
Abstract
Study Design
Meta-analysis.
Objective
To compare the effectiveness of postoperative pain control between erector spinae plane block (ESPB) and thoracolumbar interfascial plane (TLIP) block in lumbar spine surgery.
Methods
PubMed, Embase, and MEDLINE electronic databases were searched for articles containing randomized controlled trials (RCTs) published between January 1900 and January 2024. We extracted the postoperative mean pain score, the first 24-h postoperative morphine consumption, and their standard deviation from the included studies. Meta-analysis was performed using the functions available in the metafor package in R software. We pooled continuous variables using an inverse variance method with a random-effects model and summarized them as standardized mean differences.
Results
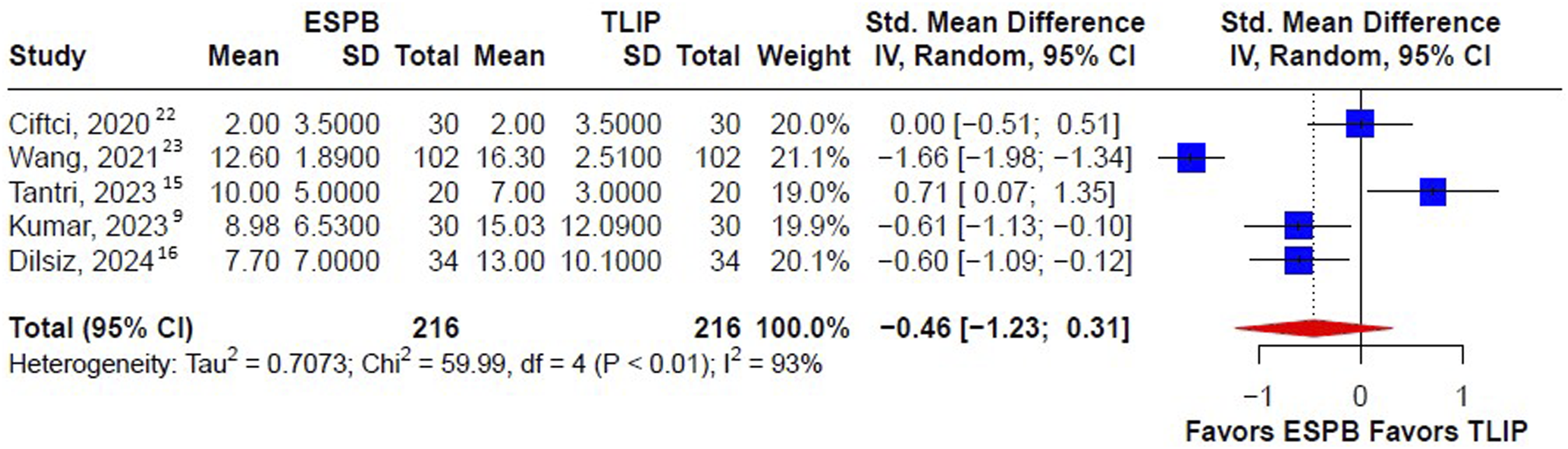
Five RCTs that directly compared the ESPB and TLIP block in lumbar spine surgery were included, enrolling 432 participants randomly into the two groups with 216 participants in each group. The pooled analyses showed that there was no significant difference between the ESPB and TLIP groups in terms of lower pain scores during the early (1 h) (standardized mean difference [SMD] −1.49, 95% confidence interval [CI], −3.10; 0.11), middle (12 h) (SMD −3.12, 95% CI, −6.86; 0.61), and late (24 h) (SMD −1.38, 95% CI, −3.01; 0.24) postoperative periods. There was also no significant difference in the first 24-h postoperative morphine equivalent consumption between the ESPB and TLIP groups (SMD −0.46 mg, 95% CI −1.23; 0.31).
Conclusion
No significant difference was observed between the ESPB and TLIP block in terms of postoperative pain control and 24-h morphine equivalent consumption for lumbar spine surgery.
