
Abstract
Spinal ependymomas comprise ~60% of all intramedullary tumors in adults. Ependymomas demonstrate distinct imaging features, such as central location within the spinal cord, symmetrical expansion, intra- and extratumoral cysts, hemosiderin caps, and strong enhancement on contrast-injected, T1-weighted magnetic resonance (MR) imaging. In adults, most ependymomas are myxopapillary, and in children, most are nonmyxopapillary. In general, nonmyxopapillary or classic ependymomas are hyperintense on T2- and hypointense on T1-weighted MR imaging, but whereas the signal intensity on T1 and T2 is variable, homogeneous contrast enhancement is usually a characteristic finding. Here, the authors provide an overview on spinal ependymomas with an emphasis on imaging characteristics and morphological background and present the case of a World Health Organization grade II ependymoma in the conus that did not enhance. Interestingly, the tumor contained a large hemorrhagic cyst. Just as hemorrhagic metastatic tumors may not enhance, a hemorrhagic ependymoma may likewise not enhance after administration of contrast agent. Thus, the differential diagnosis of a nonenhancing intramedullary lesion in the conus should include ependymoma, particularly if there is concomitant hemorrhage.
Ependymomas are the most common intramedullary spinal cord tumors in adults. They can be broadly grouped as either myxopapillary ependymomas or classic nonmyxopapillary ependymomas. Spinal ependymomas have characteristic features that can be observed both radiologically and grossly, including cystic components and hemorrhagic elements with hemosiderin caps. Moreover, spinal ependymomas almost always exhibit strong contrast enhancement on magnetic resonance (MR) imaging, with a sharp margin of enhancement around the tumor margin. The authors review histopathologic, clinical, and radiographic characteristics of spinal ependymomas and report a case of nonenhancing classic nonmyxopapillary intramedullary spinal ependymoma, which likely represents the first description in the literature of a histologically proven nonmyxopapillary ependymoma that failed to enhance after administration of intravenous contrast agent.
Case Report
History and Presentation
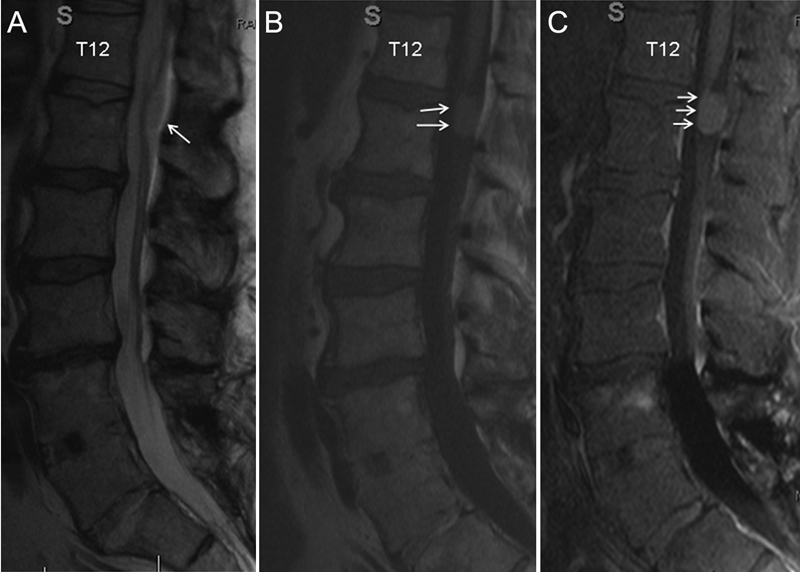
The patient is a 27-year-old woman who presented with a 4-year history of progressively worsening low back pain, which radiated to the buttocks and occasionally into the right leg and foot. The pain was exacerbated by activity, and rest provided mild relief. The patient also complained of bilateral lower extremity numbness and increasing urinary frequency. Findings on her neurological examination were normal except for absent deep tendon reflexes in the lower extremities. MR imaging of the lumbar spine revealed a complex, 17 × 73-mm, nonenhancing cystic mass at the level of the conus extending from the superior aspect of T12 to the midlevel of the L2 vertebral body. T2-weighted MR imaging showed a fluid/fluid level, consistent with a hemorrhagic component, and large amounts of intracystic hemosiderin deposits. There was minimal septal and peripheral enhancement in the lesion, with no evidence of enhancement anywhere else in the lesion (Fig. 1). An associated hydrosyringomyelia in the lower thoracic region, mild posterior wall scalloping of the T12 and L1 vertebral bodies, and mild kyphosis suggested a long-standing process (Fig. 2).
