
Abstract
Study design
Prospective, randomized control study.
Objective
To assess the safety and efficacy of fluoroscopy-guided vs ultrasound-guided Erector Spinae Plane Block (ESPB) for perioperative analgesia in lumbar fusion surgery.
Materials and Methods
66 patients requiring single-level lumbar fusion were randomized into 2 groups. One group had fluoroscopy-guided ESPB by the surgeon (Fluoro-ESPB group) and the other group had Ultrasound-guided ESPB by the anesthetist (USG-ESPB). Demographic details, intraoperative parameters (perioperative total opioid consumption, muscle relaxants used, heart rate, blood pressure), and postoperative parameters (VAS score, alertness, satisfaction score) were recorded and analyzed.
Results
During the initial 48 hours following the surgery, both groups provided good perioperative analgesia, and reported very low and comparable postoperative pain scores (VAS scale). The mean VAS score was 2.7 ± 0.5 in the Fluoro-ESPB group and 2.7 ± 0.5 in the USG-ESPB group (P = 0.91). The average time taken to deliver the block in the Fluoro-ESPB group (3.01 ± 0.97 mins) was significantly less than in the USG-ESPB group (4.74 ± 1.49 mins) (P = 0.00). The total perioperative opioid consumption (TOC), total intraoperative muscle relaxant consumption, and intraoperative blood loss were similar in both groups (Fluoro- ESPB, USG ESPB) (P > 0.05). The postoperative MOASS score was consistently high across both groups. The satisfaction scores were high and comparable (P = 0.403).
Conclusion
The fluoroscopy-guided ESPB is a safe and effective alternative to the traditional ultrasound-guided technique. It can be performed by the surgeon, reducing overall procedure time, and improving workflow.
Introduction
Lumbar spinal fusion procedures are commonly performed for various spinal disorders, with degenerative diseases being the most common indication.1,2 The total number of spinal fusion procedures has been increasing because of the growing elderly population and rising cases of lumbar degenerative diseases over the past few decades. 3
Lumbar fusion, a major surgery involving extensive muscle dissection, results in significant pain during the acute postoperative period.1,4 These surgeries necessitate increased opioid usage before, during, or after the surgery, which can result in a slower recovery from anesthesia and higher postoperative complications, especially in older patients. Pre-existing pain, along with long-term use of painkillers and opioids, can alter pain sensitivity, which makes managing postoperative pain more difficult. 5 Effective post-operative pain management can help with early movement and better recovery, reducing hospital stays and lowering the risk of complications such as deep vein thrombosis, pulmonary complications, and chronic pain syndromes.6,7
NSAIDs, opioids, and acetaminophen form the mainstay of peri-operative multi-modal analgesia. 8 It is achieved by combining different analgesics that act through different mechanisms to reduce the adverse effects. 9 Though very effective, their usage is associated with potential side effects like renal impairment, gastric ulcer, cardiovascular adverse events, liver dysfunction, dizziness, nausea, urinary retention, altered mental status, ileus, and respiratory depression.10,11
Regional pain control techniques, such as the thoracolumbar interfascial plane block (TLIP) and the erector spinae plane block (ESPB), are emerging as effective perioperative analgesia options for spine surgery12-14 due to their ease of application, low rate of complications, and ability to effectively relieve postoperative pain, resulting in reduced opioid usage. 15 In patients undergoing single-level lumbar fusion surgery, it reduces opioid usage and minimizes blood loss. 15
Traditionally, ESP blocks have been administered by anesthetists using ultrasound guidance. The cocktail is infiltrated over the transverse process of lumbar vertebrae just deep to the erector spinae muscle plane. However, this approach often requires the involvement of multiple physicians. Surgical-level marking by the surgeon is always necessary before planning the incision in lumbar fusion surgery. Hence, surgeons can use fluoroscopy to identify the transverse process in the AP image and deliver the drug. 16 Administering the ESP block simultaneously with surgical level marking can reduce overall procedure time and costs and improve workflow. While the ultrasound-guided technique requires a high level of skill and expertise from the anesthetist, Fluoroscopy-guided delivery of drugs offers a more straightforward approach for spine surgeons who are well-versed in the spinal anatomy. The limitations of ultrasound-guided ESP block in visualizing the target correctly in obese patients have been well-documented. 17 Fluoroscopy’s ability to penetrate through tissue and provide detailed imaging makes it particularly beneficial for patients with obesity.
There have been few studies demonstrating the effective postoperative analgesia produced by fluoroscopic guided erector spinae plane block.17-20 To our knowledge, this is the first randomized controlled clinical study comparing the fluoroscopic guided and ultrasound-guided erector spinae plane block in single-level lumbar fusion surgery, considering both intra-operative and postoperative parameters.
We hypothesize that fluoroscopic guidance provides comparable pain relief with reduced opioid consumption. The primary outcomes are perioperative pain control and total opioid consumption, and secondary outcomes include intraoperative blood loss, postoperative sedation, time to mobilization, hospital stay, and patient satisfaction, which would be evaluated.
Materials and Methods
This was a prospective, randomized controlled study conducted at a tertiary spine care center with approval from the institutional review board (Ref.No.IRBITA/GH/ORTHO/2024/009). Written informed consent was obtained from all participants. The study included patients over 20 years of age undergoing single-level open lumbar fusion surgery (TLIF) for degenerative listhesis/lytic listhesis or lumbar canal stenosis with instability. Patients who had local infection, bleeding disorders, poor skin conditions, previous spine surgery, systemic infection, malignancy, spine injury, or who refused to give consent were not included in the study.
