
Abstract
Study Design
Retrospective Review of a National Database.
Introduction
By utilizing a national database, this study aims to quantify the predictors of 30-day mortality after odontoid fixation and guide appropriate management for patients in whom the choice between operative and non-operative management is unclear.
Methods
The American College of Surgeons National Surgical Quality Improvement Database was queried using Current Procedural Terminology (CPT) codes and International Classification of Disease (ICD) codes to identify patients 60 or older who underwent surgical fixation of an odontoid fracture from 2005 to 2020. Risk factors for mortality significant in univariate and subsequent multivariate analysis were used to develop a scoring system to predict post-operative mortality.
Results
608 patients were identified. Patients were split into a non-mortality 30 days post-op group, and into a mortality 30 days post-op group. The following risk factors were included in the scoring system: functional dependency, disseminated cancer, albumin less than 3.5, WBC count greater than 16 k, anterior surgical approach, and pre-op SIRS. Using a cutoff value of 2, the CAAD-16 score had a sensitivity and specificity of 82% and 81%, respectively. The ASA score, cutoff at 4, showed a sensitivity and specificity of 64% and 75% respectively.
Conclusions
This sample of 294 patients represents one of the largest samples of odontoid fracture fixation patients available in the literature and comes from a nationally representative database. We structure relevant risk factors into the CAADS-16 score, which has the potential to be a clinically relevant tool to prevent short-term postoperative mortality.
Introduction
In the United States, the elderly population is the fastest growing demographic, estimated to double by 2050. 1 In patients over the age of 65, the prevalence of upper cervical spine fractures is between 2.4% and 4.7%.2,3 A study has shown that the rate of odontoid fractures in the geriatric population is rising exponentially causing an increasing need for clear treatment algorithms. 4 Odontoid fractures are one of the most common upper cervical spine fractures in elderly patients and the most common fracture of the C2 vertebra. 5 They represent about 10%–20% of all cervical fractures, and of these fractures, 60% can be classified as Type II.6,7 In addition, 62.0% to 68.9% of these cervical spine injuries occur due to low energy falls from a standing position.8,9 Costs associated with inpatient management of odontoid fractures is estimated to be approximately $1.5 billion 10 ; therefore, there is considerable importance in optimizing management strategies from a value-based perspective.
While type I odontoid fractures are generally treated non-operatively, the decision-making process for the optimal treatment strategy in type II is far more complex. Associated factors including additional injuries, medical comorbidities, non-union risk factors and even patient preference are part of the decision process. 11 Distinguishing between patients who would do well with surgical treatment without an unacceptably high risk of mortality from those patients who would not is imperative to achieving the best outcomes.
Although there have been several studies evaluating postoperative mortality following odontoid fractures in elderly patients, there is currently no risk stratification system for predicting mortality after operative treatment. By utilizing a national database, this study aims to quantify the predictors of 30-day mortality after odontoid fixation and guide appropriate management for patients in whom the choice between operative and non-operative management is unclear.
Methods
The ACS NSQIP database was queried for all patients undergoing surgical fixation for odontoid fractures from 2006 to 2020. The database contains prospectively collected demographic and preoperative information, as well as 30-day postoperative outcomes for randomly selected patients at participating sites. Trained clinical reviewers input all data, and routine data audits are performed to maintain accuracy. Furthermore, quality-overall disagreement rates were reported as 2% in 2020. 12 Patients with a diagnosis of odontoid fracture were queried using both International Classification of Diseases (ICD) 9th and 10th edition diagnosis codes in addition to Common Procedural Terminology (CPT) codes (Supplemental Table 1) to better ensure that patients with multiple secondary diagnoses or procedures were not mistakenly included. In addition, only patients over 60 years of age were included to more accurately reflect the population in which the mortality prediction tool would be most useful. Patients with any missing data elements were excluded from final multivariate analysis. In addition, any variables with less than 10 total observations were also excluded from multivariate analysis.
Potential risk factors for mortality based on previous literature and univariate analysis were selected and included in univariate analysis. Mortality was calculated using the variable “yrdeath.” Anemia was calculated using preoperative hematocrit, under 39% for men and 36% for women. Hypoalbuminemia or malnutrition was calculated using preoperative albumin less than 3.5 mg/dL.