Keywords
Introduction
With the aging of the general population and the rising prevalence of degenerative spinal diseases, the number of spinal surgeries performed has increased. 1 Although spinal surgery aims to alleviate patient discomfort, postoperative pain is inevitable, which increases the risk of perioperative complications.2-4 Therefore, the severity of postoperative pain substantially impacts patient recovery and satisfaction. Several studies 5 have reported using regional anesthetic techniques in spinal surgery to mitigate postoperative pain. The application of adjunctive regional anesthetic techniques enables healthcare professionals to provide targeted pain relief, reduce reliance on systemic opioids, and improve patient outcomes, which may facilitate early mobilization and rehabilitation. 6
Considerable research7-9 has compared postoperative pain-related outcomes among patients receiving different types of perioperative regional anesthesia, including epidural anesthesia, spinal anesthesia, and peripheral nerve blocks. Among these techniques, erector spinae plane block (ESPB) and thoracolumbar interfascial plane (TLIP) block are two widely studied regional anesthetic techniques since 2016.10,11 Both methods involve ultrasound-guided localization of the injection site and the administration of local anesthetics at the spinal level. ESPB involves injecting anesthetics into the erector spinae muscles, providing extensive cranial and caudal coverage along the paraspinal muscles to block the ventral and dorsal rami at multiple vertebral levels. 8 In contrast, the TLIP block involves injecting anesthetics into the interfascial area between the longissimus and iliocostalis muscles to reduce the risk of neuraxial side effects by targeting the dorsal rami. 12 Tseng et al 13 posited that intraoperative washout of anesthetics may occur in ESPB because the injection site is within the surgical field. Conversely, injecting the local anesthetics into the interfascial plane between the paraspinal muscles in the TLIP block allows for prolonged retention of anesthetics.
A previous network meta-analysis 14 comparing regional anesthetic techniques for lumbar spine surgery concluded that the ESPB and TLIP block were the two most effective methods. In particular, the statistical results indicated that the TLIP block was superior to the ESPB for pain management after spinal surgery. However, this meta-analysis included only two studies that directly compared the ESPB and TLIP block. Recently, three additional RCT9,15,16 directly compared the ESPB and TLIP block after spinal surgery. To clarify the comparative effectiveness of these two regional anesthetic techniques, we conducted an updated pairwise meta-analysis of the ESPB and TLIP block in alleviating postoperative pain during spinal surgery.
Methods
Study Selection
We comprehensively searched the PubMed, Embase, and MEDLINE electronic databases between January 1900 and January 2024, with no language restrictions to ensure inclusivity. Two investigators independently searched and identified relevant studies for potential inclusion. Any discrepancies were resolved by consensus among the investigators or by consulting a senior reviewer. Additional details regarding the search strategy and specific search terms are provided in eMethod 1. Our study was registered on the PROSPERO online platform to ensure transparency and accessibility of our research protocol. (CRD42023445556)
Eligibility Criteria
Articles meeting the following criteria were included: (1) randomized controlled trials, (2) studies of adults undergoing lumbar spine surgery, and (3) studies reporting comparative clinical outcomes for the ESPB and TLIP block. Studies were considered ineligible if they fell into categories such as review articles, case reports, case series, retrospective data analyses, or nonrandomized prospective studies. Additionally, if the data provided were either unavailable or irrelevant to the intended meta-analysis, the studies were excluded.
Data Extraction
Two investigators independently extracted the following data from the eligible studies: first author’s last name; publication year; sample size; intraoperative analgesia; and postoperative pain score at 1-h, 12-h, and 24-h postoperative morphine equivalent consumption (mg).
Quality Assessment
Two investigators independently used the Risk of Bias 2 (RoB 2.0) 17 tool to critically appraise the included literature. Any item on which the assessors did not reach consensus was discussed with a third investigator.
