
Abstract
Study Design
Review of the literature with critical appraisal and clinical recommendations.
Objective
To highlight contemporary concepts relating to surgical care for acute traumatic spinal cord injury (SCI) based on recent evidence that may be integrated into clinical practice.
Methods
Three recent articles relating to the surgical management of acute traumatic SCI were selected and critically appraised. Clinical practice recommendations were developed and graded as strong or conditional.
Results
Article 1: Early vs late surgical decompression for central cord syndrome. Strong recommendation to consider early surgery (<24 hours) as an option in patients with ASIA Impairment Scale (AIS) grade C central cord syndrome. Article 2: Extent of decompression in motor complete SCI. Conditional recommendation to consider laminectomy, with or without anterior surgery, to achieve circumferential decompression of the spinal cord. Article 3: Use of intra-operative ultrasound. Conditional recommendation to use ultrasound intra-operatively to confirm the adequacy of surgical decompression.
Conclusions
Timely and adequate decompression of the spinal cord are critical priorities in the management of acute traumatic SCI. The importance of timeliness extends to central cord syndrome. Careful consideration and use of operative techniques (e.g., addition of laminectomy) and adjuncts (e.g., intra-operative ultrasound) help achieve safe and adequate decompression of the spinal cord.
Keywords
Introduction
When developing clinical practice guidelines (CPG) and recommendations, the context of the CPG “topic,” like spinal cord injury (SCI), is often neglected as opposed to undergoing more scrutiny and consideration when determining recommendations. Traditional evidence based medicine recommendations utilize evidence, which often leaves the healthcare community with limited directions. The GRADE methodology (GRADE = Grading of Recommendation, Assessment, Development, and Evaluation) 1 evolved to overcome this limitation, offering direction based on not only evidence but expert opinion, patient values, risk/benefits of the intervention, and cost- effectiveness; variables that are of utmost importance in a setting of limited evidence or a catastrophic injury such as SCI.1-5 Despite GRADE, guideline authors have struggled to acknowledge and consider these variables and thus have not provided community based surgeons with the guidance they need. The AO Spine clinical practice recommendations try to overcome this limitation.
Acute SCI is a catastrophic event, often portending lifelong neurological impairment for the patient and significant economic burden to healthcare systems.2-4 Research efforts have enhanced our understanding of the pathophysiology of SCI and elucidated novel combinatorial treatment approaches involving pharmacologic, biologic, and bioengineering therapies geared toward spinal cord neuroprotection and functional regeneration.6-9
The acute medical and surgical treatment of SCI is targeted at ameliorating secondary injury. 3 To that end, the mantra, “time is spine”, has emerged, with strong evidence demonstrating improved neurological outcomes with early surgical decompression.10-13 The AO Spine CPG accordingly provide a strong recommendation for surgical decompression within 24 hours of injury.5,14,15 Further, the guidelines provide a weak (now termed conditional) recommendation to target a mean arterial blood pressure (MAP) of at least 75-80 mmHg and not higher than 90-95 mmHg for 3-7 days to optimize spinal cord perfusion. 5
The role of further neuroprotective strategies in the acute management of traumatic SCI remains an important knowledge gap and the target of future translational research. Many questions remain: What are optimal targets for MAP and spinal cord perfusion pressure, and what effect does this have on neurological outcome? When is a surgical decompression “sufficient” and what techniques can help with this assessment? How does early surgical decompression benefit different subforms of SCI, such as central cord syndrome (CCS)? 16
In this context, this review identifies and evaluates important studies related to contemporary concepts in the surgical management of patients with acute traumatic SCI and its subforms. It’s goal is to help fill these relevant knowledge gaps and provide recommendations 1 that may be useful for surgeons in their clinical practice.
Methods
To derive clinical practice recommendations, recent articles dealing with contemporary concepts of surgical decompression for acute traumatic SCI were selected for critical review by a group of experts on SCI research and treatment, assigned by the AO Spine Knowledge Forum SCI. The AO Spine Knowledge Forum SCI is a renowned group of international clinical experts in the field of SCI treatment and research, who aimed at extracting strong to conditional clinical recommendations that may be useful for spine surgeons in their clinical practice, using the well-established Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) system. 1 The goal of this review was to addresses some of the key knowledge gaps and to deliver an outlook for future directions in the surgical care of patients suffering from SCI and its subform CCS, thereby summarizing current evidence and delivering recommendations for spine surgeons to improve their clinical practice.
