
Abstract
Study Design:
Modified Delphi study.
Objective:
The objective of this study was to establish expert consensus on the application of lateral lumbar interbody fusion (LLIF) by using the modified Delphi study.
Methods:
From June 2019 to March 2020, Members of the Chinese Study Group for Lateral Lumbar Spine Surgery were selected to collect expert feedback using the modified Delphi method where 65 spine surgeons from all over China agreed to participate. Four rounds were performed: 1 face-to-face meeting and 3 subsequent survey rounds. The consensus was achieved with ≥a 70.0% agreement for each question. The recommendation of grade A was defined as ≥90.0% of the agreement for each question. The recommendation of grade B was defined as 80.0-89.9% of the agreement for each question. The recommendation of grade C was defined as 70.0-79.9% of the agreement for each question.
Results:
A total of 65 experts formed a panelist group, and the number of questionnaires collected was 63, 59, and 62 in the 3 rounds. In total, 5 sections, 71 questions, and 382 items achieved consensus after the Delphi rounds including summary; preoperative evaluation; application at the lumbar spinal stenosis, lumbar disc herniation, lumbar spondylolisthesis, adult degenerative scoliosis, postoperative adjacent segmental degeneration, and revision surgery; complications; and postoperative follow-up evaluation of LLIF.
Conclusion:
The modified Delphi method was utilized to ascertain an expert consensus from the Chinese Study Group for Lateral Lumbar Spine Surgery to inform clinical decision-making in the application of LLIF. The salient grade A recommendations of the survey are enumerated.
Introduction
More recently, a less invasive lateral lumbar interbody fusion (LLIF) technique has been reported using cages inserted through the lateral transpsoas approach.1-4 This approach reportedly has the advantages of short operative time, less bleeding, large bone graft area, high fusion rate, short hospitalization time, and lower complication rates, which has been widely used in the treatment of various lumbar diseases.1-4 Lumbar interbody fusion is an established treatment for numerous spinal disorders, such as degenerative, traumatic, infectious, and tumorous pathologies. The anterior lumbar interbody fusion (ALIF) technique, posterior lumbar interbody fusion (PLIF) technique, and transforaminal lumbar interbody fusion (TLIF) technique have been well described.5-8 At present, there are still many controversies on the preoperative evaluation, clinical indications, contraindications, complications, and postoperative follow-up evaluation.1-4,9-12
The modified Delphi method. 13 is an anonymous method of soliciting expert opinions through multiple rounds of face-to-face surveys and systematically-designed questionnaires.
The purpose of this study was to establish the consensus of experts on the application of lateral lumbar interbody fusion (LLIF) by using the modified Delphi method.
Methods
Study Design
A modified Delphi survey. 13 was performed with 1 face-to-face meeting (June 2019) and 3 subsequent web-based surveys (June 2019 to March 2020).
Development of Questionnaires
The research team prepared the proposal and was approved by the Chinese Study Group for Lateral Lumbar Spine Surgery (approval number not applicable). The research team searched the databases PubMed, Medline, EMBASE, the Cochrane library, Clinical key, Springer link, Wiley Online Library, CNKI, and Wanfang, of studies reporting LLIF with PRISMA guidelines. Case reports, commentaries, and cadaveric or experimental studies in animals were excluded. 18 comparative studies, 37 cohort studies, and 13 systematic reviews were included and used to build the questionnaire. 3 members of the research team were responsible for reviewing and evaluating the studies using the published evidence rating system. 14 to control specifically for confirmation bias and ensure validity and consistency. The questionnaire contained a summary; preoperative evaluation; application at the lumbar spinal stenosis, lumbar disc herniation, lumbar spondylolisthesis, adult degenerative scoliosis, postoperative adjacent segmental degeneration, and revision surgery; contraindications; complications; and postoperative follow-up evaluation of LLIF. There were 119 survey questions in the questionnaire, including 48 single-choice questions (40.3%), 71 multiple-choice questions (59.7%), and 382 options in total. In single-choice questions, only 1 option can be selected. And in multiple-choice questions, 1 or more options can be selected.