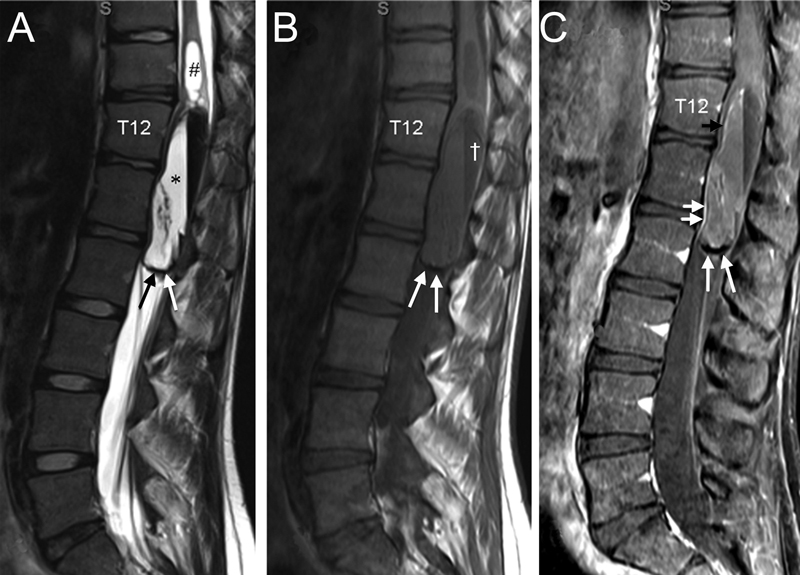
T2-weighted (A), T1-weighted (B), and contrasted T1-weighted (C) magnetic resonance images of the lumbar spine and thoracolumbar junction showing a complex cystic lesion, which extended from the superior aspect of T12 through the mid L2 vertebral body and expanded the conus. (A) A separate cyst (#) within the central spinal cord was demonstrated superior to the main collection (*). There was a fluid/fluid level with hypointense layering dependently and a hyperintense layering antidependently. It also revealed a peripheral hemosiderin ring (arrows in A to C). The dependent layering was hypointense on T1-weighted imaging († in B), and there was minimal septal and peripheral enhancement (short arrows in C).
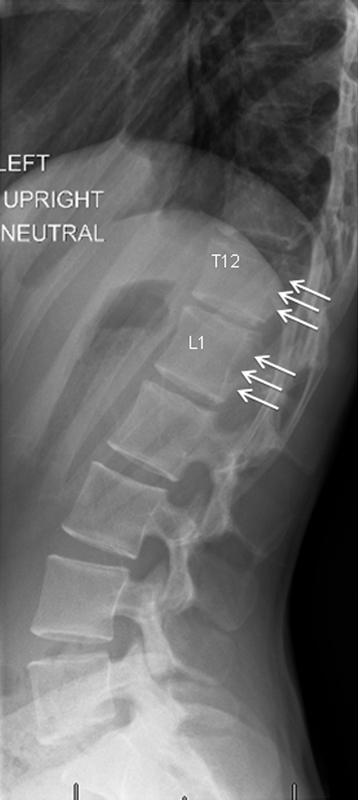
Radiograph showing mild posterior wall scalloping of T12 and L1 (arrows) suggesting a long-standing process.
