
Abstract
Study design
Guideline
Objectives
To develop an international guideline (AOGO) about the use of osteobiologics in anterior cervical discectomy and fusion (ACDF) for treating degenerative spine conditions.
Methods
The guideline development process was guided by AO Spine Knowledge Forum Degenerative (KF Degen) and followed the Guideline International Network McMaster Guideline Development Checklist. The process involved 73 participants with expertise in degenerative spine diseases and surgery from 22 countries. Fifteen systematic reviews were conducted addressing respective key topics and evidence was collected. The methodologist compiled the evidence into GRADE Evidence-to-Decision frameworks. Guideline panel members judged the outcomes and other criteria and made the final recommendations through consensus.
Results
Five conditional recommendations were created. A conditional recommendation is about the use of allograft, autograft or a cage with an osteobiologic in primary ACDF surgery. Other conditional recommendations are about the use of osteobiologic for single- or multi-level ACDF, and for hybrid construct surgery. It is suggested that surgeons use other osteobiologics rather than human bone morphogenetic protein-2 (BMP-2) in common clinical situations. Surgeons are recommended to choose 1 graft over another or 1 osteobiologic over another primarily based on clinical situation, and the costs and availability of the materials.
Conclusion
This AOGO guideline is the first to provide recommendations for the use of osteobiologics in ACDF. Despite the comprehensive searches for evidence, there were few studies completed with small sample sizes and primarily as case series with inherent risks of bias. Therefore, high-quality clinical evidence is demanded to improve the guideline.
Keywords
Introduction
Osteobiologics are widely used in spinal surgeries, over a variety of indications including degenerative pathologies, deformities, trauma, and tumour.1,2 However, the clinical use of osteobiologics in spinal surgery is not very well defined and user guided. Several factors are responsible for the current situation regarding osteobiologics. Firstly, there is a lack of high-quality clinical evidence for the use of biologics, which provides limited information to foster the knowledge and to guide the use of biologics. Secondly, regulations about the use of biologics vary highly across countries. The regulatory inconsistency further hinders the investigation of osteobiologics, especially their safety and efficacy. The fact is, in most cases, the choice of a specific osteobiologic is dictated by surgeon’s interest (familiarity, education and consulting) and/or hospital-approved inventory.
In the last couple of decades, there was an explosion of osteobiologics that aim to replace or enhance autograft use. A large number of studies focusing on lumbar and cervical degenerative cases have looked at the applicability of various graft materials. Demineralised bone matrix (DBM), synthetics and bone marrow aspirates (BMA) have been shown to have similar fusion rates to autograft or allograft; however, the level of evidence is low or limited depending on the indication.3–6 Human bone morphogenetic protein-2 (BMP-2) has been widely used for various approaches, while several complications have been associated with its use.
Among cervical spine degenerative disease surgical procedures, anterior cervical discectomy and fusion (ACDF) is commonly performed to alleviate symptoms and pain in patients which are unresponsive to conservative therapies. 7 As fusion is considered one of the primary outcomes of ACDF, therefore, the graft choice is critical to achieve satisfactory fusion rate. In an international survey among spine surgeons on graft selection in ACDF, 74% voted for the use of non-structural graft material (allograft, autograft, BMA, DBM, platelet, ceramic and BMP2) for single-level and 72.8% use it for multi-level cases. Most used osteobiologics included local graft (17%), autograft iliac crest (17%) followed by DBM (13%), allograft cancellous (8%) and ceramic (9%). 8
Due to the paucity of the published clinical data, there is no consensus among spine surgeons regarding the osteobiologics to be used at single- or multi-level ACDF in a specific clinical scenario.
There is a need to develop an international guideline to provide spine community clarity on how and when to use osteobiologics in ACDF surgery.
Materials and Methods
The overall process of guideline development was guided by the AO policies and the Guideline International Network (GIN)-McMaster Guideline Development Checklist (http://cebgrade.mcmaster.ca/guidecheck). Detailed methods are published in a separate paper. The guideline group consisted of 73 people with expertise in degenerative spine diseases and surgery from 22 countries.
