
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Describe the rate and risk factors for venous thromboembolic events (VTEs; defined as deep venous thrombosis [DVT] and/or pulmonary embolism [PE]) in adult spinal deformity (ASD) surgery.
Methods:
ASD patients with VTE were identified in a prospective, multicenter database. Complications, revision, and mortality rate were examined. Patient demographics, operative details, and radiographic and clinical outcomes were compared with a non-VTE group. Multivariate binary regression model was used to identify predictors of VTE.
Results:
A total of 737 patients were identified, 32 (4.3%) had VTE (DVT = 14; PE = 18). At baseline, VTE patients were less likely to be employed in jobs requiring physical labor (59.4% vs 79.7%, P < .01) and more likely to have osteoporosis (29% vs 15.1%, P = .037) and liver disease (6.5% vs 1.4%, P = .027). Patients with VTE had a larger preoperative sagittal vertical axis (SVA; 93 mm vs 55 mm, P < .01) and underwent larger SVA corrections. VTE was associated with a combined anterior/posterior approach (45% vs 25%, P = .028). VTE patients had a longer hospital stay (10 vs 7 days, P < .05) and higher mortality rate (6.3% vs 0.7%, P < .01). Multivariate analysis demonstrated osteoporosis, lack of physical labor, and increased SVA correction were independent predictors of VTE (r 2 = .11, area under the curve = 0.74, P < .05).
Conclusions:
The incidence of VTE in ASD is 4.3% with a DVT rate of 1.9% and PE rate of 2.4%. Osteoporosis, lack of physical labor, and increased SVA correction were independent predictors of VTE. Patients with VTE had a higher mortality rate compared with non-VTE patients.
Keywords
Introduction
Venous thromboembolic events (VTEs), which include deep vein thrombosis (DVT) and pulmonary embolism (PE), are major and potentially life-threatening complications that have been labelled as “reasonably preventable” if evidence-based guidelines are utilized. 1 In 2009, the Centers for Medicare & Medicaid Services designated VTEs after total knee and total hip replacements a nonreimbursable complication; this mandate was initiated to accelerate improvement in the quality of care and adoption of best practices across the country. 1 Given the attention paid to VTE complications by regulatory agencies and the associated potential for morbidity, it is important for spine surgeons to be aware of the rate of VTEs and the risk factors for this complication.
Recently, several authors have attempted to define the rate of VTE following surgery. Reported rates for VTEs following spine surgery have varied widely, ranging from 0.40% to 22%. 2 –10 There are a number of reasons for this variation. Many of these studies focus on all elective spine procedures 4,5,9 or are drawn from large national- and state-level databases. 2,6,7,11,12 As a result, these studies encapsulate a diverse array of spinal procedures that have a widely varying risk of DVT. Another reason for discrepancy is the definition of VTE: some studies focus exclusively on PE, 8 others on symptomatic VTE, 2,6,11,12 and others on screening ultrasonography. 5 Data on the rates of VTE in an adult spinal deformity (ASD) population, however, remains limited. While some authors have a subset of patients with “long fusions” or “thoracolumbar fusions” in their cohorts, 2,4,10 the definition of these groups is often vague and makes it difficult to infer the rates of VTE in patients with ASD.
The purpose of this study is to report the incidence and risk factors for clinically significant VTE (DVT and/or PE) in patients undergoing surgery for ASD. Identifying those patients at highest risk can be valuable information for prevention and for the judicious use of prophylactic anticoagulation in a patient population where anticoagulation use may not be desirable.
Methods
This study was a retrospective review of a prospectively collected multicenter ASD database maintained by the International Spine Study Group. After institutional review board approval at each site, patients from 11 sites were enrolled into a prospective database of operative and nonoperative ASD patients. Adult patients (age >18 years) were included if one or more of the following radiographic criteria were met: coronal Cobb angle >20°, sagittal vertical axis (SVA) >5 cm, pelvic tilt >25°, or thoracic kyphosis >60°. Exclusion criteria included neuromuscular scoliosis, infection, and malignancy. Only patients from the operative cohort were considered for this study.
Patients were separated into 2 groups: (1) patients with VTE and (2) patients without VTE (non-VTE). VTE was defined as DVT or PE diagnosed during the patients’ postoperative course at any time point. The diagnosis of VTE was recorded after a review of the patients’ hospital course and clinic notes. These reviews were performed at each follow-up interval, that is, at 6 weeks, 1 year, 2 years, and so on. There were no standardized protocols to diagnose VTE and no screening ultrasounds or computed tomography scans performed. Data on the type of VTE prophylaxis provided was not available.