Article 1
Badhiwala JH, Wilson JR, Harrop JS et al. Early vs Late Surgical Decompression for Central Cord Syndrome. JAMA Surg 2022; 157: 1024-1032 DOI: 10.1001/jamasurg.2022.4454
Clinical Rationale
The rationale for early surgical decompression after acute SCI lies in its potential to mitigate secondary injury. 8 Moderate evidence supporting the benefits of early surgical decompression has emerged and was ultimately incorporated into the most recent AO Spine Praxis Spinal Cord Institute guidelines. 15 The guideline provides strong recommendation to offer early surgery within 24 hours after injury as an option for adult patients with acute SCI regardless of level.
With an ageing demographic, the incidence of CCS is rising, and it is expected to become the most prevalent subtype of acute traumatic SCI. 17 However, the role of early surgery in CCS is a subject of ongoing debates.18-23 Additionally, timely recognition and referral of patients diagnosed with CCS remain challenging, compounded by the heterogeneity of the diagnostic criteria for CCS. This highlights the need for stronger evidence to educate clinicians and facilitate effective knowledge transfer regarding the role and timing of surgery in CCS.
The aim of this study was to evaluate the efficacy of early surgery within 24 hours of injury in the context of CCS using a large prospective multicenter dataset.
Study Summary
This study used data from three large prospective multicenter studies, harmonized into a single data set of 186 propensity score-matched CCS patients. Participants included 93 patients who underwent early decompression (<24 hours) and 93 patients who had late decompression (≥24 hours). Key outcomes measured at 1 year included motor recovery (upper extremity motor score [UEMS], lower extremity motor score [LEMS], and overall American Spinal Injury Association [ASIA] motor score [AMS]) and functional outcomes (Functional Independence Measure [FIM]).
Results showed that early surgery was associated with significantly improved recovery in upper limb motor function (mean difference [MD], 2.3; 95% CI, 0-4.5; P = 0.047), while lower limb function did not improve significantly (MD, 1.1; 95% CI, −0.8 to 3.0; P = 0.30). However, early surgery was not associated with improved overall motor score (MD, 3.2; 95% CI, −0.2 to 6.6; P = 0.07). A higher proportion of patients in the early-surgery group appeared to achieve complete independence in various functional activities, particularly those involving upper limb function (e.g., eating, grooming, bathing, dressing). However, none of these associations reached statistical significance, and there was no significant difference in 1-year FIM motor score (MD, 4.4; 95% CI, −2.1 to 11.0; P = 0.20).
Subgroup analysis revealed that the benefits of early surgery were more pronounced in patients with AIS grade C injuries. Early decompression in this subgroup resulted in significantly greater recovery in overall motor score (MD, 9.5; 95% CI, 0.5-18.4; P = 0.04), driven by improvements in both upper (MD, 4.8; 95% CI, −1.3 to 11.0; P = 0.10) and lower limb motor function (MD, 4.2; 95% CI, 0.1-8.4; P = 0.046). In contrast, patients with AIS grade D injuries showed no significant difference in motor or functional recovery between early and late surgical decompression.
The results from this study suggest a benefit of early surgical intervention for patients with AIS grade C CCS. However, the benefit of surgical intervention within 24 hours for patients with less severe CCS (AIS D) remains uncertain. 24
Methodological Review
This study was a secondary analysis of previously prospectively collected data from three large independent prospective multicenter studies: the North American Clinical Trials Network (NACTN) SCI Registry, the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS), and the National Acute Spinal Cord Injury Study (NASCIS) III. Using propensity score matching to account for confounding variables, the study aimed to assess the effectiveness of early surgical decompression (within 24 hours post-injury) for patients with central cord syndrome (CCS). Eligible patients were those with motor-incomplete cervical spinal cord injuries (AIS grade C or D) and a motor score imbalance of at least 5 points between the upper and lower extremities. Primary outcomes, such as motor recovery (UEMS, LEMS, AMS), and secondary outcomes, including FIM scores, were evaluated 1 year after injury and imputed for 20% of patients with missing data. Subgroup analyses stratified by injury severity (AIS C or D) were conducted to explore variability in outcomes and potential ceiling effects for neurological recovery. Subgroup analysis showed that patients with AIS grade C injuries who underwent early surgery had a more profound recovery in the ASIA motor scores than did patients with AIS D at baseline. Although the overall sample size was substantial (n = 186), the study lacked sufficient power for subgroup analyses because most patients were classified as AIS D at baseline (78% early cohort, 74% late cohort).
