
Abstract
Study Design
Retrospective cohort study.
Objective
Spinal metastasis from hepatocellular carcinoma is rapidly progressive and predisposes to spinal disability, cord compression and further neural injury, leading to poor prognosis. Currently, it is still challenging to look for a treatment strategy that can improve the quality of life of patients and even directly prolong the survival time. This study attempts to evaluate the clinical efficacy of separation operation combined with postoperative stereotactic radiotherapy (SRT/SRS) in the treatment of hepatocellular carcinoma patients developing spinal metastasis and epidural spinal cord compression.
Methods
Patients with metastases spinal cord compression from hepatocellular carcinoma were studied retrospectively and divided into two groups, the SO group (who undergo separation operations combined with postoperative SRS, n = 32) and RT group (who received only SRS, n = 28). The visual Analogue Scale (VAS) pain score, Frankel grade, Karnofsky performance score, and Quality of Life (SF-36) score were comparatively analyzed between the two groups.
Results
Significantly higher VAS pain scores, Frankel grades, Karnofsky performance scores and Quality of Life (SF-36) scores were demonstrated in patients with combination treatment than in patients with SRS alone.
Conclusion
Separation operations are effective surgical procedure for the treatment of spinal metastatic tumor from hepatocellular carcinoma with spinal cord compression. The combination with postoperative SRS can significantly improve the quality of life in this patient population via spinal canal decompression and spinal stability reconstruction.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the major histological subtype of liver cancer and accounts for 90% of all primary liver cancers. Due to its high malignancy, HCC is prone to metastasize prior to diagnosis in the majority of patients. In this context, this patient population generally has poor clinical outcomes. Although advancements in diagnosis and treatment in recent years have led to prolonged survival time in patients with HCC, the 5-year survival rate remains as low as 16% and decreases to 4% upon extrahepatic metastasis.1,2 Spinal metastasis from HCC is the most common and can induce nerve root compression and even epidural spinal cord compression (ESCC) due to further tumor growth and invasion. In addition, patients with spinal metastasis may suffer strong cancerous pain, be at a higher risk of pathological fracture, and sometimes develop fatal hypercalcemia. Specifically, nerve root compression caused by tumor invasion can lead to stubborn radicular pain, while ESCC is associated with a series of more severe events, such as a decline in limb movement and sensory function, more critical irreversible spinal cord injury and paraplegia, which greatly affect the quality of survival in patients. It is noteworthy that the disease course is rapidly progressive once spinal metastasis from HCC occurs and is prone to metastasis to multiple internal organs, resulting in extremely poor prognosis.3,4
By the march of treatment therapies for the past few years, HCC patients with spinal metastasis have gained more survival benefits from surgeries, molecular-targeted agents, stereotactic radiosurgery (SRS), etc. 5 In addition, great care should also be taken to improve the quality of survival in these patients.
Conservative treatment is recommended for patients with spinal metastasis, while decompression and vertebroplasty are preferred in surgeries. In cases with concurrent spinal cord compression, especially those suffering rapid progression, surgical decompression should be arranged early to avoid irreversible injuries. The separation operation was first put forward by Laufer et al. 6 in recent years. It aims to block tumors invading the spinal canal through the complete decompression of the posterior lamina and accessories, partial resection of the anterior tumor body, reconstruction of mechanical stability, and separation of the dura from the anterior tumor based on bone cements. Generally, SRS will be performed after separation surgery to reduce the in-situ recurrence rate of spinal metastatic tumors. In our department, separation operations have been adopted for spinal metastatic tumors that are accompanied by ESCC and significant regional spinal destability and have been unable to be resected en bloc since January 2019. Pedicle screws and bone cements are concurrently used to help with stability reconstruction, followed by SRS postoperatively. Such a treatment strategy can fully suppress the progression of spinal metastasis, effectively reconstruct spinal stability and significantly improve the quality of life in patients. In the current study, separation operation followed by SRS was performed in 32 HCC patients suffering spinal metastasis and ESCC, with satisfactory clinical outcomes and improved quality of survival.