Panelists
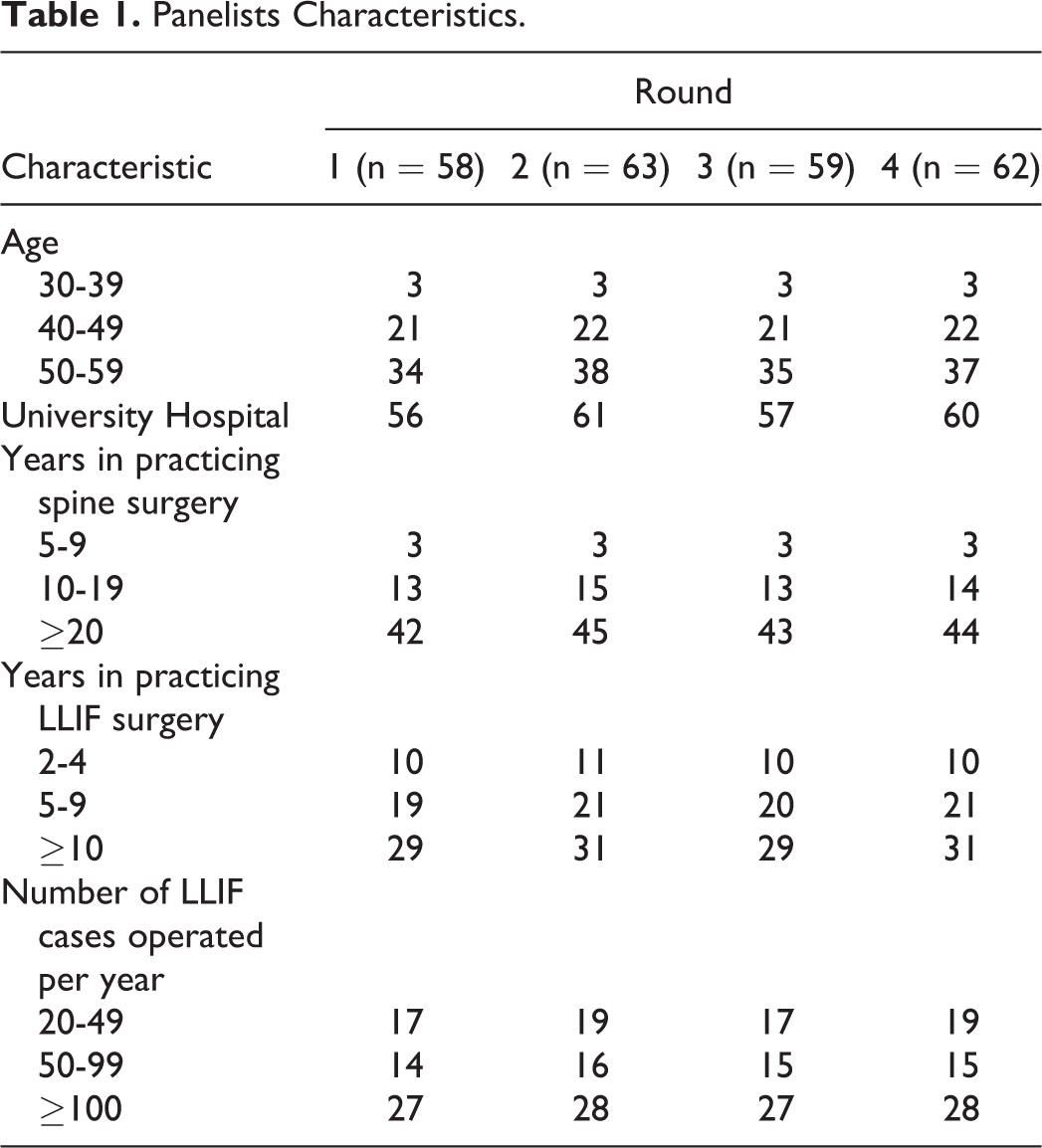
Invitation to participate was sent by email to all members of the Chinese Study Group for Lateral Lumbar Spine Surgery (n = 77). A total of 72 members replied and 65 were selected and agreed to participate. Eligibility was based on the number of years in practice (minimum of 5 years in practicing spine surgery and a minimum of 2 years in practicing LLIF surgery) and an estimated number of LLIF cases operated (minimum of 20 patients) per year. The panelists’ mean age was 50.7 years, and 95.2% had been practicing spine surgery for more than 10 years, 82.5% had been practicing LLIF surgery for more than 5 years (Table 1).