In this study, the use of propensity score matching across large combined cohorts enhanced the ability to control for confounding factors, improving the reliability of the results. Considering the study’s relatively low proportion of missing data, adequate sample size, and rigorous methodology, the strength of evidence is assessed as moderate.
Recommendation for Integrating Into Your Clinical Practice
This study provides moderate evidence supporting early surgical decompression within 24 hours of injury in AIS C patients with acute CCS. Based on this evidence, risk/benefit of the intervention and likely patient values, we
Article 2
Aarabi B, Olexa J, Chryssikos T et al. Extent of Spinal Cord Decompression in Motor Complete (American Spinal Injury Association Impairment Scale Grades A and B) Traumatic Spinal Cord Injury Patients: Post-Operative Magnetic Resonance Imaging Analysis of Standard Operative Approaches. J Neurotrauma 2019; 36: 862-876 DOI: 10.1089/neu.2018.5834
Clinical Rationale
Current clinical practice recommends expeditious spinal cord decompresion and spinal stabilisation following acute traumatic SCI.10,25 Decompression may be achieved by anterior, posterior, or combined surgical approaches.26-28 Anterior surgery can relieve anterior mass effect and reconstitute the canal size. However, posterior decompression provides direct removal and expansion of the posterior spinal canal and traumatic region while also an indirect anterior decompression by increasing the canal diameter.26-28 Regardless of technique, the primary goal of surgery is to mitigate secondary injury and to improve spinal cord perfusion and stability of the spine. While the adequacy of surgical decompression is often assumed, it is often not routinely confirmed with imaging in the postoperative setting. This study sought to compare the effectiveness of different operative techniques in achieving a “complete” spinal cord decompression in patients with cervical motor complete SCI, as determined by the demonstration of a patent subarachnoid space (SAS) around the injured spinal cord on postoperative magnetic resonance imaging (MRI). 29
Study Summary
This was a retrospective cohort study of adults (≥16 years) treated at a single level I trauma center between 2001 and 2016. Patients with subaxial cervical motor complete SCI (AIS grade A or B) who underwent pre-operative (within 8 hours of injury) and post-operative (within 48 hours of injury) MRI were included. Operative techniques were separated into anterior cervical discectomy and fusion (ACDF) alone, anterior cervical corpectomy and fusion (ACCF) alone, laminectomy alone, ACDF plus laminectomy, or ACCF plus laminectomy. The primary outcome was complete (adequate; successful) spinal cord decompression, defined as the presence of a continuous column of cerebrospinal fluid (CSF) anterior and posterior to the spinal cord on T2 or short tau inversion recovery (STIR) MRI sequences.
The study comprised 184 SCI patients. Of these, 47 (25.5%) underwent ACDF alone; 29 (15.8%) ACCF alone; 29 (15.8%) laminectomy alone; 53 (28.8%) ACDF plus laminectomy; and 26 (14.1%) ACCF plus laminectomy. A complete spinal cord decompression with patent SAS was achieved in 121 patients (65.8%). Rates of adequate decompression for ACDF and ACCF alone were 46.8% and 58.6%, respectively. These increased when ACDF or ACCF were performed in conjunction with laminectomy to 71.7% and 73.1%, respectively. Laminectomy alone resulted in successful decompression in 86.2% of patients, with higher chances of achieving a patent SAS with the more levels of laminectomy performed. On multivariable logistic regression, laminectomy (either alone or in combination with ACDF or ACCF) was the only factor associated with complete decompression (OR 4.85, 95% CI 2.2-10.6, P < 0.001). An important observation from this paper was that in only 7 cases was an extensive posterior laminectomy still not enough to re-establish a patent SAS, suggesting that while conventional bony decompression techniques are sufficient in the vast majority of patients, there are still a small number of cases where spinal cord swelling could still cause “intradural” compression.