Materials and Methods
Clinical Data
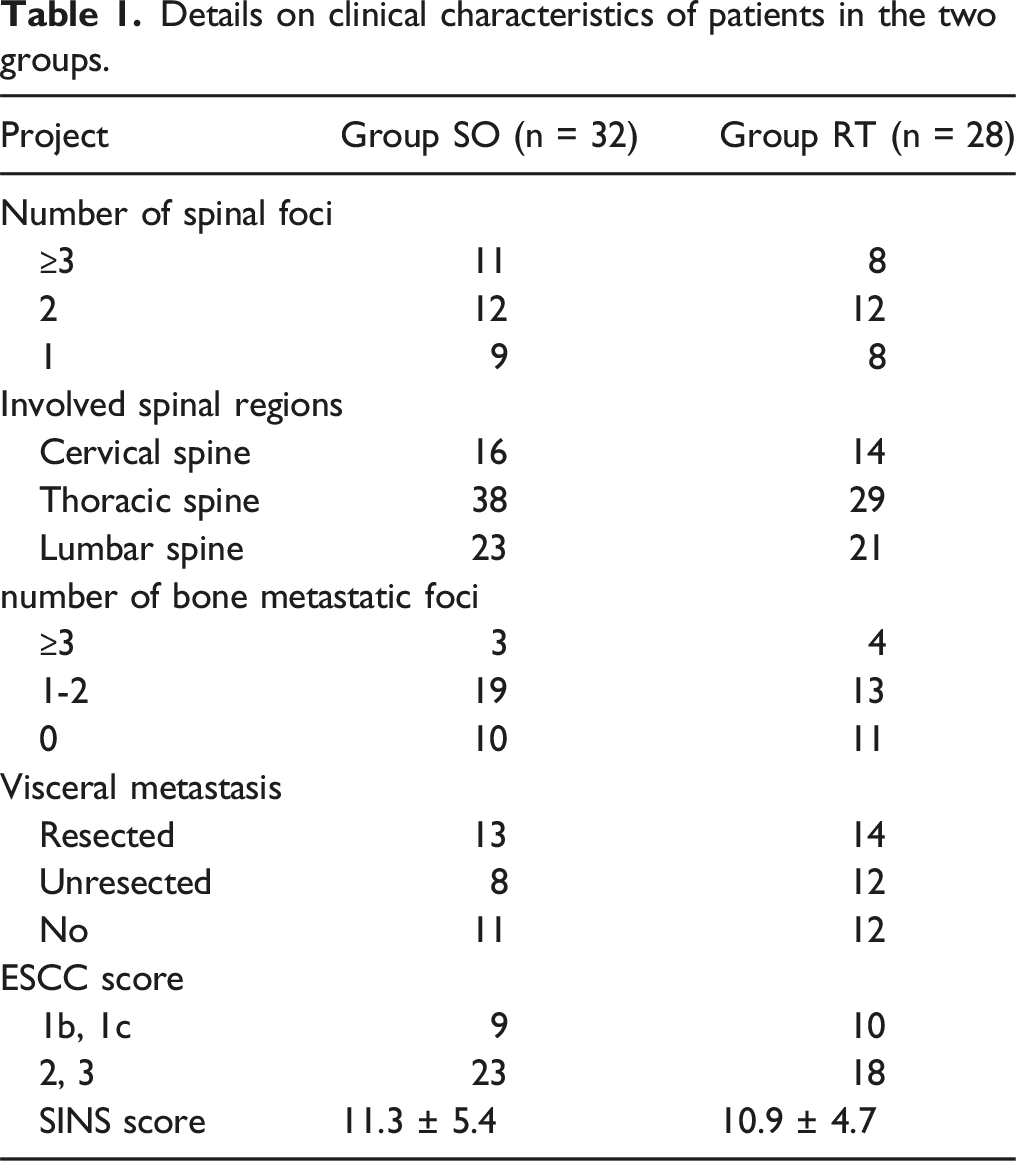
HCC patients (n = 60) who suffered spinal metastasis with ESCC and were admitted to Hunan Provincial People’s Hospital between January 2015 and December 2021 were enrolled in this study. Patients who received spinal separation surgery and subsequent stereotactic radiotherapy were included in the SO group (n = 32), and patients who only received stereotactic radiotherapy for local spinal metastasis were included in the RT group (n = 28). Approval for the study was obtained from Hunan Provincial People’s Hospital ethics committee (approval number 2021-S35) and informed consent obtained from all individuals.