Statistical Analysis
Statistical analyses were performed using the functions available in the metafor package in the R software (eMethod 2, R Foundation for Statistical Computing, New Zealand). 18 The clinical outcome of interest was the postoperative pain score at the early (1 h), middle (12 h), and late (24 h) periods, as well as 24-h postoperative morphine consumption. We extracted the postoperative mean pain score and standard deviation from the included studies, pooled them using an inverse variance method, and summarized the results as standardized mean differences. The results presented as medians (interquartile ranges) were converted to means (standard deviations) using the method described by Chi et al. 19 The restricted maximum likelihood method was used as a heterogeneity estimator to conduct random-effects meta-analyses because between-trial variance was inevitable. 20 Effect sizes were presented with corresponding 95% CIs. Heterogeneity was assessed using the I2 statistics proposed by Higgins and Thompson, with I2<25%, 25% < I2<50%, and I2>50% indicating low, moderate, and high heterogeneity, respectively. 21
Results
Study Selection
Our initial search yielded 1997 results. After screening the titles and abstracts, 109 articles were eligible for full-text article assessment. Subsequently, five studies met our inclusion criteria and were analyzed for postoperative mean pain score and 24-h postoperative morphine equivalent consumption. The selection process was summarized in Figure 1. PRISMA flowchart diagram. We initially extracted 1997 potential articles. Screening of the titles and abstracts based on the inclusion and exclusion criteria yielded 109 full-text articles. Eventually, five studies were included for qualitative and quantitative syntheses. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.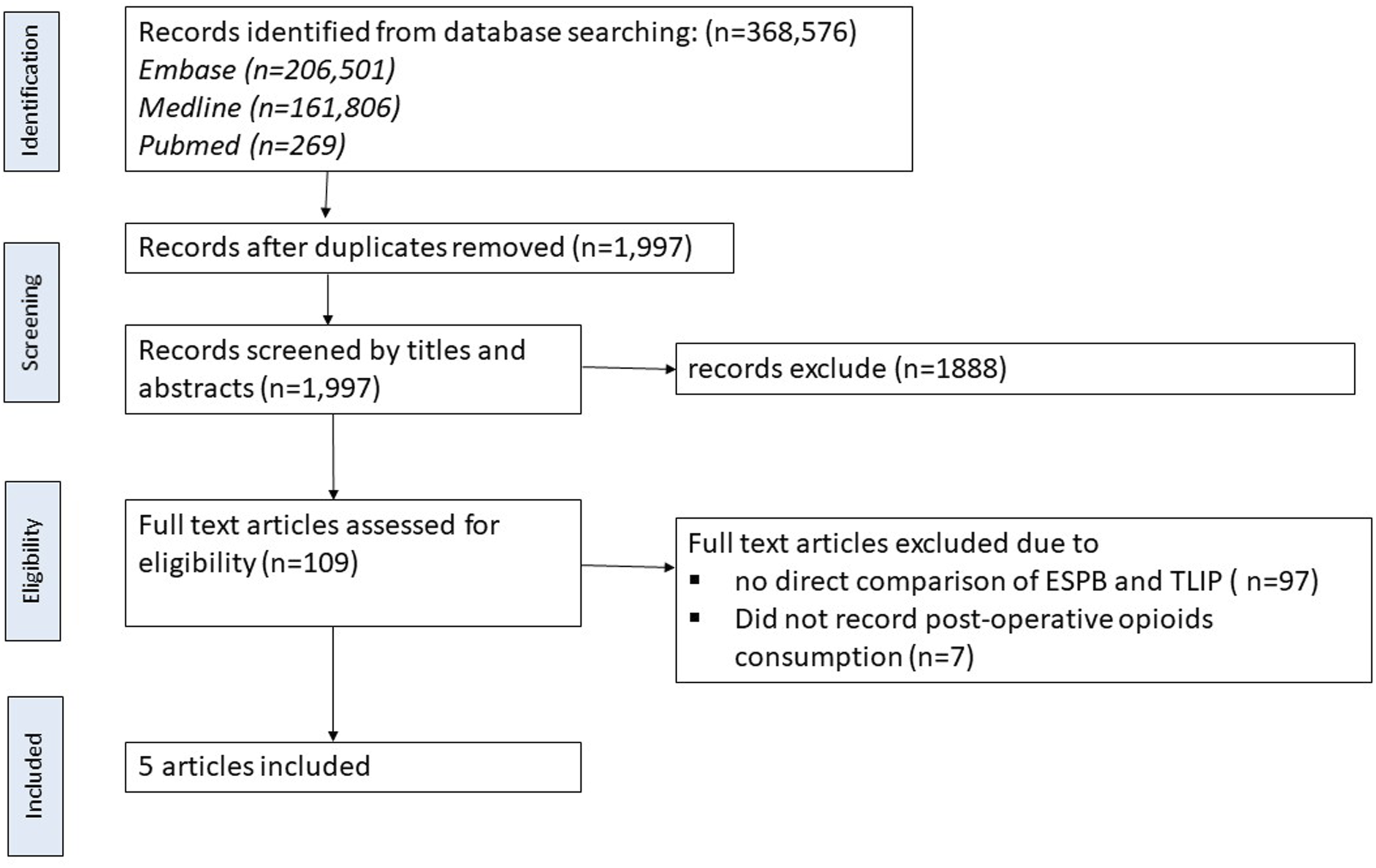
Characteristics of the Included Studies
Study Characteristics.