Surgery
An open biopsy and potential resection of the lesion was recommended to the patient. The lesion was approached via en bloc removal of the laminae T10 to L1 and a partial laminectomy of L2 to expose the spinal canal along the entire pathological area including the cephalad cyst and to find normal spinal cord rostral to the lesion. After the thecal sac and arachnoid were opened, large amounts of hemosiderin and hemorrhage were seen (Fig. 3). The filum terminale was identified using electrical stimulation, cauterized, and sectioned. The conus-expanding cyst was completely drained, and deep to the cyst, biopsies from the solid portion of the tumor were obtained. Because intraoperative frozen sections displayed small blue cells consistent with lymphoma, proceeding with an aggressive resection was not indicated as it could potentially aggravate or cause new neurological deficits. Thus, the dura was closed after partial resection of ~30% of the lesion. The T10 to L1 laminae were replaced and fixed with cranial microplates.
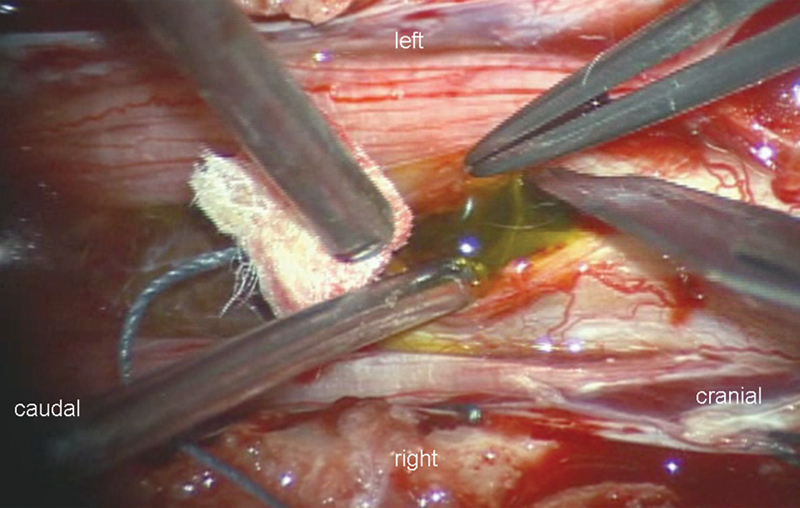
Intraoperative photograph showing the surgical site after the thecal sac and arachnoid were opened. Large amounts of hemosiderin are seen upon entering the tumor in the conus.
Pathological Analysis
Histopathologic analysis revealed evidence of rosettes and perivascular pseudorosettes on hematoxylin and eosin–stained slides (Fig. 4). The tumor cells showed heterogeneous positive staining for glial fibrillary acidic protein and S-100 markers, as well as focal apical membranous and intracytoplasmic punctate staining for epithelial membrane antigen (Fig. 4). The tumor cells were negative for Melan A and HMB45 markers. In addition, marked piloid gliosis and deposits of hemosiderin pigment were present. The final diagnosis was ependymoma World Health Organization (WHO) grade II.
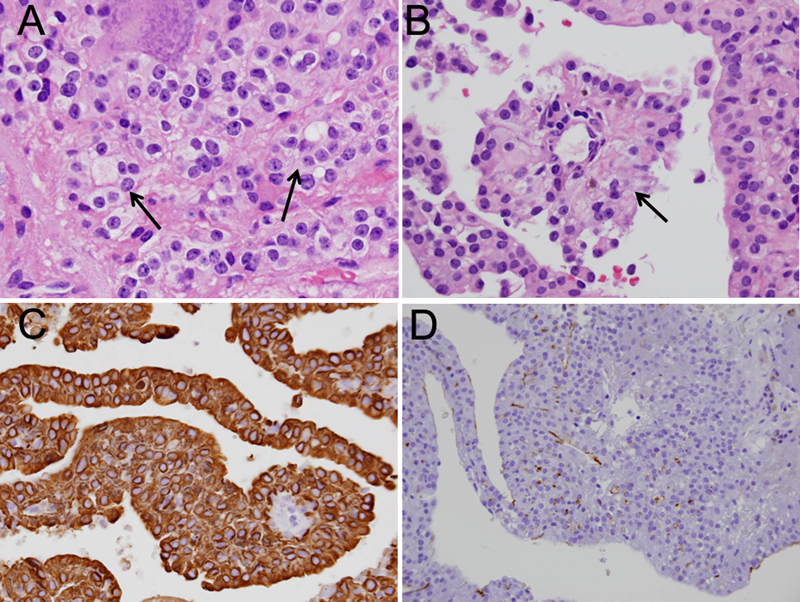
Histopathologic samples of the tumor showed rosettes (A, arrows) and perivascular pseudorosettes (B, arrow) on hematoxylin and eosin–stained slides. The tumor was strongly positive for glial fibrillary acidic protein (C) and focally positive for epithelial membrane antigen (D). The diagnosis was ependymoma.