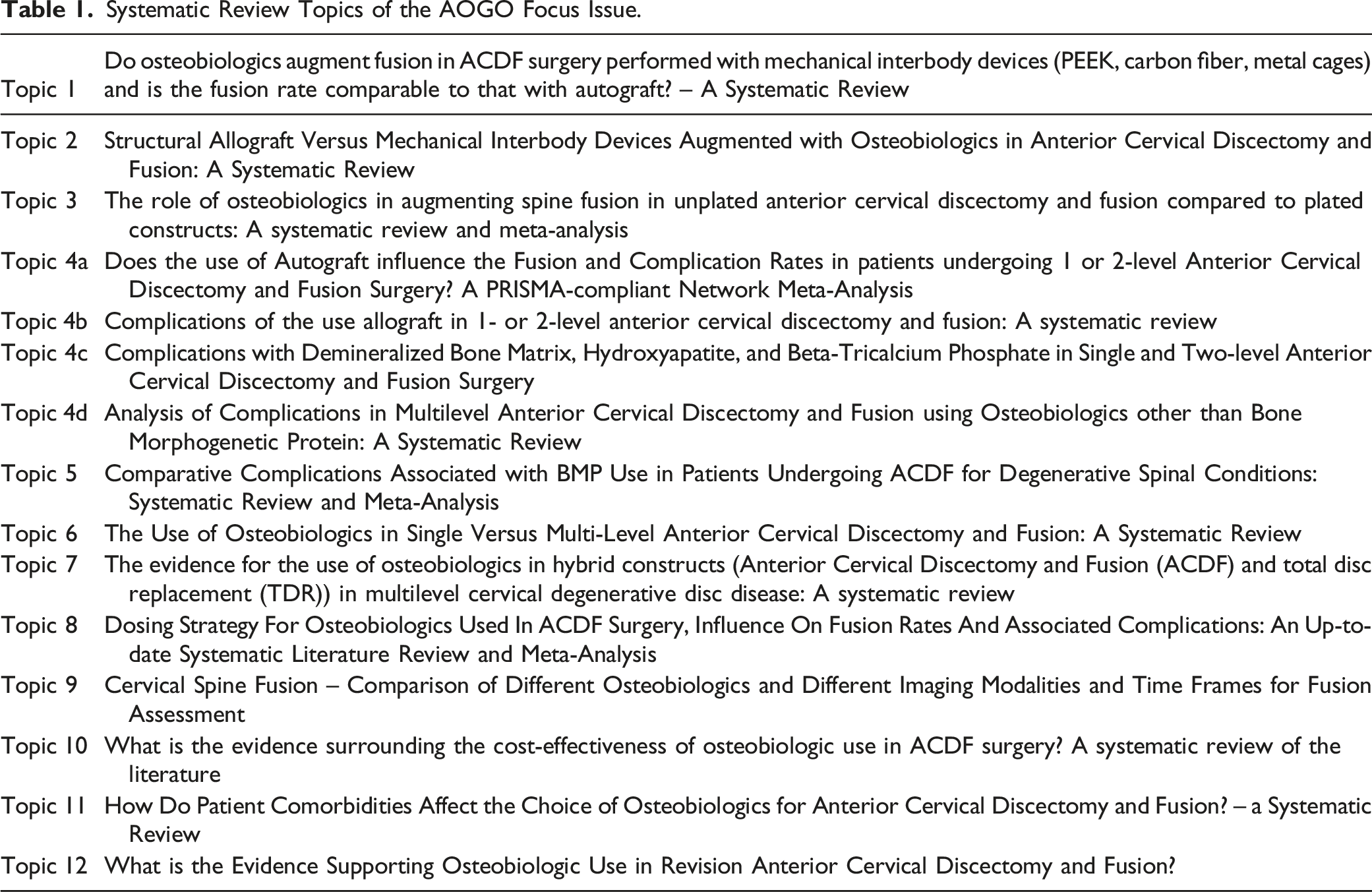
Systematic Review Topics of the AOGO Focus Issue.
