
Abstract
Study Design
Meta-analysis study.
Objectives
We aimed to compare clinical outcomes, radiologic parameters, and complications between the stand-alone anchored spacer and the plate-cage construct as treatment options for patients with multilevel cervical degenerative spondylopathy involving 3 or 4 levels.
Methods
In this meta-analysis, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search for relevant studies covered the Embase, PubMed, and Cochrane Central Register of Controlled Trials databases, encompassing data from the inception of each database up to July 1, 2024.
Results
The analysis included 12 studies, involving a total of 817 patients. Patients in the stand-alone anchored spacer group exhibited decreased intraoperative blood loss and shorter surgical durations. Clinical outcomes, including visual analog scale (VAS) scores, Japanese Orthopaedic Association (JOA) scores, Neck Disability Index (NDI) scores, and Odom’s criteria for clinical outcomes, demonstrated no significant differences between the two groups. Radiographic outcomes revealed no statistically significant difference in fusion rates between stand-alone cages and plate-cage constructs. However, the plate-cage group exhibited more favorable maintenance of segmental angle and cervical alignment (C2-C7 angle).
Conclusions
Both stand-alone anchored spacer and plate-cage constructs are viable treatment options for patients with cervical degenerative spondylopathy involving more than two levels. Stand-alone cages have the benefit of reducing intraoperative blood loss and shortening surgical durations, but they are associated with a higher risk of cage subsidence. Plate-cage constructs offer better maintenance of segmental angle and cervical alignment; however, they carry a higher risk of dysphagia.
Keywords
Introduction
Cervical spondylosis typically begins with degenerative changes in the intervertebral disk, which subsequently induce secondary alterations in the surrounding soft tissues and bony structures. This progressive process leads to gradual narrowing of the spinal canal, resulting in compression of the dural sac. As a result, patients may experience neurological symptoms, such as pain, hypoesthesia (reduced sensation) and muscle weakness. 1 Disc height loss further contributes to a reduction in neuroforaminal height, compressing exiting nerve roots and exacerbating radicular symptoms. Cage implantation addresses these issues through two complementary mechanisms: indirect decompression, achieved by restoring disc and neuroforaminal height to relieve radicular symptoms, and direct decompression of the spinal canal, which alleviates central canal stenosis. The anterior surgical approaches to address cervical spondylosis include various procedures, such as anterior cervical corpectomy and fusion (ACCF), anterior cervical discectomy and fusion (ACDF), cervical artificial disc replacement (c-ADR), and hybrid procedures. 2 Since the 1950s, anterior cervical discectomy and fusion (ACDF) have remained the established gold standard in surgical treatments for degenerative cervical conditions.3,4 To achieve solid fixation and maintain cervical lordosis, surgeons commonly opt to include an additional anterior cervical plate in fusion procedures after anterior decompression and cage implantation. The anterior plate is believed to decrease micro-movement of the cervical spine, promote fusion, reduce subsidence, and improve cervical sagittal alignment and stability. However, complications associated with the use of the anterior plate are still not uncommon.5,6
Multilevel cervical spondylosis presents a significant therapeutic challenge, with anterior plating being a commonly employed technique to enhance fusion rates. Although it has potential benefits, performing ACDF with more than two levels (
The development of self-anchored stand-alone cages with a zero-profile design aims to avoid plate-related complications and reduce operation time. Furthermore, it is claimed that self-anchored stand-alone cage provides comparable immediate stability to that achieved with the use of plate-cage construct. As a result, the emergence of a novel device called the “Stand-alone anchored spacer” has occurred. This device combines the advantages of a stand-alone cage with anchoring screw fixation. It is expected to offer immediate stability and effectively prevent plate-related complications. Therefore, these advancements present promising options in the surgical treatment of cervical spine conditions.11,12 Nevertheless, there is disagreement regarding the use of stand-alone cages, particularly concerning issues such as cage subsidence, cage migration, loss of cervical lordosis and fused segment angle, and the relatively low fusion rate. Over the past decade, an ongoing debate has arisen regarding the optimal treatment approach (plate-cage or stand-alone anchored spacer) for managing multilevel cervical spondylosis. However, a consensus has not yet been reached on this matter. 13
The objective of this study was to conduct a meta-analysis to compare clinical outcomes, radiologic parameters, and complications of the stand-alone anchored spacer and the plate-cage construct in the treatment of patients with cervical degenerative spondylopathy involving more than two levels.
Methods
Materials and Methods
This meta-analysis was carried out in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. A comprehensive systematic search was conducted across the Embase, PubMed, and Cochrane Central Register of Controlled Trials online databases, spanning from the inception of each database to July 1, 2024. The search employed a specific set of keywords, namely: stand-alone cage, plate-cage, cervical spondylosis, anterior cervical discectomy and fusion, cervical arthrodesis, three-level cervical disease, four-level cervical disease, comparative study. Additionally, a thorough examination of the reference lists within pertinent articles was performed to identify any further relevant studies that could contribute to the analysis.
Study Selection
The identification of relevant studies and the subsequent exclusion of papers were carried out independently by two authors (C.J.C.,Y.F.L.). Discrepancies were resolved through consensus reached via deliberation. Inclusion criteria encompassed articles featuring two distinct patient cohorts who underwent either anterior cervical discectomy and fusion with a plate-cage construct or a stand-alone anchored spacer. These patients presented with cervical spondylosis accompanied by myelopathy or radiculopathy. Additional criteria for inclusion in this study were studies with a Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) score of 15 or higher, as well as studies that reported functional outcome scores with a minimum follow-up duration of 1 year.
Exclusion criteria were rigorously applied to several categories, including studies not presented in the English language, biomechanical inquiries, studies involving less than three-level interventions, investigations lacking a proper control group, studies with unclear delineation of patient demographics, and studies characterized by insufficiently available data. Following the application of these exclusion criteria, the identified studies underwent a comprehensive and meticulous evaluation process. A specific emphasis was placed on evaluating the congruence of these studies with the principles outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement, which played a pivotal role in determining their eligibility for inclusion in the analytical framework.
The assessment of the quality of each individual article was conducted in strict adherence to the guidelines and benchmarks delineated by the STROBE guidelines, thus ensuring a systematic and standardized evaluation process.
Data Extraction
The process of data extraction was executed by two independent authors (C.J.C.,Y.M.H.) in a meticulous manner. If additional or missing data were required, we contacted the authors of the respective articles to obtain the required information. The extracted data encompassed the following key elements from the included articles: 1) Patient characteristics, which comprised age, gender, duration of follow-up, and the specific type of implanted medical device. 2) Clinical outcomes including Neck Disability Index (NDI) and the Japanese Orthopaedic Association (JOA) score, as well as the documentation of any observed complications. 3) Radiographic outcomes, which encompassed measurements related to disc height, the C2-C7 angle, and segmental angles. This systematic approach to data extraction ensured a comprehensive and standardized method for gathering information from the selected articles, thus enhancing the reliability and consistency of the findings.
Statistical Analysis
For the analysis of outcomes, the Mantel-Haenszel method along with variance-weighted means was employed. Heterogeneity was quantified and assessed using the I2 statistic, which operates on a scale from 0% to 100%. An I2 value exceeding 50% was indicative of substantial heterogeneity. In instances where significant heterogeneity was identified, a random-effects analysis was employed to evaluate the studies. Conversely, studies displaying negligible heterogeneity were subject to a fixed-effects analysis. The calculations for heterogeneity, mean differences, and relative risks were applied to all outcomes within this meta-analysis. Moreover, examination for the presence of publication bias was undertaken through the application of Egger funnel plots. The execution of this meta-analysis was facilitated using Review Manager (RevMan) version 5.3 software, developed by The Cochrane Collaboration. This software provided the necessary tools for data synthesis and comprehensive graphical representation of the findings.