Details on clinical characteristics of patients in the two groups.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) pathologically diagnosed as spinal metastasis from HCC by puncture or biopsy, and all the diagnoses were confirmed by postoperative pathology; (2) clinically presenting with regional spinal pain and movement disorder, all patients have neurological deficit or potentially have neurological deficit (neurologically intact at presentation in spite of ESCC); (3) complete imaging data (including liver CT, anteroposterior and lateral spinal radiographs, MRI), laboratory data and clinical data; (4) definite diagnosis of metastasis by whole-body radionuclide bone scan, thoracoabdominal and cranial CT, ultrasound, or PET-CT; (5) absence of any severe systemic disease, no definite contraindication for surgery and being surgery-tolerated.
Exclusion Criteria
(1) preoperative instability neoplastic score (SINS) < 7; (2) under poor physical condition and being intolerable to surgery; (3) suffering an uncontrollable primary tumor and expected to survive <3 months based on Tomita and modified Tohuhashi sore.
Therapeutic Strategies
Group SO
General anesthesia was achieved. Thoracolumbar metastasis was managed through the posterior approach. The involved accessories, pedicle, and posterior longitudinal ligament were fully resected and the affected spinal vertebral body was partially resected. A 360° circumferential decompression was obtained at the lesion level. Subsequently, the tumor tissues adherent to the dural sacs were carefully stripped and the anterior tumor tissues were also maximally scraped off. The defects were filled with soybean-sized, spherical bone cement (doughing time) to fully separate the anterior tumor and the dural sacs. Following hardening of the bone cement, internal fixation was performed using posterior pedicle screws, connecting rod and transverse connector (Figure 1). Cervical metastasis was usually managed through the posterior-anterior approach. After Posterior pedicle screw or lateral mass screw instrumentation was adopted for fixation, Steel plate instrumentation was applied for anterior fixation following resection of the tumor tissues and placement of a bone cement-based titanium mesh. Schematic picture of separation for thoracolumbar metastatic tumors. (A) Full resection of the spinous process and laminae, pedicle, and partial resection of the vertebral body invaded by the tumor, to complete 360° circumferential decompression; (B) filling of the defects with bone cements at doughing time to fully separate the anterior tumor and the dural sac; (C) internal fixation a posterior pedicle screw, connecting rod and transverse connector.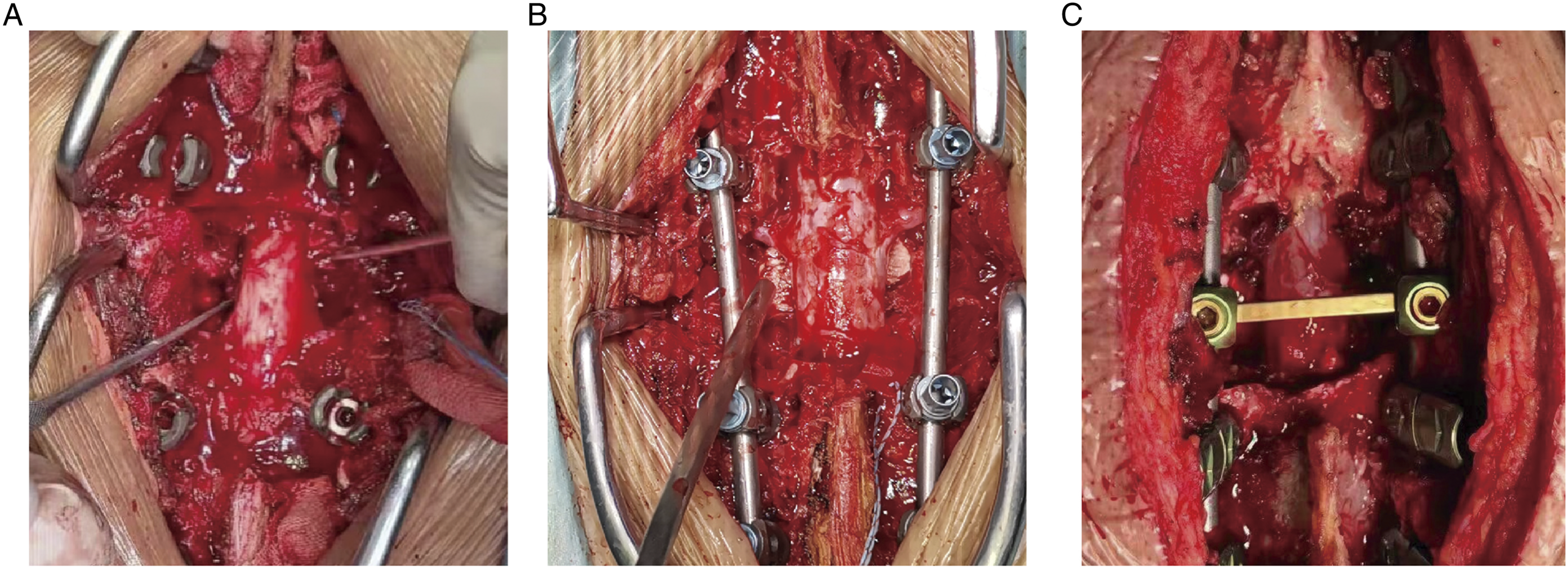
Postoperatively, routine infection prevention, hemostasis, analgesia, dehydration and symptomatic supportive therapy were provided. SRS was performed on the surgical area 3 weeks after surgery on the basis of good healing of the incision. Systemic antitumor treatments included chemotherapy, targeted therapy, immunotherapy and supportive therapy. An active pain-relieving strategy was highlighted, accompanied by psychological comfort and hospice care.