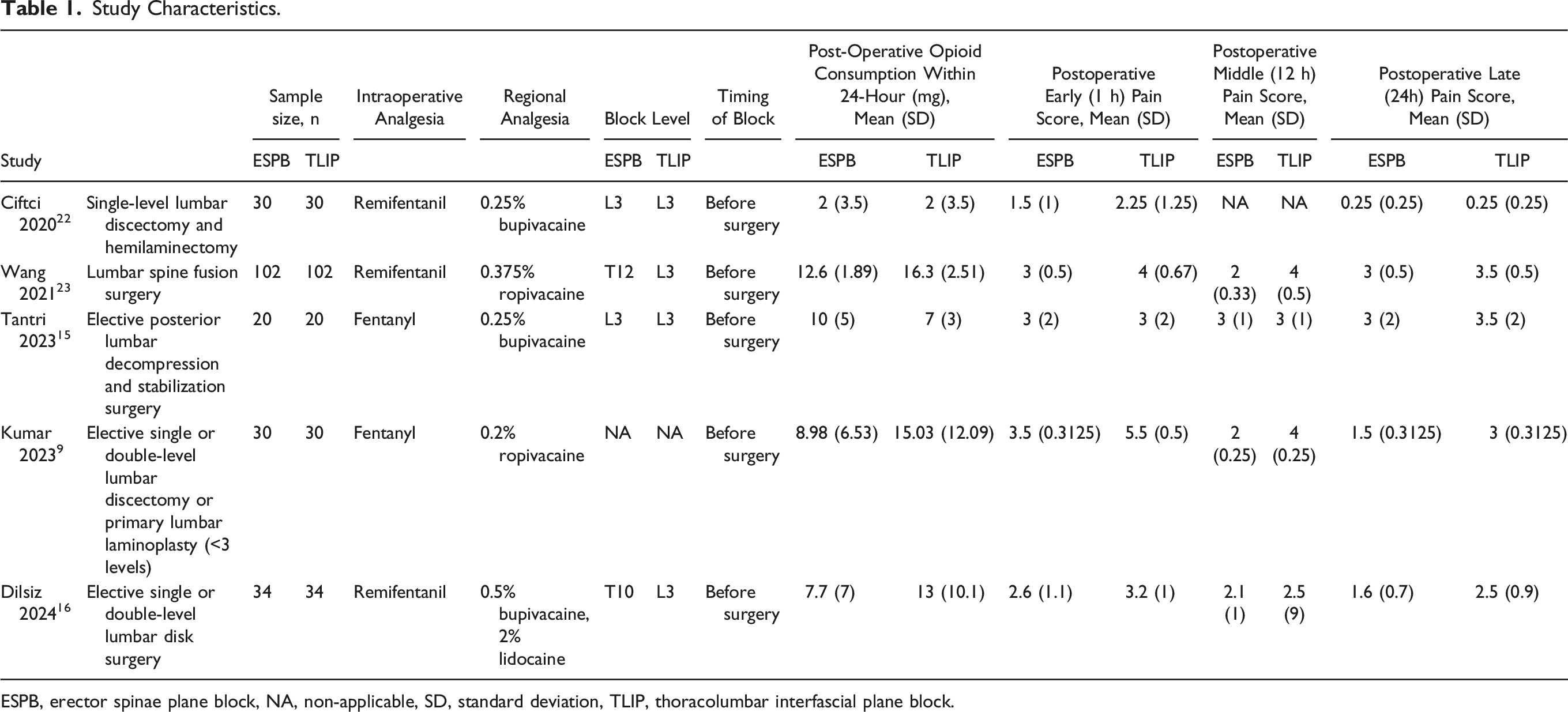
ESPB, erector spinae plane block, NA, non-applicable, SD, standard deviation, TLIP, thoracolumbar interfascial plane block.