Results
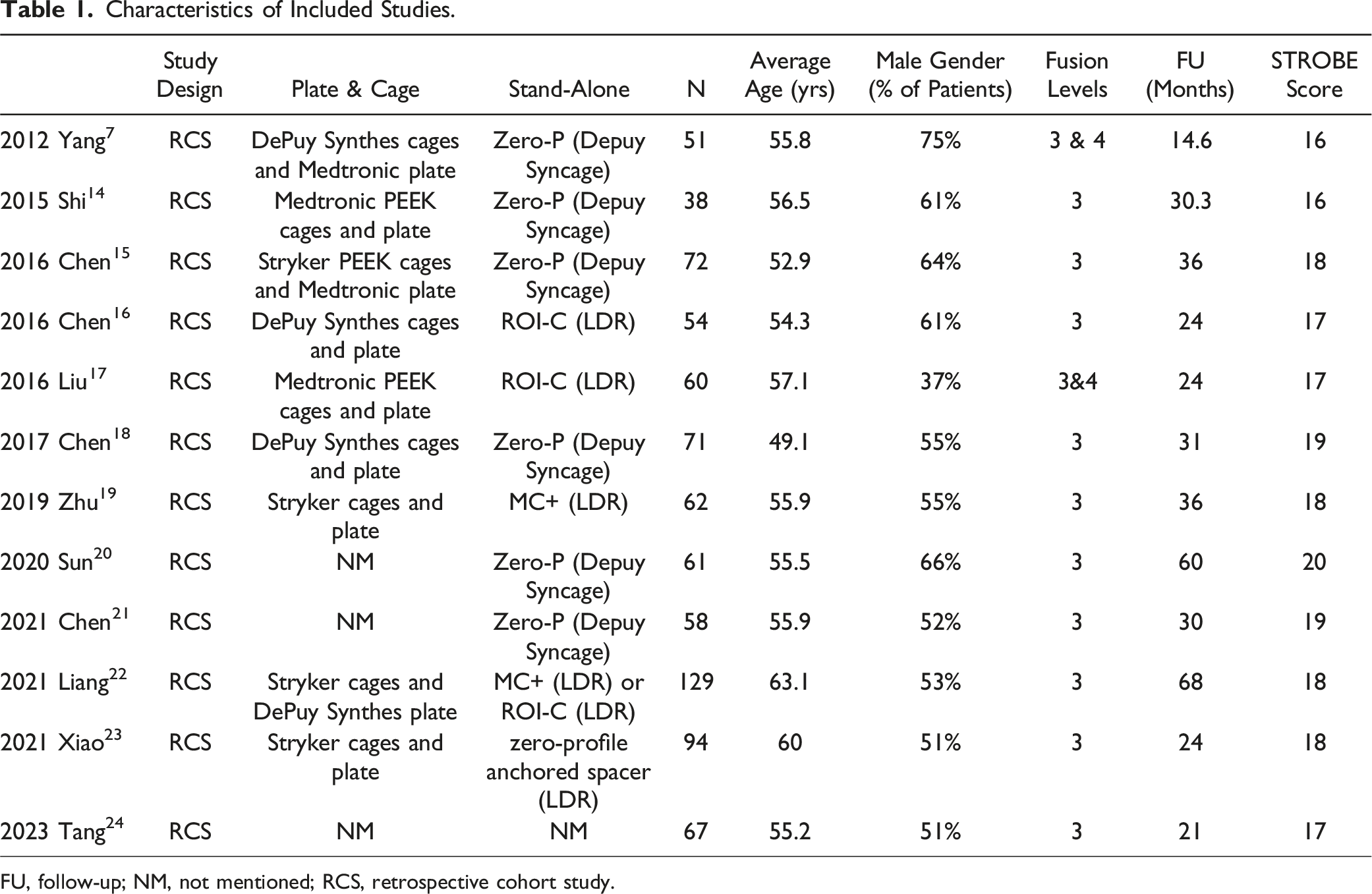
The initial phase of our investigation yielded a total of 823 potentially relevant articles through our search strategy. Subsequent removal of duplicates and articles not aligned with the scope led to a meticulous review of the full texts of 63 articles. Following the application of our well-defined inclusion and exclusion criteria, a total of 12 studies were identified as suitable for inclusion in the meta-analysis (see Figure 1 for a flowchart detailing the selection process).7,14-24 The patient characteristics within these 12 studies are succinctly summarized in Table 1. This collection of studies involved a cumulative cohort of 410 individuals who underwent anterior cervical fusion with a stand-alone cage and 407 patients who received treatment with a plate-cage construct. Flow diagram depicting the study selection in accordance with the PRISMA guidelines. Characteristics of Included Studies. FU, follow-up; NM, not mentioned; RCS, retrospective cohort study.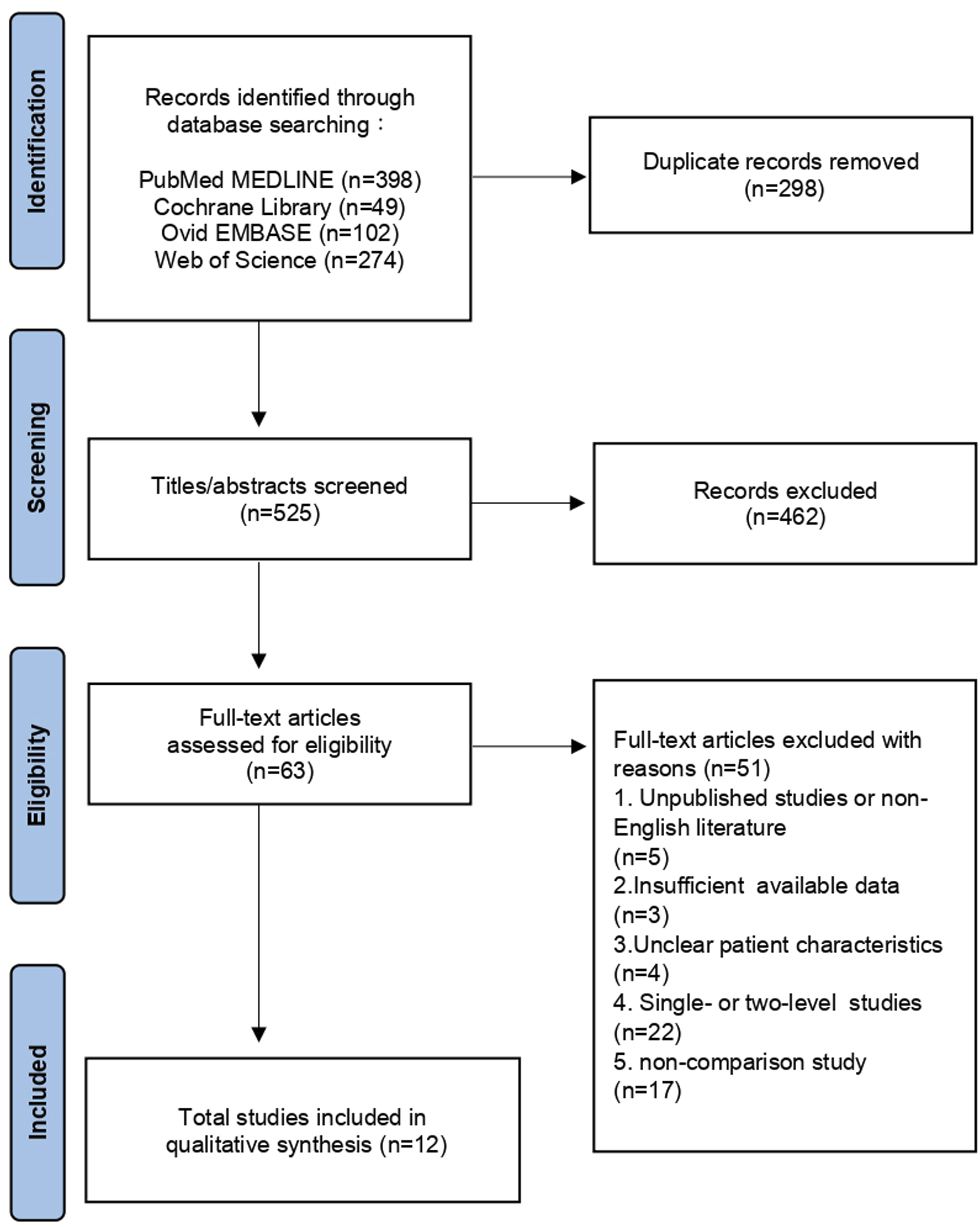
Risk of Bias Assessment
Bias Assessment of Studies With the ROBINS-I Tool.