Demographic data collected included age, gender, race, and body mass index (BMI). Data on comorbidities was also recorded along with American Society of Anesthesiologists (ASA) classification and Charlson Comorbidity Index (CCI). Full-length standing spine radiographs were used to assess patients’ deformity, and each radiograph was analyzed and verified by a centralized research team. Operative data collected included estimated blood loss (EBL), operative time, and intraoperative case details (such as osteotomy type, decompressions, anti-fibrinolytic use, etc). Postoperative variables such as length of stay, intensive care unit (ICU) stay, and complication data were also collected for all patients. Follow-up time points were at 6 weeks, 1 year, 2 years, and annually afterward. Reporting of complications included the complication type (eg, neurologic, infectious, etc), the complication time (intraoperative vs postoperative), and complication severity (major vs minor). Major intraoperative complications consisted of cardiac arrest, spinal cord injury, death, nerve root injury, optical deficit, vessel and/or organ injury, blood loss >4 L, pneumothorax, and having an unplanned staged surgery. Major postoperative complications were defined as bowel and/or bladder deficit, death, deep vein thrombosis, deep infection, motor deficit, myocardial infarction, optical deficit, pneumonia, pulmonary embolism, reintubation, sepsis, stroke, acute respiratory distress, pancreatitis, tracheostomy, unplanned return to the operating room, and arrhythmia. Last, Health-related quality of life (HRQOL) data was collected. This included the Oswestry Disability Index (ODI), 36-Item Short-Form Health Survey (SF-36; physical component score [PCS] and mental component score [MCS]), and the Scoliosis Research Society-22r questionnaire (SRS; subdomains: activity, pain, satisfaction, mental, appearance, and total). 13 –15
Statistical Analysis
A Shapiro-Wilk test of normality showed that the distribution of demographic and radiographic variables in the VTE and non-VTE groups was nonnormal (P < .05). As a result, an independent samples Mann-Whitney U test was used to compare continuous variables in the VTE and non-VTE groups. A χ2 test was used to compare categorical variables. Once risk factors were identified, a multivariate binary logistic regression was performed with VTE as the dependent variable. Since this was an exploratory model, all variables with P < .1 were included in the model. Area under the curve (receiver operating characteristic) was used to measure the accuracy and the ability of the predictor to discriminate between patients with or without complications. 16 SPSS Statistics version 23.0 (IBM Corp, Armonk, NY) was used to perform all the analysis. Level of significance was set to P value <.05 for all tests.
Results
Overview
A total of 737 patients with 6-week follow-up were identified in the database. Out of the 737 patients, 450 were more than 2 years from their surgery and were eligible for 2-year follow-up. Of this subset, 369 (82.0%) had data available for analysis. The mean age was of 58.2 ± 14.9 years with 565 (76.7%) females and 172 (23.3%) males. Average BMI was 27.5 ± 6. The rate of VTE in this patient population was 4.3% (n = 32). Of patients with VTE, 14 had a DVT (1.9%) and 18 had a PE (2.4%). Of the 32 cases of VTE, 30/32 (93.8%) were identified postoperatively. Two cases of PE (2/32, 6.2%) were identified intraoperatively. VTE prevalence ranged from 1% to 9.5% among individual centers (P = .128) and 2.0% to 7.9% in individual calendar years (P = .381). Two patients with VTE died during the follow-up period (2/32, 6.3%); the cause of death was not recorded in the database.
Demographic and Radiographic Variables
Our univariate analysis revealed no difference in age between the VTE and non-VTE groups (VTE = 64.2 vs non-VTE = 61, P = .063; Table 1). Similarly, there was no difference between groups in BMI (P = .260), race (P = .820), CCI (P = .274), and ASA (P = .667). Patients with VTE were less likely to be involved in physical labor jobs (odds ratio [OR] = 0.4, 95% confidence interval [CI] = 0.2-0.8, P = .006). When specific comorbidities were compared, patients with VTE were noted to have higher rates of liver disease (OR = 5.0, 95% CI = 1.03-24.2, P = .027) and osteoporosis (OR = 2.3, 95% CI = 1.02-5.1, P = .037; Table 2). There was no difference between groups with regard to rate of smoking (P = .612), cancer (P = .795), and clotting disorders (P = .706), although these conclusions are limited by the relatively low number of smokers and patients with cancers and clotting disorders.
Comparisons of Demographics Between VTE and Non-VTE Groupsa.
