
Abstract
Study Design
Delphi survey.
Objectives
To obtain an expert consensus on various dilemmas in the surgical treatment of adult spinal tuberculosis (TB) patients.
Methods
Stage I included a literature review, stage II the identification of 40 Key Opinion leaders (KOLs) and a set of 46 questions, stage III included analysis of 3 rounds of the Delphi survey, and stage IV had final analysis and recommendations. For each question, the level of agreement needed to reach a consensus was set at greater than or equal to 70.0%.
Results
The first and second Delphi survey rounds received 62 and 58 responses, respectively, with 16 questions having more than 70% and two questions having 100% agreement in the first stage. The second stage saw a 70% agreement on six questions. Thus, a consensus was obtained on 22 questions. The recommendations that emerged were as follows: neurodeficit with corresponding radiology and neurological deficit appearing/deteriorating while on anti-tubercular chemotherapy(ATT) are absolute indications for surgery, duration of ATT before neurological deterioration need not be considered, epidural abscess does not need decompression unless concordant clinical neurological findings are present, pain not responding to medical management is not a surgical indication, active pulmonary TB, drug-resistant TB, and tubercular sacroiliitis are not considered as surgical indications, and hemoglobin and other health markers have little contribution to surgical indications.
Conclusion
In order to resolve several conundrums in the surgical treatment of adult spinal TB, this Delphi survey is the first to achieve a national consensus from spine experts. The final recommendations cover the serological, radiographic, and clinical aspects of spinal TB.
Introduction
Tuberculosis (TB) of the spine remains an important pathology affecting patients globally. The disease burden is not restricted to underprivileged populations or any particular geographical region. The spine is affected in 50% of cases of extrapulmonary TB, 1 which constituted 16% of patients of TB screened by WHO in 2017. 2 The pathophysiology has been well documented, and the diagnostic workup well established, with biopsy being the gold standard. Adjuvant modalities like MRI, GeneXpert (Cartridge-based nucleic acid amplification test - CBNAAT), and AFB culture provide diagnostic support. The treatment is essentially medical, comprising of anti-microbial chemotherapy with surgery offered to selected patients. 3
While pediatric TB spine patients form a completely different group with the additional challenges of growth of the spine and rapid destruction of vertebrae leading to major deformities, the adult population needs specific guidelines for surgical treatment. Cord compression of up to 76% of canal encroachment might not always lead to clinical neurological involvement, 4 and the latter per se might not be the sole criteria of early surgery. 5 Radiological criteria to define the extent of bone destruction, the degree of kyphosis, the severity of canal compromise, etc., as well as clinical criteria to define the degree of neurological compromise, the severity of pain, or mechanical instability, may all be considered individually or collectively to define surgical indications in TB spine cases. Surgery may also be indicated for the correction of deformity, which has been tackled differently for active and healed disease, and identifying the instability score in TB spine 6 might be relevant. Similarly, acute, active spinal tuberculosis needs to be treated differently from residual tubercular lesions in the spine.
The existing lack of consensus and individual preferences lead to the requirement for the development of guidelines for surgical indications for adult patients with TB spine. Such a consensus can be obtained through a Delphi-based approach involving experts with substantial experience in treating such patients and with significant contributions to the existing literature on this issue. Our survey aimed to develop a national consensus through a Delphi survey on the indications of surgery in biopsy-proven active adult tuberculosis of the spine.
Materials and Methods
The Delphi-based study was developed in 4 stages after IRB approval (Reference number ASSI/2021/007) through the Research Committee of the Association of Spine Surgeons of India (ASSI).
Stage I – Literature Review and Preparation of a Preliminary Questionnaire