Group RT
SRS was carried out, during which bed rest was maintained. Systemic antitumor treatments were arranged in a manner consistent with that of Group SO. All the patients completed SRS at tumor radiotherapy center of our hospital.
Evaluation
Tomita scores 7 range from 0 to 10 points used to predict survival time and devise treatment plans based on patient tumor origin and metastasis.
Modified Tokuhashi score 8 is 15 points in total, on the basis of Karnofsky performance scores.
ESCC Class
Class 0, bone metastasis only 9 ; Class 1a, the crura is involved but remains normal in morphology; Class 1b, the crura is deformed but the spinal cord is not involved; Class 1c, the spinal cord is involved without compression; Class 2, the spinal cord is compressed, with surrounding cerebrospinal fluid (CSF); Class 3, the spinal cord is extruded to one side without surrounding CSF.
SINS scores 10 range from 0 to 18 points used to measure spinal stability, based on the specific location that the tumor invades the vertebral body to, bone and posterior damahe and spondylolisthesis.
VAS pain scores range from 0 (no pain) to 10 (most severe pain imaginable), which are self-reported based on the subjective feeing of pain.
Frankel Grading
A, no sensory and motor function; B, partial sensory function and no motor function; C, failure of independent walking with partial motor function; D, able to walk dependently with partial neural injury; E, normal.
Karnofsky performance score (%): 80-100% (normal performance), able of walking independently, normal daily life, and no special needs; 50-70% (medium performance), able to perform self-care but failing to work, requiring the assistance of another individual to some extent; <50% (poor performance), failure of self-care, rapid disease progression and requiring medical care.
Quality of life: Quality of Life (SF-36) was measured in Group SO at three time points: before the operation, at 1 week after the operation, and at 3 months after the operation. Assessment was performed in 8 simple dimensions, including physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE) and mental health (MH), and 3 composite dimensions including physical component summary (PCS), mental component summary (MCS), and role-social component summary (RCS).
Statistical Analysis
SPSS 22.0 was used for statistical analysis of the data. Measurement data are reported as the mean ± standard deviation. Comparisons for demographic data were completed using one-way analysis of variance (ANOVA). Inter- and intragroup comparisons were conducted using independent-sample t tests, and multigroup comparisons were performed by nonparametric rank sum tests. The examination standard was set as α = .05.
Results
32 patients in the SO group successfully completed the operation, and the operation time was 170-380 minutes, with an average of 255.2 minutes; The intraoperative bleeding volume was 300-2100 mL, with an average of 581.5 mL. During the perioperative period, 21 patients received allogeneic blood transfusion. After the treatment, the survival time was 5-23 months, with an average survival time of 10.6 ± 4.2 months. There was no postoperative internal fixation loosening, breakage and other related complications. Postoperative wound infection occurred in 2 cases, healing was achieved after debridement, drainage and systematic antibiotics in 1 case, and after dressing change in the other case. One case of upper thoracic vertebral metastatic tumor developed incision effusion after operation, which was healed after repeated fluid extraction and pressure bandaging. 28 patients in RT group also successfully completed radiotherapy, and the survival time after treatment was 6-17 months, with an average survival time of 9.5 ± 2.7 months. There was no significant difference in survival time between the two groups (P > .05).