Quality Assessment of the Included Studies
After conducting a quality assessment of the included studies using RoB 2.0, we observed that two studies were classified as having a high risk of bias, whereas the remaining three studies had some concerns regarding the risk of bias. A graphical representation of the risk of bias assessment is shown in Figure 2. Quality assessment of included studies. Quality assessment was conducted using RoB 2.0, a revised Cochrane risk-of-bias tool for randomized trials. The risk of bias in each domain is classified as high, some concerns, and low, as shown in the legends. Two studies were classified as having a high risk of bias (Ciftci 2020
22
: bias due to deviation from the intended intervention and bias in selection of the reported result; Wang 2021
23
: bias in deviation from the intended intervention, measurement of the outcome, and bias in selection of the reported result), whereas the remaining three had some concerns regarding the risk of bias (three studies, Tantri 2023,
15
Kumar 2023,
9
and Dilsiz 2024,
16
had bias in deviation from the intended intervention, measurement of the outcomes, and selection of the reported result).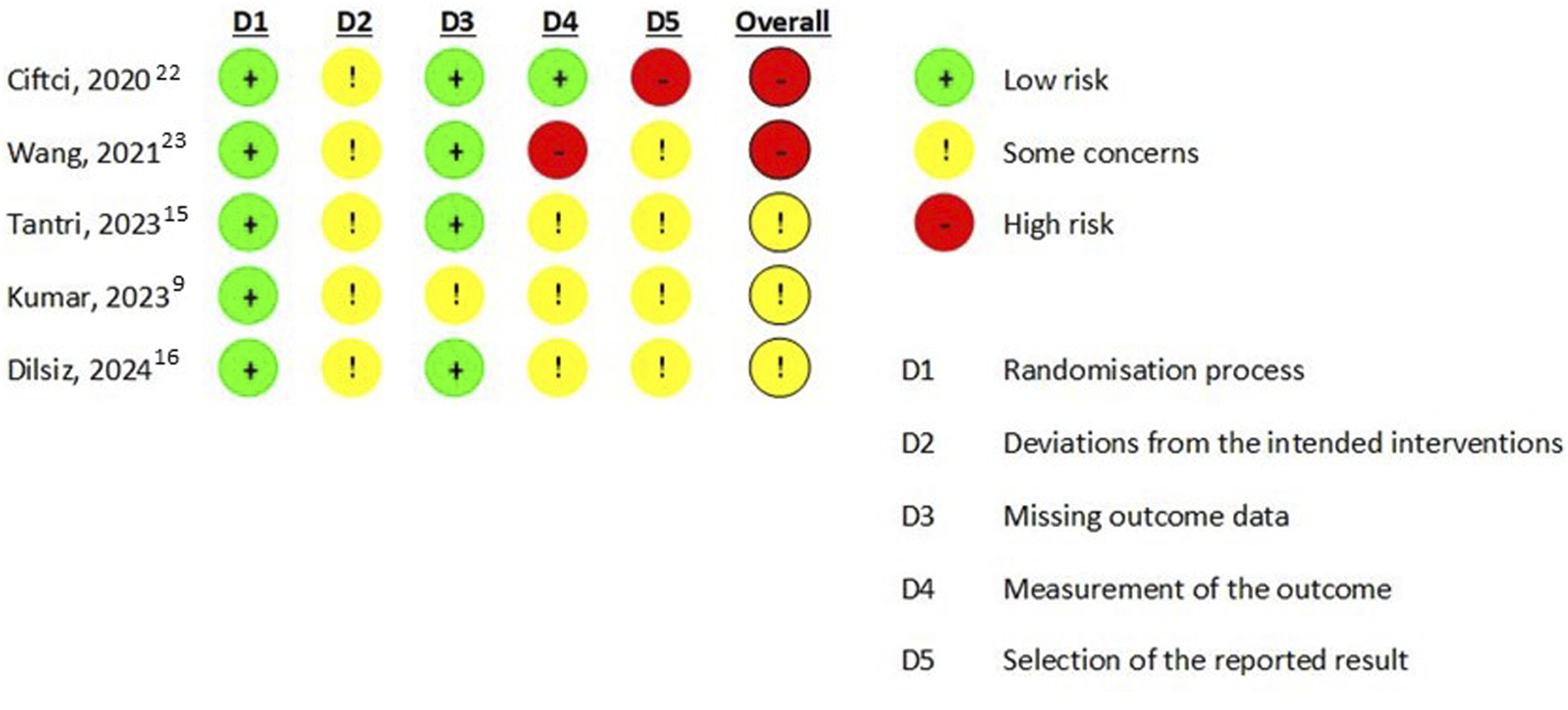
Postoperative Pain Scores and Morphine Equivalent Consumption
Postoperative pain scores were analyzed and compared between the TLIP block and ESPB groups at three different time points: early (1 h), middle (12 h), and late (24 h). The results and findings are shown in Figure 3. The pooled analyses showed that there was no significant difference between the ESPB and TLIP groups in terms of lower pain scores during the early (SMD -1.49, 95%, CI −3.10; 0.11), middle (SMD −3.12, 95% CI, −6.86; 0.61), and late (SMD −1.38, 95% CI, −3.01; 0.24) postoperative periods. Moreover, as shown in Figure 4, there was no difference in the first 24-h postoperative