At the very outset, the principal investigator (PI) and his colleagues did a literature survey, and 5671 studies were picked up, then shortlisted to 298 articles. Based on these papers, a series of questions were prepared to address surgical indications in adult spine TB. A flowchart describing how studies were included in the review in accordance with the PRISMA standards is depicted in Figure 1. Articles were located using Google Scholar, Elsevier Springer Link, PubMed, Cochrane Library, and Embase databases. Studies on pediatric patients, patients with residual disease, and patients with deformities secondary to healed tuberculosis were excluded. Flowchart detailing the inclusion of studies in the review for the formulation of questions as per the PRISMA guidelines.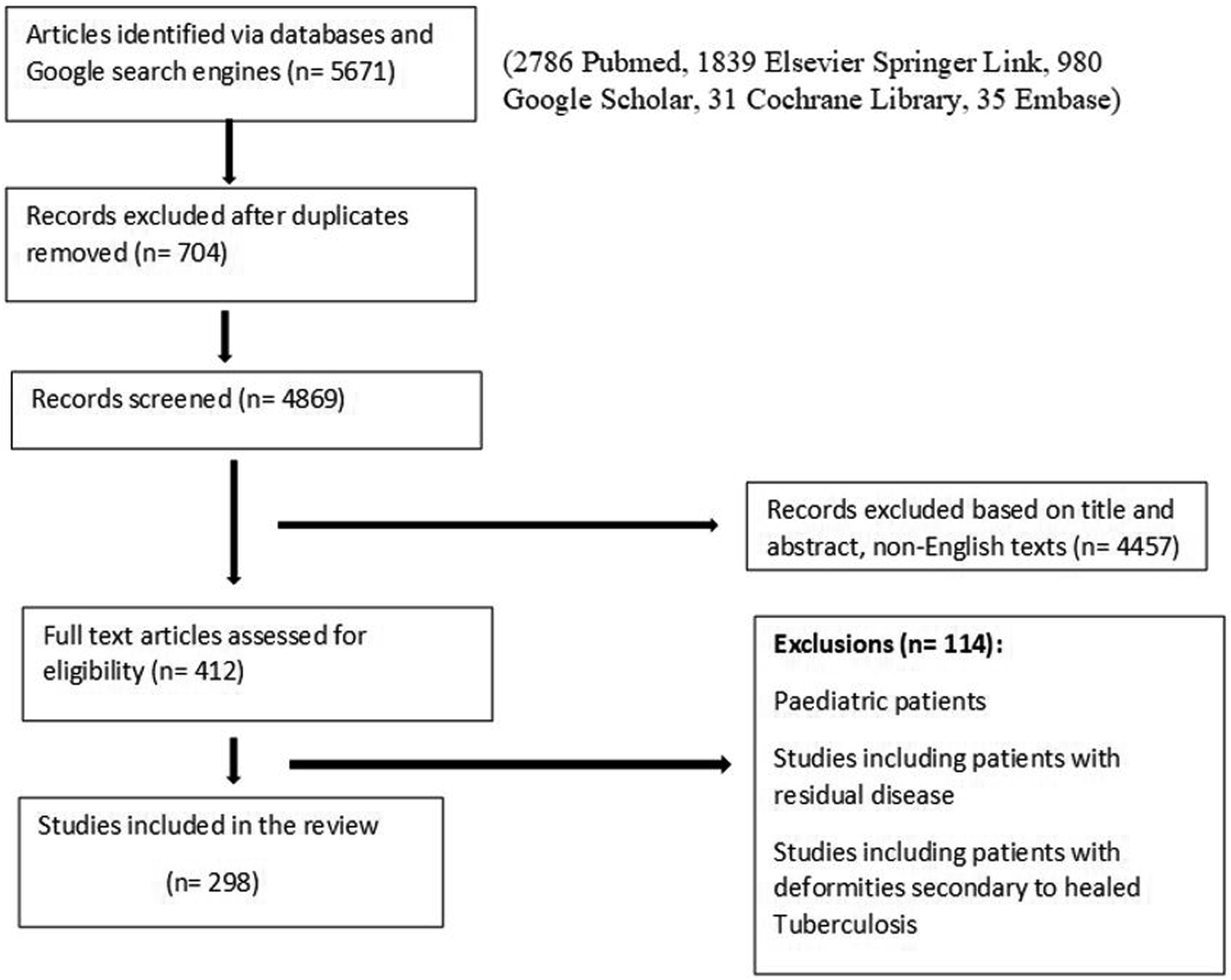
Stage II: Identification of Key Opinion Leaders (KOLs) and Preparation of the Final Questionnaire
Stage IIa - Selection Criteria and Identification of KOLs
Forty key opinion leaders (KOLs) were identified from the Association of Spine Surgeons of India (ASSI) database (both Orthopaedic and Neurosurgeons) who had substantial contributions to the literature on TB spine and were willing to act as panelists. Twenty consented and took part in formulating the questionnaire and the study protocols.
Stage IIb – Preparation of Questionnaire for Delphi Survey
The gaps in our knowledge regarding active adult spine Tb surgery were first identified, and a set of 46 questions was prepared to address these gaps. The questionnaire consisted of 4 domains– (1) Demographic data of the responder (including the number of patients with TB spine treated per year and the number of presentations/publications recorded) (2) Clinical domain: addressing pain, neurological status, and medical comorbidities (3) Radiological domain: addressing Xray, CT scan, MRI, and other imaging modalities (4) Serological domain: addressing relevant blood parameters.
The first and second authors drafted the initial questionnaire for the Delphi survey. The first web meeting with the Key Opinion Leaders was held in September 2021, in which 20 members participated, and the questions were finalized. Based on previous publications, it was decided to consider a 70% consensus as passable 7 while a 60%–70% consensus would merit reframing of the questions to eliminate ambiguities, if any, for a further second round. It was also decided that a lack of consensus on issues deemed critical by the KOLs would also merit the reframing of questions in the second round of the Delphi.
After thoroughly discussing the questions, the final questionnaire was approved at a second web meeting involving the first two authors and all the KOLs. The questionnaire was then sent out as a web-based survey to ASSI members with more than 10 years of experience in spine care and over 40 years of age as was predecided (to selectively engage the more experienced surgeons). All the questions were in the Likert format, with answers ranging from 1 to 5 (strongly disagree to strongly agree). Participation in the survey implied consent.
Stage III – Analysis of First, Second, and Third Delphi Survey Rounds
The questions which had more than 70% consensus
7
(agreement or disagreement) were filtered out, and of the remaining questions, those that had 60 to 70% consensus were rephrased, and representative case scenarios in the form of clinical and radiological data were added. These were sent out as the second round of the survey. Again, 70% consensus was taken as a cut-off, and those questions that did not achieve it were discarded. After the second-round survey, the data were analyzed. A final web meeting of all KOLs was called for discussing the data received. Questions with more than 90% consensus were taken up and a finer elaboration of those questions was done, which was recorded through a live online submission. The project timeline is depicted in Figure 2. Flowchart depicting project timeline.
Stage IV – Final Analysis and Recommendations
The final set of data were analyzed, and recommendations were created based on the results. The responses were entered into and analyzed using SPSS (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). Only descriptive statistical tools were used. For the purpose of analysis, the “strongly agree” and “agree” answers were clubbed together as: “agree” responses, and the “strongly disagree” and “disagree” responses were placed together as “disagree. The quantitative data has been described as mean +/- SD and range, while categorical data as percentages (proportions).