VAS Pain Score
VAS pain scores before treatment and 1 week and 3 months after treatment.

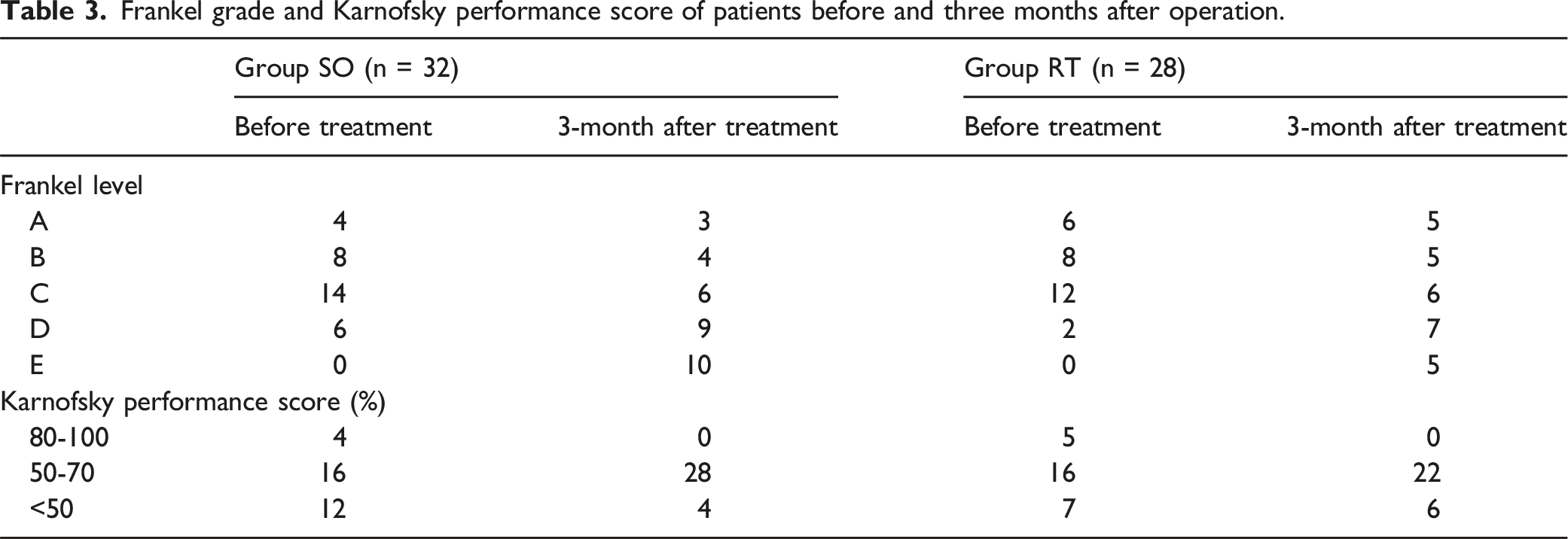
Frankel Grade and Karnofsky Performance Score
Frankel grade and Karnofsky performance score of patients before and three months after operation.