Follow-up
The patient elected to proceed with observation of the lesion by regular MR imaging scans. At 6-month follow-up, the lesion had slightly decreased in size, and the patient had not experienced any new neurological deficits (Fig. 5).

X-ray and magnetic resonance images at 6 months’ follow-up. Sagittal alignment is conserved (A). Magnetic resonance images (B and C) shows the partially resected tumor. A slight decrease in size and subtotal involution of the cephalad cyst is noted.
Discussion
Clinical Overview of Spinal Cord Ependymomas
Intramedullary spinal cord tumors account for 4 to 10% of all central nervous system (CNS) tumors. 1 The most common intramedullary spinal cord tumors in adults are ependymomas, comprising ~60% of all such tumors. 1 , 2 , 3 , 4 In the pediatric population, ependymomas are the second most common intramedullary spinal tumors after astrocytomas, constituting ~30% of all pediatric intramedullary spinal lesions. 5
Ependymomas are benign, slow-growing tumors 6 that can arise anywhere in the neuraxis. They originate from ependymal cells that line the cerebral ventricles and the spinal canal. Hence, they normally occupy a central location within the spinal cord and expand symmetrically, which can cause interruption of spinothalamic tracts. 1 This is useful in differentiating them from the infiltrating asymmetric appearance of astrocytomas. Intramedullary spinal ependymomas are occasionally associated with neurofibromatosis type 2. 1
Spinal ependymomas exhibit a bimodal age distribution, with peaking incidences in the third and sixth decades, and with a mean age of diagnosis around 38.3 years of age. 1 There is a slight male predominance (between 54% and 58%). 1 , 7 The clinical symptoms of spinal ependymomas are usually mild, leading to delay in diagnosis. The mean duration of symptoms prior to diagnosis is 36.5 months. 1 The most common symptoms associated with intramedullary spinal ependymomas include back or neck pain (67%), sensory deficits (52%), motor weakness (46%), and bowel or bladder dysfunction (15%). 1 Prognosis depends on the preoperative neurological status, the grade and histological type of the tumor, the comprehensiveness of the surgical resection, and the evidence of dissemination. 8 , 9 Although spinal ependymomas lack a capsule, it is generally possible to develop a clear plane between the tumor and spinal cord and achieve a complete resection. 4 , 7 , 10 , 11 Shorter duration of symptoms usually correlates with better postoperative outcome. 12 The 5-year rate of survival is ~82%. 1 Postoperative radiotherapy after complete resection does not prolong survival. 8 , 11 It is reserved for recurrent disease or lesions that undergo subtotal resection, 10 , 12 , 13 , 14 both of which may also be considered for revision surgery. 15
Histopathologic and WHO Classification of Spinal Ependymomas
Histopathologically, spinal ependymomas usually appear as uniform cells with moderately hyperchromic nuclei.16 There are five different histopathologic types of spinal ependymomas, namely cellular, tanycytic, epithelial, papillary, and myxopapillary. The most common histological subtype of spinal ependymomas is the cellular type. These are made of either cuboidal cells or low columnar cells and are characterized by the presence of perivascular pseudorosette formation, in which the neoplastic ependymal cells are distributed in a ring fashion around blood vessels.17 Tanycytic ependymomas comprise elongated cells similar to the cells seen in astrocytomas. Epithelial ependymomas are composed of either linear or glandular arrangements of cells that form true ependymal rosettes. Papillary ependymomas are rare and are histologically similar to choroid plexus papilloma. 7 Myxopapillary ependymomas arise almost exclusively from the filum terminale and represent 30% of all spinal ependymomas. 18 Myxopapillary ependymomas are distinguished by their intracellular and perivascular accumulation of mucin. 18 In fact, myxopapillary ependymoma is the only histological subtype of spinal ependymomas that can be distinguished based on neuroimaging.
