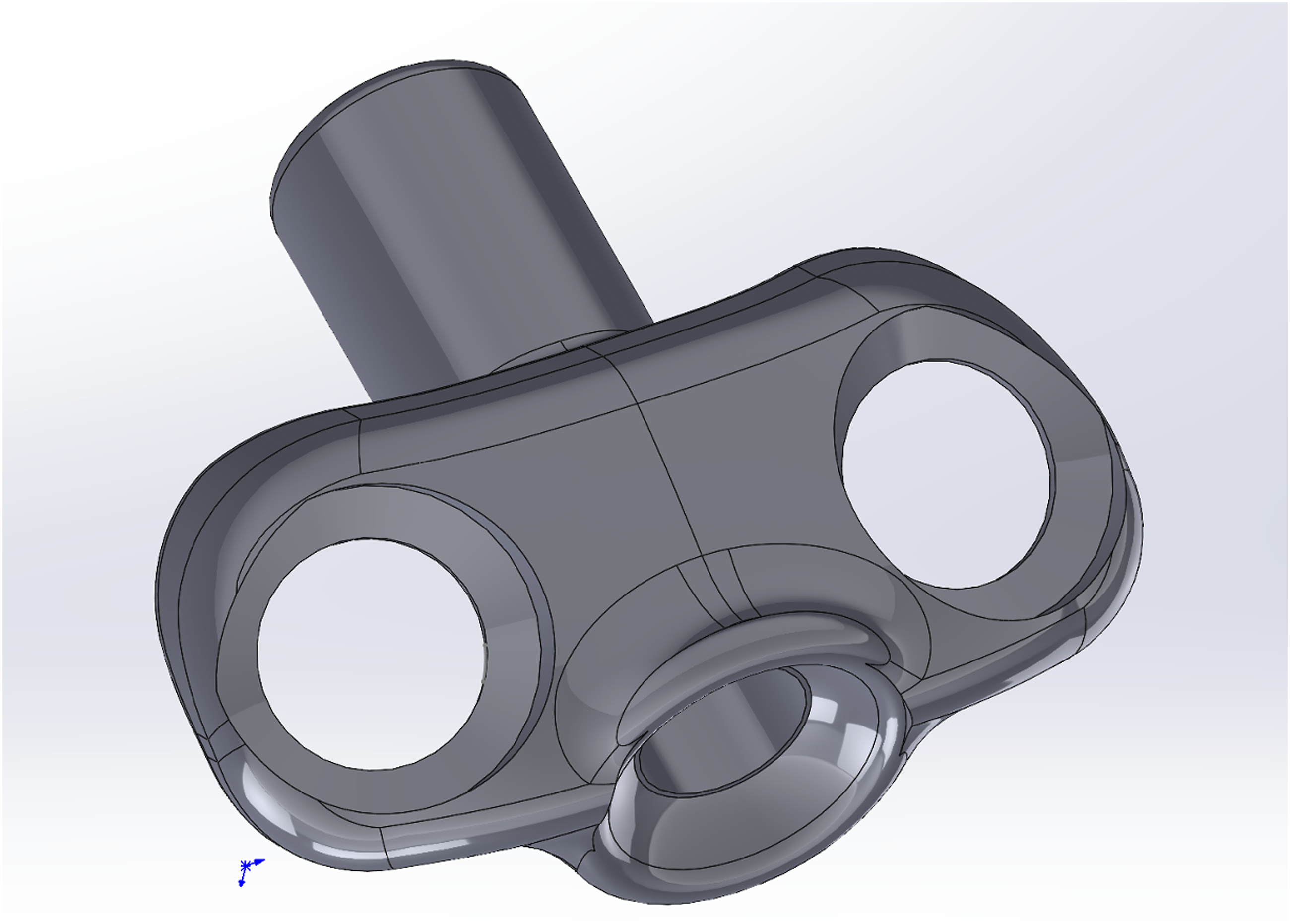
An initial prototype of the plate was produced using modeling clay. Subsequently, the technical design of the plate was developed, and a prototype was created from acrylonitrile-butadiene-styrene copolymer (Alphacam GmbH, Germany) using a 3D printer (Dimension Elite, Stratasys, USA). The original osteosynthesis plate was manufactured using laser rapid manufacturing from commercially pure titanium (∼Titanium Grade 2-3) (Stryker GmbH & Co KG, Germany).
Biomechanical Comparison of ASF and the Novel OSP in Synthetic Bones as Proof of Feasibility
As a proof of concept, comparative biomechanical testing of ASF and the novel OSP was performed in synthetic bone. For this purpose, a DFTII was simulated on artificial bone models of the human axis by performing an osteotomy (n = 8). The osteotomy was conducted as a straight osteotomy, corresponding to a Type A fracture, as classified by Eysel and Roosen. 13 Although ASF is ideally indicated for ventrodorsally descending Type B fractures, a Type A osteotomy was selected in this experimental setting due to its greater reproducibility. Subsequently, osteosynthesis was performed using either the conventional ASF (n = 4) or the new OSP (n = 4).