Results
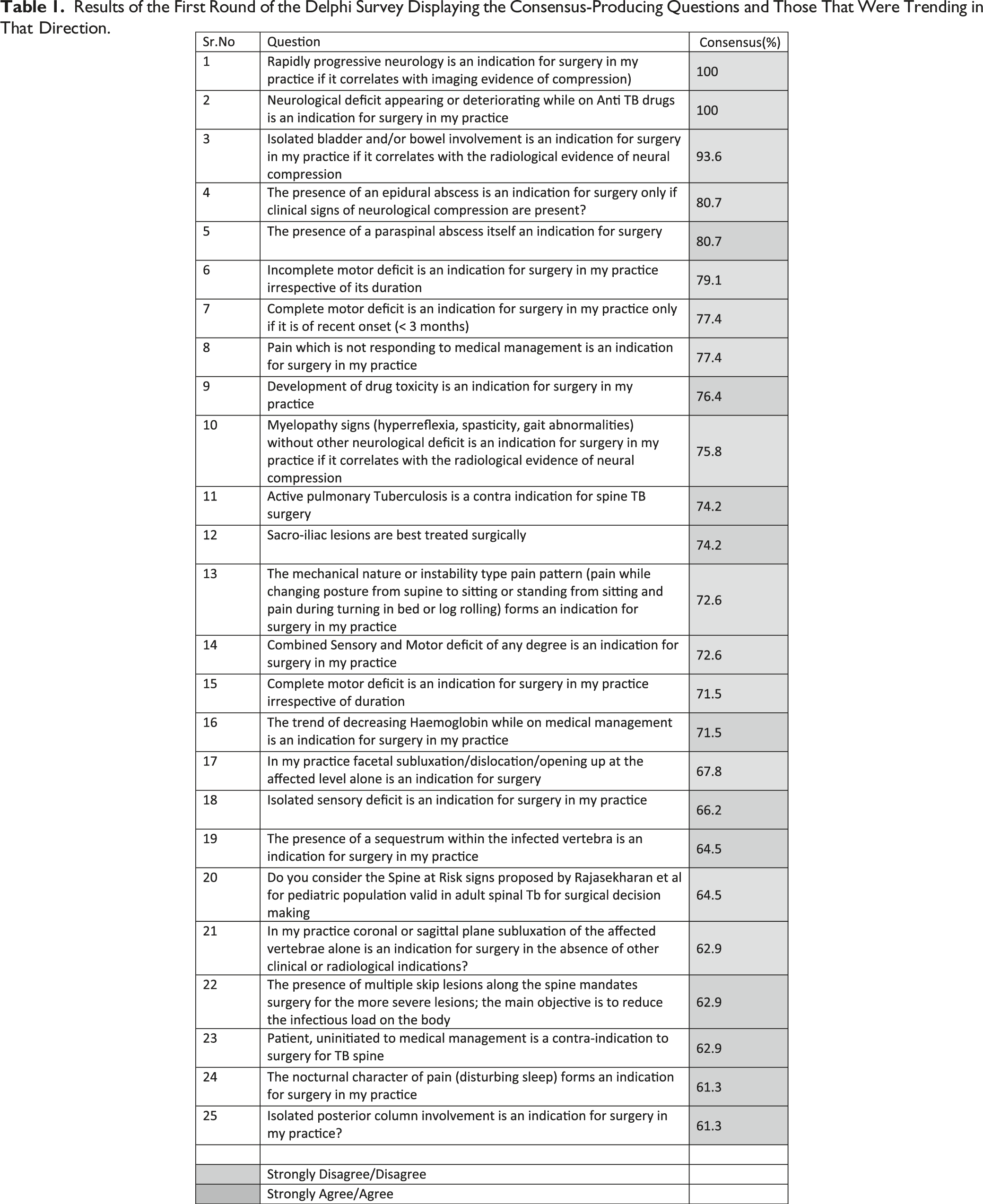
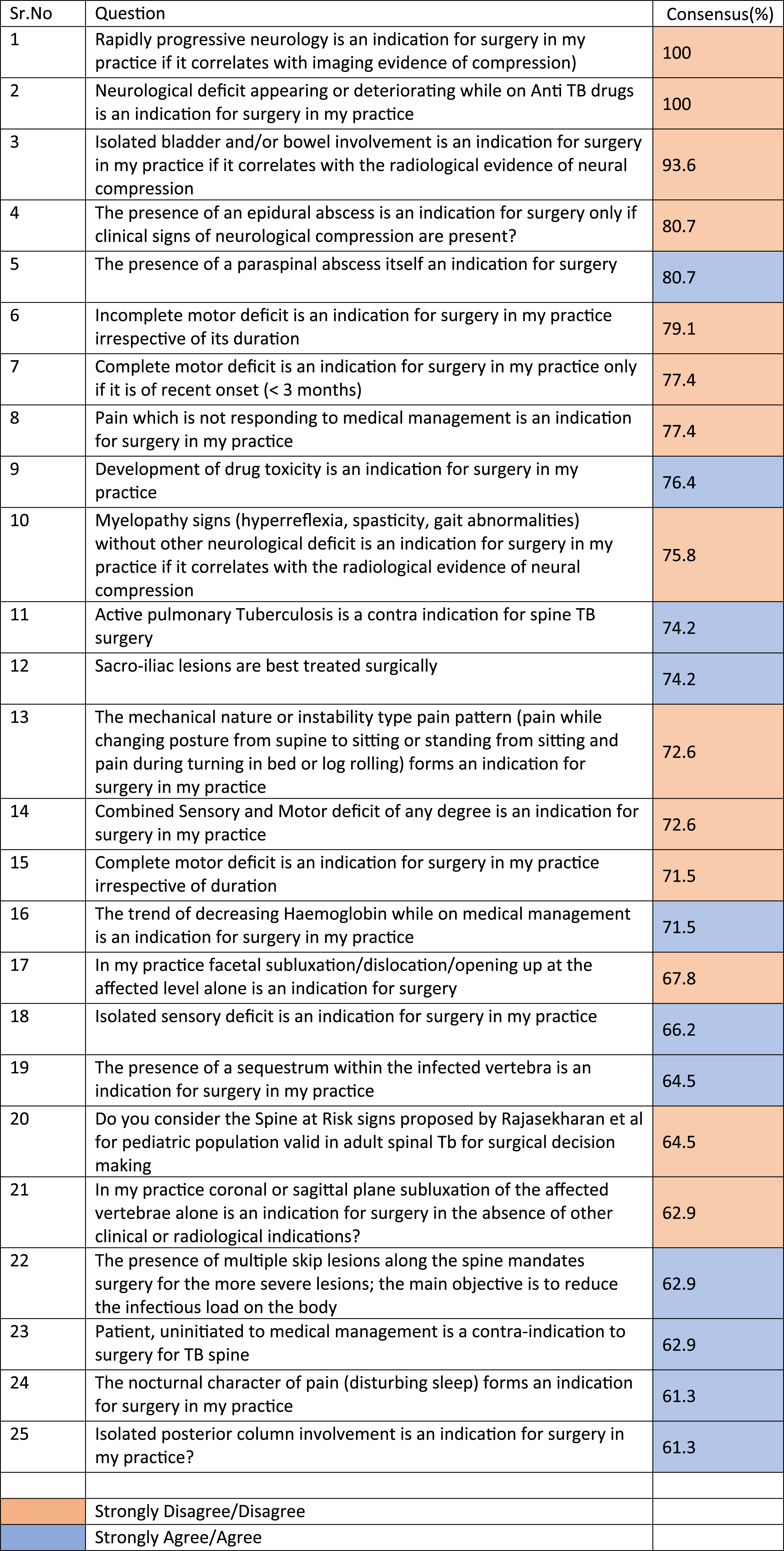
Results of the First Round of the Delphi Survey Displaying the Consensus-Producing