Quality of Life (SF-36)
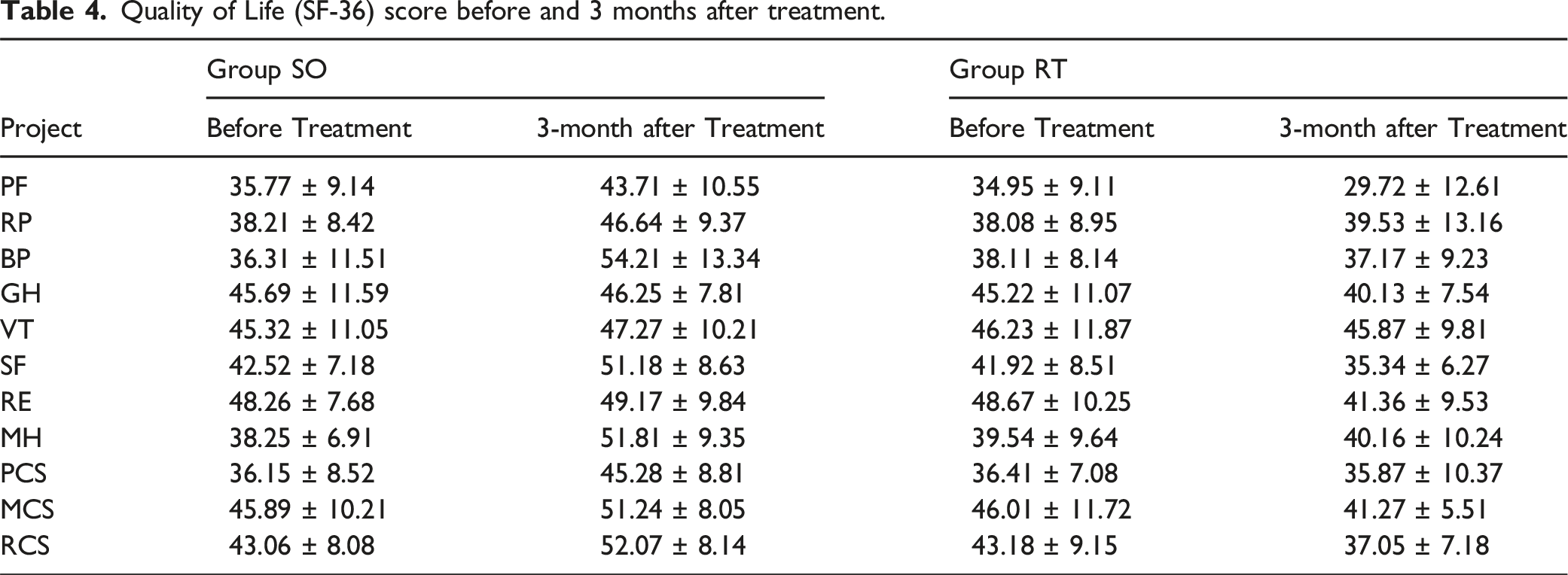
No significant difference in the Quality of Life (SF-36) score was observed between the two groups before treatment (P > .05). At the 3-month follow-up, Group SO witnessed great improvements in terms of PF, RP, BP, SF, MH, PCS, MCS, and RCS, compared to those before treatment (P < .05). Additionally, Group SO was superior to Group RT regarding PF, RP, BP, GH, SF, RE, MH, PCS, MCS, and RCS (P < .05).
Quality of Life (SF-36) score before and 3 months after treatment.
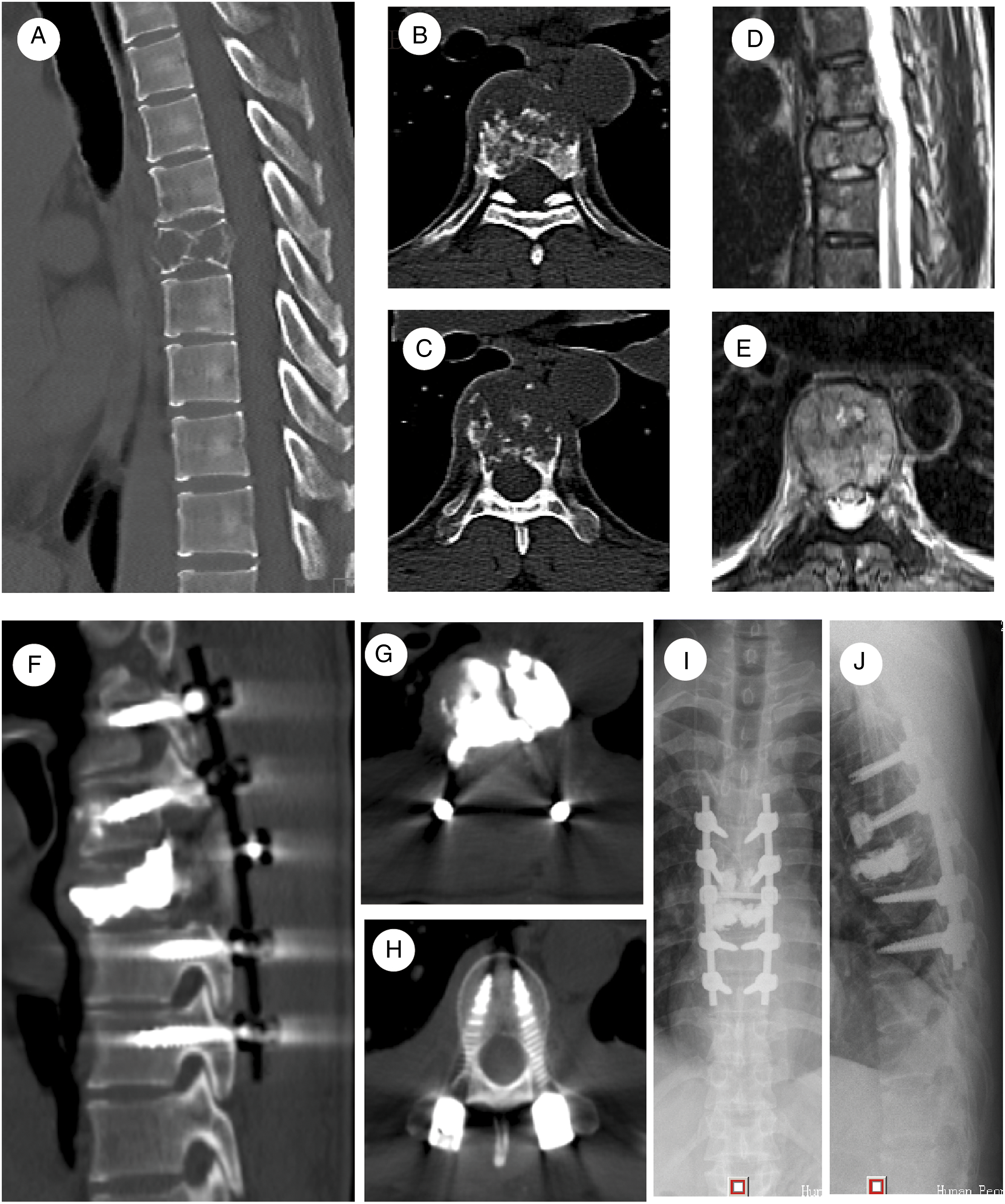
Typical imaging manifestations. (A-E) Osteolytic bone destruction in the thoracic vertebral body (T7) on preoperative CT and MRI, accompanied by dural sac compression due to tumor invasion (Tomita score 7, modified Tokuhashi score 11, SINS score 13, and ESCC Class 2). (F-J) Satisfied screw-rod internal fixation, bone cement filling in the thoracic vertebral body (T7), and complete separation between the dural sac and the anterior tumor on postoperative radiograph and CT.
Discussion
Spinal metastasis has long been considered a great challenge in the treatment of tumors. The literature reports that approximately 40% of patients with a malignant tumor die from the severe complications of bone metastasis. 