Insertion of the Classic Anterior Screw
A K-wire was positioned at the entry point of the surgical axis through the DAX in the ventrocaudal cortical bone of the CAX. The K-wire was advanced along the surgical axis through the CAX and across the plane of the osteotomy into the DAX across the cranial tip. After drilling, the 3.5 mm cannulated partially threaded screw (DePuySynthes, Johnson & Johnson Medical GmbH, Germany) was inserted over the K-wire. Achieving a bicortical position of the screw was crucial to achieve a compression of the osteotomy. The screw was tightened until the closing of the osteotomy avoiding overwinding.
Insertion of the Osteosynthesis Plate
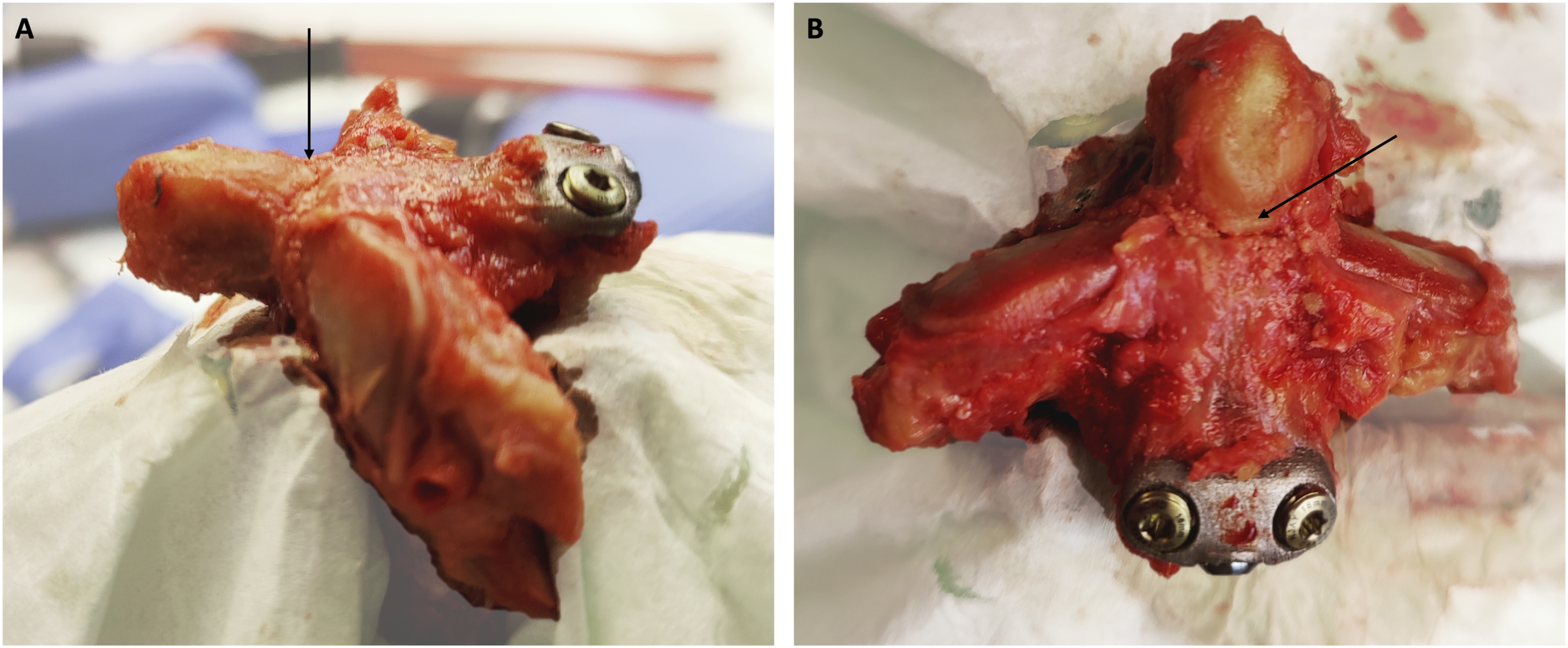
The insertion of the OSP is shown step by step (Figure 2). A K-wire was positioned at the entry point of the CAX. The CAX was reamed over the K-wire to create a channel for the guide cannula of the osteosynthesis plate utilizing a 4 mm canulated drill. The OSP was inserted in the CAX over the K-wire. The bilateral wings of the plate were oriented ventral to the CAX. The 3.5 mm osteosynthesis screw (DePuySynthes, Johnson & Johnson Medical GmbH, Germany) is introduced via the guide cannula. Achieving a bicortical position of the screw is crucial. The osteosynthesis plate was anchored on both sides in the CAX using 4 mm fixed angle screws (Stryker GmbH & Co KG, Germany), tightened with a torque wrench at 2.26 Nm. The osteosynthesis screw was tightened until the closing of the osteotomy avoiding overwinding. The OSP was finally fixed with screws in a cadaveric human C2 vertebra, following an osteotomy corresponding to a DFTII (Figure 3). Schematic representation of the insertion of the osteosynthesis plate (OSP) into the C2 vertebral body. A: Depicted is the material required for OSP implantation. Along with a K-wire, the OSP and a screw for the actual osteosynthesis procedure (3.5 mm, blue screws) are needed, as well as screws for fixed angle anchoring of the plate in the corpus axis (CAX) (4.0 mm, golden screws) (black arrow marking the CAX of the specimen). B: Firstly, a K-wire is placed in a caudoventral to craniodorsal direction across the fracture, along the surgical axis from CAX to the dens Axis (DAX). This is then drilled through