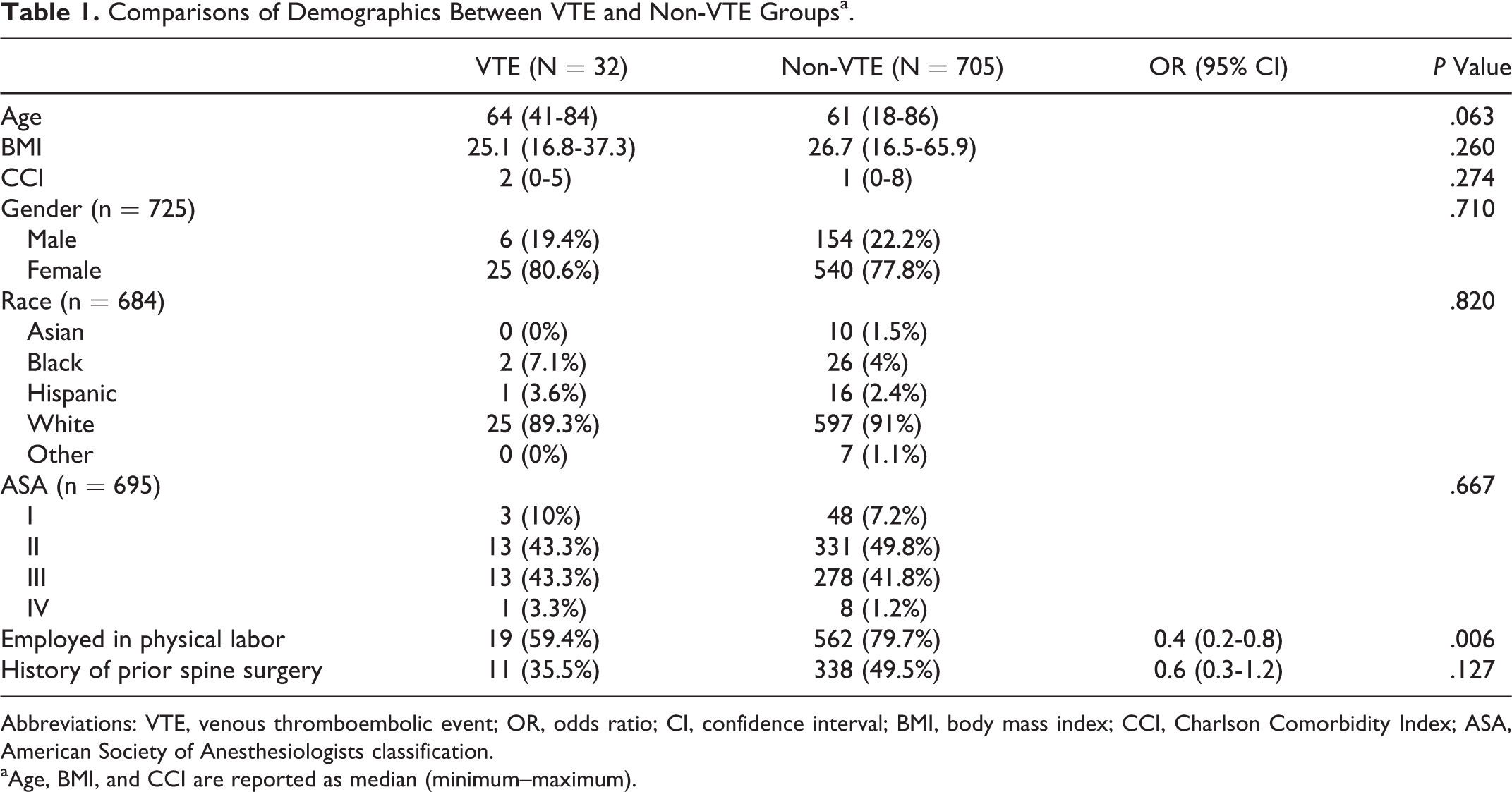
Abbreviations: VTE, venous thromboembolic event; OR, odds ratio; CI, confidence interval; BMI, body mass index; CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists classification.
aAge, BMI, and CCI are reported as median (minimum–maximum).
Comparisons of Percentage of Patients With Specific Comorbidities Between VTE and Non-VTE Groups.