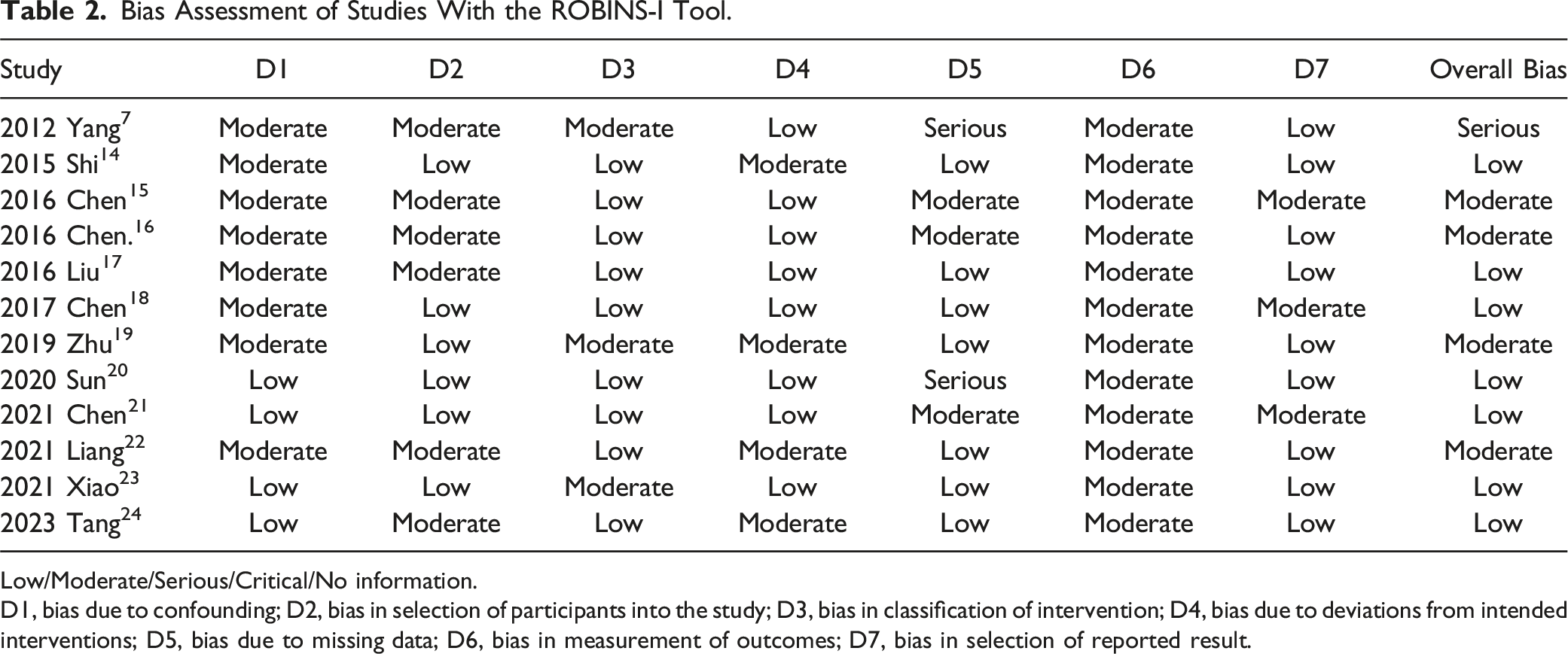
Low/Moderate/Serious/Critical/No information.
D1, bias due to confounding; D2, bias in selection of participants into the study; D3, bias in classification of intervention; D4, bias due to deviations from intended interventions; D5, bias due to missing data; D6, bias in measurement of outcomes; D7, bias in selection of reported result.
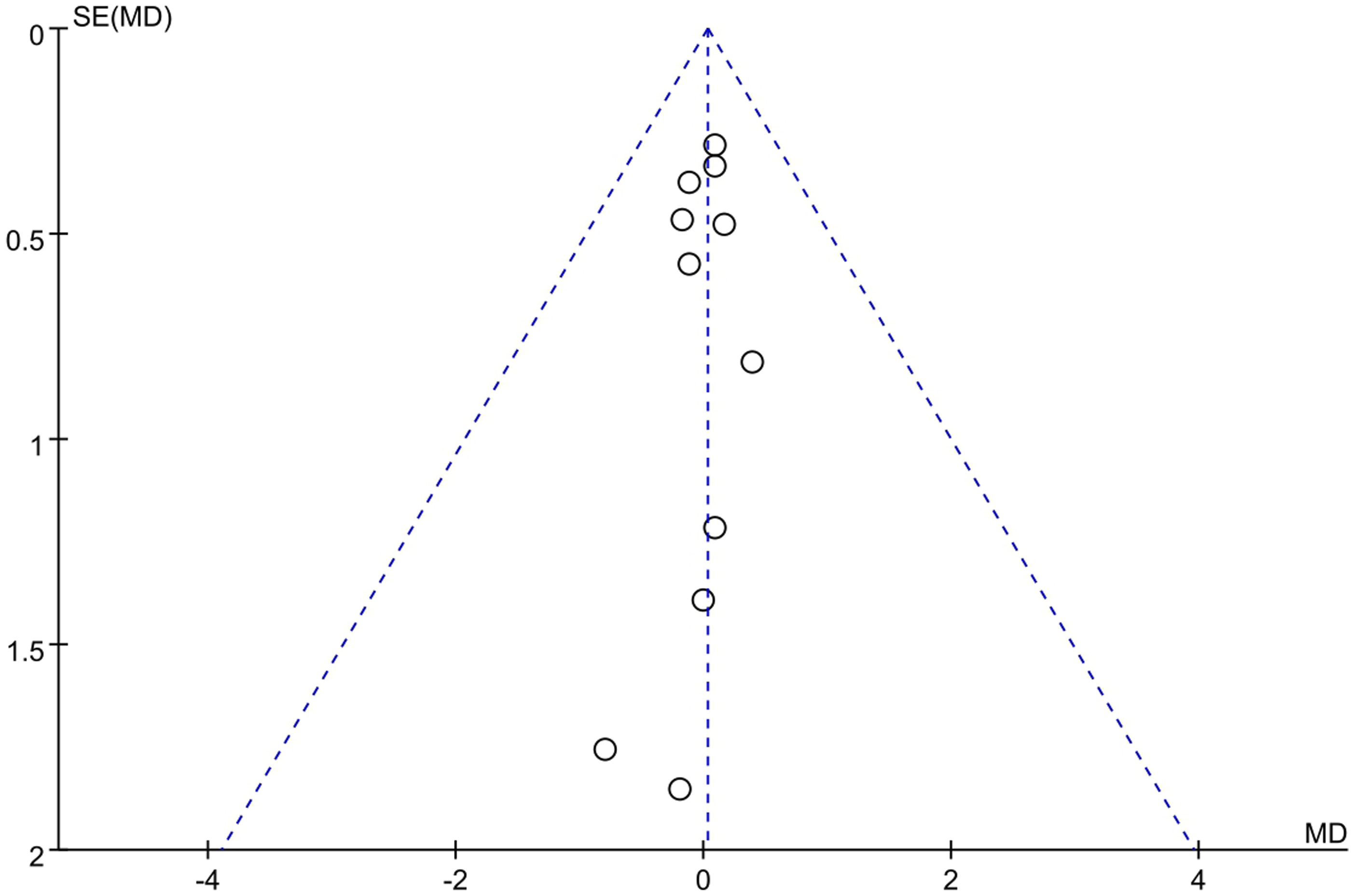
The funnel plots displayed a symmetrical pattern, which indicates that publication bias is unlikely.