with a canulated 4.0 mm drill. C: The OSP is then introduced into the CAX over the K-wire and contoured accordingly. The screw guide sleeve is aligned at the correct angle over the K-wire. D: Next, the cannulated 3.5 mm screw is inserted to carry out the osteosynthesis. It is crucial to exceed the dorsocranial cortex of the DAX, resulting in a bicortical position of the screw. Due to the drilling in the CAX and the guide sleeve, the fully threaded screw functions as a traction screw. E: The ventral cortex of the DAX is then perforated using a sharp awl. F: The ventral wings of the OSP are instrumented using 4.0 mm fixed angle screws. Subsequently, the ventral screws are finally tightened using a torque wrench, followed by compressing the fracture using the traction screw. G: The OSP, fully inserted and fixed with screws, in a lateral view. H: The OSP, fully inserted and fixed with screws, in a ventral view. Osteosynthesis plate (OSP) fixed with screws in a cadaveric human C2 vertebra. (A) Sagittal view. The dens Axis (DAX) is oriented to the left, and the corpus Axis (CAX) is on the right side of the image. The OSP lies ventrally, with a low-profile contour, in close proximity to the CAX and is anchored with fixed angle screws. The black arrow indicates the line of the osteotomy. (B) Frontal view. The DAX is positioned at the top,and the CAX is at the bottom of the image. The OSP was inserted into C2, following an osteotomy corresponding to a Type II fracture of the DAX according to Anderson and D'Alonzo. The black arrow again indicates the osteotomy.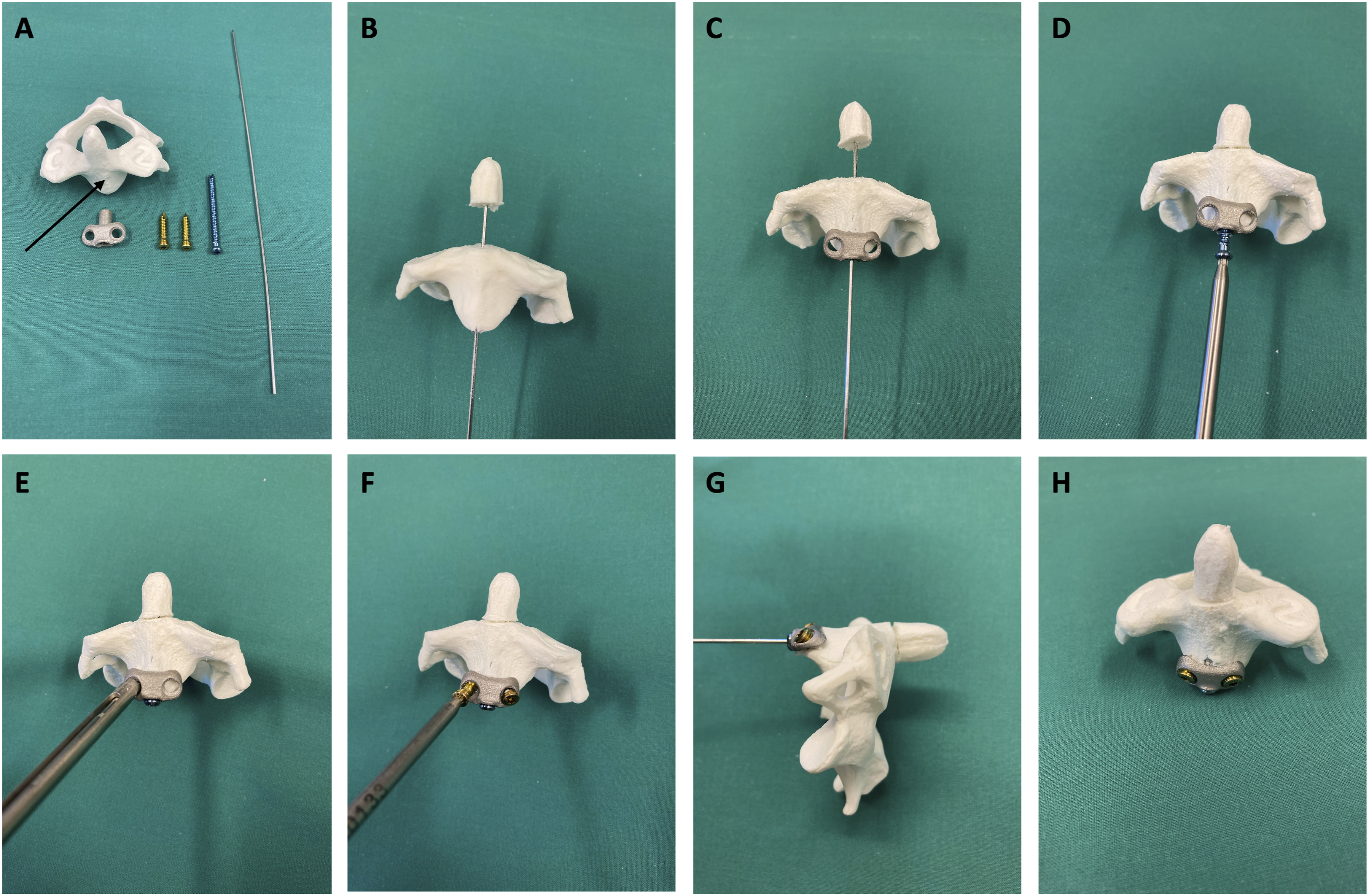
Biomechanical Testing of ASF Compared to the Novel OSP in Synthetic Bones
Dynamic testing was performed using a Sincotec testing machine with pneumatic actuators (Clausthal-Zellerfeld, Germany). A pulsating load for anteroposterior compression and tensile (ie, extension and flexion in the atlantoaxial joint (AAJ)) starting with ±15 N and 5 Hz was applied, rising the amplitude by 10 N every 5000 cycles until failure (load to failure). Osteosynthesis failure in the artificial bone was defined as a displacement of >1 mm during a sequence of 5000 cycles. All superstructures were individually milled from 7075 aluminum and the specimen bodies were cast with the embedding material Technovit 4021 (Kulzer, Hanau, Germany).