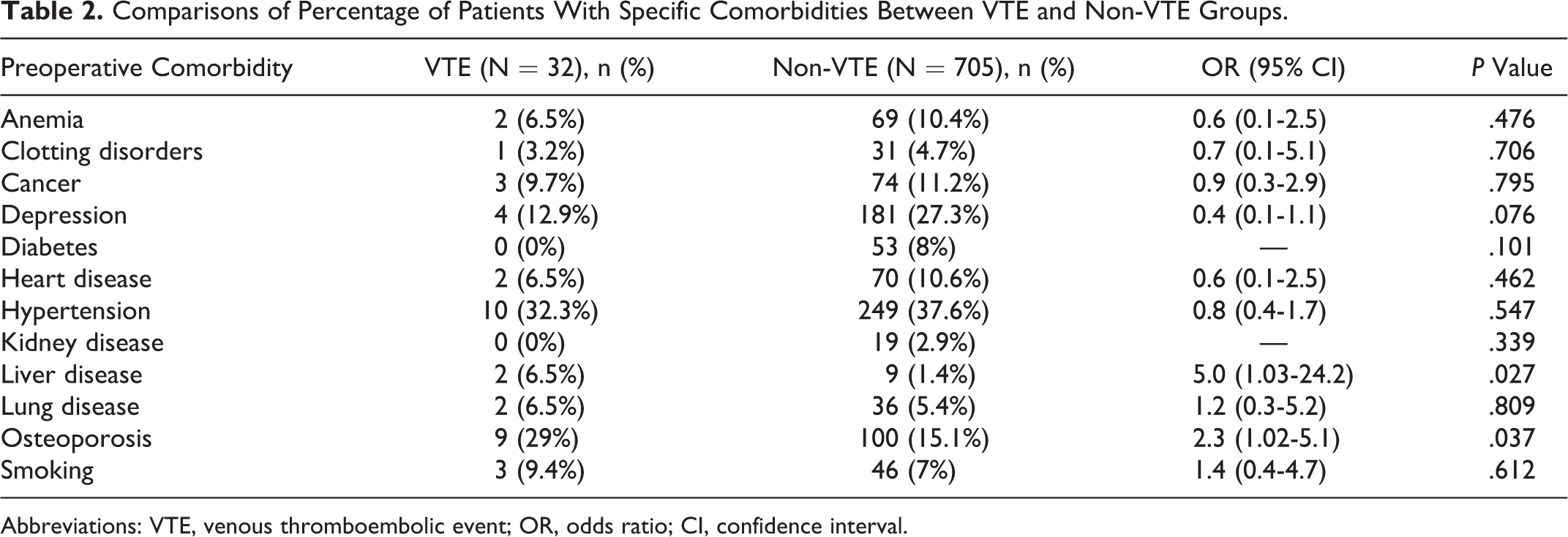
Abbreviations: VTE, venous thromboembolic event; OR, odds ratio; CI, confidence interval.
Patients with VTE had a greater SVA (92.5 mm vs 55 mm, P = .004) and larger upper thoracic (28.0° vs 18.0°, P = .042) and thoracolumbar (39.0° vs 30.0°, P = .031) coronal curves at baseline (Table 3). Patients with VTE had a greater SVA correction at 6 weeks compared with the non-VTE group (72 mm vs 31 mm, P = .004). At 2-year follow-up, there were no significant radiographic differences between the groups.
Radiographic Comparisons Between VTE and Non-VTE Patients at Immediate Postoperative Visita.
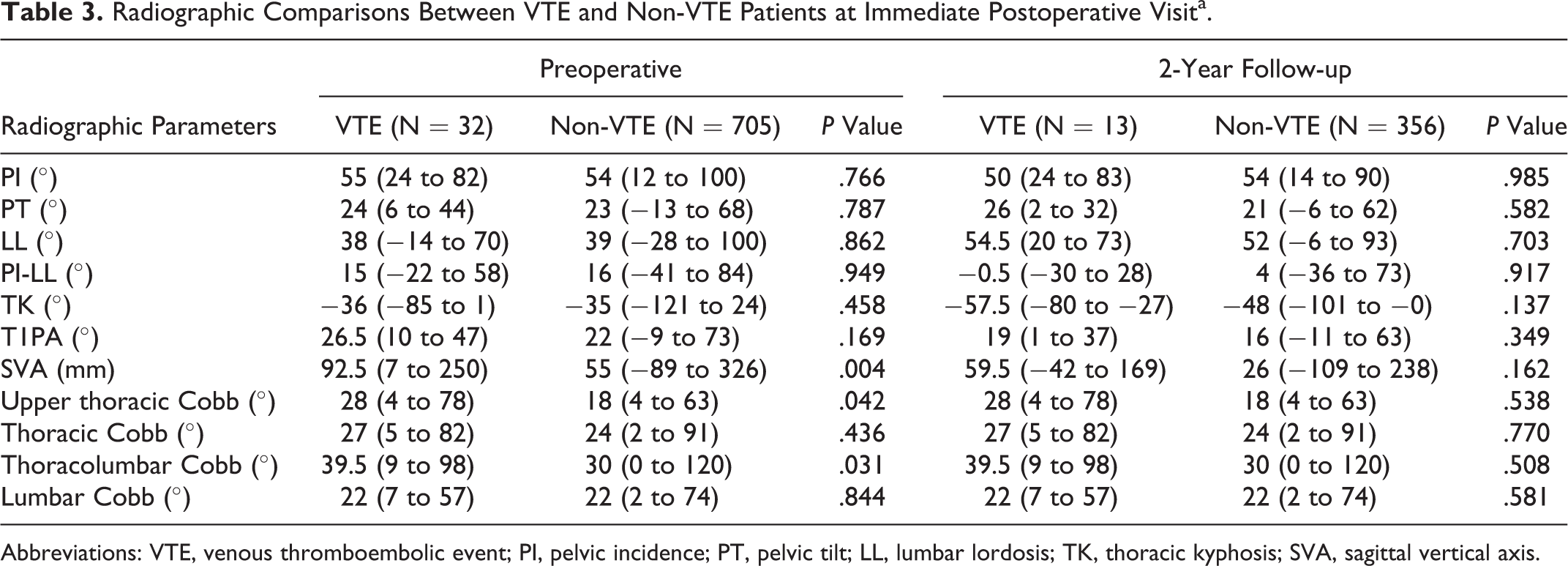
Abbreviations: VTE, venous thromboembolic event; PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis; SVA, sagittal vertical axis.