morphine equivalent consumption between the ESPB and TLIP groups (SMD −0.46 mg, 95% CI -1.23; 0.31). A summary of the findings of this meta-analysis was presented in Table 2. Forest plot of postoperative pain score (VAS) among patients receiving the ESPB vs the TLIP block at three time periods: (a) early (1 h), (b) middle (12 h), and (c) late (24 h). The forest plot shows the postoperative pain score at three time points among patients undergoing lumbar spine surgery who received the TLIP block or the ESPB as regional anesthesia. The size of the squares is proportional to the weight of each study. The results are summarized using the standard mean difference with a corresponding 95% CI. The horizontal lines indicate the 95% CI of each study, and the red diamonds indicate the pooled estimate with 95% CI. ESPB, erector spinae plane block; TLIP, thoracolumbar interfascial plane; CI, confidence interval. Forest plot of 24-h postoperative opioid consumption among patients who received the TLIP block and the ESPB. All opioids were converted to i.v. morphine doses equivalent (i.v. morphine 1 mg = i.v. fentanyl 10 μg = i.v. sufentanil 2 μg = i.v. tramadol 10 mg = i.v. pethidine 7.5 mg). The size of the squares is proportional to the weight of each study. The result is summarized using the standard mean difference with a corresponding 95% CI. The horizontal lines indicate the 95% CI of each study, and the red diamond indicates the pooled estimate with 95% CI. Summary of Meta-Analyses.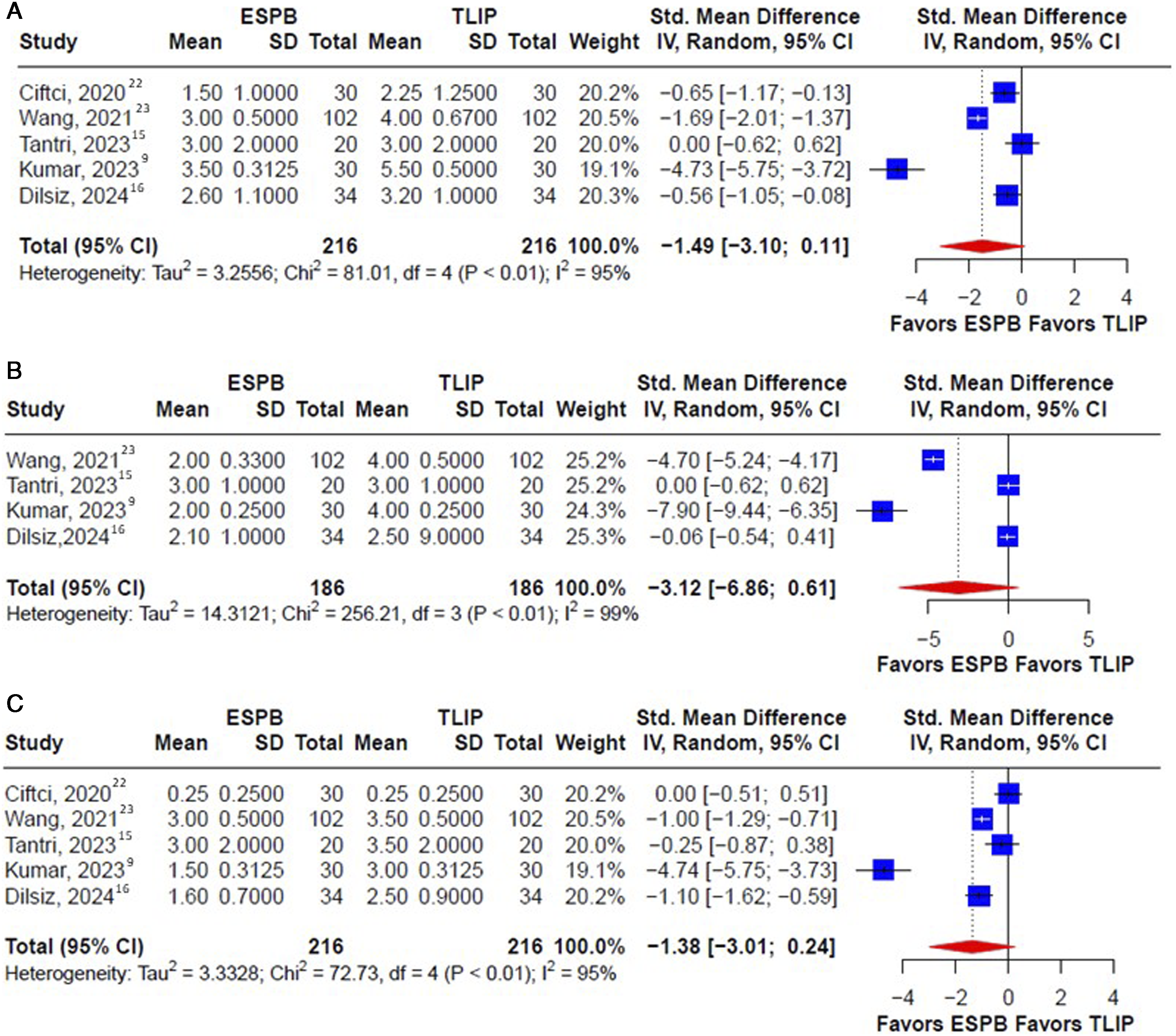

Discussion
This meta-analysis aimed to compare the effectiveness of the TLIP block and the ESPB in postoperative pain control among patients undergoing lumbar spine surgery. Our findings revealed no significant differences between the TLIP block and ESPB in terms of postoperative pain scores or morphine equivalent consumption