A total of 71 consecutive patients were assessed for eligibility. Five patients were excluded, and the remaining were randomly assigned to either the Fluoroscopic guided ESPB (Fluoro-ESPB) group or the Ultrasound-guided ESPB (USG-ESPB) group using computer-generated numbers. The allocation details of the study have been reported per the consolidated standards of reporting trials (CONSORT) guidelines for reporting randomized trials (Figure 1). CONSORT flow diagram.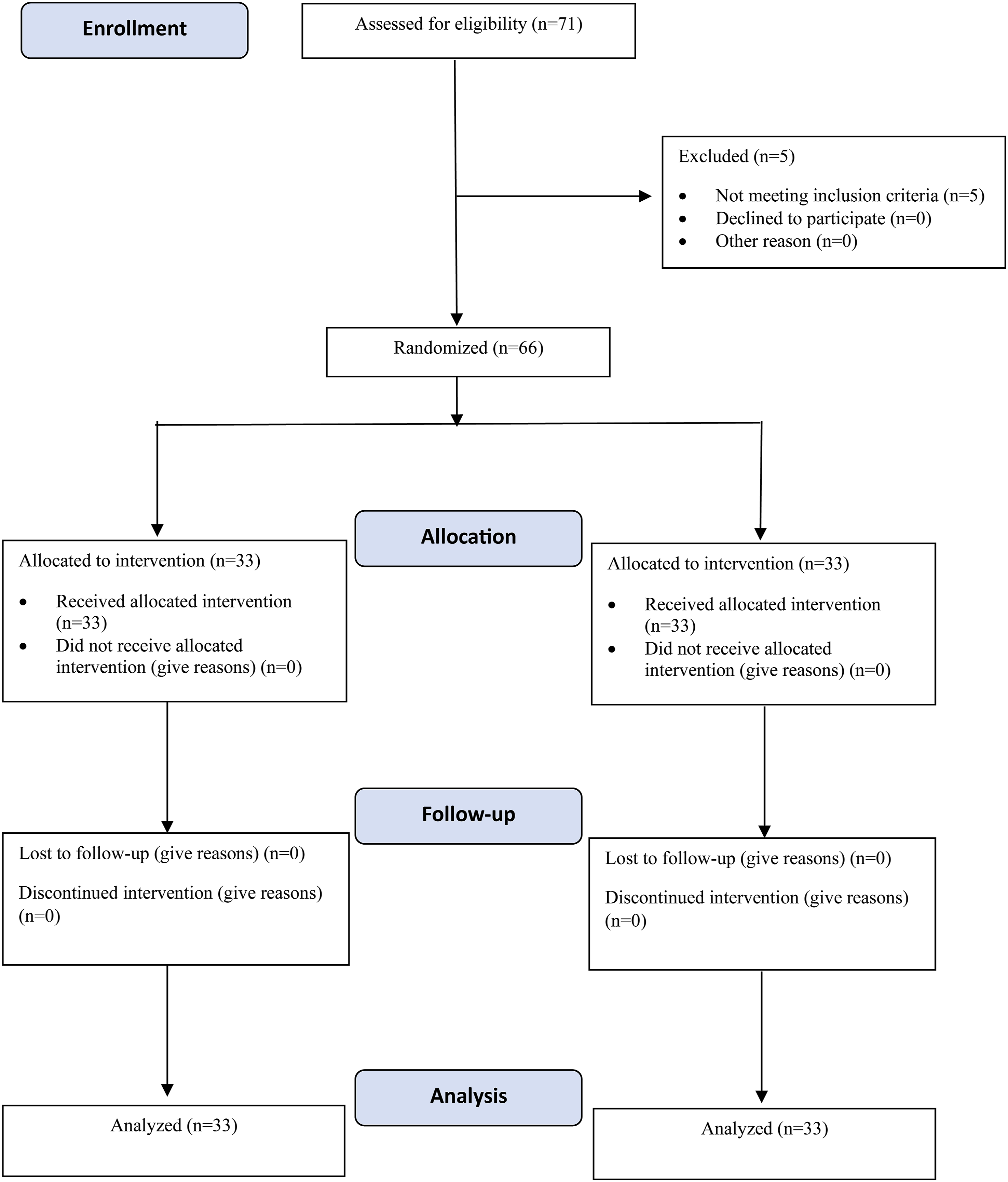
Patients in both groups were given 75 mg of Pregabalin and 1gm of Acetaminophen on the night before surgery and underwent standard general anesthesia techniques.
Patients were randomly assigned to 1 of 2 groups. Out of 66 patients, 33 received bilateral Fluoroscopy-guided ESPB by 2 senior spine surgeons with more than 15 years of experience, and 33 received bilateral Ultrasound-guided ESPB by 2 senior anesthetists with more than 15 years of experience. Both groups received the same standard technique of general anesthesia (GA). Induction of GA was initiated with titrated doses of Propofol, not exceeding 2 mg/kg. Fentanyl at 2mics/kg and Rocuronium at 0.6 mg/kg were used for intubation. GA was maintained with sevoflurane in a mixture of oxygen and nitrous oxide at a 50:50 ratio and titrated to a minimum alveolar concentration (MAC) of 1. Fentanyl was repeated at 1mics/kg at 1 hourly interval and 0.5mics/kg for breakthrough pain. Muscle relaxation was maintained with 1/5th of the intubating dose of rocuronium at 25-minute intervals.