Questions and Those That Were Trending in That Direction.
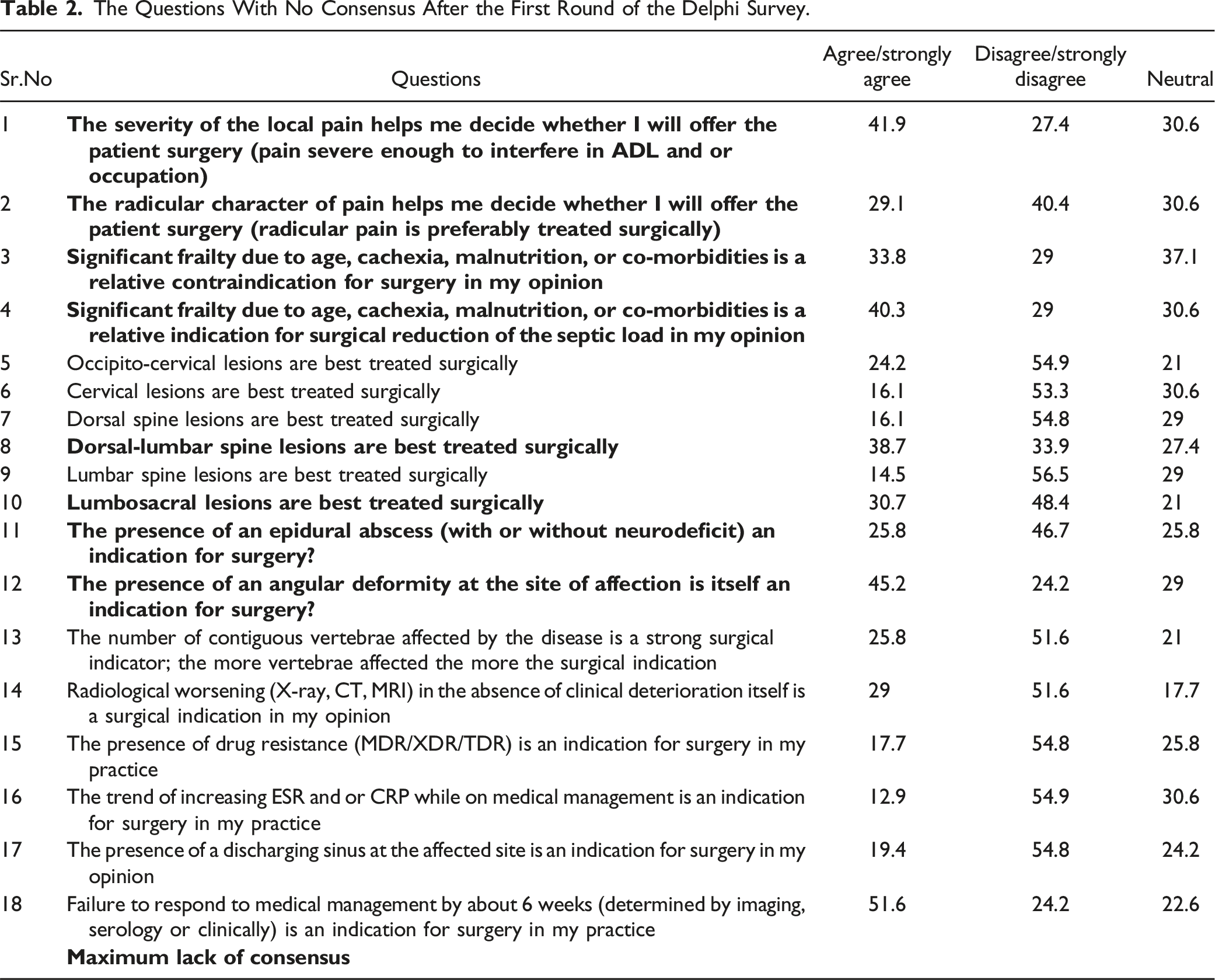
The Questions With No Consensus After the First Round of the Delphi Survey.