Biomechanical Testing of ASF Compared to the Novel OSP in Cadaveric Human C2 Vertebrae
After the feasibility analysis in synthetic bone was completed, the actual biomechanical testing of ASF was conducted in comparison to the novel OSP in human C2 vertebrae. The cadaveric human C2 vertebrae (n = 14) were obtained post mortem during autopsies. The performance of the osteotomy and instrumentation using ASF (n = 7) and OSP (n = 7) were carried out following the same procedures as described above for synthetic bone. The selection of whether instrumentation was done using ASF or OSP was determined by randomization.
Analysis of the Bone Microstructure of Cadaveric Human C2 Vertebrae
As part of a previously published study, the C2 vertebrae were already analyzed regarding their bone microstructure. 24 Fourteen of these C2 vertebrae were randomly selected for the biomechanical analysis presented here. Their osseous structural parameters are shown again, to exclude differences in bone quality among the experimental groups. The fresh-frozen human C2 were scanned and analyzed using a high-resolution second-generation XTremeCT II (Scanco Medical, Switzerland). The samples were scanned with a spatial resolution of 62 μm, and the analysis was conducted using the corresponding software (Scanco Medical, Switzerland). The trabecular bone microarchitecture of the C2 was analyzed, and the following parameters were determined: Bone volume per tissue volume (BV/TV), bone mineral density of the bone volume (BMD of BV, mg HA/cm3), trabecular thickness (Tb.Th, mm), number of trabeculae (Tb.N, 1/mm) and the trabecular separation (Tb.Sp, mm).
Biomechanical Testing in Cadaveric Bones
Dynamic testing was performed using a Sincotec testing machine with pneumatic actuators (Clausthal-Zellerfeld, Germany). A pulsating load for anteroposterior compression and tensile (ie, extension and flexion in the AAJ) starting with ±10 N with 2.5 Hz was applied, rising the load every 5000 cycles with an additional load of 5 N (10 N amplitude) in each direction until failure (load to failure). Osteosynthesis failure in the cadaveric bone was defined as a displacement of >2 mm during a sequence of 5000 cycles.