11 Spinal metastasis from malignancy is generally accompanied by a series of severe complications, such as stubborn cancerous pain, unpredictable pathological fracture, and life-threatening hypercalcemia, which critically affect the quality of life of patients. HCC, a highly malignant tumor that is refractory and highly prevalent in China, is prone to spinal metastasis. In that way, the spinal canal is vulnerable to invasion, leading to nerve root and spinal cord compression, which make patients at a high risk of ECSS and result in poor clinical outcomes.
Individualized treatment and multidisciplinary combined therapy are currently recommended in the treatment of spinal metastasis. 12 Under this modality, a comprehensive evaluation of the degree of tumor metastasis and expected survival time of patients will be performed first. Tomita and Tokuhashi are well recognized scoring systems with wide applications. In addition, recent years have witnessed a new way to achieve a comprehensive analysis, which is performed at four levels: neurologic and oncologic issues that may affect tumor treatment, spinal mechanical instability, and systemic disease. 13 Second, based on the evaluation, a specific treatment plan will be made, such as surgery, radiotherapy, chemotherapy, targeted therapy, nuclear medicine therapy and immunotherapy. Finally, follow-up will be scheduled to give an overview of patient condition regarding pain, imaging manifestation and quality of life, which can help timely adjust the treatment to obtain better clinical outcomes.