Perioperative Comparisons
Concerning perioperative comparisons, it was observed that patients who underwent treatment with a stand-alone cage exhibited a decrease in intraoperative blood loss (11.52, 95% CI 3.73 to 19.32, P = .004, under the random-effects model). Besides, the stand-alone cage group necessitated a shorter surgical duration when compared to the plate-cage group (18.79, 95% CI 8.79-28.78, P = .0002, under the random-effects model). However, there was no statistically significant difference in the length of hospital stay between these two groups (.06, 95% CI -0.17-0.29, P = 0.63, under the fixed-effects model). (Figure 3) Comparisons between the plate-cage and stand-alone cage groups regarding blood loss (A), surgical time (B), and length of admission (C). IV: inverse variance.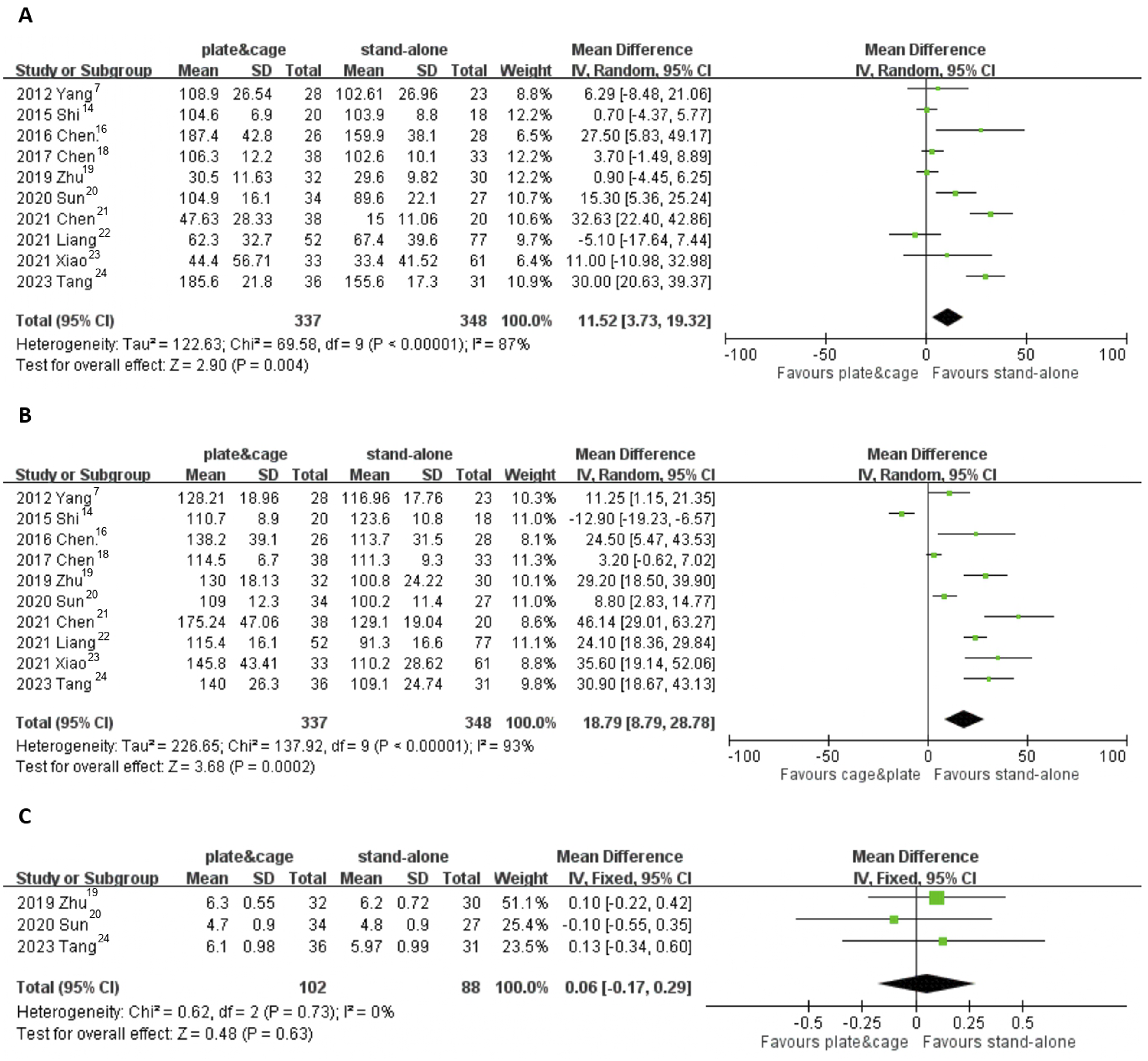
Clinical Outcomes
With regard to clinical outcomes, there exists no statistically significant difference between the two groups in terms of VAS score (−0.03, 95% CI −0.94 to 0.89, P = 0.95, under the random-effects model). Similarly, there were no significant differences observed between these two groups in terms of functional outcomes, as measured by functional outcomes of Japanese Orthopaedic Association (JOA) scores (0.08, 95% CI −0.12 to 0.27, P = 0.43, under the fixed-effects model) and Neck Disability Index (NDI) scores (0.03, 95% CI −0.27 to 0.33, P = 0.85, under the fixed-effects model). According to the Odom’s criteria, the percentages of patients with excellent and good clinical outcomes were 92.3% in the