Panelists Characteristics.
Delphi Rounds
The survey consisted of 4 rounds; 1 face-to-face meeting and 3 subsequent survey rounds. If the questions were agreed by 70.0% or more experts, they were reached to a consensus. If the questions were agreed by 30.0% or fewer experts, they were excluded from the consensus. And the questions will go to the next round if they were agreed between 30.0% to 70.0% experts.
In the first round: 58 panelists met face-to-face, discussed, and modified the survey questionnaires.
The second round: The panelists received the modified questionnaires using the online platform https://www.wjx.cn (WenJuanXing, CSX, CHN) and were asked to make their choices according to their experiences.
The third round: Questions that did not reach consensus in the second round were revised for additional clarification. And the panelists received the new survey and were asked to make their choices.
The fourth round: For the questions that did not reach consensus in the third round, the research team changed some multiple-choice questions into single-choice questions, and further clarified the questions and options based on published studies. The panelists received the new survey and were asked to make their choices.
Data Analysis
The research team analyzed the results of every round. A response rate of >70.0% were considered valid for each round of the survey. And the consensus was defined as ≥70.0% of the agreement for each question. The recommendation of grade A was defined as ≥90.0% of the agreement for each question. The recommendation of grade B was defined as 80.0-89.9% of the agreement for each question. The recommendation of grade C was defined as 70.0-79.9% of the agreement for each question.
Results
Of 77 panelists invited, 65 participated, responses were received from 63, 59, and 62 for each survey, respectively (Table 1).
Sixty-three panelists responded to the first questionnaire (second round) and 176 options achieved consensus. Fifty-nine panelists responded to the second questionnaire (third round) and 37 options achieved consensus. Sixty-two panelists responded to the third questionnaire (fourth round) and 25 options achieved consensus.
In total, 71 questions including 238 options achieved consensus after the Delphi rounds. Grade A consensus was achieved in 34.9% of options, Grade B in 23.7% of options, and grade C in 41.4% of options.
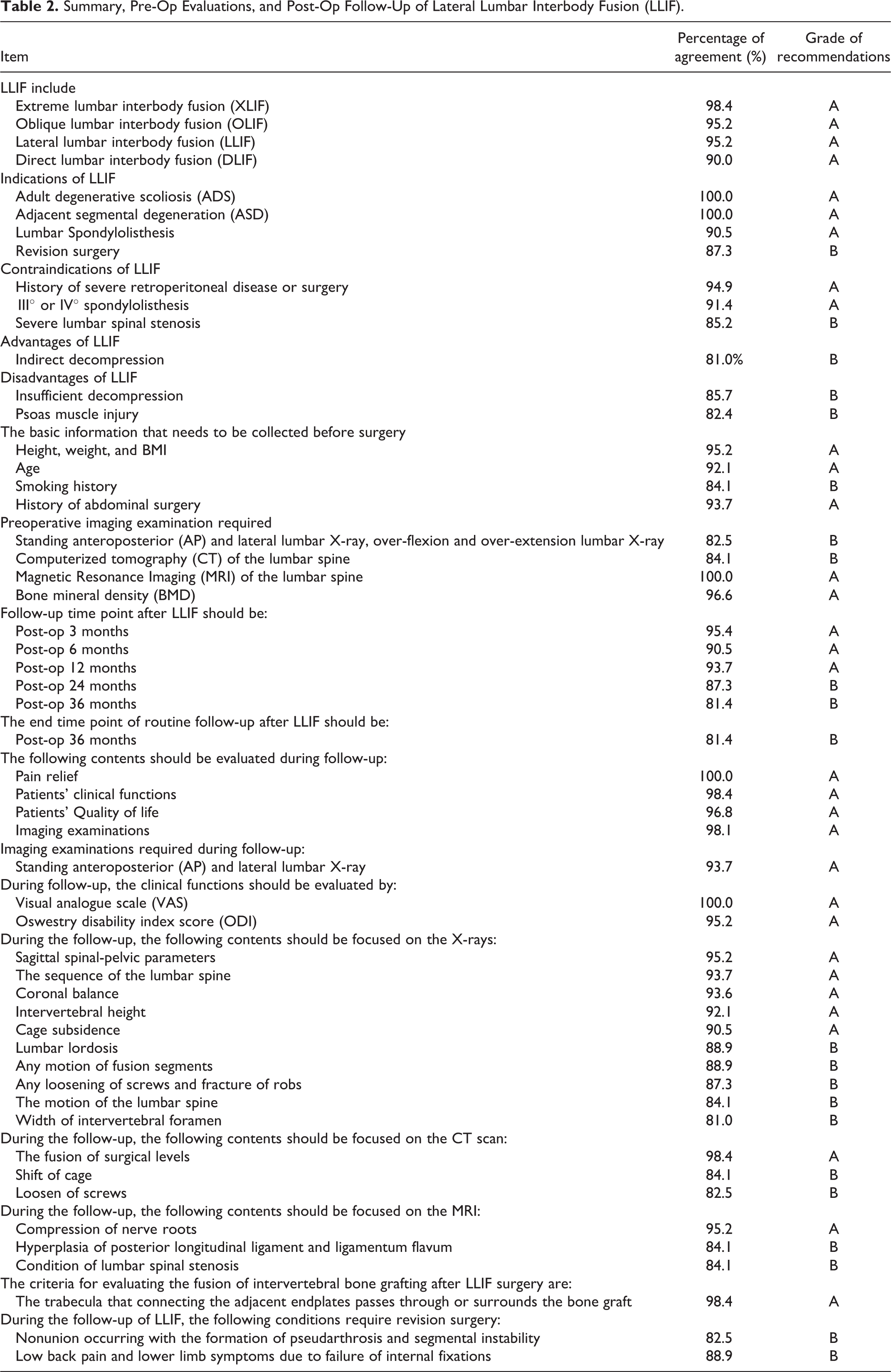