Each recommendation is defined as a strong or conditional recommendation according to the GRADE approach (https://gdt.gradepro.org/app/handbook/handbook.html). Strong recommendations were made when desirable consequences clearly outweighed undesirable consequences and conditional recommendations when desirable consequences probably outweighed undesirable consequences. Strong recommendations are worded as ‘we recommend’ and most surgeons should follow the recommended action, and conditional recommendations are ‘we suggest’ and surgeons should likely follow the recommended action but recognise that different choices will be appropriate for each individual.
Recommendations
Autograft Versus Cage With Osteobiologic
Conditional recommendation based on low certainty evidence.
In primary ACDF surgery for degenerative conditions, we suggest that either structural iliac crest autograft or a cage with an osteobiologic (such as tricalcium phosphate, demineralised bone matrix, hydroxyapatite or allograft) can be used with similar outcomes.
Remarks
This recommendation applies to the use of different cages such as PEEK or titanium but does not address the use of morselised autograft (bone dust) in a cage. The choice of iliac crest autograft or cage plus osteobiologic may be dependent on availability, current costs and resources, which may vary with the institution and clinical situation (such as in patients with comorbidities). However, there is little to guide the use of autograft, cage or osteobiologic based on comorbidities. It is important to discuss donor site morbidity with patients when using autograft.
Summary of the Evidence
We conducted a systematic review of studies published up to October 2020 comparing the use of autografts to the use of mechanical interbody devices augmented with osteobiologics (Table 1, Topic 1). There were 2 randomised controlled trials (both using a titanium device with either human cancellous allograft or hydroxyapatite coating) and 6 non-randomised studies (most using a PEEK device but also titanium with tricalcium phosphate).9–16: DBM was not assessed in the studies. Across all studies, there were little to no differences in fusion (from 12 to 0% in favour of autograft). The incidence of reoperations was also similar between autograft and osteobiologics across all studies (difference of 3–4%). Pain was measured in 3 studies10,13,14 and function in 4 studies,9,13–15 all showed little to no differences between autograft and osteobiologics. Neurological, soft tissue and surgical complications were reported together in most trials. From the RCTs (n = 375), there was no difference in complications.10,13 However the non-randomised studies (n = 392) found slightly more complications with autograft (8.9% vs 4.4%); these studies were at higher risk of bias.9,11,12,14–16 When using autograft, donor site morbidity may occur. In RCTs, the incidence was 8% (14/172), but it was 22% (24/107) in non-randomised studies.10–16 A systematic review was also conducted for cost-effectiveness (Table 1, Topic 10) and found that costs were variable across studies and appeared to be locally dependent. There was no data to inform the use of different osteobiologics in patients with different comorbidities. Overall, evidence suggests that the benefits and harms are similar when using autograft or a device plus osteobiologic, with the exception of donor site morbidity with autograft (low certainty evidence).
Allograft Versus Cage With Osteobiologic
Conditional recommendation based on very low certainty evidence.
In primary ACDF surgery for degenerative conditions, we suggest either allograft or a cage with an osteobiologic depending on factors such as availability, costs and resources.
Remarks
Because of the lack of evidence for differences in benefits, other factors will play a greater role in choice of allograft or cage. Factors may vary based on availability of allograft, with the institution and clinical situation (such as in patients with comorbidities). However, there is little to guide the use of allograft, cage or osteobiologic based on comorbidities.
Summary of Evidence
We conducted 3 systematic reviews of studies published up to October 2020: 1 included study comparing the use of allografts to the use of mechanical interbody devices augmented with osteobiologics (Table 1, Topic 2); the other review included studies assessing effects of allograft only (Table 1, Topic 4b); and, the other review included studies assessing complications of mechanical interbody devices augmented with osteobiologics only (Table 1, Topic 4c). Three studies compared allograft to ceramic glass or DBM;17–19 2 (n = 110) were at lower risk of bias and found trivial differences in fusion (0–14% at 1 year and 3% at 2 years).17,18 In these 2 comparative studies, fusion occurred in 73% and 100% with osteobiologics, which was similar to the range (68.5–100%) reported when using allograft in 14 non-comparative studies (n = 1455). One study (n = 71) measured pain (VAS, 0–10, worse), pain was reduced by 2 points with allograft and 1.2 points with osteobiologic. 18 Complications were inconsistent across the comparative studies. However, across 18 non-comparative studies, complications occurred in similar numbers for dysphagia/dysphonia (.4–22%), wound-related complications (0–7%), new neurologic deficit (0–1.9%) and post-operative radiculopathy (0–2%) (Table 1, Topic 4b and Topic 4c). Overall, evidence suggests that the benefits (such as fusion) and harms (such as complications) are similar when using allograft or a cage with osteobiologic, but this evidence is of very low certainty. The costs were variable across studies and appear to be locally dependent, but costs for cell-based allografts may be relatively higher in most institutions (Table 1, Topic 10). There was no data to inform the use of different osteobiologics in patients with different comorbidities.