Methodological Review
This was a single-center retrospective observational cohort study. Enrollment was consecutive over a 16-year period and inclusion and exclusion criteria were clearly stated. An appropriate flowchart of study eligibility and enrollment was provided. Interventions (comparator groups) and outcomes were specified clearly and a priori. Patients underwent standard SCI assessment by ASIA or International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 30 A number of clinically relevant covariates, including demographic (e.g., age, sex), injury (e.g., mechanism of injury, Injury Severity Score [ISS], injury type [AOSpine subaxial cervical spine classification]), imaging (e.g., canal diameter, vertebral height, intramedullary lesion length [IMLL]), and treatment (e.g., time to surgery, operative technique) characteristics were assessed and included in the analysis. Co-interventions, including protocols relating to the initial rescue and resuscitation and steroid administration, were described in detail. Univariable comparisons were made by appropriate parametric and non-parametric tests. Univariable logistic regression was followed by multivariable regression to identify variables independently associated with outcome. The latter utilized a stepwise selection algorithm based on minimization of the Bayesian Information Criterion (BIC). Effect modification and interaction terms were included. Appropriate regression diagnostics were performed, including evaluation of collinearity, analysis of residuals, and examination of influential observations. The final model included age, sex, ISS, preoperative IMLL, post-operative IMLL, injury type, and performance of laminectomy.
This was a methodologically sound observational cohort study. Still, by virtue of the retrospective single-center design, there is risk of unmeasured confounding and selection bias. The quality of evidence is therefore rated as weak.
The authors conclude that although the importance of timely and complete decompression of the injured spinal cord is gaining wider recognition, the definition of sufficient decompression remains heterogeneous, and decompression has not been established according to evidence-based guidelines. This study highlights the significance of laminectomy as a supplemental or stand-alone procedure for achieving complete spinal cord decompression.
Recommendation for Integrating Into Your Clinical Practice
Based on the results of this methodologically rigorous observational study, we provide a conditional recommendation that laminectomy (+/− fusion) be considered, either for posterior-alone decompression or in addition to anterior decompression/fusion, to achieve circumferential spinal cord decompression in the setting of acute SCI.
Article 3
Chryssikos T, Stokum JA, Ahmed AK et al. Surgical Decompression of Traumatic Cervical Spinal Cord Injury: A Pilot Study Comparing Real-Time Intraoperative Ultrasound After Laminectomy With Postoperative MRI and CT Myelography. Neurosurgery 2023; 92: 353-362 DOI: 10.1227/neu.0000000000002207
Clinical Rationale
Intraoperative ultrasound (IOUS) offers real-time intraoperative guidance in many spinal surgical interventions, and provides critical information to guide surgical decision-making (extent of neural decompression, position of spinal implants, excision of tumors, etc.).31,32 IOUS has also been advocated as a tool to evaluate the extent of surgical spinal cord decompression in acute traumatic SCI. 33 While MRI is considered the imaging gold standard in evaluating spinal cord compression, no randomized study has directly compared the use of IOUS to post-operative MRI and CT myelography on the assessment of successful spinal cord decompression. Identifying this knowledge gap, Chryssikos el al. (2023) performed a retrospective study to address a specific research question: whether the degree of intraoperative decompression as evaluated by IOUS is equivalent to post-operative gold standard imaging. 32
Study Summary
Real-time IOUS was utilized in 51 consecutive patients who underwent IOUS evaluation during posterior cervical spine surgery for acute traumatic SCI at a single institution. The surgical plan consisted of posterior laminectomy with or without fixation in all cases, with 11 patients undergoing additional anterior surgery (corpectomy or discectomy) and fusion, either before or after laminectomy. Use of real-time IOUS resulted in 5 cases having additional laminectomy performed beyond the preliminary surgical plan during the index surgery, such that all 51 patients were determined to have adequate spinal cord decompression based on surgeon judgment of the IOUS findings at the time of laminectomy. A group of 5 reviewers independently evaluated the post-operative MRI and CT myelography images to determine if adequate decompression was achieved. Concensus was that 43/51 had adequate decompression and 8/51 patients had inadequate spinal cord decompression. Among these 8 patients with inadequate decompression on postoperative imaging, 6 would have benefited from additional bony decompression (laminectomy) and 2 had severe intradural spinal cord swelling and would have potentially benefited from expansion duraplasty (although extradural compression from epidural blood/fluid accumulation likely also played a role in reducing the patency of the CSF space around the injured cord). Smaller pre-/post-operative intramedullary lesion length (IMLL), higher AIS grade neurological injury, and less severe spine injury morphology were associated with satisfactory decompression.