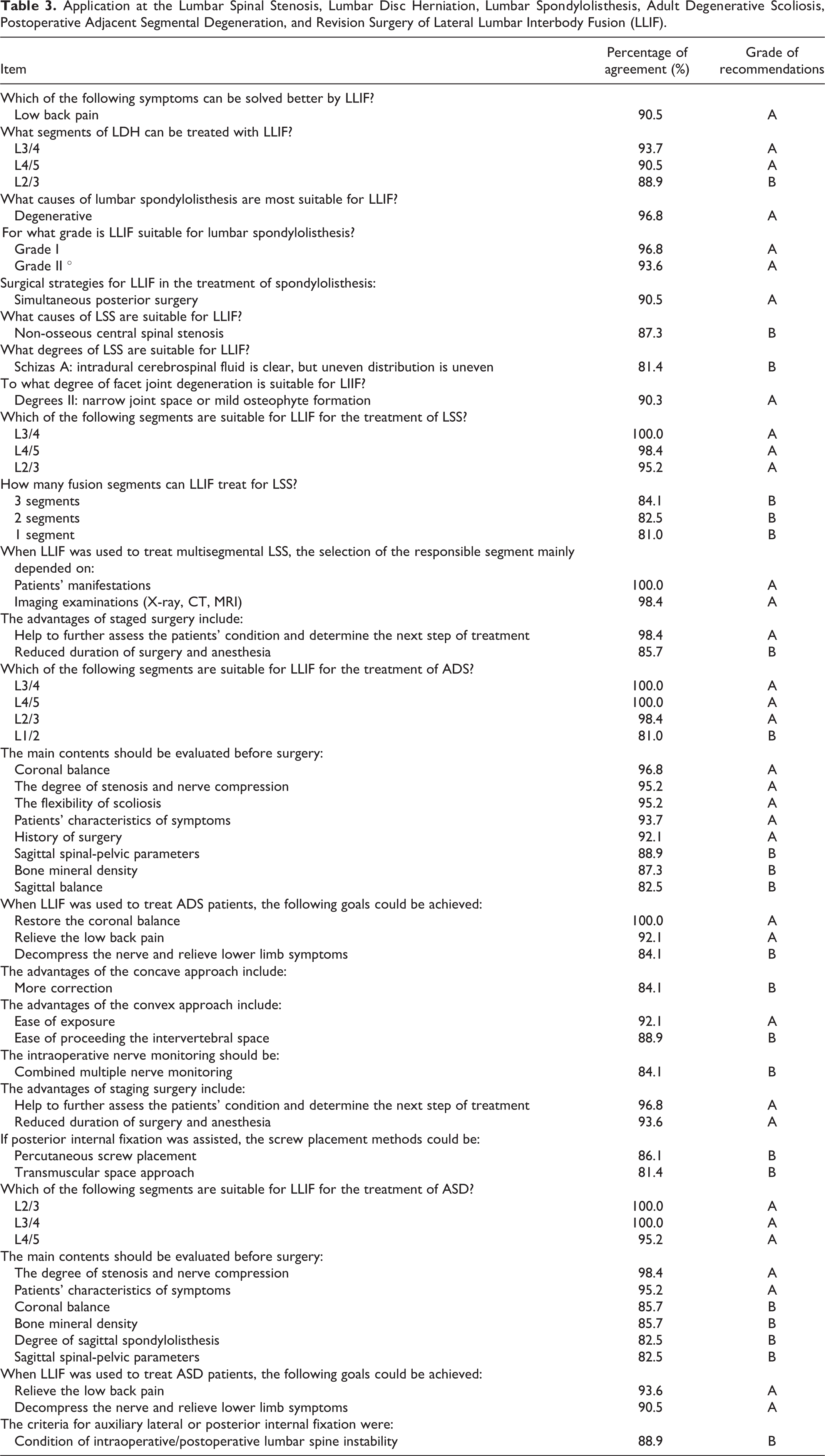
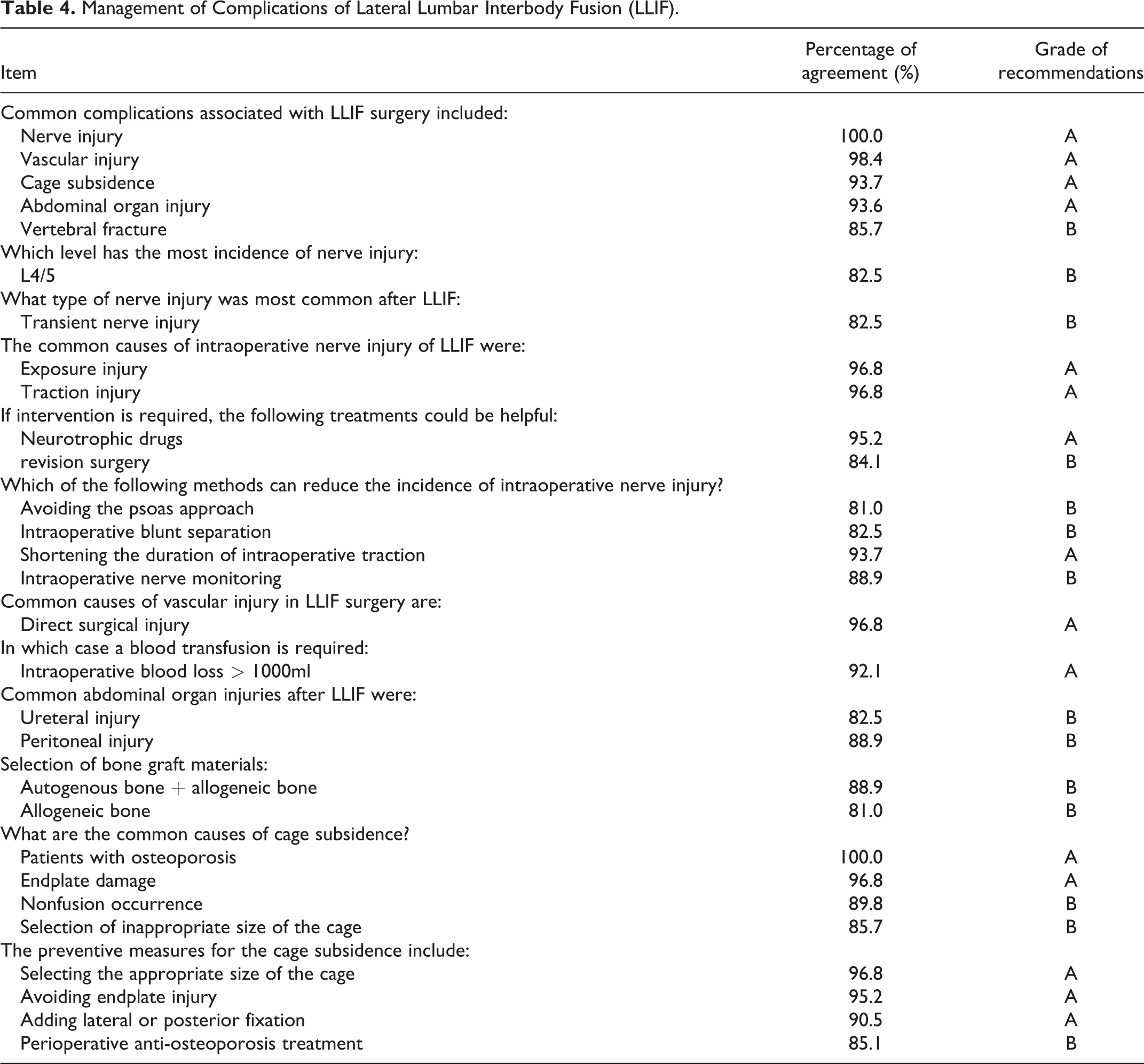
Tables 2, 3, and 4 summarized grade A and B recommendations and percentage of agreement regarding the summary of LLIF including indications, contraindications, advantages, and disadvantages; the preoperative evaluation; the LLIF application at LDH, LSS, lumbar spondylolisthesis, ADS, ASD, and revision surgery; the postoperative follow-up and evaluations; the management of complications, etc.
Summary, Pre-Op Evaluations, and Post-Op Follow-Up of Lateral Lumbar Interbody Fusion (LLIF).
Application at the Lumbar Spinal Stenosis, Lumbar Disc Herniation, Lumbar Spondylolisthesis, Adult Degenerative Scoliosis, Postoperative Adjacent Segmental Degeneration, and Revision Surgery of Lateral Lumbar Interbody Fusion (LLIF).
Management of Complications of Lateral Lumbar Interbody Fusion (LLIF).
Discussion
The research team searched several Chinese and English databases and most of the items in the consensus were supported by evidence-based studies.