Use of BMP-2
Conditional recommendation based on very low certainty evidence.
When using a cage with osteobiologic in ACDF surgery, we suggest osteobiologics other than BMP in common clinical situations.
Remarks
There may be clinical situations where BMP-2 may be a reasonable choice. However, given the potential increase in harms, close monitoring for anterior soft tissue complications (such as dysphagia) is warranted when used.
Summary of Evidence
A systematic review was conducted and included 12 non-comparative studies assessing the use of BMP and 9 studies comparing BMP to autograft, allograft or other osteobiologics in ACDF surgery (Table 1, Topic 5). Studies of large retrospective databases where biases in the reporting of outcomes may occur were not included in the development of the recommendation. There may be no difference in fusion with BMP at doses > or <.75 mg/level or with autograft, allograft or other osteobiologics (∼98% and ∼87%, respectively). However, there may be slightly more complications with BMP-2, such as dysphagia/dysphonia and other soft tissue complications regardless of dose (26% vs 21% and 27% vs 20%, respectively). Other complications may be similar or slightly lower with BMP-2, including medical, neurological and failure-related complications. The effect of dosage of BMP-2 was inconsistent across complications. Overall, few studies exist that assess the effects of BMP-2 in ACDF surgery resulting in very low certainty evidence. Although the use of BMP-2 is feasible, BMP-2 is relatively more expensive than other osteobiologics, and these costs may not outweigh any perceived benefits in common clinical situations.
Single- or Multi-Level Surgery
Conditional recommendation based on low certainty evidence in effects
We suggest that an osteobiologic can be used in single- or multi-level primary ACDF surgery for degenerative conditions.
Remarks
Surgeons may decide to use osteobiologics in single- or multi-level fusion based on clinical situation. The choice of osteobiologic may be dependent on factors such as availability, institution and clinical situation.
Summary of Evidence
We conducted a systematic review and found 8 studies18,20–26 comparing the use of osteobiologics and autograft or allograft in single- vs multi-level ACDF, and there was however very limited data for ≥ 3 levels (Table 1, Topic 6). Studies reported no differences in fusion or in patient-reported outcomes, such as pain or function. Information about complications comes primarily from studies that are non-comparative. In a systematic review of studies assessing allograft and studies assessing osteobiologics, complications were similar: dysphagia/dysphonia occurred in ACDF with single- or two-levels in 0–14% with allograft vs 1–22% with osteobiologic; wound-related complications in 0–2% (5 studies, n = 696) with allograft and 23% (43/188) in another study vs 0–7% (8 studies, n = 647) (Table 1, Topic 4b and Topic 4c). Other complications were typically <3% with allograft or osteobiologic at single- or two-levels. There were also very few to no complications with osteobiologics in 3-level ADCF in 3 studies (n = 96).27–29 In other studies reporting the use of osteobiologics in multi-level surgery the graft material used was heterogeneous – a mix of autograft, allograft and/or osteobiologic and complications could not be synthesised.30–33 Overall, there is low certainty evidence that the benefits (such as fusion) and complications are similar in single- or multi-level ACDF surgery when using osteobiologics. The costs are variable across studies and appear to be locally dependent.
ACDF–TDR Hybrid Construct Surgery
Conditional recommendation based on very low certainty evidence.
In ACDF–TDR hybrid construct surgery for degenerative conditions, we suggest for the fusion level using either structural iliac crest autograft or allograft or a cage with osteobiologic (such as DBM, bovine bone or BMP-2) to achieve similar outcomes.