All superstructures were individually milled from 7075 aluminum and the specimen bodies were cast with the embedding material Technovit 4021 (Kulzer, Hanau, Germany). In Figure 4 the setup for dynamic biomechanical testing in the Sinotec testing machine is presented (Figrue 4). Presentation of the setup for dynamic biomechanical testing in the Sinotec testing machine with pneumatic actuators (Clausthal-Zellerfeld, Germany). (A) Sagittal view. (B) Axial view. (A) pulsating load for compression and tension (ie, extension and flexion in the atlantoaxial joint), starting from −10 N to +10 N at a frequency of 2.5 Hz, was applied to the DAX using an applied clamp, increasing the load every 5000 cycles with an additional load of 5N (10 N amplitude) in each direction until failure.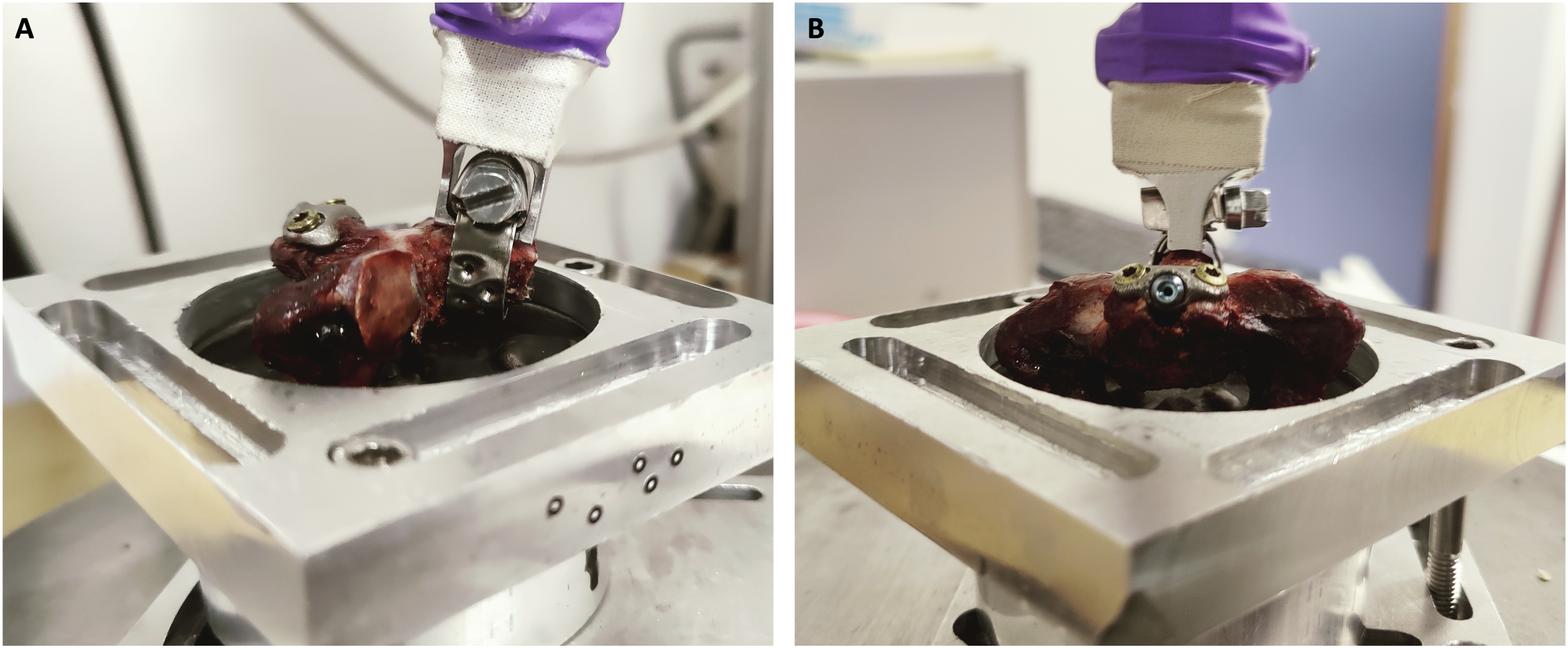
Statistical Analyses
For statistical analysis, the software SigmaPlot 13 (Systat Software Inc, San Jose, CA, USA) was used. All values are given in mean ± standard deviation. The Shapiro-Wilk test was used to test for normal distribution. For group comparisons, 2 tailed t test was performed for parametric and the Mann-Whitney test for non-parametric data. The calculation of effect size was done using Cohen’s d. Values up to 0.2 are considered negligible, 0.2-0.5 indicate a small effect, 0.5-0.8 signify a moderate effect size, and values above 0.8 indicate a strong effect size. Differences in terms of gender distribution were analyzed using Fisher’s exact test. The significance level was set at P < 0.05.
Results
Biomechanical Comparison of ASF and the Novel OSP in Synthetic Bones as Feasibility Analysis
The comparative biomechanical analysis of ASF and OSP in synthetic bone shows a significantly lower load to failure in N of the ASF at a mean of 51.25 ± 7.50 N compared to the OSP at a mean of 68.75 ± 11.09 N (P = 0.0399, d = 1.849) (Figure 5A). A: Presentation of data on the load to failure in artificial bone for anterior screw fixation (ASF) (light grey) and osteosynthesis plate (OSP) (dark grey). There is a significantly lower load to failure in ASF compared to OSP (P = 0.0399, d = 1.849). B: Presentation of data on the load to failure in cadaveric bone for ASF (light grey) and osteosynthesis plate OSP (dark grey). There is a significantly earlier failure of osteosynthesis in ASF compared to OSP (P = 0.0459, d = 1.190). The Y-axes represent the load to failure in Newton (N). The boxes indicate the interquartile range (IQR). Whiskers indicate the minimum and maximum values. The dots represent each individual data point.