Using R statistical software (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/), all included cases were subject to descriptive statistics and univariate analysis. Shapiro-Wilk tests were conducted to assess normality of data. If data was normal, two-sample Student t-tests were utilized. If data was not normal, Mann-Whitney U test was utilized. Fisher’s exact test was used to compare categorial variables when categories had five or fewer occurrences, while chi-squared was utilized when categories had greater than five occurrences. Multicollinearity was estimated using the variance inflation factor (VIF) with a threshold of 5 45. All factors found to be significant (P < .05) on univariate analysis were assessed via bivariate analysis. All variable significant in bivariate analysis (P < .05) were included a multivariable logistic regression model to build a risk estimating equation (REE), which was used to calculate predicted probability of 30-day mortality. A receiver operating curve (ROC) was generated, and analysis conducted to calculate the area under the curve (AUC) using the trapezoid rule. 13 The Hosmer-Lemeshow test was used to assess goodness of fit.
The CAADS-16 score was derived as a practical tool for patients who are in consideration for operative fixation for odontoid fractures. CAADS-16 is an acronym: cancer, albumin less than 3.5, anterior surgical approach, functional dependency, pre-op SIRS, and WBC greater than 16k. For reference, the current study compared the CAADS-16 score to the American Society of Anesthesiologists (ASA) physical status classification score in its ability to accurately predict 30-day mortality. Significance was set at P < .05 for all statistical analyses.
This study did was exempt for IRB approval due to it utilizing a deidentified national database. This study also did not require consenting patients due to utilizing an available database.
Results
Cohort Characteristics and Univariate Analysis
Characteristics of the Full Cohort.
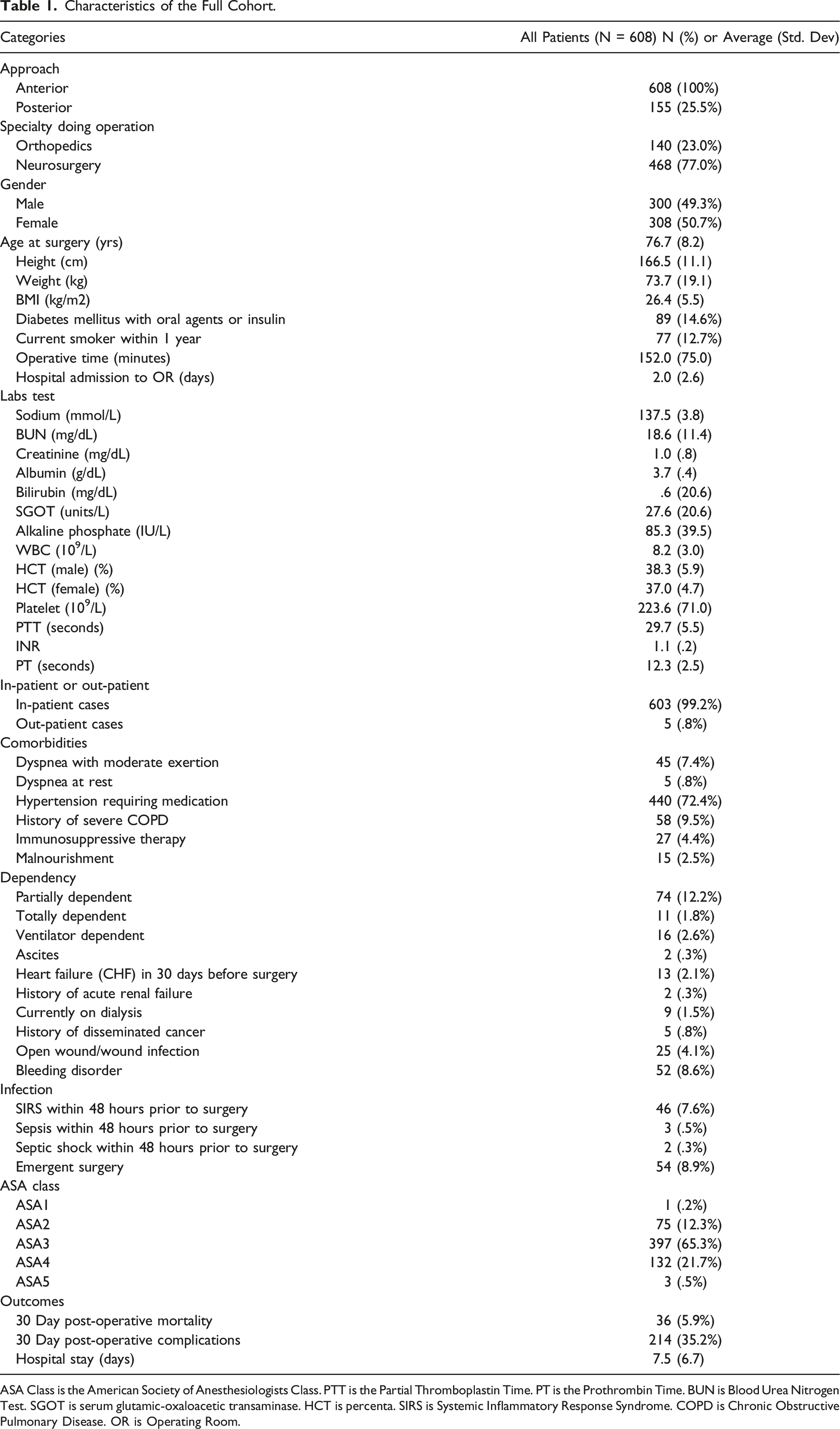
ASA Class is the American Society of Anesthesiologists Class. PTT is the Partial Thromboplastin Time. PT is the Prothrombin Time. BUN is Blood Urea Nitrogen Test. SGOT is serum glutamic-oxaloacetic transaminase. HCT is percenta. SIRS is Systemic Inflammatory Response Syndrome. COPD is Chronic Obstructive Pulmonary Disease. OR is Operating Room.