Remarks
The choice of iliac crest autograft or allograft or osteobiologics may be dependent on availability, current costs and resources which may vary with the institution and clinical situation (such as in patients with comorbidities). However, there is little to guide their use based on comorbidities.
Summary of Evidence
A systematic review was conducted by Hoelen et al to compare the effects of using an osteobiologic vs none (or autograft or allograft) in hybrid surgery (Table 1, Topic 7). They searched for studies published between 2000 and 2021 and found 7 studies.34–40 No study directly compared hybrid surgery using an osteobiologic compared to allograft or autograft but instead compared hybrid surgery to ACDF or TDR alone. Most of the studies (5/7) were conducted in Asia: 3 in China37,39,40 and 1 in South Korea reported in 2 publications.36,38 One study was conducted in Italy 34 and another in the USA. 35 Fusion (n = 99) was 88% (with BMP) and 100% (with bovine bone) vs 100% with allogenic bone. Range of motion (C2–C7) was reduced by 6.8° and 11.1° with osteobiologics vs reduced by2.7° and increased by 1.28° with iliac and allogenic bone. There were similar reductions in neck and arm pain (range from 3.4 to 6.5) and in the Neck Disability Index (range 18% to 47%) with osteobiologic vs iliac or allogenic bone. Few studies reported complications, but when reported proportions were similar with the use of osteobiologics or not in hybrid construct surgery. Costs are variable across studies and appear to be locally dependent. Overall, benefits (such as fusion) may be similar when using an osteobiologic or autograft or allograft in hybrid construct surgery, and evidence does not suggest that there are greater complications when using osteobiologics. However, the evidence is very uncertain.
Revision Surgery
No recommendation was made for the use of osteobiologics in revision surgery because evidence was not identified.
Conclusions and Usage
Despite the comprehensive review of evidence, there were often few studies with small sample sizes and primarily non-randomised studies and case series with inherent risks of bias, and therefore, the certainty of the evidence for the benefits and harms, and the costs was low or very low. Additionally, no information on comorbidities or risk factors was available. Although our certainty in the evidence will likely increase over time with new studies, at present, we do have some evidence that harms are not increased with the use of osteobiologics in common clinical situations. For this reason, the guideline group suggested the use of autograft, allograft, or cage with an osteobiologic. This means that surgeons can choose to use 1 graft over another or 1 osteobiologic over another primarily based on clinical situation, and the costs and availability of the materials. In such cases, surgeons will need to be informed of their local situation when making decisions.
The development of this guideline also has implications for future research with well-controlled study groups and defined outcomes. As the evidence on osteobiologics grows, the AOGO will update this guideline to reflect new advancements and evidence. KF Degenerative is leading a separate effort on a global prospective clinical study and collecting the evidence on the use and effects of osteobiologic in ACDF and other spine surgeries.
Supplemental Material
Supplemental material - AO Spine Guideline for the Use of Osteobiologics (AOGO) in Anterior Cervical Discectomy and Fusion for Spinal Degenerative Cases
Supplemental material for AO Spine Guideline for the Use of Osteobiologics (AOGO) in Anterior Cervical Discectomy and Fusion for Spinal Degenerative Cases by Hans-Jörg Meisel, Amit Jain, Yabin Wu, Christopher T. Martin, Juan Pablo Cabrera, Sathish Muthu, Waeel O. Hamouda, Ricardo Rodrigues-Pinto, Jacobus J Arts, Arun-Kumar Viswanadha, Gianluca Vadalà, Pieter-Paul A. Vergroesen, Stipe Ćorluka, Patrick C. Hsieh, Andreas K. Demetriades, Kota Watanabe, John H. Shin, K Daniel Riew, Luca Papavero, Gabriel Liu, Zhuojing Luo, Sashin Ahuja, Tamás Fekete, Atiq Uz Zaman, Mohammad El-Sharkawi, Daisuke Sakai, Samuel K. Cho, Jeffrey Wang, Tim Yoon, Nancy Santesso, and Zorica Buser in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.