In this consensus, LLIF includes extreme lumbar interbody fusion (XLIF), oblique lumbar interbody fusion (OLIF), lateral lumbar interbody fusion (LLIF), crenel lumbar interbody fusion (CLIF), and direct lumbar interbody fusion (DLIF). Indications of LLIF include lumbar disc herniation (LDH), lumbar spondylolisthesis of grade I and II, lumbar spinal stenosis (LSS), adult degenerative scoliosis (ADS), revision surgery, and adjacent segmental degeneration (ASD). Contraindications of LLIF include the history of severe retroperitoneal disease or surgery, congenital lumbar spinal stenosis, severe lumbar spinal stenosis, lumbar spondylolisthesis of grade III and IV, the noose of the facet joints, and severe degenerative facet joint lesions. They were consistent with published literature.1-12,15-22
Kwon et al. 19 and Xu et al. 20 suggested that LLIF can treat I°/II° lumbar spondylolisthesis. Ozgur et al. 21 also indicated that severe spondylolisthesis was one of the contraindications to LLIF. Chester et al. 22 suggested that almost all LLIF patients needed to undergo second-stage open posterior spinal fusion and segmental pedicle screw fixation. Heo et al. 23 investigated patients with lumbar disc herniation treated by OLIF combined with intervertebral foraminal endoscopy, and the follow-up showed that the postoperative recovery of the patients was good.