Intraoperative variables
VTE and non-VTE patients had a similar operating room time (413 vs 369 minutes, P = .306), EBL (1900 vs 1300 mL, P = .271), number of levels fused (14.1 vs 14.0, P = .683), and interbody fusion (OR = 2.0, 95% CI = 0.9-4.6, P = .084; Table 4). Three-column osteotomies did not increase the risk of VTE (OR = 0.9, 95% CI = 0.3-2.3, P = .760 for PSO, and OR = 1.3, 95% CI = 0.3-5.7, P = .714 for VCR). Patients with a VTE were more likely to have undergone a same-day combined (anterior-posterior) surgical approach (OR = 2.4, 95% CI = 1.1-4.9, P = .018) but not a staged anterior-posterior procedure (OR = 1.8, 95% CI = 0.8-4.0, P = .173). Anti-fibrinolytic drugs (including aminocaproic acid and tranexamic acid) were used at similar rates in both groups (OR = 0.7, 95% CI = 0.3-1.3, P = .245).
Comparison of Surgical Parameters Between VTE and Non-VTE Groupsa.
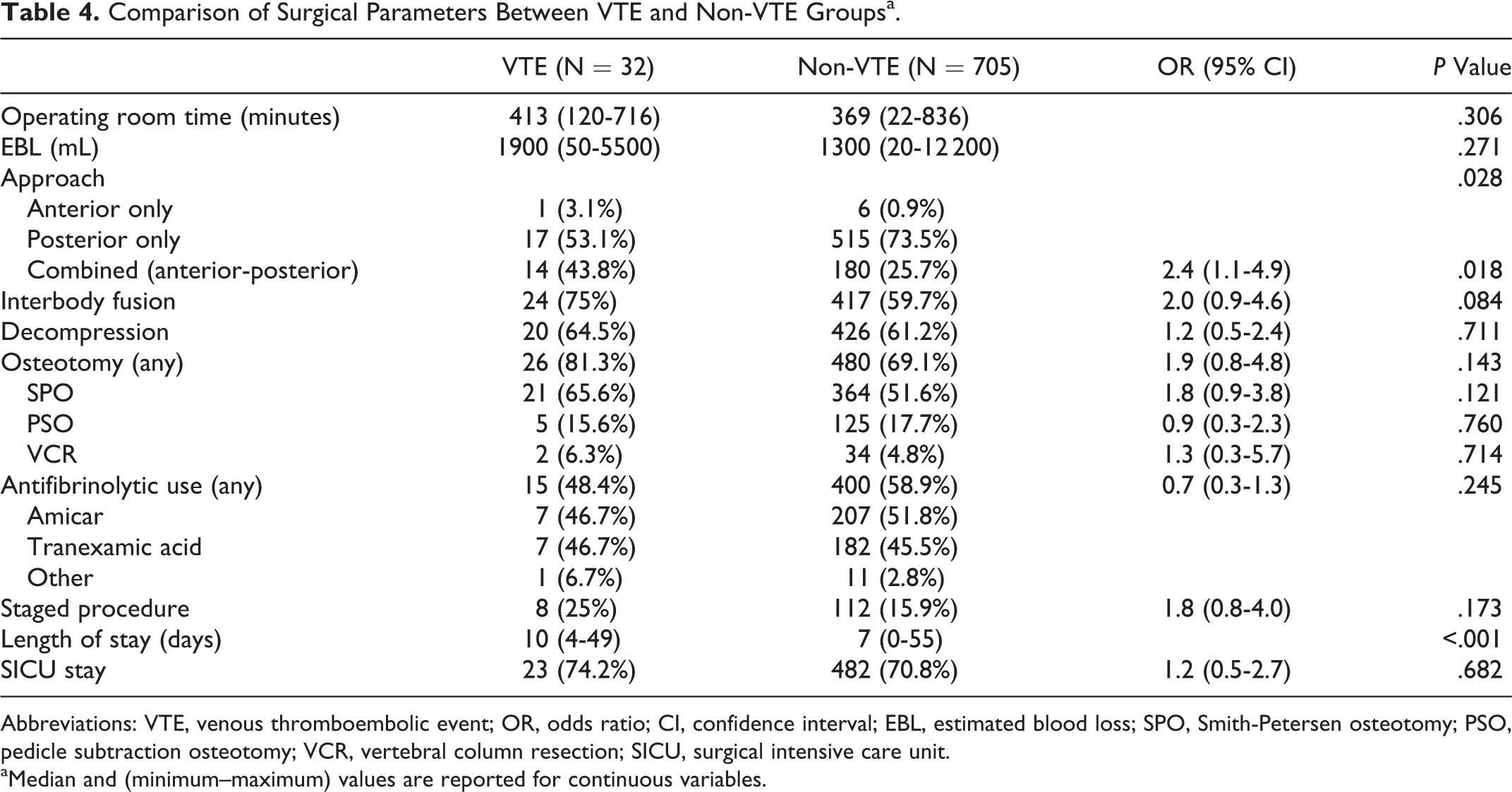
Abbreviations: VTE, venous thromboembolic event; OR, odds ratio; CI, confidence interval; EBL, estimated blood loss; SPO, Smith-Petersen osteotomy; PSO, pedicle subtraction osteotomy; VCR, vertebral column resection; SICU, surgical intensive care unit.