stand-alone cage group and 91.3% in the cage-plate group (Relative Risk [RR] 0.91, 95% CI 0.36 to 2.32, P = 0.84, under the fixed-effects model). (Figure 4) Comparisons between the plate-cage and stand-alone cage groups regarding VAS (A), JOA (B), and NDI (C) scores, and Odom’s criteria (D). M-H: Mantel-Haenszel.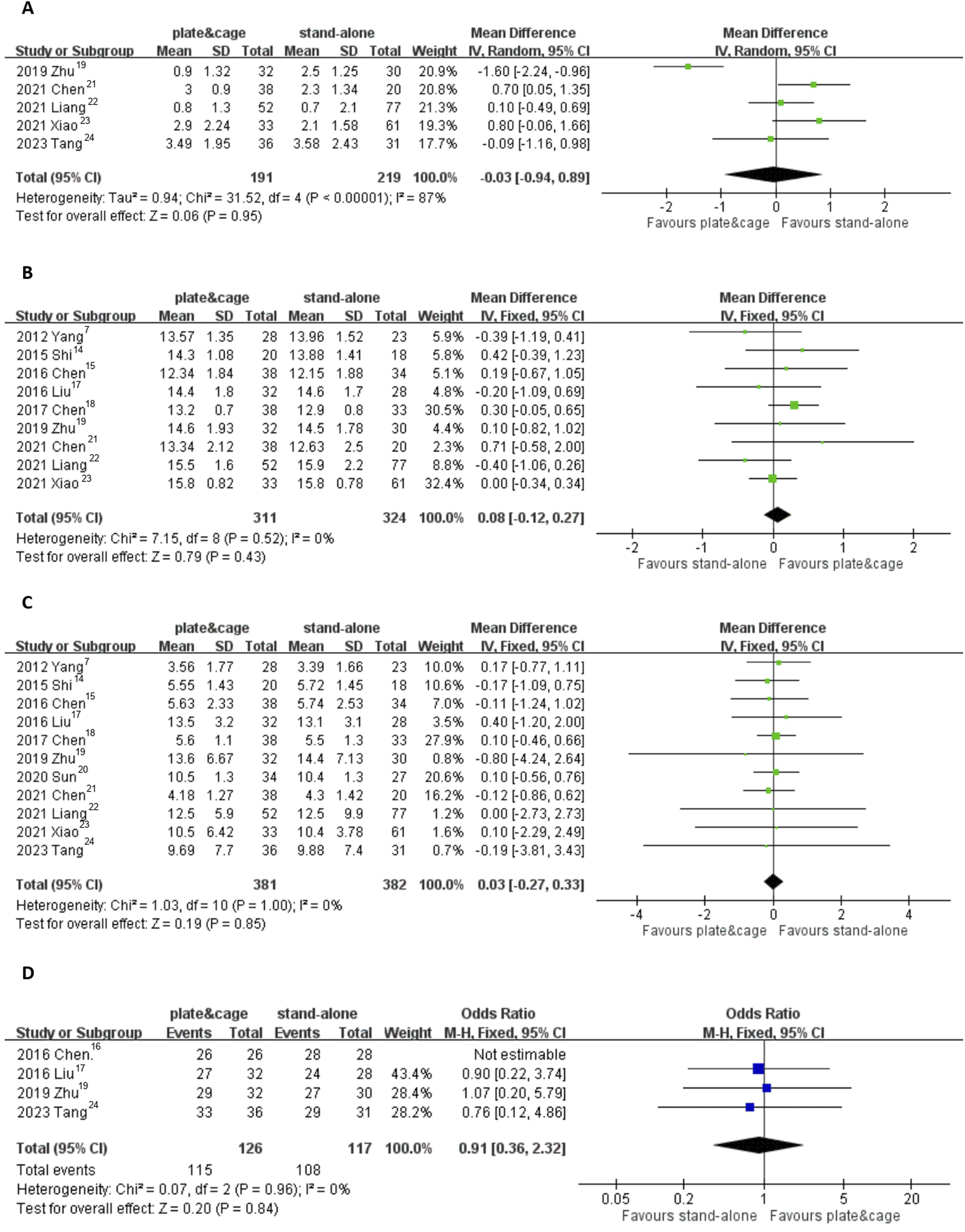
Radiographic Outcomes
In terms of radiographic outcomes, the fusion rate within the plate-cage group ranged from 89.5% to 100%, while within the stand-alone cage group, it ranged from 83.3% to 100%. Notably, there was no statistically significant difference found between these two groups (Relative Risk [RR] 1.00, 95% CI 0.97-1.03, P = 0.86). No significant difference in post-surgery disc height was noted between the two groups (0.21, 95% CI -0.35 to 0.78, P = 0.46, under the random-effects model). However, the plate-cage group demonstrated a more favorable maintenance of segmental angle compared to the stand-alone group (3.12, 95% CI 1.17 to 5.06, P = 0.002, under the random-effects model). Moreover, the plate-cage group exhibited a more favorable maintenance of cervical alignment, as indicated by the C2-C7 lordotic angle, compared to the stand-alone group (3.31, 95% CI 2.24 to 4.38, P < 0.00001, under the fixed-effects model). (Figure 5) Comparison between the plate-cage and stand-alone cage groups regarding fusion rate (A), disc height (B), segmental angle (C), and C2-C7 angle (D).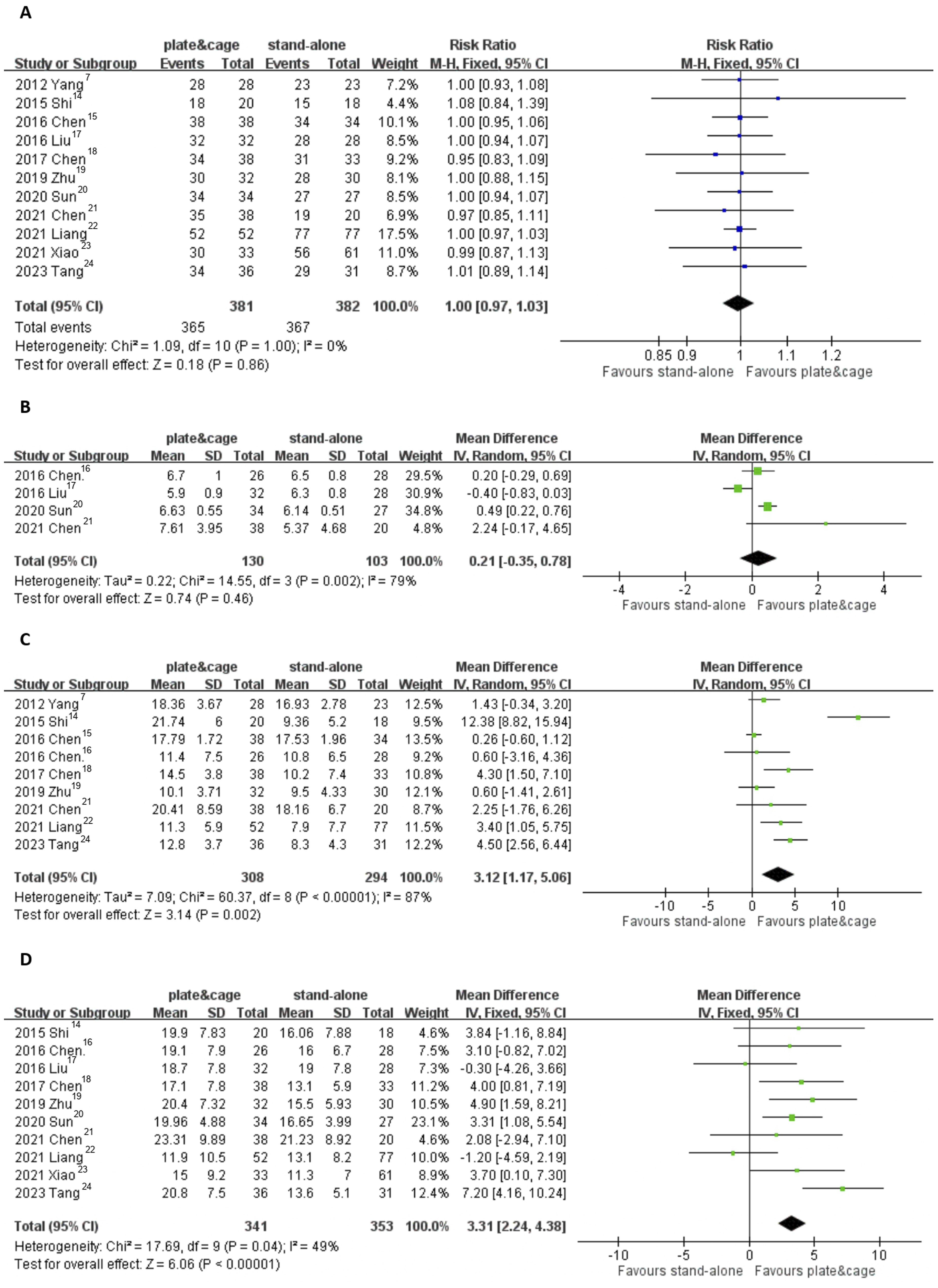
Complications
Overall Complications Recorded in the Included Studies.