According to the WHO grading system, ependymomas can be broadly classified into one of three different categories. WHO grade I tumors are either subependymomas or myxopapillary ependymomas. WHO grade II lesions are low-grade, nonanaplastic tumors, and WHO grade III ependymomas exhibit anaplastic features and mitotic figures. Overall, about half of intramedullary spinal cord ependymomas are classic ependymomas (mainly WHO grade II), and the other half are of the myxopapillary type (WHO grade I), although this distribution varies with age. In adults, most spinal ependymomas are of the myxopapillary type (WHO grade I), which occur almost exclusively at the filum terminale and within the conus or the cauda equina (Fig. 6). 5 , 16 On the other hand, pediatric spinal ependymomas are more commonly classic nonanaplastic ependymomas (WHO grade II). 5
T2-weighted (A), T1-weighted (B), and contrast-enhanced T1-weighted magnetic resonance (MR) imaging showing myxopapillary ependymoma (World Health Organization grade I) at the filum terminale. This is the most common spinal ependymoma in the adult population. The myxopapillary ependymoma is hyperintense on T2- and T1-weighted MR images (arrows in A, B). It enhances homogeneously with contrast agent (short arrows in C).
The location of spinal cord ependymomas usually correlates with their WHO grade. For instance, classic spinal cord ependymomas are most common in the cervical region (67%; Fig. 7), followed by the thoracic region (49%), distal cord, and the conus medullaris (6.5%). 1 , 6 On the other hand, myxopapillary ependymomas (WHO grade I) are the most common type of primary tumors in the lower cord, conus, cauda equina, and filum terminale. 6 , 19
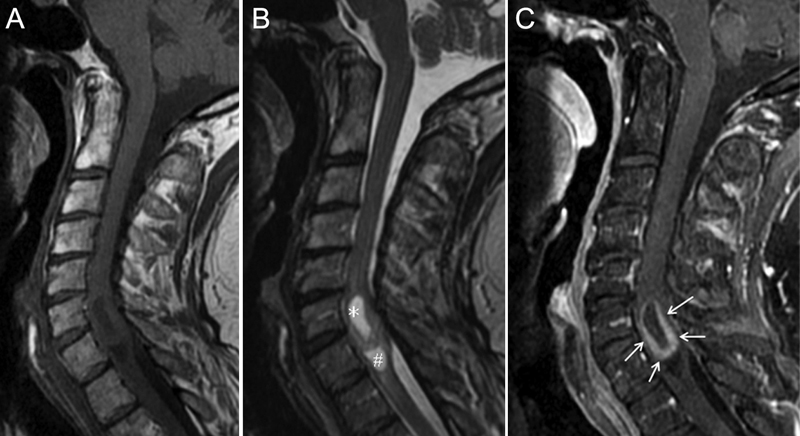
A classic ependymoma (World Health Organization grade II) in the cervical spine on sagittal T1-weighted (A), T2-weighted (B), and T1-weighted magnetic resonance images after injection of gadolinium (C). It is centrally located within the spinal cord, is cystic (*) with peripheral enhancement of the solid tumor portion (arrows), and reveals an inferior polar cyst (#).