aMedian and (minimum–maximum) values are reported for continuous variables.
Complications
VTE patients had a higher rate of intra- and perioperative complications compared with the non-VTE group. However, there was no difference in the rate of postoperative complications between the groups (OR = 1.5, 95% CI = 0.7-3.2, P = .247). VTE patients had a longer length of stay (10 vs 7 days, P < .001; Table 5) and a higher rate of mortality compared with non-VTE patients (OR = 9.3, 95% CI = 1.7-50.1, P = .002). Unfortunately, we were unable to determine the cause of mortality in these cases.
Comparison of Complications Between the VTE and Non-VTE Groupsa.
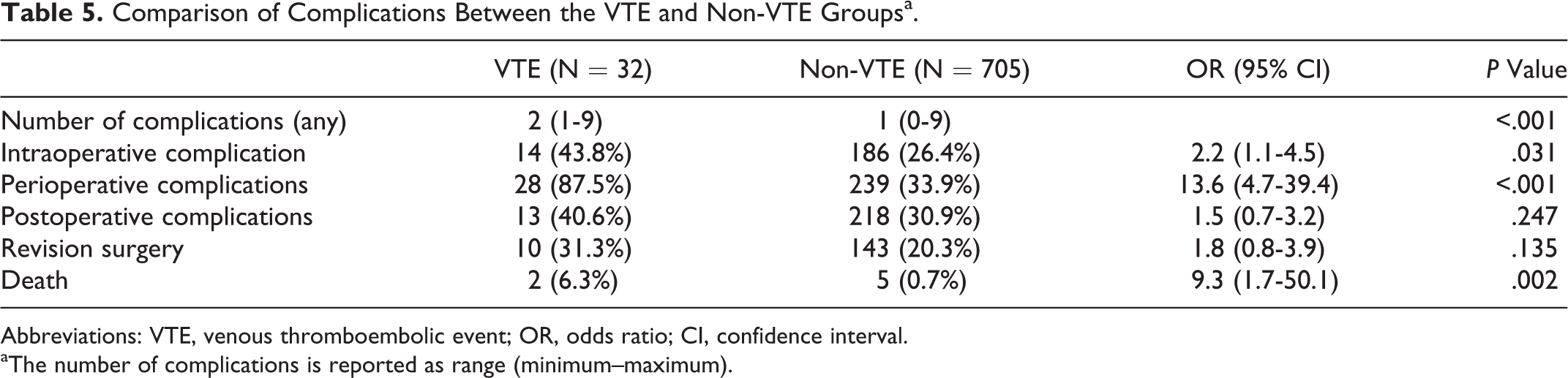
Abbreviations: VTE, venous thromboembolic event; OR, odds ratio; CI, confidence interval.
aThe number of complications is reported as range (minimum–maximum).
HRQOL Scores
Patients with VTE were more likely to have a lower SF-36 PCS score at baseline (27 vs 31, P = .011; Table 6). However, there were no other differences in HRQOL scores at baseline and at final follow-up, and there were no differences in HRQOL scores between groups.