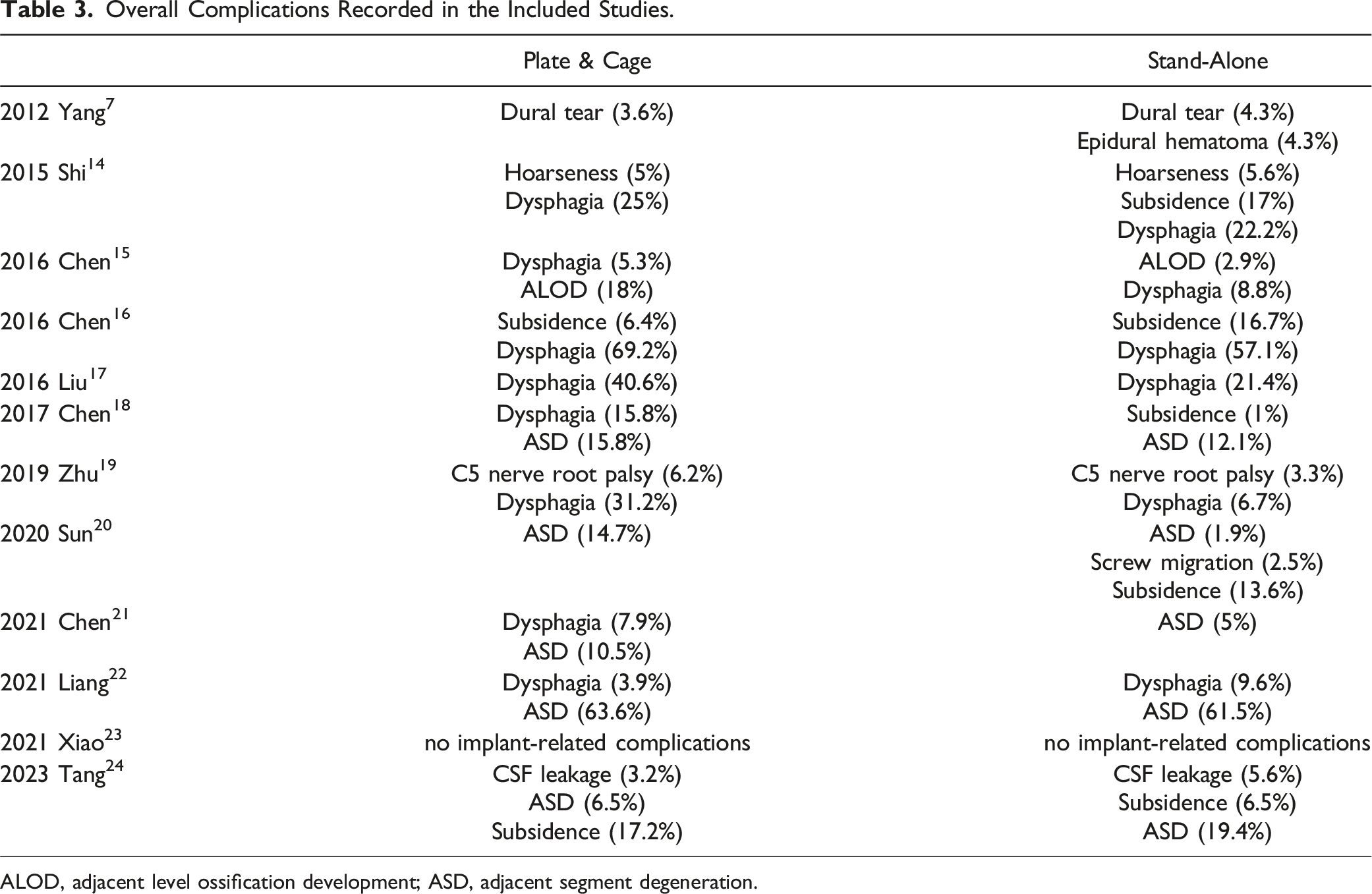
ALOD, adjacent level ossification development; ASD, adjacent segment degeneration.
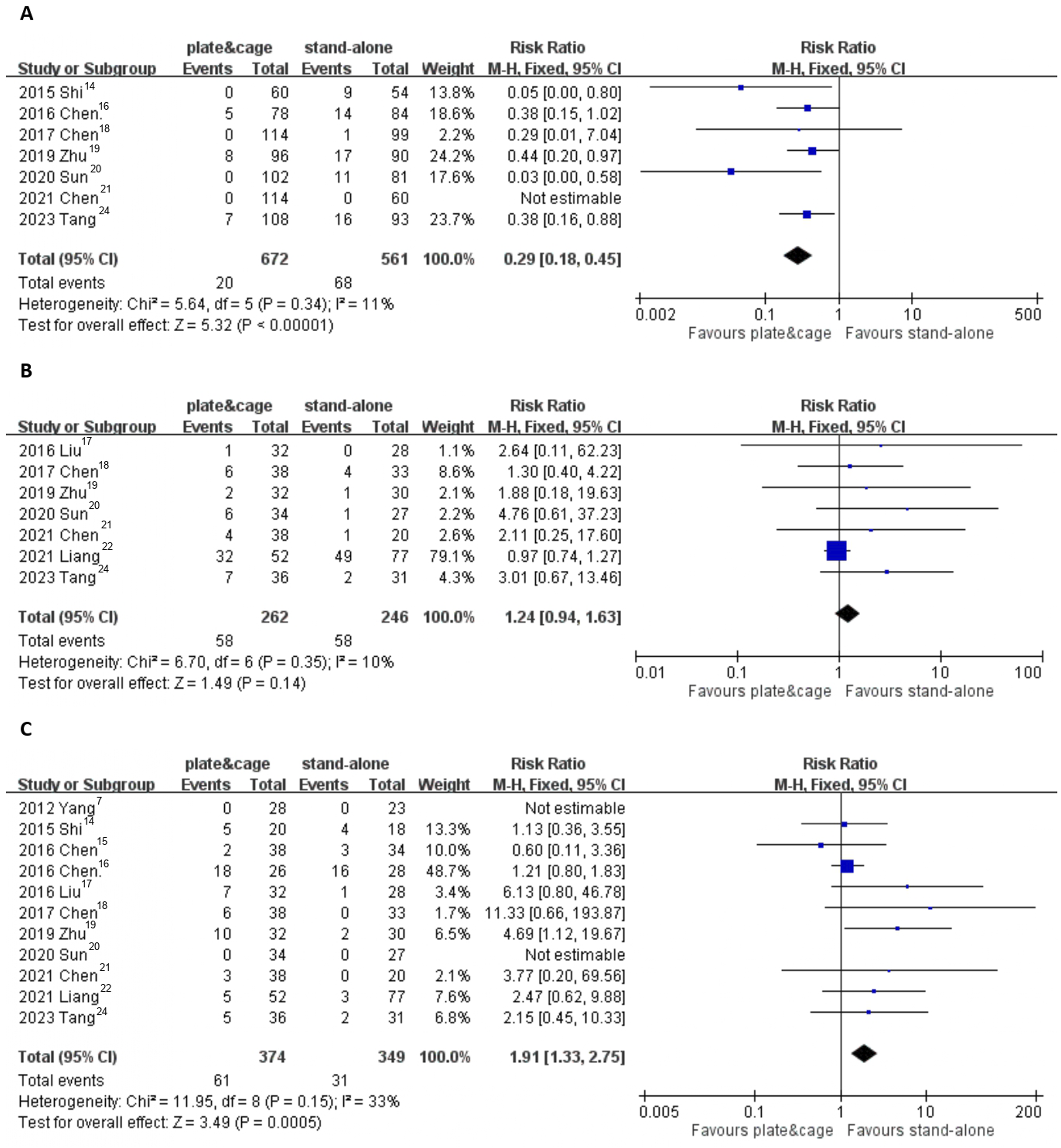
Comparison between the plate-cage and stand-alone cage groups regarding subsidence (levels) (A), ASD (B), and dysphagia (C).