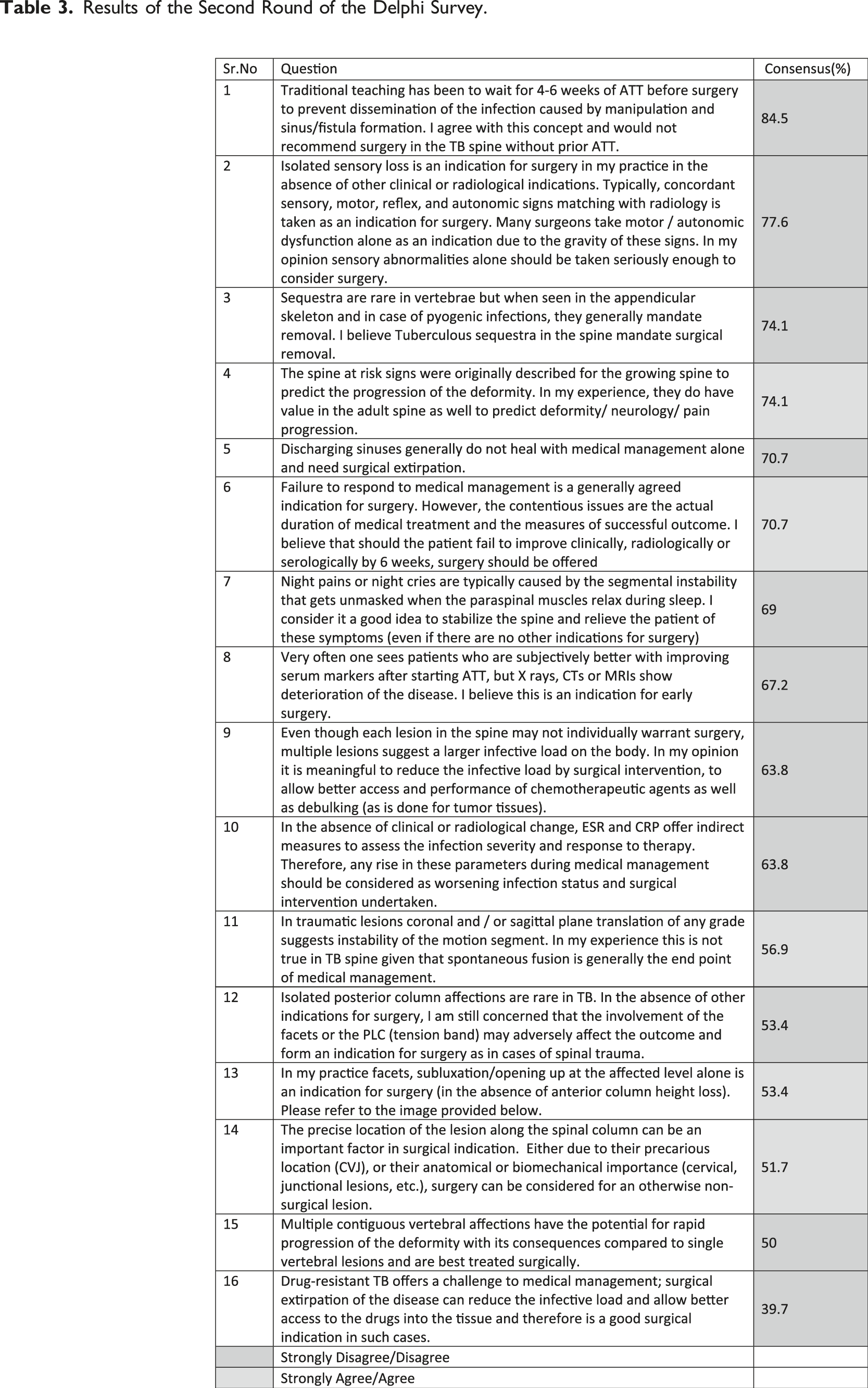
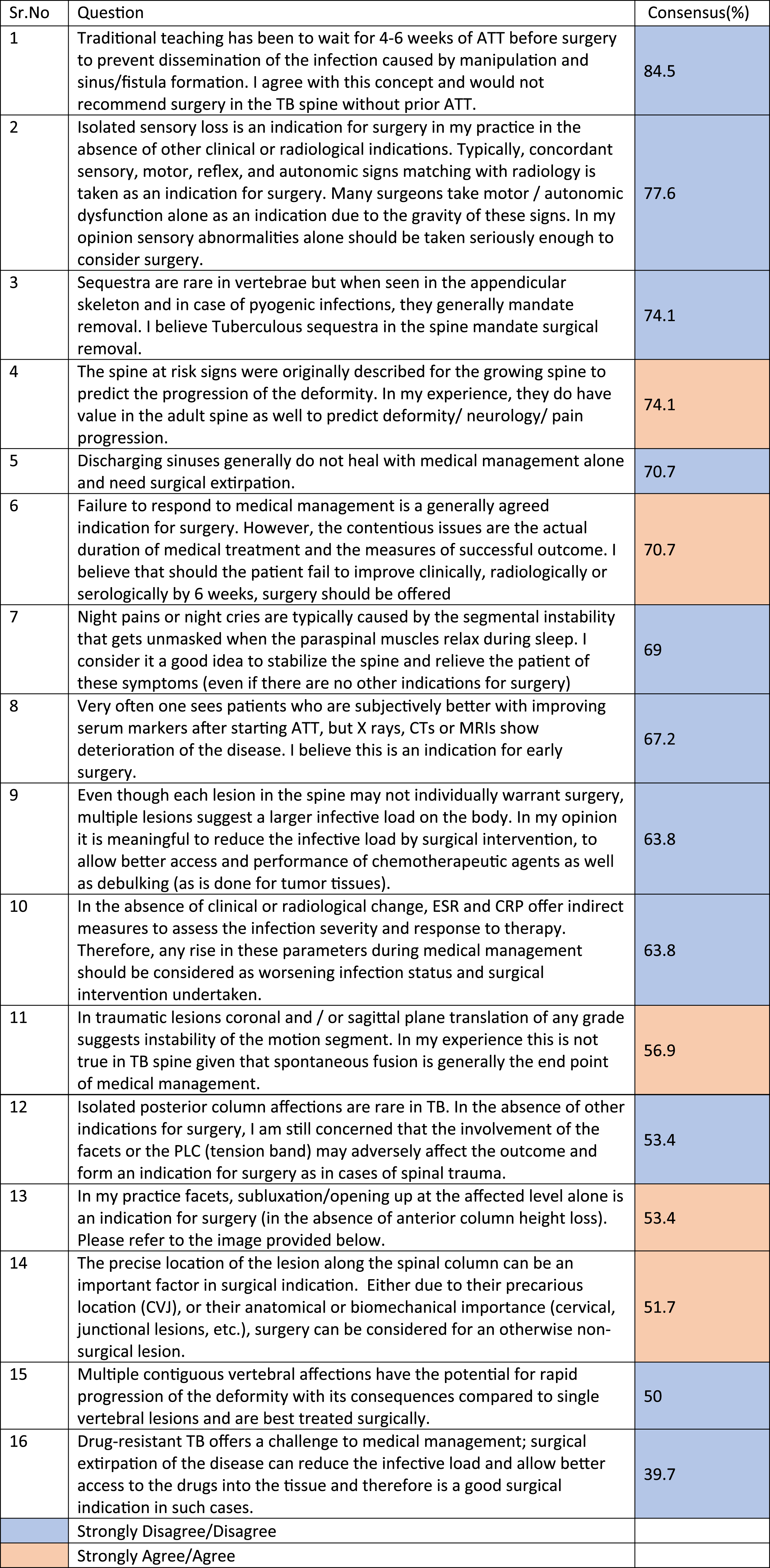
Results of the Second Round of the Delphi Survey.
A further web meeting of the KOLs and a third round (face-to-face) of Delphi were conducted online in September 2022 to iron out some remaining granularity within the topics discussed (Appendix 3). Following the final meeting, the KOLs’ final recommendations were prepared as follows –
Key Consensus Areas
Clinical Domain.
(1) Progressive neurological deficit with correlating radiology and neurological change appearing/deteriorating while on ATT are indications for surgery (100% consensus). The KOL qualified this question further by saying that progression refers to deterioration by 1 MRC grade of motor power or the appearance of bladder/bowel dysfunction (71.4%consensus). The duration of anti-tubercular chemotherapy (ATT) availed before neurological deterioration need not be considered while planning surgery (KOL consensus). (2) Isolated bladder/bowel dysfunction associated with spinal TB lesions in adults also mandates surgery (93.6% consensus). The KOLs further debated this on the background of the Cauda Equina-related debate regarding the timing of decompression and refined that irrespective of the duration of the dysfunction, such patients do need decompression (85.7% consensus). (3) The phase 1 survey agreed that if neurodeficit is the indication of surgery, then incomplete neurological deficit always needs surgery, while complete neurological dysfunction is best treated surgically if recent (less than 3 months in onset). This issue was re-debated by the expert panel, who opined that ongoing mechanical compression must be decompressed irrespective of the duration in the TB spine (71.4% concordance). (4) Pain not responding to medical management and myelopathic signs were also indications for surgery (77.4 and 75.8% concordance). The KOL defined mechanical instability as radiological and clinical and recommended surgery with 71.4% concordance. (5) There was consensus that active pulmonary TB or drug-resistant TB, or tubercular sacroiliitis would not constitute an indication for surgery (74.2, 76.4, and 74.2%consensus, respectively). (6) There was over 80% consensus in the second round that surgery can be performed without prior initiation of ATT when indicated. They also concluded that while sensory abnormalities alone do not constitute a surgical indication, failure to respond clinically, radiologically, and serologically to six weeks of ATT could be an indication for surgery.