Technique for Ultrasound-Guided Erector Spinae Block
Ultrasound-guided ESPB was performed using the method described by Goel et al. 15
Fluoroscopy Guided ESPB Technique
After administering general anesthesia, the patients were positioned in a prone position. The surgical area was disinfected, and the surgeon marked the surgical level under fluoroscopic guidance in the anteroposterior view. Under the same view, the transverse process (TP) of the target vertebra was visualized (Figure 2). A 23 G 90 mm Quincke’s spinal needle was inserted 1 cm lateral to the transverse process in a steep trajectory (10-20°) towards the transverse process. After contacting the TP, the needle was slightly retracted by 2 mm until its tip sat in the interfacial plane below the muscle. The block was administered by injecting 20 mL of 0.25% Bupivacaine after a negative aspiration test to avoid intravascular injection. The block was similarly administered on the other side. Fluoroscopy-guided ESPB technique (A) Placing the needle at the marked site, 1 cm lateral to transverse process (TP), and inserting it in a steep trajectory (10-20°) towards the TP (B) confirmation of needle position in Fluoroscopy (true AP view) (C) After contacting the TP, the needle was slightly retracted by 2 mm until its tip sat in the interfacial plane below the muscle and an anesthetic solution was injected after negative aspiration. (D) The block was similarly administered on the other side.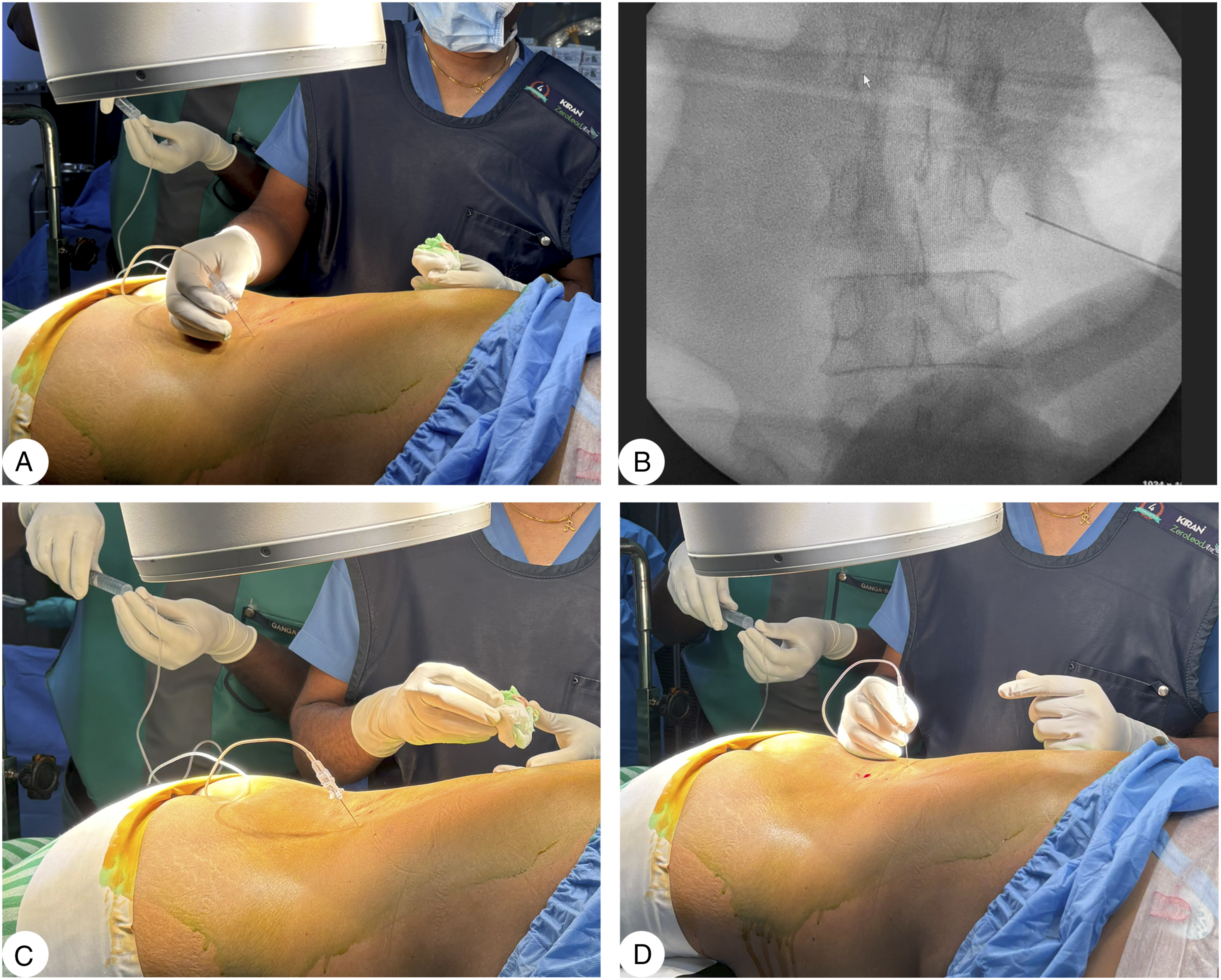
The bupivacaine used in this study was Anawin 0.25% (Bupivacaine Hydrochloride Injection IP), manufactured by Neon Laboratories Ltd., India. It was supplied as a 0.25% (2.5 mg/mL) injection solution. It contains Bupivacaine Hydrochloride IP (2.5 mg/mL), and Sodium chloride and water for injection in a preservative-free formulation.
The total consumption of Fentanyl and muscle relaxant (Rocuronium) was documented throughout the surgery. The amount of blood loss, duration of surgery, opioid usage, and muscle relaxant use were monitored during the surgery for all patients. After the surgery, analgesia was provided with 1gm of intravenous paracetamol every 6 hours along with pregabalin 75 mg once a day, with the first dose administered 12 hours after surgery. Rescue analgesia was administered when the visual analogue scale (VAS) was ≥5 in the form of fentanyl 1 mcg/kg body weight, with a minimum interval of 2 hours between doses.
Postoperative parameters including postoperative pain score using the Visual Analogue Scale (VAS), level of alertness using the Modified Observer’s Alertness/Sedation Score (MOASS), time to mobilization, the total amount of opioids consumed (TOC), and all complications were recorded for the first 48 hours after surgery. The information was recorded at 2-hour intervals for the first 4 hours, then at 4-hour intervals until the 12th hour, and finally at 12-hour intervals until 48 hours. All the patients also filled out a 10-point questionnaire (Total Satisfaction Score) at the end of 72 hours postoperatively.
Results
66 patients planned for single-level lumbar fusion (TLIF) surgery were enrolled in the study. Based on randomization, 33 patients were allocated into each group.
Demographic and Clinical Characteristics of the Groups
Demographic and Clinical Characteristics of the Groups.