Analysis of the Bone Microstructure of Cadaveric Human C2 Vertebrae
Age and Bone Microstructure Parameters of the Experimental Groups ASF and OSP. The Data Presented Here Represent a Subgroup Analysis of Previously Published Data. 24
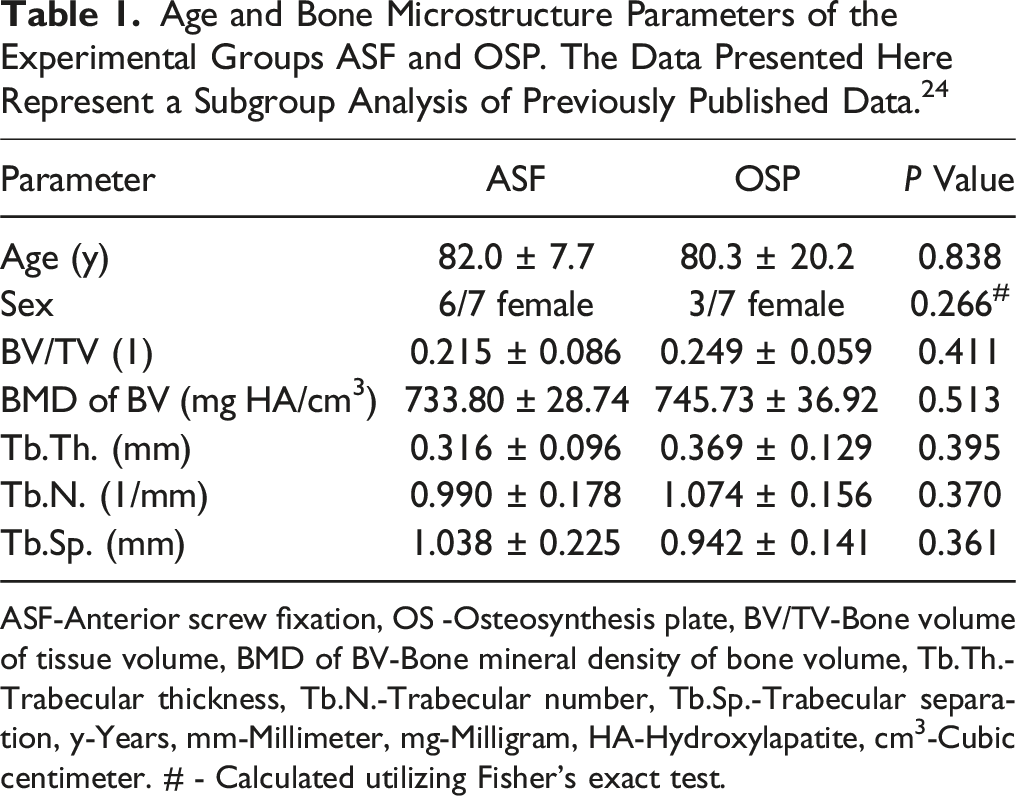
ASF-Anterior screw fixation, OS -Osteosynthesis plate, BV/TV-Bone volume of tissue volume, BMD of BV-Bone mineral density of bone volume, Tb.Th.-Trabecular thickness, Tb.N.-Trabecular number, Tb.Sp.-Trabecular separation, y-Years, mm-Millimeter, mg-Milligram, HA-Hydroxylapatite, cm3-Cubic centimeter. # - Calculated utilizing Fisher’s exact test.
Biomechanical Comparison of ASF and the Novel OSP in Cadaveric Human C2 Vertebrae
The comparative biomechanical analysis of ASF and OSP in human C2 vertebrae also revealed a significantly lower load to failure in N of the ASF at a mean of 42.14 ± 14.68 N compared to the OSP at a mean of 62.86 ± 19.76 N (P = 0.0459, d = 1.190) (Figure 5B).