Cystic Components in Intramedullary Spinal Ependymomas
Between 50% and 85% of spinal ependymomas are associated with cystic components. 1 , 7 , 19 , 20 , 21 , 22 These cysts may be either intratumoral, rostral to the lesion, or caudal to it (Figs. 1 and 7). 1 , 7 More than one type of cystic change may exist in the same patient: Intratumoral cysts are also known as true tumoral cysts and occur in ~24% of all cases of intramedullary spinal ependymomas (Figs. 1 and 7). 23 They are thought to be secondary to degeneration, necrosis, and liquefaction within the lesion itself, 7 and administration of contrast agent results in peripheral rim enhancement around the cyst. 1 , 7 , 24 , 25 Cysts of the central canal are thought to be caused by reactive dilation at the rostral or caudal pole of the tumor (polar or satellite cysts) or obstruction of the central canal. 1 , 7 These occur in ~62% of all cases of intramedullary spinal ependymomas23 and do not enhance (syringomyelia; Fig. 7). 1 , 7 Intratumoral cysts—the only cystic changes with peripheral enhancement after administration of contrast material—must be distinguished from the other two types of cystic changes because they must be included in the excision in light of the fact that they may be lined with abnormal tumorigenic glial cells. 21 , 25 In tumors associated with rostral/caudal cysts, only the solid lesion needs to be resected, and the cysts may be drained or aspirated during surgery. 1 , 7 , 25 Secondary reactive cysts tend to resolve on their own after excision of the tumor. 7 , 25 Moreover, ~60% of spinal ependymomas are associated with cord edema.
Hemorrhage in Intramedullary Spinal Ependymomas
Hemorrhage is a common finding in spinal ependymomas, and the presence of a hemosiderin cap is considered almost pathognomonic for these tumors. This hemosiderin cap appears as a “cap sign” on T1- and T2-weighted MR images as a rim of extreme hypointensity along the tumor margin at the interface between the tumor and the spinal cord (Fig. 1). 1 , 26 Between 20% and 33% of all spinal ependymomas are associated with this cap sign. 1 In certain cases, spinal ependymomas can result in subarachnoid hemorrhage. 27 , 28 In one study of 26 spinal ependymomas conducted by Kahan et al, 7 ~20% of all lesions demonstrated evidence of chronic hemorrhage on MR imaging. The pathophysiology behind hemorrhage in spinal ependymomas remains a topic of debate. Some authors attribute it to the high vascularity of the tumor, 29 , 30 and others attribute it to the interface between the ependymoma and the normal cord that is vulnerable to bleeding. 26
Neuroimaging of Intramedullary Spinal Ependymomas
On neuroimaging, spinal ependymomas usually span three to four vertebral segments, 30 although the involvement of as many as 15 segments has been reported. 1 In ~10% of cases, MR imaging demonstrates evidence of long-standing tumor lesions, evidenced by the presence of bone remodeling, scoliosis, erosion of the medial aspect of the pedicles, laminar thinning, and scalloping of the posterior vertebral bodies (Fig. 2). 1 , 3 , 31 These osseous changes are most commonly caused by ependymomas arising at the lumbar and lumbosacral spine. 7
The two main imaging modalities used for the assessment of spinal ependymomas are computed tomography (CT) and MR imaging, the latter being the imaging modality of choice. CT has the advantage of demonstrating subtle foci of calcification within the tumor, which is particularly useful in intracranial ependymomas, but calcification is uncommon in spinal ependymomas. 1 , 5 MR imaging is superior in defining the size and properties of the lesion. 1 Moreover, MR imaging is more sensitive than CT in the detection of leptomeningeal spread and in the characterization of associated structural abnormalities such as cysts, hemorrhage, or edema. 1 , 32 Classic nonmyxopapillary spinal ependymomas usually demonstrate high T2 signal intensity and low T1 signal intensity (Fig. 7) 5 , 7 , 23 , 33 ; however, ~20% of spinal ependymomas demonstrate low T2 signal, which is suggestive of isolated hemorrhage. 34 Moreover, a significant percentage of myxopapillary ependymomas are hyperintense on both T1- and T2-weighted images, likely because of the presence of a significant amount of mucin (Fig. 6). 7 , 18 , 23 , 33
Contrast Enhancement in Intramedullary Spinal Ependymomas