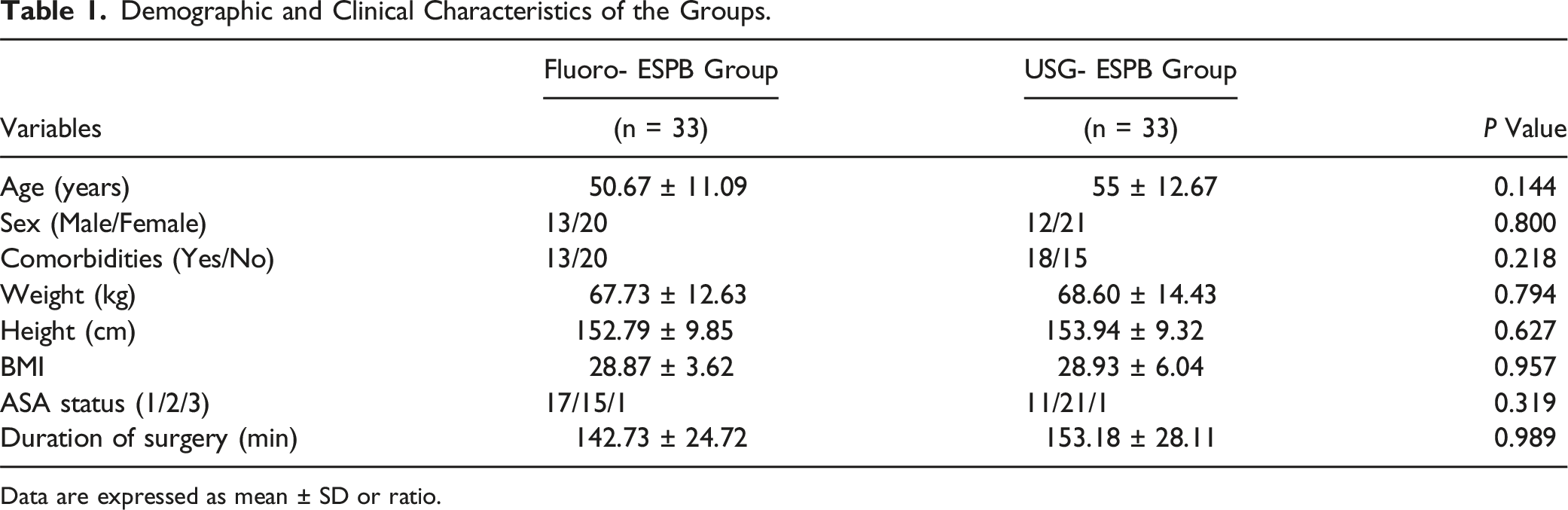
Data are expressed as mean ± SD or ratio.
Perioperative Analgesia
During the initial 48 hours following the surgery, both groups provided good perioperative analgesia and reported very low and comparable postoperative pain scores (VAS scale) (Figure 3). The mean VAS score was 2.7 ± 0.5 in the Fluoro-ESPB group and 2.7 ± 0.5 in the USG-ESPB group (P = 0.91). This suggests that both techniques were equally effective in managing postoperative pain. Comparison of VAS Score between the 2 Groups.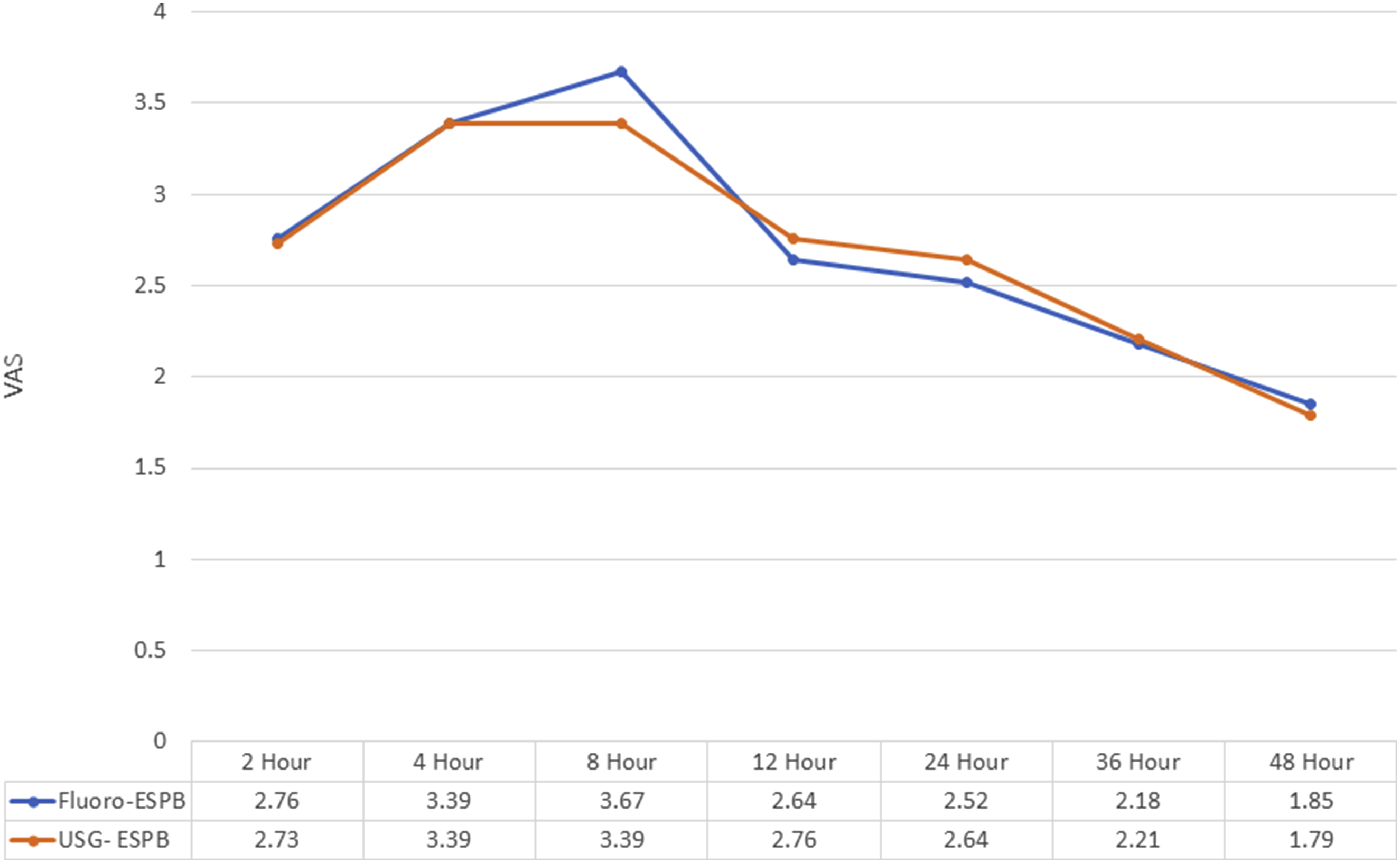
Time Efficiency
Primary and Secondary Outcome Parameters.