within the first postoperative 24 h. A study by Hong et al, 14 including 34 RCTs, suggested that the TLIP block demonstrated the highest analgesic efficacy following lumbar spine surgery based on measures of postoperative opioid consumption and pain scores, whereas ESPB ranked second in terms of efficacy. However, most studies included in their analysis compared a single pain control technique with a control group, limiting the number of studies to direct pairwise comparisons between different pain control interventions. Their network meta-analysis primarily relied on indirect comparisons, whereas our study specifically focused on direct head-to-head comparisons between the TLIP block and ESPB. Our research revealed no significant differences in the clinical outcomes between the two pain control methods.
Numerous studies24-28 have explored the potential advantages of regional anesthesia, particularly focusing on two specific techniques, the ESPB and TLIP block, within the context of lumbar spine surgery. RCTs examining the effects of ESPB compared with control groups have consistently demonstrated superior outcomes in terms of pain reduction and postoperative morphine consumption. ESPB exhibited a reassuring safety profile, with no reports of severe complications associated with this technique.23-25 Similarly, the efficacy of the TLIP block has been substantiated in multiple prospective studies, revealing significantly lower postoperative pain scores and reduced morphine consumption compared with control groups or wound infiltration techniques.26,27 Nonetheless, the current literature offers limited information regarding a direct comparison of the effectiveness of the ESPB and TLIP block. 29 Our extensive literature search yielded only five RCTs9,15,16,22,23 that prospectively investigated and compared the effectiveness of these block techniques.