In the comparative biomechanical analysis of ASF and OSP in geriatric human cadaveric bones, typical osteosynthesis failures were observed (Figure 6). In the case of ASF, osteosynthesis failure typically occurred at the osteotomy site accompanied by ventral cut out of the ASF from the CAX in 3 cases. Conversely, the OSP also exhibited osteosynthesis failure at the osteotomy site, but the OSP remained anchored in the CAX, in all cases. A breakage or deformation of the OSP itself was not observed in any of the cases. Typical failure modes of osteosynthesis with osteosynthesis plate (OSP) and anterior screw fixation (ASF). (A) OSP: Sagittal view. Osteosynthesis failure is evident in the form of displacement at the osteotomy site (indicated by the black arrow). No plate loosening was observed in the corpus axis (CAX). (B) ASF: Sagittal view. Osteosynthesis failure as significant displacement at the osteotomy site and anterior screw cutout from the CAX (indicated by the black arrow).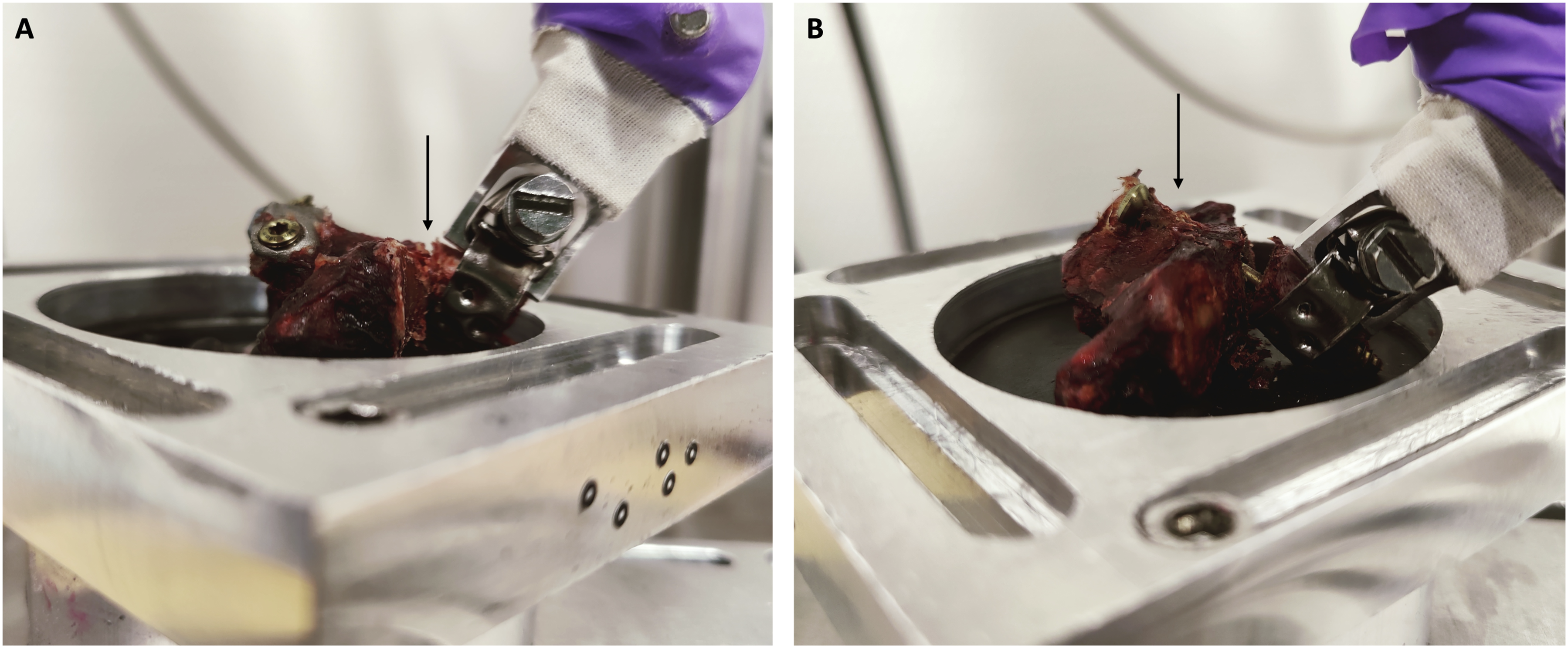
Discussion
Within this study, a novel OSP for the treatment of DFTII was developed and manufactured. Additionally, the OSP was biomechanically compared to the common ASF, in synthetic bone as a proof of concept and subsequently in geriatric human C2 vertebrae, which were acquired post mortem. The current study demonstrated significant biomechanical superiority of the newly designed OSP compared to standard ASF in terms of load to failure, indicating higher stability. The data indicate high effect sizes.
The experimental human cadaveric groups deliberately included geriatric individuals with no significant differences in age, sex or bone quality between the groups, making them comparable. These individuals correspond to a clinically relevant geriatric cohort with a high risk of compromised bone quality due to advanced age and osteoporosis.2,4,25
It was observed that there is a reduced bone microstructure specifically in the region of the base of the DAX and the CAX in comparison to the tip of the DAX.25-27 A previous analysis of the bone microstructure of the axis in geriatric patients demonstrated a decrease in cortical and trabecular bone microstructure from the apex of the DAX to the base of the CAX that could contribute to material loosening following ASF in the region of the base of the DAX and CAX. 24
Therefore, the recent OSP is fixed angle by design and firmly anchored in the CAX region, effectively countering a ventral screw cut out in the CAX and the base of the DAX from our clinical and biomechanical perspective. In the biomechanical testing, we observed that in cases of ASF failure, besides dislocation at the level of the osteotomy, there was typically a ventral cut-out of the screw from the CAX. This phenomenon was generally not observed with OSP.