Criteria of Fusion, Subsidence and Adjacent Disc Degeneration
Fusion
Fusion was evaluated in the included studies using a combination of radiographic and motion-based criteria: • Radiographic fusion: Defined by the presence of continuous trabecular bridging across the graft–endplate or cage–endplate interface and the absence of radiolucent gaps between the graft or cage and the vertebral endplate. • Motion criteria: Assessed using flexion-extension radiographs, with solid fusion defined as ≤2 mm of motion between adjacent spinous processes. Follow-up evaluations were typically conducted over a period of 1 to 2 years.
Subsidence
The included studies defined subsidence as radiographic evidence of implant migration into the adjacent vertebral endplate, resulting in a reduction in disc height. Most studies quantified subsidence as a decrease in intervertebral disc height exceeding 2-3 mm on follow-up radiographs compared to immediate postoperative imaging. Alternative definitions included a loss of mean disc height greater than 10% of the initial measurement or significant implant migration causing segmental instability.
Adjacent Segment Degeneration (ASD)
ASD was assessed based on radiographic criteria observed at adjacent levels. Evaluations were conducted using lateral radiographs during the final follow-up, ensuring consistency and standardization across the included studies. The criteria included: • New or enlarged anterior osteophyte formation. • Narrowing of the intervertebral disc space, typically defined as a reduction exceeding 30%. • Calcification of the anterior longitudinal ligament.
Discussion
Our meta-analysis found no significant differences in clinical outcomes, fusion rates, or complication incidence between ACDF with stand-alone anchored spacers and plate-cage constructs for treating multilevel cervical degenerative spondylopathy. Stand-alone spacers offered shorter surgeries and less blood loss, while plate-cage constructs better preserved cervical lordosis. Notably, plate-cage had a higher dysphagia risk, and stand-alone spacers had a higher risk of subsidence. This first comparison between the two treatments offers insights for clinical practice.
Cervical spondylosis progresses with degeneration of disks and surrounding structures, causing spinal constriction and neurological symptoms. 1 ACDF, the gold standard for cervical disc diseases, uses anterior plating to enhance fusion, maintain lordosis, and prevent subsidence. 26 Despite its benefits, multilevel procedures with cage-plate constructs can face issues like irritation and dysphagia. 27 The zero-profile implant, an advancement in ACDF, combines a stand-alone cage with screws for stability and reduced soft tissue contact, mitigating complications. 28 FDA-approved since 2008, Zero-P’s use has expanded to multiple segments, showing promise in short-term outcomes for one or two levels. 29 Limited research has been conducted on cervical issues involving more than two levels. Thus, the present study aims to address this gap by comparing the efficacy of stand-alone anchored spacers and plate-cage constructs in the surgical management of more than multilevel cervical degenerative spondylopathy. In our perspective, while clinical efficacy is vital for immediate patient well-being, radiographic outcomes are equally crucial for ensuring the long-term success and durability of surgical interventions. Therefore, when assessing the efficacy of surgical techniques for cervical spondylosis, both types of outcomes should be considered.
Preserving lordotic alignment is crucial in ACDF for treating cervical degenerative disc diseases, as it impacts spinal function and mobility. Sagittal malalignment post-ACDF can cause neck pain and worsen neurological issues, affecting recovery and potentially speeding up degeneration in adjacent segments. 30 Burkhardt et al.’s study on 144 two-level ACDF surgeries showed the plate-cage construct better preserved cervical lordosis than the locked stand-alone cage, though both had similar clinical outcomes. 31 Contrarily, studies noted more significant loss of lordosis with Zero-p over three years,20,32 while He et al. found no difference between the groups. 33 In our study, we observed that the post-operative C2-C7 angle and segmental angle were both more favorable in the plate-cage group when compared to the stand-alone anchored spacer group. Stand-alone cages, while initially effective in achieving cervical alignment, lack the rigid structural support provided by anterior plates. Over time, micro-motion at the fusion site and the gradual settling of the cage into the vertebral endplates may lead to a progressive loss of cervical lordosis. This settling effect is particularly prominent in multilevel constructs, where the cumulative load can exacerbate segmental collapse. In contrast, plate-cage constructs offer enhanced mechanical stability by rigidly anchoring the fusion construct, thereby better preserving cervical alignment and reducing the risk of long-term lordosis loss.
Studies have confirmed the safety and effectiveness of three-level ACDF using both cages and plate fixation,34,35 but complications like screw loosening, plate breakage, and neurovascular or trachea-esophagus injuries are more common in multilevel ACDF.7,8 Dysphagia, especially after multilevel ACDF, is a significant issue, with unclear mechanisms.36,37 Factors contributing to dysphagia include the surgical exposure of discs and vertebrae, esophageal injury, soft tissue edema, and adhesions around cervical plates.6,38 Lee et al found that thicker cervical plates could increase dysphagia risk, 39 suggesting that plate removal and adhesion lysis could improve outcomes. 40 The stand-alone anchored spacer, combining stand-alone cage benefits with anchor fixation, aims to provide stability while reducing dysphagia risks compared to traditional plate-cage constructs. In our meta-analysis, we found that patients who underwent fusion surgery with a plate-cage construct had a higher risk of experiencing dysphagia at the final follow-up. The higher rates of dysphagia observed with plate-cage constructs are likely multifactorial. The anterior plate can cause increased soft tissue irritation due to its direct contact with the esophagus. Factors such as plate thickness, screw prominence, and postoperative adhesion formation around the anterior cervical spine may contribute to esophageal irritation and swallowing difficulties. This complication highlights the need to consider patient-specific factors and anatomical variations during plate selection and surgical planning.
Cage subsidence is a major issue in multilevel ACDF, potentially causing loss of cervical lordosis. Liu et al.’s meta-analysis, covering surgeries from one to four levels, found that the zero-P group had significantly more subsidence than the plate-cage construct group. 41 Lee et al. also highlighted the risk of subsidence and poor fusion rates with stand-alone cages due to reduced biomechanical stability. 42 Our analysis confirms a higher subsidence risk in the stand-alone group, though a systematic review suggests subsidence doesn’t impact clinical outcomes or fusion rates. 43 The higher subsidence rates associated with stand-alone cages can be attributed to their reliance on the vertebral endplate for load-bearing stability. Without additional support from an anterior plate, stand-alone cages are more susceptible to stress concentration at the bone-implant interface. This stress concentration is particularly pronounced in patients with compromised bone quality, such as those with osteoporosis or advanced age, increasing the likelihood of implant subsidence. Additionally, the absence of an anterior plate to redistribute mechanical loads may further exacerbate this phenomenon.