In the present study, all included RCTs directly compared the ESPB and the TLIP block, given that direct comparisons are reportedly superior to comparisons with controls. In general, the postoperative pain scores were evaluated at different time points in all the included trials. We extracted the postoperative pain scores at 1, 12, and 24 h and the 24-h morphine equivalent consumption for the statistical analyses. These objective parameters enable comparisons of effectiveness between different regional anesthetic methods. The high heterogeneity in the meta-analysis may be associated with the lack of standardized methodologies for conducting the trials. For example, a thoracic level regional block was performed despite participants undergoing lumbar spine surgeries. In particular, the studies by Wang et al 23 and Dilsiz et al 16 involved ESPB at the T12 and T10 levels, respectively, and the TLIP block at the L3 level. Meanwhile, Ciftci at al. 22 and Tantri at al. 15 administered the injection at the L3 level regardless of the regional anesthetic method. It is imperative to establish a standardized protocol for determining the appropriate block level based on the surgical site to optimize the analgesic efficacy of the technique.
Additionally, participants in different studies might have received postoperative analgesics other than opioids, such as diclofenac and paracetamol, in accordance with institutional protocols. The administration of these analgesics could introduce bias into the evaluation of postoperative pain scores. Furthermore, even though patient-control analgesia was used in all the included studies, the protocol employed also varies across the studies, for instance, the regimen, continuous basal infusion, and hourly maximal dose. This might have caused the notable difference in 24-h postoperative morphine consumption due to different pain control effectiveness. Ciftci et al 22 demonstrated a lower postoperative morphine consumption than the other studies owing to a low dose of morphine released during each compression. Moreover, it is important to acknowledge the variability in the regimen and dosage of anesthetics utilized in nerve block procedures across different studies. Such variations could influence the outcomes and interpretation of the efficacy of the nerve block interventions. The aforementioned differences contributed to the substantial heterogeneity after pooling the results. Rigorous methodologies must be employed to conduct trials comparing these regional block techniques and establish credible evidence for the benefits of these techniques.
Nevertheless, this study has several strengths. Most importantly, we included recently published RCTs that made pairwise comparisons between the TLIP block and ESPB using credible study endpoints, such as postoperative pain score and 24-h opioid consumption. Through this meta-analysis, we intend to motivate future research to directly compare these blocks with a more rigorous and standardized methodology and provide clinical implications from an evidence-based perspective.
Limitations
This meta-analysis had several limitations. First, only five studies were included in the analysis. This limited sample size reduced the generalizability of the findings and may have affected the statistical power of the analysis. Second, there were variations in the methods and data presentation used to compare postoperative pain among the included studies. Each study included in the analysis employed different approaches and formats to assess and report pain outcomes. This heterogeneity in methodology and data presentation can introduce bias and make it challenging to accurately synthesize and compare the results. Third, the meta-analysis included articles focusing on different spinal surgical techniques and did not specify whether minimally invasive approaches were used, which may have influenced the intensity of postoperative pain. Finally, long-term differences in pain scores between these procedures were not reported. We hope to include related follow-up data in future studies.
Conclusion
Both the ESPB and TLIP block can effectively alleviate postoperative pain after spinal surgery. This meta-analysis indicated no statistically significant difference between the ESPB and TLIP block in terms of postoperative pain control and 24-h morphine equivalent consumption for lumbar spine surgery. However, it is crucial to consider heterogeneity in study designs especially the block level and institutional anesthetics and postoperative pain management protocol.
Supplemental Material
Supplemental Material - Erector Spinae Plane Block Versus Thoracolumbar Interfascial Plane Block in Lumbar Spine Surgery: A Meta-Analysis of Randomized Controlled Trials
Supplemental Material for Erector Spinae Plane Block Versus Thoracolumbar Interfascial Plane Block in Lumbar Spine Surgery: A Meta-Analysis of Randomized Controlled Trials by Wei-Thing Khor, Yu Chang, Chih-Hao Tien, Liang-Yi Chen, Hao-Hsiang Hsu, Pang-Shuo Perng, Chia-En Wong, Heng-Juei Hsu, and Jung-Shun Lee, in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated/analysed during this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.