Radiological Domain.
(1) One of the major outcomes of this survey, with over 80% concordance, was that epidural abscess does not need decompression unless simultaneous clinical neurological findings are present. Similarly, the survey concluded that the presence of a paraspinal abscess itself is not a surgical indication (unless pressure signs supervene); however, the KOLs could not agree upon the duration one should wait for the abscess to resolve with drug therapy alone. (2) Regarding the surgical indications for tubercular sacroiliitis, no consensus could be reached among the KOLs, but the survey was in favor of treating most cases non-surgically (74.2% concordance). (3) The survey, as well as the KOLs, agreed that though the Spine at Risk signs was developed to predict the progression of deformity in pediatric spine TB, it could be validated further for use as a marker of instability in adult spine TB as well, subject to appropriate studies.
Serological Domain.
(1) The survey and the KOLs concluded that hemoglobin and other health markers like S. albumin, liver function tests, ESR, CRP, and others have little contribution to surgical indications (85.7%consensus).
Key Non-Consensus Areas
Clinical Domain.
(1) There was no agreement on whether the presence of a discharging sinus is an indication for surgery; this question was refined and put to the KOLs, who again could not reach a consensus on what period one should wait for a sinus to heal by drug therapy alone. (2) Following the first round of Delphi, there was no consensus on the nature of pain (radicular or local), the severity of local pain, significant frailty, location of the lesion (occipito-cervical, cervical, dorsal, dorso-lumbar, lumbar, or lumbosacral lesions) forming an indication for surgery. (3) The presence of drug resistance in spinal TB and the presence of a discharging sinus demonstrated a trend toward disagreement for surgery (54.8%) but did not reach a level of consensus. (4) Following the second round of Delphi, there was a strong trend toward disagreement about night cries/night pains (69%) alone constituting an indication for surgery, but no consensus was reached. (5) Following the third round of Delphi, the main areas of non-consensus which persisted were the waiting period for non-healing discharging sinuses despite effective ATT, surgical treatment of sacroiliac joint TB, and the presence of paraspinal abscess as a surgical indication.