Comparison of Patients Who Suffered Mortality and Those Who Did Not.
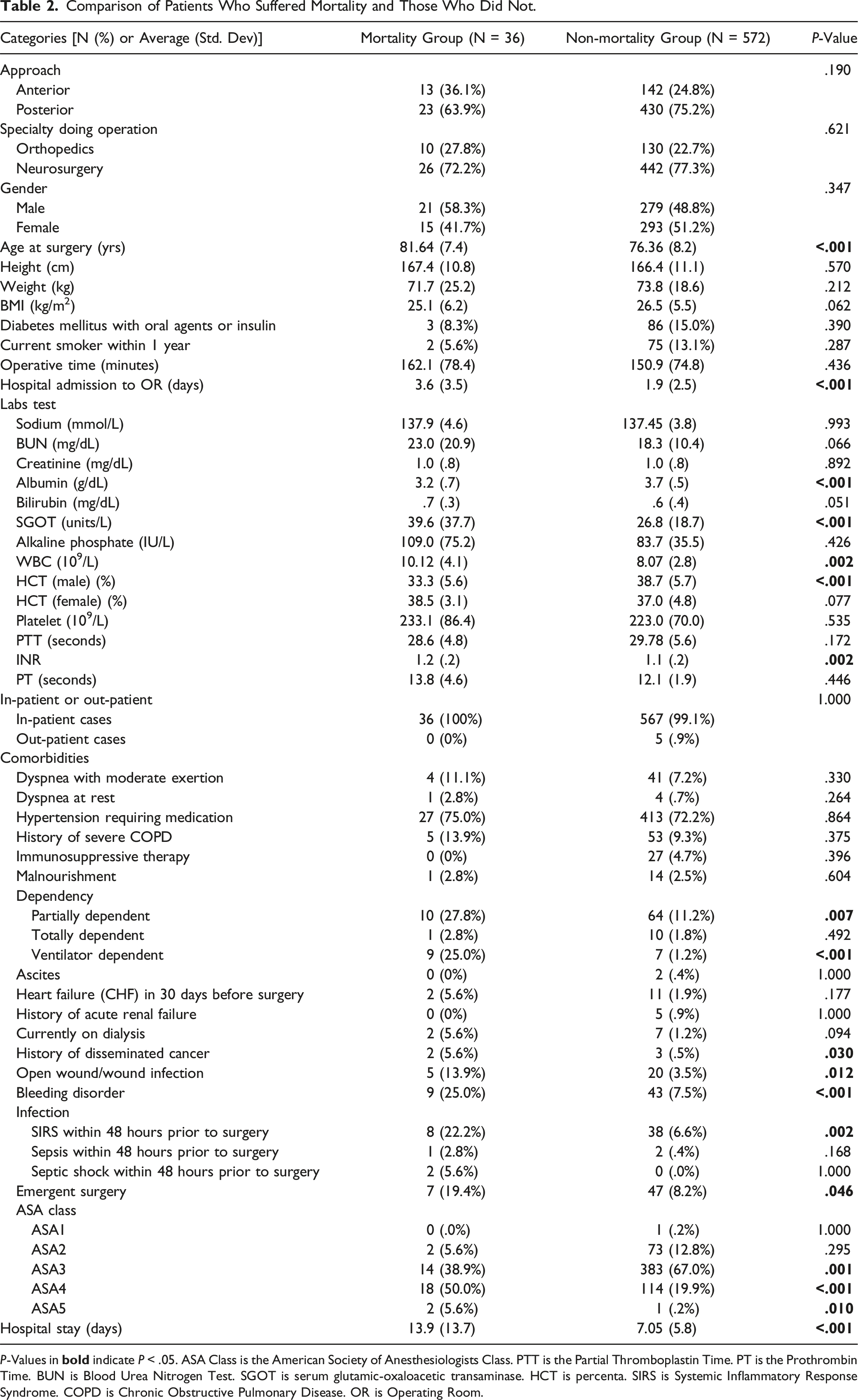
P-Values in
Multivariable Analysis and Risk Model Development
These were the following variables included in the multivariable regression: anterior vs posterior approach, specialty (orthopedic vs neurosurgery), sex, age greater than 75 years, BMI, albumin levels less than 3.5 g/dL, white blood cell count greater than 12000 per microliter, HCT levels less than 38% for males and less than 35% for females, INR greater than 1, hypertension, functional dependency, dialysis, cancer, bleeding disorders, presence of preop SIRS, and length of time from admission to surgery greater than 2 days. Patients that did not have complete data for any of the previously mentioned variables were excluded. This left 294 patients for the multivariate analysis.
Bivariate and Multivariate Logistic Regression With Significant Variables From Univariate Analysis.
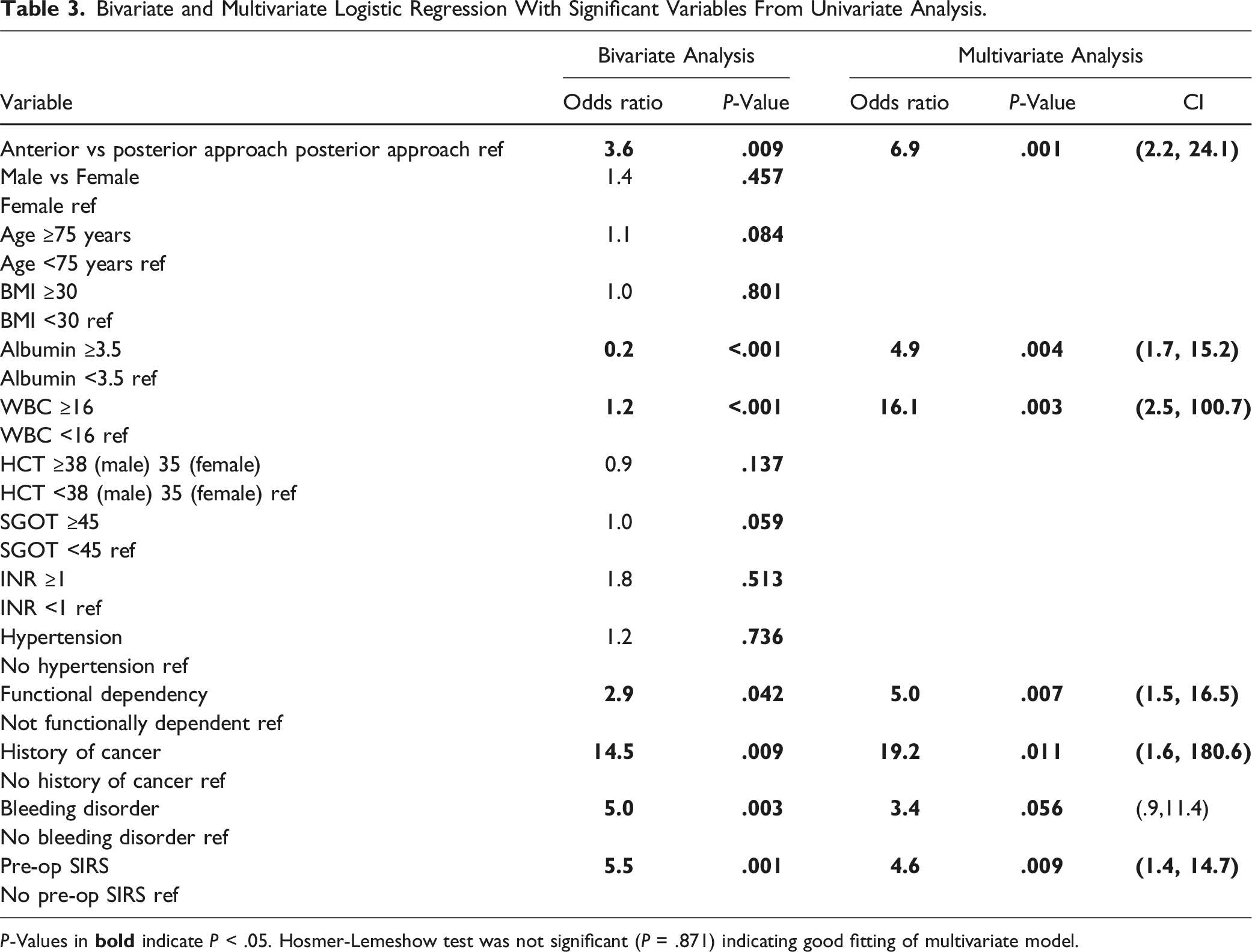
P-Values in
Creation of CAADS-16 Score
Using the previously outlined risk factors, the CAADS-16 score was developed. A single point was assigned for the presence of each factor, with a range of possible scores from 0 to 6. In the current sample, 119 patients had a score of 0, 106 had a score of 1, 62 had