Due to the atlantoaxial anatomy, with the atlas arch located anteriorly to the tip of the DAX and the ligamentum transversum positioned dorsally, additional stabilization of osteosynthesis in DFTII against anteroposterior compressive and tensile forces (ie, extension and flexion in the AAJ) appears necessary. This requirement is also achieved through the anterior fixation of the OSP in the CAX. In the current study, the ASF and OSP were loaded with such anteroposterior compressive and tensile forces as described above, as they represent a relevant loading momentum for the osteosynthesis. However, rotational forces in the AAJ are also relevant loads on osteosyntheses. In this study, rotational stability was initially not tested in order not to further limit the group size and, thus, the robustness of the data. The analysis of rotational movements in the AAJ should be the subject of further studies. Furthermore, the current study compared the OSP against a single screw for ASF. Studies have shown that the use of 2 screws for ASF is associated with increased stability. 28 However, there is also data showing that, particularly in geriatric patients, as in the current study, the use of 2 screws is associated with higher failure rates. 29 As with rotational stability, this work focused on testing a single procedure against the OSP to maximize group strengths. However, testing the OSP against 2 screws for ASF as well as against other osteosynthesis techniques, such as augmented screws for ASF 30 appears interesting and should also be addressed in follow-up work based on the current data.
Considering the current knowledge about the geriatric patient population, the ASF is not the method of choice worldwide,15,17,18 favoring dorsal fusion of C1/C2 to be considered the preferred approach. 15
However, the data of this study have clinical relevance as, there are patients for whom dorsal fusion is not suitable due to increased surgical trauma or the need for prone positioning in the Mayfield clamp. In such cases, the OSP could offer an alternative, particularly for specific fracture morphologies. The OSP could be a viable option for geriatric patients with DFTII according to the Anderson and D’Alonzo classification 1 and subtype A or B according to Eysel and Roosen, 13 who also have an increased perioperative risk with posterior procedures or have a strong desire to preserve rotation in C1/C2. However, an essential aspect is that implanting the OSP might also increase access morbidity compared to a classic ASF. Although the OSP is designed to be inserted via a classic atraumatic approach to the ventral cervical spine, it certainly requires more space for implantation than a screw for ASF alone. Furthermore, these can also be inserted percutaneously,31,32 which would not be possible with the OSP. Complications such as dysphagia could occur more frequently with OSP compared to ASF. Due to the experimental status of the OSP procedure presented here, there is currently no available data to quantify the risk of dysphagia associated with this implant. Clinical studies would be required to evaluate this aspect.
A limitation of this study is the solely geriatric population tested, so no statement can be made about younger individuals. However, this was intended, as the geriatric collective corresponds to the clinical target collective. A further limitation of this study is the relatively small sample size, with only 7 specimens per group. A larger sample size would enhance the robustness and generalizability of the results. However, the availability of anatomical specimens is inherently restricted. Furthermore, a potential limitation is the exclusive focus on Type II A fractures without further subdivision into Type II A, II B, and II C fractures. While investigating additional subgroups, particularly Type II B fractures, would provide clinically relevant insights, dividing the already limited sample size could compromise statistical power. Furthermore, the study only assessed flexion and extension movements without considering rotational stability and compared the OSP solely to single-screw anterior screw fixation (ASF). Future studies should evaluate the biomechanical properties of the OSP across different fracture and fixation subtypes and movement patterns to better define its potential advantages over conventional screw fixation. Another limitation is that the OSP was only examined biomechanically in comparison to the ASF and not in comparison to the dorsal fusion of C1 and C2. Since the real alternative for geriatric patients is not the ASF but the dorsal fusion, a comparative analysis should ideally be conducted. However, directly comparing the biomechanics of the OSP with the dorsal fusion of C1/C2 seems of little scientific value due to their markedly different features. A sensible approach for a comparative analysis would be to implant the OSP in a clinical geriatric patient population with DFTIIA or DFTIIB as part of a prospective controlled randomized study, comparing it with the dorsal C1/2 fusion in terms of stability, fusion and patient reported outcome measures.
Conclusion
The novel OSP biomechanically surpasses the common ASF for stabilizing DFTII in synthetic bone and geriatric human C2 vertebrae. It has the potential to serve as an alternative anterior treatment option for DFTII in daily use. Before, the clinical benefits and feasibility need to be investigated in the context of a prospective controlled and randomized trial.
Footnotes
Acknowledgments
We thank Stryker GmbH & Co KG, Germany for their support in the manufacturing of the OSP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.