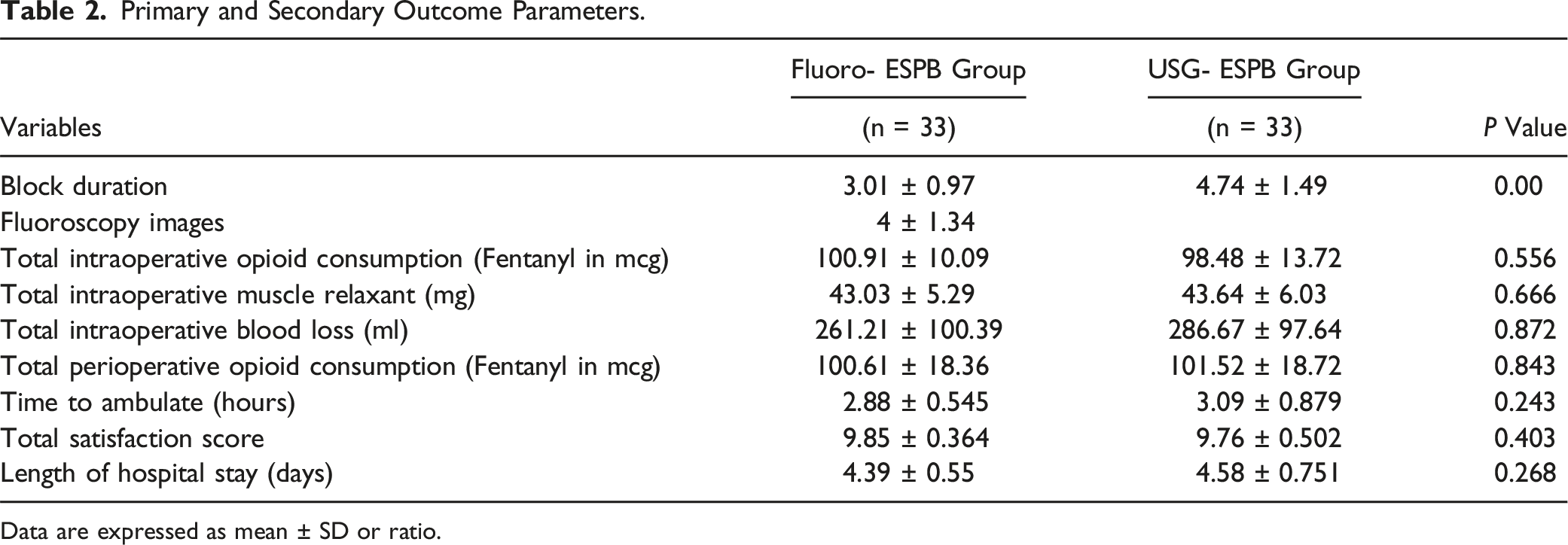
Data are expressed as mean ± SD or ratio.
Intraoperative Parameters
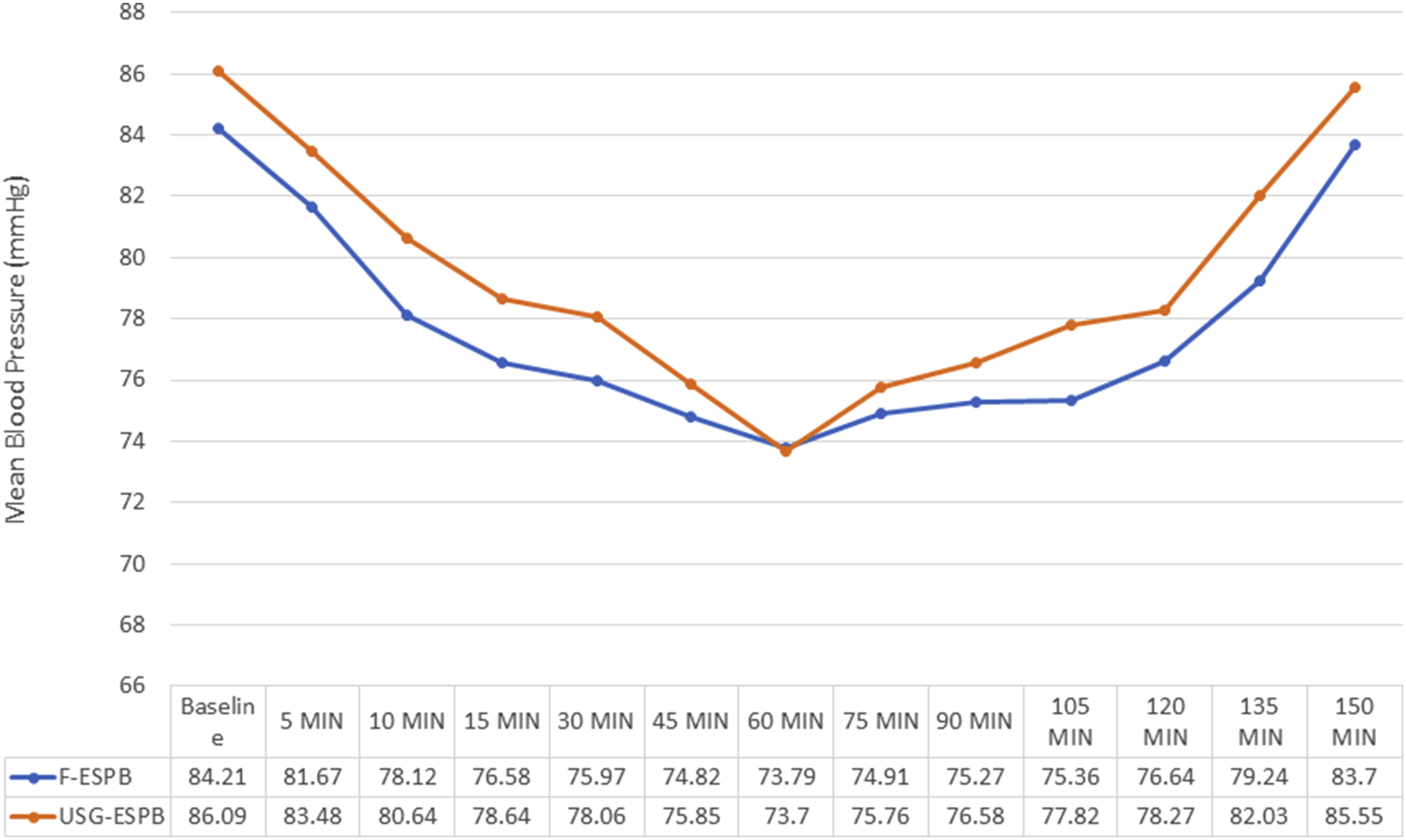
In the initial 48 hours after surgery, the total opioid consumption (TOC) was similar in both groups (Fluoro- ESPB, USG ESPB) at 100.61 ± 18.36 mcg and 101.52 ± 18.72 mcg respectively (P = 0.843). Additionally, the intraoperative consumption of total muscle relaxants was comparable between both groups, with Fluoro-ESPB at 43.03 ± 5.29 mg and USG-ESPB at 43.64 ± 6.03 mg (P = 0.666). The amount of intraoperative blood loss was 261.21 ± 100.39 mL in the Fluoro-ESPB Group and 286.67 ± 97.64 mL in the USG-ESPB Group, which was also similar (P = 0.872) as shown in