Baseline HRQOL and 2-Year Outcomes for the VTE and Non-VTE Groups.
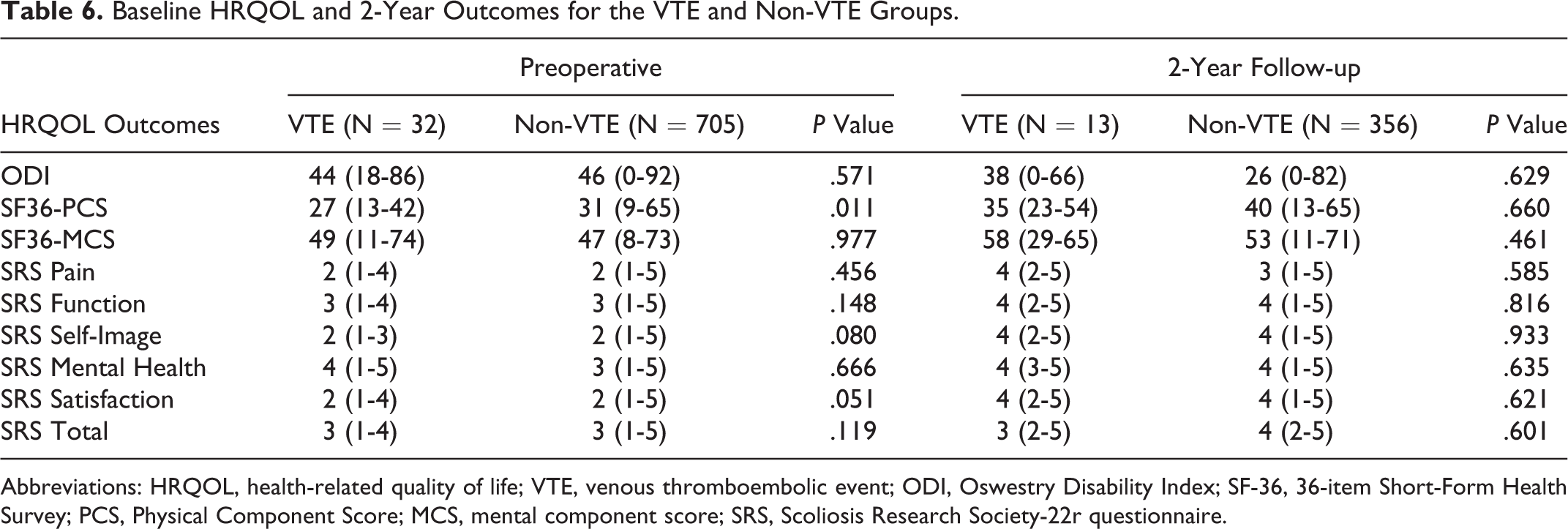
Abbreviations: HRQOL, health-related quality of life; VTE, venous thromboembolic event; ODI, Oswestry Disability Index; SF-36, 36-item Short-Form Health Survey; PCS, Physical Component Score; MCS, mental component score; SRS, Scoliosis Research Society-22r questionnaire.
Independent Predictors of VTE
Our regression model adjusted for all variables with P < .1, namely, age, history of physical labor, depression, liver diseases, osteoporosis, preoperative SVA, and SVA correction. All 737 patients were included. Increased SVA correction (OR = 1.007 per mm of correction, 95% CI = 1.001-1.013, P = .015), osteoporosis (OR = 2.68, 95% CI = 1.07-6.7, P = .035), and lack of physical labor at baseline (OR = 3.0, 95% CI = 1.2-7.3, P = .002) all increased the risk of VTE. For this model, the r 2 was .113, and the area under the curve was 0.740 with P = .050.
Discussion
In this review of a multicenter database, we report a 4.3% rate of clinically significant VTEs among all patients undergoing surgery for ASD. The rate of DVT was 1.9%, while the rate for PE was 2.4%. Our multivariate model found that increased SVA correction, a diagnosis of osteoporosis, and a lack of physical labor at baseline were independent predictors of an increased VTE risk. We also found that patients with VTE were more likely to have a longer length of stay in the hospital (10 days vs 7 days) and had a higher mortality rate (6.3% vs 0.7%). While we do not know the cause of mortality in all these cases, these findings may be of value to deformity surgeons when discussing the risks and benefits of surgery and, in particular, discussing the risk of complications with patients.