a score of 2, and 7 patient had a score of 3. No patients in our sample had scores of 4 or 5 or 6. Risk of mortality increased with higher scores; for a score of 0, 1, 2, and 3, observed mortality rates were 1.7%, 1.9%, 21.0%, and 71.4%, respectively (Figure 1). The AUC using the CAADS-16 score was .84. Using a cutoff value of 2 as a positive result, the CAADS-16 score has a sensitivity of 82% and a specificity of 81% (Figure 2). This was the cut-off value with the greatest sum of sensitivity and specificity, which also maximizes both these values. Box and whisker plot for each available CAADS-16 score in our cohort 165 x 103 mm (400 x 400 DPI). ROC curves for CAADS-16 score and ASA classification. The AUC is displayed in the legend, and the cut off values are represented in the squares of the curve. The ASA classification was cut off as 4 and the CAADS-16 score was cutoff at 2, chosen as the optimal cut offs for sensitivity and specificity.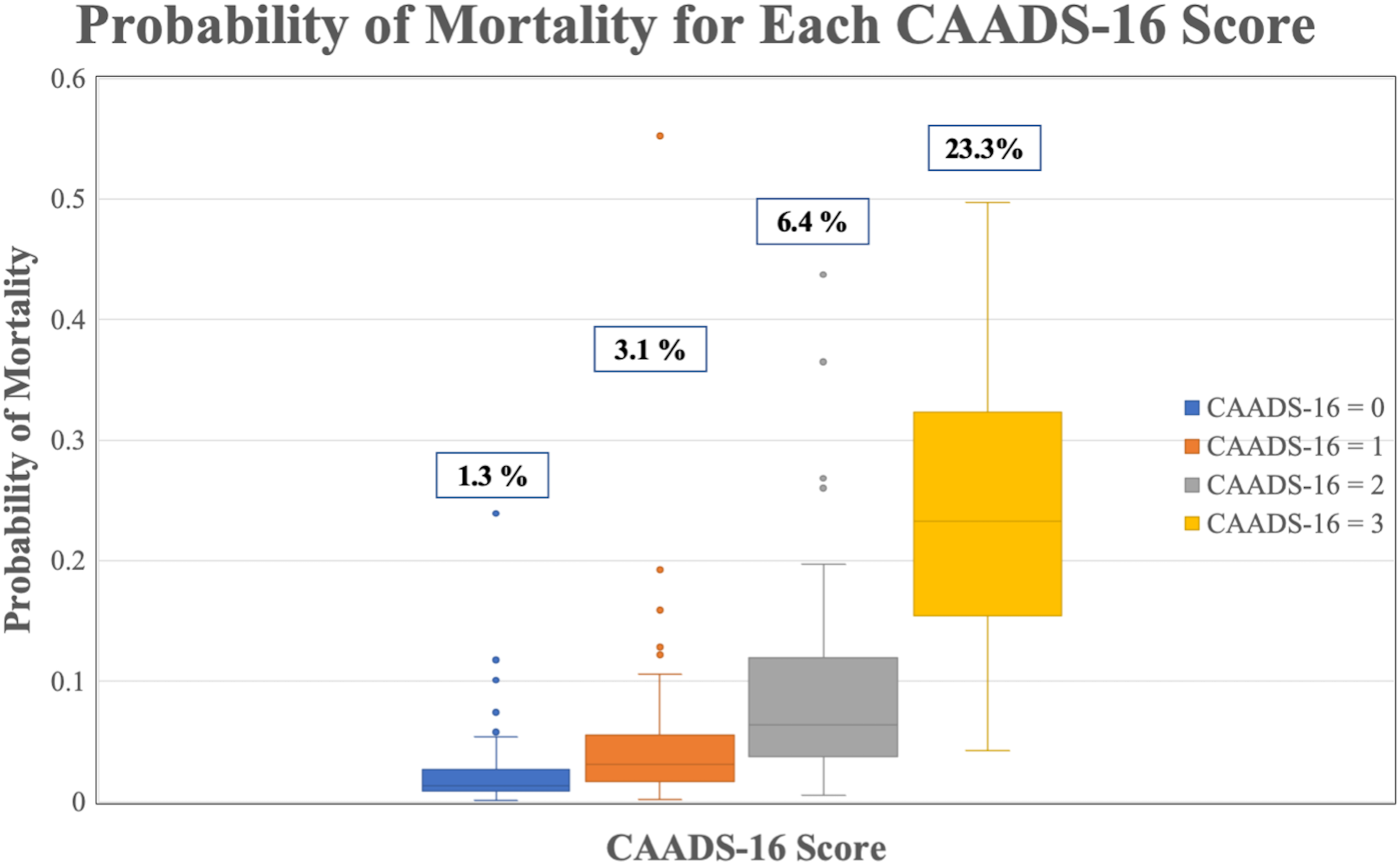
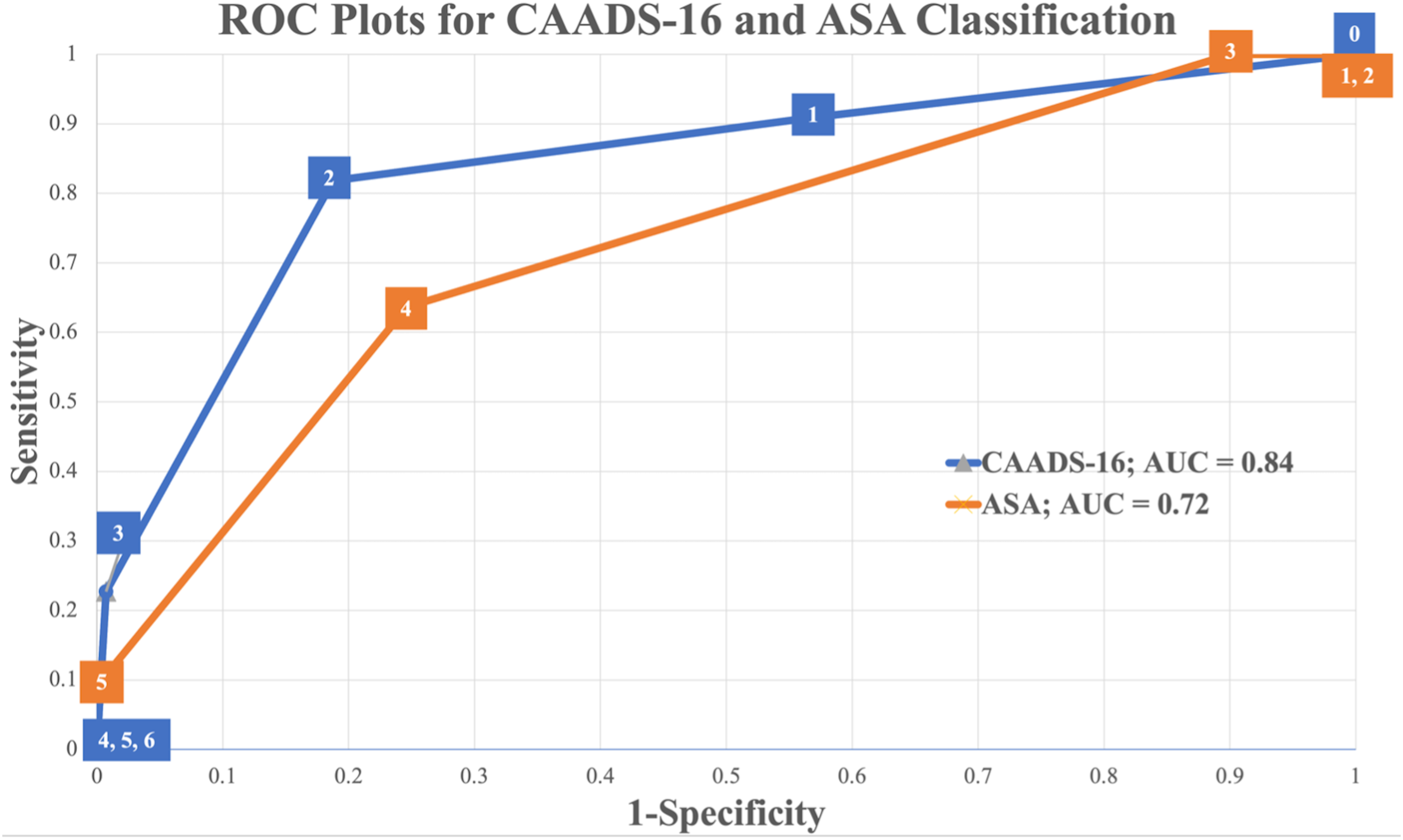
Doing a similar analysis on the ASA classification the following was found. In the current sample, 0 patients had an ASA score of 1, 27 had an ASA score of 2, 186 had an ASA score of 3, 79 patients had an ASA score of 4, and 2 patients had an ASA score of 5. Risk of