Table 2. Furthermore, both groups experienced a similar decrease in hemodynamic parameters compared to the baseline (Figures 4, 5). Comparison of Intraoperative Heart Rate between the 2 groups. Comparison of Intraoperative Mean Blood Pressure between the 2 groups.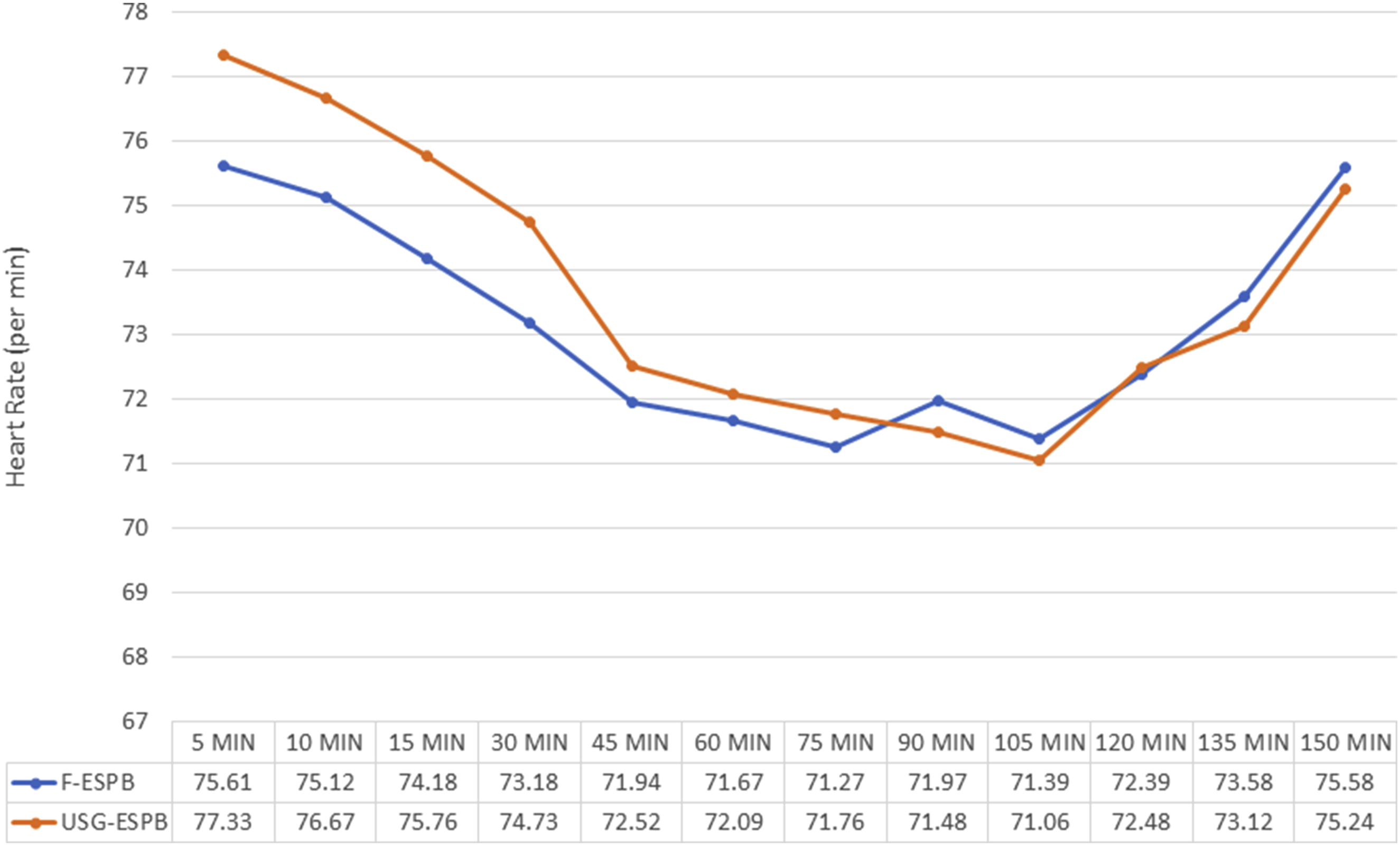
Post-Operative Parameters
The postoperative MOASS score was high and consistent across both groups, indicating similar levels of alertness (Figure 6). Both techniques reduced opioid consumption. Only 1 patient in the fluoro-ESPB group and 2 patients in the USG-ESPB group required an additional dose of fentanyl in the postoperative period. The mean time needed to ambulate was 2.88 ± 0.545 hours for the