Radiotherapy is currently the most common and effective treatment mode for radiosensitive tumors with spinal metastasis, such as myeloma, small cell lung cancer, lymphoma and breast cancer, with a satisfactory local control rate. However, for tumors which is not sensitive to radiotherapy, such as HCC, the local control rate is commonly not ideal. In recent years, SRS with more precise 14 and less complications comparing to conventional RT has improved therapeutic outcomes in this population to some extent. Nevertheless, long-course radiotherapy is generally accompanied by a series of adverse events involving in the immune system, hematopoietic system and other systems, while spinal irradiation can even lead to radiation-induced injuries, making patients at a high risk of irreversible neural damage. When performing SRS for spinal metastasis, we should pay particular attention not to be too close to the dural sac to avoid damaging the spinal cord. Therefore, the therapeutic effect of SRS on spinal metastasis will be greatly reduced when the tumor obviously compresses the dural sac or has obvious adhesion. Moreover, the residual local instability after radiotherapy is also a problem that needs to be paid attention to for the spinal metastatic tumor with severe local osteolysis destruction.
Under this background, separation operations have emerged. 6 It aims to eliminate spinal cord compression, partially resect the tumor, separate the anterior vertebral body and the dural sac using bone cements and perform posterior fixation. In this way, tumor invasion to the spinal canal can be further inhibited. Additionally, the spinal cord can be less damaged under high-dose SRS. It is also noteworthy that the combination of separation operation with postoperative SRS is associated with a lower rate of in situ recurrence. Before the formal proposal of “separation surgery”, the results of a prospective randomized controlled clinical study led by Patchell et al 15 indicated that for symptomatic spinal metastases, postoperative radiotherapy after spinal decompression surgery provided better functional outcomes and pain control compared to radiotherapy alone. In addition, surgical intervention increased the likelihood of walking recovery, maintained walking for a longer time, and had a smaller survival advantage. Since then, more and more scholars have recognized the therapeutic value of separation surgery for spinal metastases. For instance, the results of a prospective multicenter AOSpine study proved that surgical intervention provides immediate and continuous improvement in pain, nervous system, function, and Health-related Quality of Life (HRQOL) outcomes, with an acceptable risk for patients with locally symptomatic metastatic epidural spinal cord compression lesions and a survival prognosis of at least 3 months. 16 Liu’s study 17 suggested that separation surgery-radiosurgery therapy is a safe and effective treatment option for patients with metastatic epidural spinal cord compression, and stereotactic radiotherapy provided higher local control rates compared with image-guided intensity-modulated radiotherapy. Laufer et al. 18 retrospectively analyzed 1515 patients with spinal metastasis at the largest cancer center in the United States, and all patients previously received either hybrid therapy (ie, separation surgery and radiotherapy) or only posterior instrumentation for instability with concomitant radiotherapy. The results showed an improvement in overall survival by 1% with each successive year after surgery mainly in patients with lung, renal, and colon cancer. Those large-scale clinical research data all demonstrated the benefits of surgical intervention, especially separation surgery, in improving the quality of life and even prolonging the survival period of patients with spinal metastases. Based on all the previous results, there is a viewpoint that the combination of systemic and local treatment strategies is expected to improve patient survival, and continuous progress will address the need for improved survival in patients with metastatic spinal disease. 19 However, as of now, there have been no report specifically analyzing the role of separation surgery - stereotactic radiotherapy in spinal metastasis from HCC.
In the current study, a separation operation was adopted for patients with spinal metastases from HCC, which were accompanied by ESCC and significant regional spinal disability and were unable to be resected en bloc. Pedicle screws and bone cements were concurrently used to help with stability reconstruction, followed by SRS postoperatively. At follow-up, patients receiving such a separation surgery-stereotactic radiotherapy treatment strategy had less pain, more stable efficacy, and higher quality of survival, which were superior to those of patients receiving SRS alone.
Therefore, we recommend that the treatment modality combining separation operation and postoperative SRS is a viable option for spinal metastases from HCC, which are accompanied by ESCC and significant regional spinal disability and are unable to be resected en bloc. Such a modality can achieve full spinal cord decompression and spinal canal stability, decrease second spinal cord compression due to in situ recurrence, and eventually alleviate patient pain and improve the quality of survival.
Of course, this study also suffers from some shortcomings. This study is a retrospective study rather than prospective study, and there exist selection and information bias, so the conclusions obtained are less reliable than randomized controlled trial. The number of cases included in this study is relatively small, and studies with larger sample sizes may yield more reliable or even different results. Furthermore, the separation surgery conducted in this study is an open surgery with significant trauma and slow postoperative recovery. How to improve the surgical techniques to minimize trauma will be the future direction of development. 20
ORCID iD
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.