Anand et al. 24 used XLIF to treat ADS patients, the Cobb angle, Visual analogue scale (VAS), and Oswestry dysfunction index (ODI) scores were also improved significantly at the 2-year follow-up. Tormenti et al. 25 conducted a comparative study of XLIF combined with open posterior fixation (8 cases) and PLIF (4 cases) for ADS patients, and the results showed that the cobb angle of patients in the XLIF group was corrected significantly better than PLIF group. Acosta et al. 26 investigated that DLIF could effectively restore the coronal and sagittal balance of the lumbar spine.
The advantages of LIIF include more minimally invasive, higher fusion rates, indirect decompression, improved spinal stability, shorter hospital stay, better restoration of coronal balance, and better restoration of sagittal balance in our study. Studies.15,23,27 have shown that the complication rates of LLIF are lower than that of TLIF and PLIF, but there is a risk of injury of the lumbosacral plexus nerve during psoas muscle dissection. LLIF has greater mechanical stability than PLIF, not only because it uses a larger cage, but also because structures such as the posterior ligaments are well protected.
Pereira et al. 15 and Xu et al. 16 suggested that LLIF was increasingly used in the treatment of lumbar spinal stenosis and degenerative disc diseases. Karikari et al. 17 reported that the average blood loss of patients receiving LLIF in segments L1 to L2 alone was 46 ml, and that of patients receiving LLIF in more than 2 segments was 175 ml. Attenello et al. 18 indicated that open internal fixation had a better correction, but it was also associated with higher complications.
In this study, whether auxiliary lateral or posterior internal fixation is required for LLIF surgery should be determined via the intraoperative stability of the cage, condition of intraoperative/postoperative lumbar spine instability, and integrity of posterior ligament complex. Louie et al. 28 concluded that the LLIF of stand-alone was safe and effective. John et al. 29 demonstrated that the open internal fixation group had a better correction, but it was also associated with higher complications. The advantages of staging surgery reached to consensus in this study include the reduced duration of surgery and anesthesia, reduced risks of complications, reduced the difficulty of correction, and help to further assess the patients’ condition and determine the next step of treatment.
Moreover, the consensus indicated that the selected cage could appropriately increase the height of the intervertebral space of the surgical segment and the location of the cage should be placed in the middle of the intervertebral space.
Sembrano et al. 30 and Park et al. 31 indicated that compared with a non-lordosis cage, the cage with lordosis can achieve greater correction of lordosis in surgical segments, but there is no significant difference in the restoration of global lumbar lordosis. They also suggested that place the cage in the front 1/3 of the vertebrae is more conducive to restore lordosis.
As for nerve monitoring in LLIF, most studies.32-36 reported that nerve monitoring should be performed during LLIF to reduce the incidence of nerve injury. However, there is also a study. 37 suggesting that the incidence of nerve injuries has no significant difference between the groups that use or don’t use intraoperative nerve monitoring. Multiple nerve monitoring is recommended according to this consensus.
Zhu et al. 38 demonstrated that the operation time, intraoperative blood loss, the hospital stay of the OLIF group was significantly better than that of the PLIF group, while the VAS/ ODI score and intervertebral space height restore of the OLIF group was better than that of the PLIF group at 3 months after surgery. The fusion rate of the 2 groups was the same at 12 months after surgery.
The complications of LLIF include nerve injury, vascular injury, abdominal organ injury, vertebral fracture, pseudarthrosis, and cage subsidence in this study. Hijji et al. 39 found that the common complication after LLIF was transient nerve injury, with an incidence of 36.1%, and the permanent injury was only 4.0%. Joseph et al. 40 also concluded that the incidence of revision surgery was about 3.74%, and the reasons for revision surgery after LLIF included incision infection, nerve damage, epidural hematoma, psoas hematoma, adjacent segment degeneration, and formation of pseudarthrosis.