Methodological Review
There were no statistical differences in the number of laminectomy levels, laminectomy width, use of posterior or anterior fusion, or the rostral/caudal-most level of laminectomy between those with adequate vs inadequate decompression. Nor were there differences in the timing of treatment including: time of injury to imaging, time from injury to surgery, or time between the pre- and post-operative imaging. Logistic regression analysis showed that IMLL was the strongest predictor of inadequate decompression, with greater IMLL having a higher likelihood of inadequate decompression on postoperative MRI or CT myelography. The study possesses high internal validity due to the limited number of operating surgeons and surgical practice. In the future, with further experience and careful comparisons, IOUS imaging capability could become comparable to post-operative MRI or CT myelogram.
Recommendation for Integrating Into Your Clinical Practice
Given the single-center, retrospective design of the study the overall quality of this evidence is low; however IOUS is a simple, inexpensive, noninvasive technique to assist surgeons during the operative treatment of acute traumatic SCI as it helps to confirm adequate spinal cord decompression. Thus we provide a
Discussion
Content Summary and Clinical Recommendations
This article explores topics that are critical knowledge gaps in the surgical care of acute SCI.15,16,34,35 First, the optimal management of patients with CCS remains unclear. In the context of a global aging population, CCS has become the most common form of acute SCI and hence is a topic of special relevance. 18 Article 1 was selected as it adresses the key question of whether patients with CCS benefit from early surgical decompression within 24 hours after injury; this has long been a topic of controversy. 24 Based on the results, a strong recommendation is provided to offer early surgery within 24 hours after injury as an option to patients with AIS C CCS, and a conditional recommendation to offer early surgery within 24 hours of injury for patients with AIS D CCS. 1
Articles 2 and 3 address the question of how to achieve and confirm sufficient surgical decompression of the spinal cord after acute traumatic SCI. While Article 2 examined the completeness of surgical decompression across different standard surgical approaches as measured by post-operative MRI, 29 Article 3 evaluated the utility of real-time ultrasound as an intra-operative adjunct to assess the extent of spinal cord decompression and its correlation with post-operative imaging. The results of Article 2 led the reviewers to derive a conditional recommendation that laminectomy be considered, either as a stand-alone operation or in addition to anterior surgery, to achieve circumferential spinal cord decompression in the setting of acute SCI. Following the results of Article 3, a conditional recommendation was derived that ultrasound is an effective tool to help confirm adequate spinal cord decompression intra-operatively in real-time.
In the near future, the phase III multicenter, prospective, randomized controlled DISCUS trial, which is still recruiting, is expected to deliver strong evidence and important answers to the question wether adjunct expansion duroplasty, in addition to standard bony decompression, is beneficial for the neurological outcome of patients with acute traumatic SCI. 36
Overview of Reviewed Articles and Clinical Recommendations According to the GRADE Methodology.