Our reported rate of VTE is higher than the overall rates reported by other series of spine surgery patients. 2,4,9 This higher rate of VTE in our cohort is not surprising as the procedures performed in this cohort are technically demanding, requiring long operative times (average operative time time was >6 hours) with lengthy hospital stays (average hospital stay was >7 days). Indeed, the overall rate of VTE in this study might be understated because up to 40% of VTE cases are diagnosed at hospitals that are different from the institution where a patient’s surgery was performed. 2 In addition, not all patients are routinely screened for VTEs and our incidence represents those patients who were symptomatic and subsequently worked-up for VTEs. This fact may introduce a reporting bias and may explain why our reported rate of DVT (1.9%) was lower than our reported rate for PE (2.4%). The screening process can also falsely report the incidence of DVT relative to PE since routine computed tomography to rule out PE does not always include a run through the lower extremities to rule out DVT. The relevance of this is uncertain, since lower extremity DVTs have not been shown to embolize proximally to become a PE, while more proximal DVTs in the proximal thigh and pelvis have been associated with PEs. 17,18
In our univariate analysis of operative variables, only one (anterior-posterior approach) was associated with an increased risk for VTE. This finding has been previously identified in the literature. 2,9,18 We showed that the use of anti-fibrinolytic agents did not increase the risk of VTE in our cohort. The use of these agents has been shown to decrease blood loss in several areas of orthopedics, and our data suggests that they may be used safely in carefully selected ASD patients as long as relevant comorbidities such as a history of stroke, PE, tumors, and cardiac stenting procedures are considered. Our data also found no increase in the risk of VTE with osteotomies in deformity correction; however, this finding must be interpreted with caution given the relatively low numbers of VTE in patients with 3-column osteotomies and the fact that increased SVA correction was found to be a risk factor for VTE in a multivariate analysis.
A connection between SVA correction and VTE has not previously been reported in the literature; it is impossible to study in large database trials and is likely not routinely measured in cases with degenerative pathology. Unfortunately, the retrospective nature of this study makes it difficult to determine exactly why SVA correction might increase risk of VTE. It is possible that patients with larger deformity corrections are undergoing more significant operative procedures and are slower to mobilize postoperatively. Another possibility is that correction of kyphotic deformities leads to traction along the anterior spinal cord, leading to stretching and epithelial injury of the vena cava, which, in turn, increases the risk of VTE. This finding is of considerable clinical importance. There is data now to suggest that increased SVA correction predisposes to complications such as proximal junctional kyphosis. 19 There is also greater attention being paid to age-based correction targets, with the recognition that larger SVAs might be normal in older patients. 20,21 Our study provides adds to this body of work and suggests that surgeons must be judicious when planning their corrections and must take age, patient function, and the risk of complications into account when doing so.
In addition to operative variables, our analysis identified 2 preoperative variables that were independent predictors of VTE risk: the lack of physical labor at baseline and osteoporosis. These are also unique findings that have not previously been reported in the literature. The finding of osteoporosis, in particular, is of particular interest to deformity surgeons given the older, female-predominant patient population encountered in the field (and reported on in this article). The treatment of osteoporosis with selective estrogen receptor modulators may produce a hypercoagulable state that has been shown to increase the risk of VTE. 22–24 Furthermore, it is possible that osteoporosis is a general marker of frailty and immobility as is the lack of physical labor at baseline. A lack of physical activity might result in compromised venous circulation and increased venous stasis.
Last, our results suggest that VTE may have a significant economic impact. Patients diagnosed with VTE tended to have a longer hospital stay and higher mortality rates than the non-VTE cohort. While we were unable to determine the cause of mortality and are unable to conclude if VTE was the cause of the longer hospital stay, this finding brings attention to the possible need for prophylaxis regimens in those with a prolonged length of stay. A targeted VTE prophylaxis regimen for these patients might be an area for further research.
In addition to the retrospective study design, our conclusions are limited by the fact that VTE remains a relatively rare phenomenon in spine surgery. Even in a series of 737 patients, we only had 32 cases of VTE.
Additionally, the multicenter aspect of this protocol and the staged follow-up makes it difficult to accurately determine the type of VTE prophylaxis administered (pneumatic compression boots, aspirin, etc) and the clinical context in which VTE was diagnosed. It is possible that VTE was diagnosed as an incidental finding in some cases. However, we believe this is unlikely as the tests to diagnose VTE are seldom ordered in our clinical practice unless there is a high level of clinical suspicion. Additionally, we could not determine the timing of VTE following surgery. Despite these limitations, to our knowledge, this is the largest series of deformity patients that can examine questions that pertain to radiographic correction as well as preoperative, intraoperative, and postoperative factors.
In summary, we report the overall rate of VTE of 4.3% in an ASD cohort. We report risk factors for VTE that are highly relevant to deformity surgeons such as SVA correction and osteoporosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted with funding support provided to the International Spine Study Group Foundation (ISSGF) from DePuy Synthes Spine, K2M, NuVasive, Innovasis, Biomet, Orthofix, as well as individual donations.