Fluoro-ESPB group and 3.09 ± 0.87 hours for the USG-ESPB group (P = 0.243). The satisfaction scores were comparable, with a mean value of 9.85 ± 0.36 for the Fluoro-ESPB group and 9.76 ± 0.50 for the USG-ESPB group (P = 0.403). The mean length of hospital stays was similar between the 2 groups, with 4.39 ± 0.55 days for the Fluoro-ESPB group and 4.58 ± 0.75 days for the USG-ESPB group (P = 0.268). Comparison of MOASS between the 2 groups.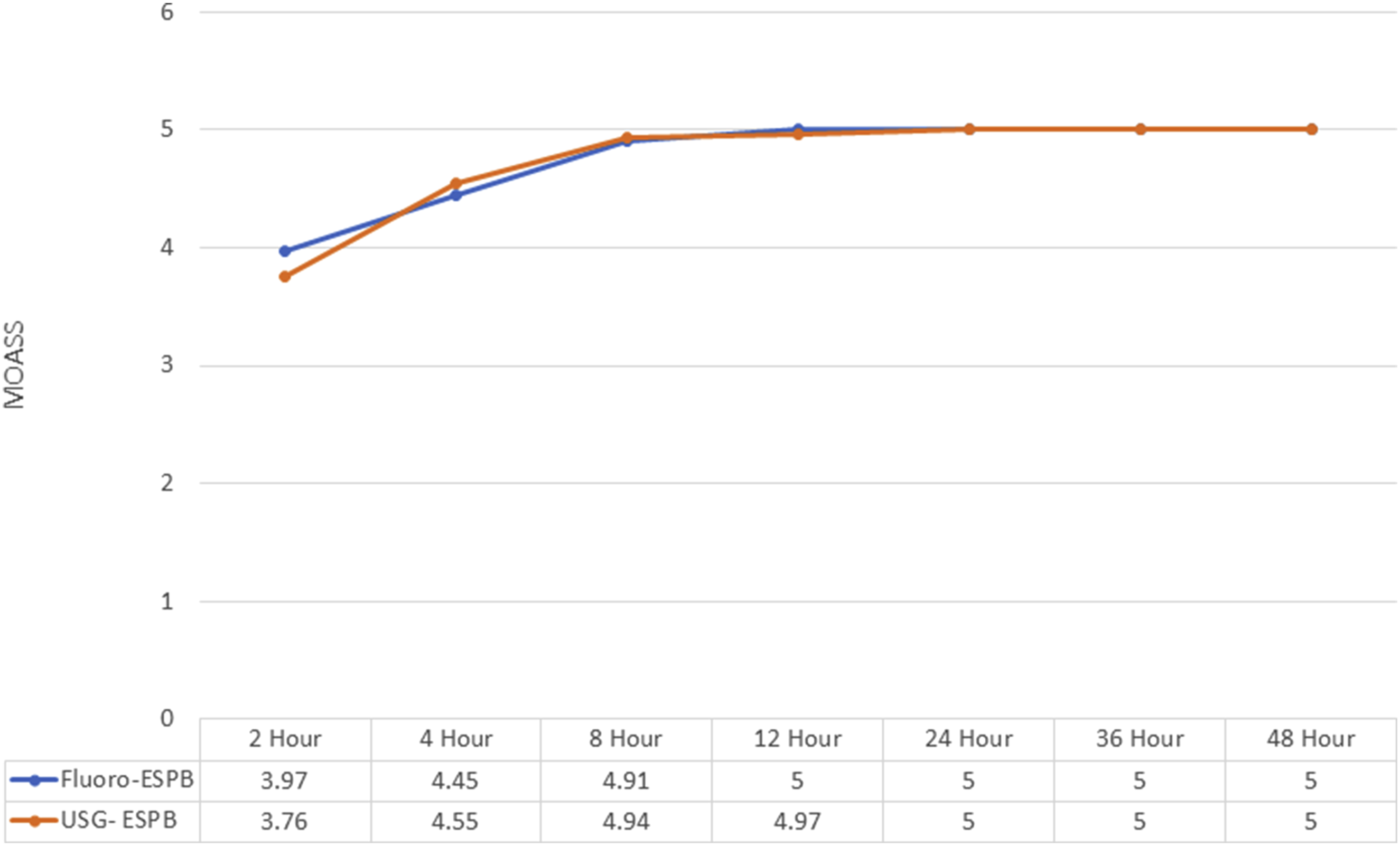
Three patients in the Fluoro-ESPB group and 3 patients in the USG-ESPB block groups developed nausea and vomiting in the postop period requiring medication. We did not encounter any block-related complications in any of our patients.