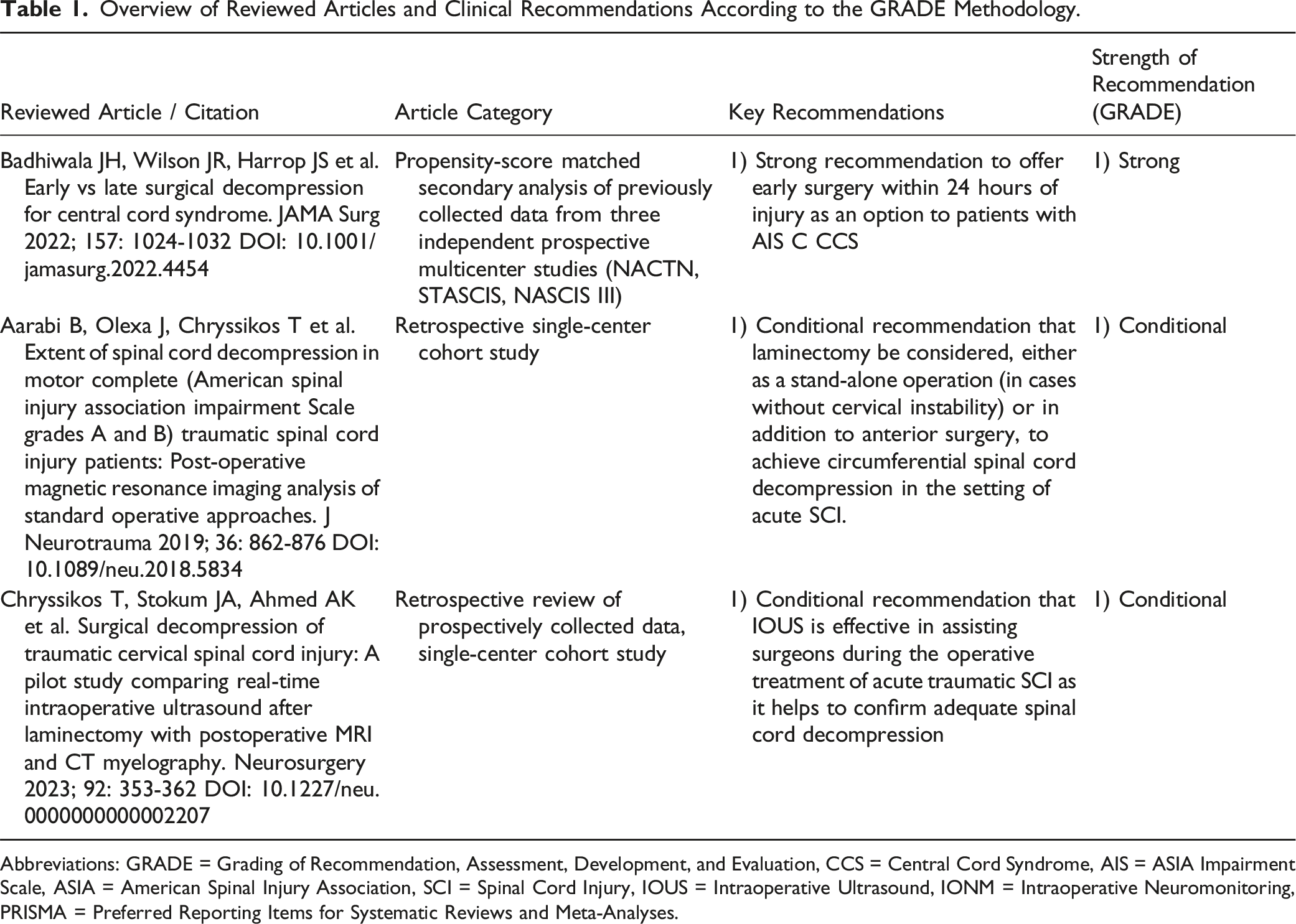
Abbreviations: GRADE = Grading of Recommendation, Assessment, Development, and Evaluation, CCS = Central Cord Syndrome, AIS = ASIA Impairment Scale, ASIA = American Spinal Injury Association, SCI = Spinal Cord Injury, IOUS = Intraoperative Ultrasound, IONM = Intraoperative Neuromonitoring, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Outlook
With its critical review of recent articles dealing with contemporary concepts of surgical decompression for acute traumatic SCI, this review addresses some of the key knowledge gaps and delivers an outlook for future directions in the surgical care of patients suffering from SCI and its subform CCS, thereby summarizing current evidence and delivering recommendations for spine surgeons to improve their clinical practice.
While the selection and critical review of the articles was up to the assigned experts, the AO Spine Knowledge Forum SCI is a renowned group of international clinical experts in the field of SCI treatment and research, who aimed at extracting strong to conditional clinical recommendations that may be useful for spine surgeons in their clinical practice, using the well-established Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) system. 1
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.