mortality increased with higher scores; for a score of 2, 3, 4, and 5 observed mortality rates were 0%, 4.3%, 15.2%, and 100%, respectively. The AUC using the AUC score was .72. Using a cutoff value of 4 as a positive result, the ASA score has a sensitivity of 64% and a specificity of 75% (Figure 2).
Discussion
In our study, we created the CAADS-16 score, to help predict 30-day mortality after odontoid fracture fixation in elderly patients. This tool will help physicians guide appropriate management for patients where the choice between operative treatment and non-operative treatment remains unclear. The ASA classification is a risk classification that has seen widespread use. But the agreement between surgeon judgements and the ASA physical status classification is lacking, especially between different specialties. 14
The CAADS-16 score demonstrated an AUC of .84. Additionally, it performed better than the ASA classification, a commonly used classification system, to assess preoperative risk, is more focused toward mortality, and does not rely on subjective clinical assessment for any of its parameters.
A necessary criterion for the implementation of a new system is its ease of use in clinical practice. 15 Regarding its practicality, the CAADS-16 score is relatively simple to implement and can be recorded accurately with minimal training. The simplicity of the components, with values of one for each risk factor, allows for ease of use which is a clear advantage in clinical situations where time and efficiency are paramount. The most appropriate use of the CAADS-16 score is to identify patients at high risk for mortality before surgery, allowing management to be tailored accordingly if necessary. It also provides a quantitative description of 30-day mortality, which can also be used to counsel patients and give them better insight into their given course of treatment.
Disseminated cancer has been previously described as a significant risk factor for surgical morbidity and mortality in various types of surgery for odontoid fractures.16,17 In one such paper, patients receiving surgery for malignancy resection with a previous diagnosis of disseminated malignancy had 30-day mortality rates ranging from 33.7% to 26.6%, with variation based on year of surgery. 18 In another study, patients with cancer had increased odds of mortality and morbidity compared to those without, with OR 3.32 (2.87-3.85) for mortality, and 1.28 (1.19-1.38) for morbidity as defined by the presence of any 30-day medical complication, readmission, or unplanned reoperation. 19
Similarly, hypoalbuminemia has been cited as an independent risk factor for morality in various surgical specialties.20-25 Finally, leukocytosis has also been investigated as an independent risk factor for postoperative complications. In patients receiving surgery for Stanford Type A aortic dissections, patients with WBC above 11k had significantly higher rates of mortality compared to those who did not -20.9% vs 8.1% (P = .001). 25 Other studies have observed similar relationships between increasing WBC count and risk of in-hospital mortality among patients with acute MI undergoing coronary artery bypass grafting. 26 There is, however, considerable conflicting evidence regarding the prognostic value of elevated WBC and mortality. 27 For example, among approximately 11,000 cardiac surgery patients, elevated WBC above 11k was associated with increased risk of infectious complications, but not mortality. 28 Given the inconclusive nature of the relationship between leukocytosis and mortality in the literature, it should be noted that the current study used a higher threshold WBC value of 16k as opposed to the more typical 11k upper range on most WBC assays. This may explain why elevated WBC was found to be significant in the current results and may be a topic for further investigation in future studies.