Discussion
Effective postoperative pain management is crucial following spinal fusion surgery to promote early mobilization and reduce postoperative mortality and morbidity. The most commonly used method for managing postoperative pain following lumbar fusion surgery is opioid-based patient-controlled intravenous analgesia. 21 However, it is associated with adverse effects. 10 Therefore, for effective pain management, regional applications such as epidural, spinal, and plane blocks are more rational than using drugs with systemic effects. New evidence suggests that targeted fascial plane nerve blocks can significantly improve pain management during posterior spine surgeries. 22 Among them, the erector spinae plane block (ESPB) has been found to provide effective pain relief for patients undergoing spine surgeries and was originally developed to manage chronic thoracic neuropathic pain. 23
Studies by Goel et al, 15 Sing et al, 24 Liu et al, 25 have demonstrated the efficacy of the ESP block for postoperative analgesia after lumbar fusion surgery compared with conventional (opioid-based) multimodal analgesia and resulting in reduced opioid consumption. All these studies used the traditional ultrasound-guided technique for delivering the block by the anesthetist. This technique’s limitations include relying on the operator’s skills, which necessitates training and expertise. It may be challenging to obtain clear images in patients with obesity, anatomical variations, or poor acoustic windows.26,27 Additionally, the ultrasound technique has limited depth perception, which could result in suboptimal needle placement. Transient motor and sensory deficits following ultrasound-guided ESPB have been reported in the literature.28,29 Fluoroscopy-guided delivery of erector spinae plane block is a newer technique. Studies by Sonbol et al, 19 Owen et al, 16 Robertson et al, 20 and Patel et al 18 demonstrated its efficacy in lumbar fusion surgery. Fluoroscopy provides excellent penetration of tissues, allowing visualization of deeper structures and more precise needle placement, which can be advantageous in patients with obesity or significant anatomical variations. 30 Fluoroscopy allows for continuous monitoring during needle advancement, reducing the risk of inadvertent vascular or nerve injury.
Our study revealed that administering the ESPB took significantly less time using the Fluoroscopy guided technique (3.01 ± 0.97 mins) compared to the ultrasound-guided technique (4.74 ± 1.49 mins). This can be attributed to the real-time imaging provided by fluoroscopy, which allows for precise needle placement and reduces the need for multiple attempts. Additionally, locating the transverse process is easier with fluoroscopy than with ultrasound. 31 Therefore, this innovative fluoroscopy-guided technique enhances time efficiency and workflow in the operating room and can be performed by the spine surgeon while marking the level before surgery. The average number of fluoroscopy images taken during the fluoroscopy-guided technique was 4 ± 1.34.
Radiation exposure is a valid concern, but it can be effectively managed through strict adherence to safety protocols. 32 When compared to other routine medical imaging procedures, the level of radiation exposure remains relatively low and manageable. The benefits of precise needle placement, improved block efficacy, and reduced procedure time highlight the value of fluoroscopy-guided ESPB.
Studies by Robertson et al 20 and Patel et al 18 demonstrated that fluoroscopy guided ESPB facilitates effective anesthetic spread within the target plane, and provided consistent and reliable postoperative pain management.
Following the procedure, both groups of patients reported significantly low pain scores on the Visual Analog Scale (VAS) within the initial 48 hours. The results were remarkably similar, showing no significant difference in pain relief between the 2 techniques. The total opioid consumption in the first 48 hours after surgery was similar in both groups and significantly lower compared to the control group in the randomized controlled study by Goel et al, which compared the effectiveness of ultrasound-guided ESPB in single-level lumbar fusion surgery. 15 Only 1 patient in the fluoro-ESPB group and 2 patients in the USG-ESPB group needed additional doses of fentanyl in the postoperative period. Our study findings have shown that both techniques (fluoroscopy-guided and ultrasound-guided) demonstrated high efficacy in peri-operative pain management and they were similar in efficacy as evidenced by consistently low levels of postoperative pain and equivalent total opioid consumption across both groups during the perioperative period.
Additionally, intraoperative blood loss was comparable between the groups (Table 2). The hemodynamic parameters showed a similar decrease compared to the baseline in both groups. Studies by Patel et al 18 and Goel et al. 15 have demonstrated that ESPB provides better hemodynamic stability intraoperatively due to reduced nociceptive stimulus. This leads to reduced intraoperative blood loss in ESPB patients, which may be attributable to the combination of sympathetic blockade 15 and pre-emptive analgesia given before real tissue damage.
The fluoroscopy guided erector spinae plane block (ESPB), as a regional anesthetic technique, provides effective perioperative pain management in lumbar fusion surgery and significantly reduces opioid consumption. It can be integrated into Enhanced Recovery After Surgery (ERAS) protocols, contributing to multimodal analgesia and improved postoperative outcomes. ESPB has already been successfully incorporated into ERAS pathways for percutaneous nephrolithotomy, demonstrating its efficacy in reducing pain and opioid requirements. 33 However, its role in spine surgery ERAS protocols remains underexplored and requires further well-designed clinical studies to evaluate its benefits, optimize its technique, and compare its effectiveness with other regional anesthesia methods.
Our study’s strength lies in its prospective, randomized clinical trial involving 2 groups with similar demographic and operative profiles. This is the first study to compare the fluoroscopy-guided technique with the traditional ultrasound-guided technique for delivering ESPB in lumbar fusion surgery. It also considered patient-related outcomes like MOASS and Patient Satisfaction Scores, in addition to intraoperative hemodynamic parameters. All the patients in both groups had good pain relief. All the patients in both groups received multimodal analgesia using paracetamol and Fentanyl as rescue analgesia in the perioperative period. There were no block-related complications. Patients in both groups have reduced incidence of nausea and vomiting, this can be explained by reduced usage of opioids in both groups.
The study has a few limitations. First, the sample size is relatively small, and hence a larger sample with a longer follow-up would strengthen the results and enhance the clinical findings of the study. The anesthesiologist and surgeon, who were not blinded to the 2 groups, gave the block, which may result in intrinsic performance bias.
Conclusion
Both fluoroscopy-guided and ultrasound-guided ESPB techniques provide sufficient perioperative pain relief after lumbar fusion surgery and can be used as additional components in multimodal pain management. However, the fluoroscopy-guided ESPB can be administered by the surgeon himself, making it a safe and effective alternative to the traditional ultrasound-guided technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Ganga Orthopaedic Research and Education Foundation.