In this study, the cage subsidence most often occurs in the upper endplate, and the common causes of cage subsidence include osteoporosis, without lateral or posterior fixation, cage located inappropriately, high BMI, endplate damage, and selection of the inappropriate size of the cage. Le et al. 41 found that greater cage or posterior fixation may be needed to reduce the risk of cage subsidence for patients with osteoporosis. Lang et al. 42 suggested that cage sinking into vertebral body > 2 mm as the evaluation standard for cage subsidence in their study. However, Tohmeh et al. 43 and Bocahut et al. 44 used cage sinking into vertebral body > 4 mm as the evaluation standard for cage subsidence. Marchi et al. 45 suggested that the criteria for the postoperative fusion of LLIF were as follows: 1. The trabecula that connecting the adjacent endplates passes through or surrounds the bone graft; 2. The motion range in the fusion segments < 5°; 3. The shift of the fusion segment ≤3 mm; 4. The transparency line at the upper and lower ends of the intervertebral bone grafting does not exceed 50%.
In the Delphi survey, the selection of panelists is the key to success in the establishment of expert consensus. The improper selection of experts will increase the bias in the investigation and lead to the decline of the response rate in the consultation process. In this study, panelists were selected from the medical systems of more than a dozen provinces, municipalities, and autonomous regions in China to form an expert group. Although their ages, the number of years in practice, and experience impact beliefs on LLIF are different, they are all members of the Chinese Study Group for LLIF and fulfill the selection criteria which was well represented in terms of age and medical practice. In the process of expert evaluation, the questionnaire recovery rate was more than 90%, and the proportion of experts who proposed modification was high. Most of the treatments in the resulting expert consensus are well supported by evidence-based medicine.
Furthermore, the modified Delphi method is a popular method of soliciting expert opinions through multiple rounds of face-to-face surveys and systematically-designed questionnaires. It has been employed and widely used to help enhance effective decision-making. The method gathers opinions from a diverse panel of experts and anonymity eliminates the risk of biased opinions. Also, there is an opportunity given to participants to further express their views in the face to face round. There are fewer drawbacks of the modified Delphi method such as there are no systematic guidelines and participants are required to be continually involved in answering a similar question in multiple rounds. 13
There are also some limitations in this study: (1) the selected panelists are all from China, therefore, the expert consensus does not apply to other countries and regions. (2) There is a lack of statistical analyses in the Delphi rounds. No reliability analyses were performed, which may significantly bias the findings of the present study. (3) XLIF, OLIF, LLIF, CLIF, and DLIF are not well distinguished. Although these technologies are typical representatives of lateral intervertebral fusion technologies, there are some differences.46-47
Conclusions
The modified Delphi method was utilized to ascertain an expert consensus from the Chinese Study Group for Lateral Lumbar Spine Surgery to inform clinical decision-making in the application of LLIF. LLIF is an minimally invasive, effective and safe approach for treating numerous degenerative lumbar disorders. The best indications for LLIF are ASD, ADS, and lumbar degenerative listhesis grades I and II; The major contraindications are >grade 3 listhesis and retroperitoneal surgery/ disease; Pre-op MRI and DEXA are mandatory; Convex side access is better in ADS; Nerve injury is caused by exposure and traction injuries and is best relieved by neuropathic drugs.
Footnotes
Authors’ Note
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. We have permissions for the use of software, questionnaires/(web) surveys, and scales in the studies. We have full control of all primary data and we agree to allow the journal to review their data if requested. We state that we have consented to participate. All authors declared that they have not been exempt from the requirement and they all approved to submit this article to Global Spine Journal.
Acknowledgment
We thank the members of Chinese Society for the Study of the Lumbar Spine and Chinese Study Group of Lateral Lumbar Interbody Fusion who participated as panelists.
Author Contributions
The authors Yong Hai and Jingwei Liu contributed equally to this study and they are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.