Functional dependency has been frequently cited as a predictor of mortality as well.29-31 It is likely that functional status is a surrogate for a patient’s overall frailty/fragility, which has also been assessed as a factor positively correlated with postoperative mortality. 32 Functional dependency has also been associated with increased post-operative morbidity and mortality in patients undergoing surgery for hip fracture. 33 Although this factor may be more difficult to objectively assess than presence of cancer, decreased albumin, 34 or elevated WBC count, it nevertheless represents an important prognostic factor in the CAADS-16 score, and may still be obtained with relative ease through history taking methods either from the patient, or from a designated caregiver.
Finally, anterior surgical approach for odontoid fracture fixation was also identified as a significant risk factor for 30-day mortality and included in the CAADS-16 score. This has previously been previously demonstrated in the literature. 35 Rates in the literature for 30-day overall mortality following odontoid fracture fixation with any technique range from 4% to 19.2% comparable to our own overall mortality rate of 7.8%.35-37 In addition, 30-day mortality for patients undergoing anterior odontoid fixation has been reported in a previous systematic review from White et al to be 7% based on 4 prior studies.38-42 Our own observed rate was 15.6%, which was higher than previously reported - the current study also encompassed a larger range of years and a larger sample size (294 in the current study vs 134 in White et al). While the precise reason for our higher observed 30-day mortality with anterior compared to posterior fixation is not entirely clear from the present results, it is in-line with prior expert recommendations regarding odontoid fracture fixation in the elderly.43,44 These reviews recommend posterior C1-2 fixation for unstable fractures, and hard cervical collar or cervicothoracic bracing for stable fracture patterns. The current findings support these recommendations.
This study has several limitations. While CPT codes provide a codified way to identify procedures, the use of CPT codes may vary by surgeon and may not be fully representative of the procedure. We attempted to mitigate this by combining with ICD 9 and ICD 10 codes to choose cases more accurately. Due to the nature of ICD 9 and 10 codes, it was not possible to capture exact fracture patterns for all years of the included study - in particular, ICD 9 codes do not differentiate between Type I, II and III fracture patterns. ICD 10 codes do make this distinction and were tailored accordingly to capture only Type II fractures. Although operative management for Type I and Type III odontoid fractures is relatively rare, the potential inclusion of patients with these fracture patterns may impact results. Additionally, as this was a study utilizing a national database, it is susceptible to any inherent coding errors or inaccuracies present in the database itself. Furthermore, our study is retrospective and therefore subject to potential biases and confounding factors. For example, albumin levels could have only been obtained for patients who the operating surgeon suspected to be at a higher risk. Finally, due to the relatively small sample size and difficulty in identifying relevant risk factors in other databases that lack direct laboratory values such as NSQIP, it was not practical to externally validate the CAADS-16 score. In the future, external validation would be an important step in ensuring the generalizability of the CAADS-16 score to the patient population of interest. In addition, there were only 36 cases of mortality in this cohort. Due to this, our model could be subject to overfitting due to the number of covariates we utilized. We attempted to minimize for this by filtering by significant univariate parameters, then significant bivariate parameters. A large population is necessary for validation of these results, which can be done as more years of the NSQIP database are available. This would work to narrow the confidence intervals of our predictor variables.
Despite these limitations, the current study provides valuable insight into the risk factors for short-term mortality following odontoid fracture fixation. To our knowledge, this sample of 294 patients represents one of the largest samples of odontoid fracture fixation patients available in the literature and comes from a nationally representative database. Finally, we not only present the relative risk factors, but also structure them into the CAADS-16 score, which has the potential to be a clinically relevant tool for spine surgeons to prevent short-term postoperative mortality.
Conclusion
The CAADS-16 score is a simple and effective tool that can be used to identify patients at high risk of 30-day mortality following odontoid fracture fixation and can aid in the decision between operative and non-operative modalities. We believe that this score has the potential to improve clinical decision-making and patient outcomes in this patient population. However, further studies are needed to confirm the validity and generalizability of our findings.
Supplemental Material
Supplemental Material - Predicting Mortality Following Odontoid Fracture Fixation in Elderly Patients: CAADS-16 Score
Supplemental Material for Predicting Mortality Following Odontoid Fracture Fixation in Elderly Patients: CAADS-16 Score by William ElNemer, Eric Solomon, Michael Raad, Amit Jain, and Sang Hun Lee in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Permission
No copyrighted material used. AJ; Globus Medical: Paid consultant. Stryker: Paid consultant. DePuy, A Johnson and Johnson Company: Paid consultant. SL; Medtronic: Paid consultant; Paid presenter or speaker.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.