Multilevel ACDF may increase the risk of accelerated degeneration in adjacent spinal segments due to added rigidity. Research indicates anterior plating could hasten degenerative changes in neighboring segments,44,45 possibly due to increased motion transfer leading to faster disc degeneration and new pathologies. 17 A study comparing zero-profile anchored spacers with cage-plate constructs for three or four-level cervical disease management found no adjacent disc degeneration in the zero-profile group. 17 In our meta-analysis, the rate of adjacent segment degeneration (ASD) was comparable between both groups. We recognize that the follow-up durations in the included studies are insufficient to capture the majority of ASD cases, given its gradual progression over time. With an estimated incidence of approximately 3% per year, long-term follow-up studies are critical to fully understand the impact of surgical techniques on ASD development. Furthermore, poor segmental alignment and the use of long plates that abut the adjacent disc space may accelerate the onset of ASD. Optimal cage-plate constructs, when combined with adequate alignment restoration and long-term follow-up of 5 to 10 years, are likely to result in improved fusion rates and lower ASD incidence. However, these long-term effects could not be determined from this study due to the limitations in follow-up durations within the prior studies included in our analysis.
Previous systematic reviews and meta-analyses have been conducted to examine the comparison between zero-profile cages and plate-cage construct in one and two level ACDF. A study conducted by Cheung et al, which encompassed a thorough analysis of 19 studies, unveiled that the stand-alone cage approach offered advantages such as reduced occurrence of dysphagia, minimized intraoperative blood loss, and a decreased likelihood of adjacent segment disease. Nevertheless, it was also associated with higher rates of subsidence and less successful restoration of cervical lordosis. 26 A systematic review focused on two-level ACDF revealed that the locking stand-alone cage was related to notably greater disc height loss, an increased risk of subsidence, and a decrease in cervical lordosis during follow-up. 46 A recent systematic review carried out by Boer et al. found no difference in clinical outcomes (measured by neck disability index and visual analog scale) or radiological outcomes (including fusion rate and cervical lordosis) between the two groups, However, stand-alone devices were associated with shorter operative times. 47 The convergence of these studies highlights the complexity of decision-making in this domain, encouraging further investigation and advancements in treatment options to optimize patient outcomes.
Limitations
This study has certain limitations that need to be acknowledged. Firstly, the inclusion of only 12 retrospective cohort studies that met our criteria raises the possibility of publication bias. Despite our efforts to include more diverse study designs, the available literature was limited to cohort studies. Secondly, there were inconsistencies in the reporting of outcomes, and incomplete baseline and surgical data were present, which may introduce bias when pooling such data. While this study primarily focused on the impact of construct design on clinical and radiographic outcomes, it did not account for several other factors known to significantly influence fusion success. These include patient-related variables such as osteoporosis, smoking status, and comorbidities, as well as procedural factors like the number of levels fused, cage material, and the use of biologics. The omission of these variables represents a notable limitation of this meta-analysis and highlights the need for future studies to include comprehensive data collection on these factors to better understand their impact on fusion outcomes. Thirdly, the follow-up period varied and was relatively short to mid-term (ranging from 14 to 68 months), which could impact the assessment of functional outcomes and subsequent complications. We recognize that this relatively short to mid-term follow-up may impact the assessment of long-term outcomes such as sustained fusion rates and late-onset complications. To address this, we recommend that future studies incorporate follow-up durations of at least 5 to 10 years. This would allow for a more comprehensive evaluation of both immediate and long-term effects, providing a clearer understanding of the durability and potential late-onset complications associated with these surgical interventions. Finally, the statistical power of this meta-analysis is constrained by the relatively small number of included studies and participants for certain outcomes, such as Odom’s criteria and VAS scores. Meta-analyses typically require a larger number of studies and data points to ensure reliable and robust conclusions. However, the limited availability of studies on this topic restricts the precision and generalizability of some findings. Consequently, these results should be interpreted with caution, as they may not provide definitive conclusions. To address this gap, future research should prioritize conducting larger, high-quality randomized controlled trials to validate and expand upon these findings.
We evaluated heterogeneity using the I2 statistic and identified significant variability in some of the pooled data across the included studies. Beyond the differences revealed through meta-regression and subgroup analyses, additional sources of heterogeneity likely include inconsistencies in reporting and measurement methods, such as variations in the definitions and criteria for key outcomes like fusion, subsidence, and adjacent segment degeneration. These inconsistencies may have contributed to discrepancies in the pooled results. Geographic and institutional differences, including variations in surgical techniques, perioperative care protocols, and postoperative rehabilitation practices, could also have influenced outcomes, particularly perioperative metrics such as blood loss and surgical duration. Furthermore, variability in patient demographics, such as age, comorbidities, and the severity of cervical spondylosis, likely introduced clinical diversity not fully addressed by subgroup analyses. Lastly, the retrospective nature of the included studies may have introduced selection and reporting biases, further amplifying heterogeneity. Recognizing these factors is crucial for accurately interpreting the pooled results and underscores the need for standardized protocols in future research.
To address the limitation of clinical diversity among patients with cervical spondylosis, future research should consider including a broader range of patient demographics, including older adults and individuals with various comorbid conditions. These studies should aim for longer follow-up periods to capture long-term outcomes and potential late-onset complications. Conducting multicenter studies across different geographical locations and healthcare settings can further ensure that the results are representative of broader patient populations and clinical practices. By implementing these strategies, future studies can provide more comprehensive and applicable insights, thereby improving the external validity of the results.
Conclusion
In summary, our comprehensive meta-analysis examined the use of stand-alone anchored spacer and plate-cage construct in anterior cervical fusion techniques. Stand-alone anchored spacer showed advantages in terms of reduced blood loss and surgical duration, while plate-cage constructs demonstrated benefits in maintaining cervical lordosis. Both groups had comparable clinical outcomes, fusion rates, and complications. However, the plate-cage group had a higher risk of dysphagia, while the stand-alone group was associated with a greater risk of cage subsidence. These findings offer valuable insights for clinical decision-making.
When planning surgeries, surgeons must carefully consider both clinical and radiographic outcomes, as well as the associated complications of each technique. For patients at higher risk of intraoperative complications, stand-alone anchored spacers may be particularly advantageous due to their shorter surgical durations and reduced blood loss. However, this benefit must be weighed against the higher risk of cage subsidence, which can negatively impact long-term cervical alignment and patient outcomes. In contrast, plate-cage constructs demonstrate superior maintenance of cervical lordosis and segmental alignment, making them more appropriate for patients where long-term spinal stability is a priority. Nevertheless, these constructs carry a higher risk of complications, such as dysphagia and hardware-related issues, which should be considered during preoperative planning. Ultimately, the choice of surgical approach should be personalized, considering patient-specific factors such as age, comorbidities, and the severity of cervical spondylosis. While immediate clinical efficacy is essential for patient well-being, the long-term success and durability of the intervention also rely on achieving and maintaining critical radiographic outcomes. By aligning surgical techniques with individual patient needs, clinicians can optimize both short-term and long-term outcomes.
Footnotes
Acknowledgments
We are grateful to the Skeleton Materials and Bio-compatibility Core Lab, Clinical Medicine Research Center, National Cheng Kung University Hospital for assistance with this study.
Author Contributions
All authors contributed to the study conception and design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Taiwan National Science and Technology Council (grants: MOST 110-2314-B-006 -027 -MY3, and NSTC 112-2314-B-006-075). This study was also supported by National Cheng Kung University Hospital, Tainan, Taiwan (grants: NCKUH-11302030 and NCKUH-11303016).
Correction (June 2025):
This article has been updated to correct a grant number in the Funding statement.
Data availability statement
All data generated or analyzed during this study are included in this published article.