Radiological Domain.
(1) There was no consensus regarding the number of vertebrae affected, the degree of collapse or destruction of the vertebrae, and the region of the spine affected that might be construed as surgical indications. (2) The presence of an epidural abscess (with or without neurological deficit), angular deformity, and an increasing number of contiguous vertebrae affected were all considered grey zones for surgical indications, with no agreement reached. (3) Though a majority of the Delphi participants did not agree that radiological worsening (in the absence of clinical worsening) while on effective medical therapy was an indication for surgery (54.8%), there was no consensus. (4) Following the second round of Delphi, a majority disagreed that deteriorating radiology after initiating effective ATT (67.2%), debulking for reduction of infective load (63.8%), and isolated posterior column involvement with PLC tension band involvement (53.4%) were indications for surgery. However, no consensus was reached. (5) A majority of the participants agreed that facetal subluxation or opening up at the affected level (53.4%) and the anatomical location of an otherwise non-surgical lesion (%) (precarious location like CVJ, anatomical or biomechanical important sites like junctional lesions) were indications for surgery. No consensus was achieved.
Serological Domain.
(1) There was a disagreement regarding increased ESR and/or CRP while on effective ATT being surgical indications (54.8%) but did not reach a level of consensus. Following the second round, this proportion increased. (63.8%).
Discussion
This study aims to fill a major knowledge gap in our understanding of spinal tuberculosis- what are the indications for surgery in adult spinal TB during the active phase? Although there is a veritable amount of research on the subject, there is an absence of consensus studies, white papers, best practice guidelines, or Delphi-based studies on adult spinal tuberculosis. Surgical indications are hazy and extremely individualized, particularly for patients with no neurological deficit. In the absence of adequate evidence-based literature, the Delphi survey remains the methodological choice for establishing and comparing diagnostic and therapeutic practices and validating healthcare issues.8–10 In India and the surrounding nations in South Asia, spinal TB is very prevalent, and most spine surgeons have considerable exposure to various clinical and radiological grades of the disease. India has been ranked second in the world for spinal TB publications over the previous two decades. 11 In the current study, through a Delphi-based nationwide survey that included questions about clinical vignettes for surgical decision-making, the authors sought to analyze the common treatment practices and variability among spine surgeons who have expertise in the subject concerning surgical management of biopsy-proven, active, adult spinal TB.
There is no universal agreement on the surgical indication for patients presenting with neurological deficits. Treatment of neurological deficits in patients with spinal TB is the subject of much contemporary discussion.5,12–15 This varies from aggressive surgical decompression of the neural structures for all neurologic impairments 14 to simply recommending surgical management for complete paraplegia of recent onset. 15 Several authors have expressed that complete neurological recovery is possible with non-surgical management with appropriate chemotherapy. However, the first round of Delphi gave two important outcomes with 100% concordance- progressive neurological deficit (at least 1-grade MRC deterioration of motor power) with corresponding imaging evidence and neurological deficit appearing or deteriorating while on anti-TB drugs (irrespective of ATT duration) are indications for surgery. Isolated bladder and/or bowel involvement with corresponding radiological evidence is also a surgical indication. Experts also differ in their approach to neurological events based on their chronology- for instance, early neurological involvement is aggressively operated, while some authors have advocated medical therapy alone in these cases under strict observation.5,13,16 These observations are based primarily on published case series. The first round of the Delphi survey found that if neurodeficit is the indication for surgery, then incomplete neurological deficits always require surgery, whereas complete neurological dysfunction is best addressed if it is recent and if substantial recovery is to be expected (onset within three months). However, the expert panel re-debated this issue, concluding that continuous mechanical compression in the TB spine must be decompressed regardless of duration (71.4% concordance).
It is an established surgical convention that pus formation anywhere in the body, from any cause, is best treated by surgical evacuation. However, in tuberculous infection, chemotherapy alone has proven to be extremely effective in treating paraspinal and epidural abscesses 17 ; nonetheless, many surgeons use the above surgical dictum to treat these situations as surgical indications. Proponents of early surgery argue that delay in evacuation of the pus might result in the failure of medical management. Yet this has not been established in clinical situations- most authors have reported excellent results even without surgery. 18 As a result, surgical drainage is often reserved for abscesses that worsen despite chemotherapy or signs of mechanical pressure of the abscess due to its size or location.12,19 One of the significant findings of this survey (over 80% consensus) was that epidural abscess does not require decompression unless there are concordant clinical neurological symptoms. Similarly, the survey indicated that a paraspinal abscess is not a surgical indication (unless pressure signs are present). However, the KOLs could not agree on how long one should wait for the abscess to resolve with drug therapy alone. Other issues that lacked consensus were the treatment of persistent large paraspinal abscesses on successive MRI scans despite otherwise effective ATT, and the waiting period for non-healing sinuses despite otherwise effective ATT.