Contrast-enhanced MR imaging has been used as a diagnostic tool since 1984 35 and was first employed for the diagnosis of intraspinal tumors in 1985. 36 For a long time, enhancing intramedullary spinal lesions were considered tumorigenic until proven otherwise, and nonenhancing lesions were consequently considered benign. 22 , 36 , 37 , 38 In fact, contrast enhancement has been demonstrated in all types of spinal cord neoplasms, regardless of the grade or the degree of invasiveness. 25 Contrast enhancement has been ascribed to the actively dividing nature of these tumors, and it has been hypothesized that the invasive nature of malignant tumors results in fenestration of the endothelium and subsequent leakage of contrast material into the extravascular space. 1 , 25 It is well accepted that spinal ependymomas almost always enhance intensely after administration of intravenous contrast material. 1 , 2 , 3 , 5 , 7 , 10 , 33 , 39 , 40 , 41 For instance, in a study of seven intramedullary spinal ependymomas of all WHO grades conducted by Parizel et al., 37 all seven ependymomas demonstrated complete contrast enhancement after administration of contrast material. In addition to their overall contrast enhancement, spinal ependymomas usually demonstrate a sharp margin of enhancement around the tumor margin. 10 , 34
Here we report the rare case of a nonenhancing spinal cord ependymoma, which was histologically proven to be a WHO grade II lesion. Although some have suggested that the absence of contrast enhancement does not necessarily exclude the possibility of intramedullary neoplastic lesions,24 only a few authors have reported cases of histologically proven nonenhancing spinal tumors. 42 Failure to enhance after contrast administration seems to be a characteristic of tumors associated with significant hemorrhagic components. For instance, although metastatic tumors of the CNS almost always exhibit contrast enhancement, 43 this enhancement is occasionally minimal to absent in metastatic CNS tumors associated with significant hemorrhage. 44 , 45 In addition to hemorrhage, some authors have suggested that the isolated nature of certain tumors results in a pattern of minimal to no enhancement on MR imaging. 44 In a study of 130 intramedullary spinal cord tumors, White et al 25 found 11 cases (9%) that failed to enhance. Eight of these nonenhancing tumors were astrocytomas, and one was a subependymoma. The series comprised 83 ependymomas, all of which showed full enhancement pattern. In fact, one of the most well-established radiological features of spinal ependymomas is their ability to exhibit intense homogenous enhancement on postcontrast MR imaging. 1 , 2 , 3 , 5 , 7 , 10 , 33 , 39 , 40 , 41 Only rarely does one find cases in the literature of spinal ependymomas with minimal to no enhancement. For instance, out of 16 spinal ependymomas reported by Kahan et al, 7 3 (19%) demonstrated only rim enhancement, 1 (6%) demonstrated minimal enhancement, and 1 (6%) demonstrated no enhancement at all. The nonenhancing lesion was a myxopapillary ependymoma, and the histopathologic type and WHO grade of the minimally enhancing and only rim-enhancing lesions were not reported. More than a decade later, such cases of spinal ependymomas with abnormal patterns of enhancement remain poorly documented in the literature. Our present case report likely represents the first report in the literature of a histologically proven nonmyxopapillary ependymoma that failed to enhance after administration of intravenous contrast.
Conclusion
Spinal ependymomas are the most frequent intramedullary tumor in adults. In general, complete removal of these surgically amenable lesions should be attempted as this improves prognosis. Spinal ependymomas demonstrate distinct imaging features, such as intra- and extratumoral cysts, hemosiderin caps, and strong enhancement of the solid tumor portion, which aid to establish a preliminary preoperative diagnosis. Nevertheless, our illustrated case report suggests that lack of enhancement after administration of contrast agent does not preclude the diagnosis of a spinal ependymoma, particularly when the imaging study reveals hemorrhage into the tumor.
Disclosures
Andrew A. Fanous, None
Gregory F. Jost, None
Meic H. Schmidt, None
Footnotes
Acknowledgments
We thank Kristin Kraus, M.Sc., for editorial assistance with this paper.