Many factors must be considered while deciding whether to perform surgery, including age and comorbidities of the patient, the lesion's location, particularly the proximity to neural elements, the number of vertebrae implicated, the kyphosis angle, and neurological deficits, to list a few. 20 While intractable pain not responding to medical therapy, myelopathy signs, and mechanical instability were indications for surgery in this survey (concordance rates 77.4, 75.8, and 71.4%, respectively), there was no consensus on the nature of pain (radicular) or the severity of local pain as indications for surgery. On the contrary, night cries/night pains (69%) showed a strong trend towards disagreement (no surgical indication). The survey disagreed that concomitant active pulmonary TB, development of drug toxicity, or tubercular sacroiliitis would form an indication for surgery (76.4 and 74.2% concordance). The survey and KOLs found that hemoglobin and other general health marker levels, such as serum albumin, liver function tests, ESR, and CRP, have little influence on surgical indications (85.7% agreement). There was also no agreement among respondents about the surgical indications for the lesion's location, the severity of the local pain, significant fragility, the presence of an epidural abscess (without neurodeficit), angular deformity, and an increasing number of adjacent vertebrae affected. Similarly, drug resistance, radiological worsening without clinical worsening, elevated ESR and/or CRP, and a discharging sinus all showed a tendency toward disagreement (54.8%), but did not reach a threshold of statistically significant consensus.
What is the Value of This Study, and What Needs to be Done in the Future
This Delphi-based survey serves several purposes in the surgical management of adult spinal tuberculosis. This consensus study is meant to establish best practice guidelines to help surgeons treat patients with spinal tuberculosis. This is the first nationwide study to obtain a consensus on various dilemmas in the surgical treatment of spinal tuberculosis. This consensus is the product of several rounds of expert input, which culminated in the final findings from spine specialists (KOLs) from various parts of India. This collection of questions and answers can serve as the foundation for a shared language and strategy to address most outstanding issues related to surgical indications in adult spine TB. Alongside the establishment of national guidelines, it is also hoped that studies to validate each of the recommendations will be undertaken in the future.
This survey deals exclusively with single parameter indications for surgery in a given condition: what would be the thought process when multiple parameters are present but at sub-threshold levels? Evidently, this is where a scoring system (akin to the TLICS system for thoracolumbar spine trauma) needs to emerge, incorporating the various domains that have been addressed by the current survey.
The surgical indication is a rather broad term- depending on the precise location and various other denominators, the actual procedure may vary significantly. For example, decompression for neurological compromise, stabilization for instability, debridement, and evacuation for collection of pus and granulation tissues, reconstruction for large-scale tissue destruction, and combinations of the above. Future studies would also hopefully elucidate the optimal surgical strategy in a given clinical situation.
How Does the Existing Literature Compare With the Current Findings
Given that there is no good quality evidence for the treatment of such patients, the best that current literature can offer is a wide variety of surgical indications and techniques. Wang et al. proposed that the diagnosis of recurrence or reactivation can be aided by the reappearance of signs and symptoms, biochemical indicators including ESR and C-reactive protein, and radiological worsening of the deformity. 21 However, this survey showed a strong trend towards disagreement against the use of deteriorating radiology after initiating sensitive ATT (67.2%), rising ESR, and/or CRP (63.8%) as indications for the failure of medical management. Qian’s series utilized the neurological status (Frankel grades D and E), severe back pain, extensive formation of sequestrum, and significant spinal instability were inclusion criteria for a randomized controlled trial comparing surgical interventions for thoracolumbar spinal TB 22 where they demonstrated the beneficial effects of surgery in these conditions. In another RCT 23 by Jin and coworkers on TB of the lumbosacral spine, the authors used one of the following surgical indications- large abscess, dead bone, bony cavity, sinus tract, spinal instability, kyphosis, compression of neural structures that resulted in dysfunction, and drug resistance. Paradoxically, in the current survey, the presence of drug resistance (54.8%), a discharging sinus (54.8%), debulking for infection load reduction (63.8%), and isolated posterior column involvement with PLC tension band involvement (53.4%) all showed a substantial propensity for disagreement as grounds for surgery. Predictive indicators of late deformity can be seen in early deformity. The term “spine-at-risk signs” was coined by Rajasekaran et al. for these straightforward radiological markers in children. 24 However, facetal subluxation or opening up at the affected level as a surgical indication for adult spinal TB did not reach a consensus (53.4% agreement).
Strengths and Limitations of the Study
This study’s creative use of an online poll as a technique is one of its strengths. Twenty spine specialists from across the country were able to contribute their experiences live using this strategy. This strategy also enabled experts to contribute their unbiased, anonymous opinions through the medium of the first 2 phases of the survey. The formation of KOLs to refine the question set and final data analysis adds a distinct finesse to the study.
While this set of questions is a useful tool for the surgical management of adult spinal tuberculosis, it has certain limitations. The results of the Delphi-based survey were based on respondents only from India. Several countries like China, South Africa, Turkey, Brazil, and East Asia have extensive experience in treating such conditions, and in the future, the study could be expanded to include these regions. This study's findings were restricted to adequately experienced ASSI members who were willing to fill out the survey, leaving out those who did not respond or fulfill these criteria. The validity of the recommendations should be tested in a clinical context, despite the fact that spinal experts from across the country provided their insights for our study. Additionally, some issues like quality of life, particularly in the context of early pain relief and return to work offered by surgery, were not adequately addressed in the questionnaire.
Conclusion
According to our knowledge, this is the first study that has established a national consensus on the indications of surgery while treating active adult spinal TB. This study hopes to give a complete picture of surgical indications that form an unresolved concern in the management of spine TB.
Supplemental Material
Supplemental Material - Delphi-Based Survey for Surgical Indications in Biopsy Proven Active Adult Spinal Tuberculosis
Supplemental Material for Delphi-Based Survey for Surgical Indications in Biopsy Proven Active Adult Spinal Tuberculosis by K. Venugopal Menon, MS, MCh, MSC, Saumyajit Basu, MS, DNB, FRCS, Gauri Oka, MBBS, MPH, Kushal Gohil, MS, DNB in Global Spine Journal.
Footnotes
Acknowledgments
We thank the members of the Association of Spine Surgeons of India who participated as Key Opinion Leaders.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.