
Abstract
Study Design
Retrospective cohort study of a prospectively collected single-center database.
Objective
Distal Junctional Kyphosis (DJK) is one of the most common complications in adult cervical deformity (ACD) correction. The utility of radiographic alignment alone in predicting and minimizing DJK occurrence warrants further study. To investigate the impact of post-operative radiographic alignment on development of DJK in ACD patients.
Methods
ACD patients (≥18 yrs) with complete baseline (BL) and two-year (2Y) radiographic data were included. DJF was defined as DJK greater than 15° (Passias et al) or DJK with reop. Multivariable logistic regression (MVA) identified 3-month predictors of DJK. Conditional inference tree (CIT) machine learning analysis determined threshold cutoffs. Radiographic predictors were combined in a model to determine predictive value using area under the curve (AUC) methodology. “Match” refers to ideal age-adjusted alignment.
Results
140 cervical deformity patients met inclusion criteria (61.3 yrs, 67% F, BMI: 29 kg/m2, CCI: 0.96 ± 1.3). Surgically, 51.3% had osteotomies, 47.1% had a posterior approach, 34.5% combined approach, 18.5% anterior approach, with an average 7.6 ± 3.8 levels fused and EBL of 824 mL. Overall, 33 patients (23.6%) developed DJK, and 11 patients (9%) developed DJF. MVA controlling for age, and baseline deformity, followed by CIT found 3M cSVA <3.7 cm (OR: .2, 95% CI:.06-.6), and TK T4-T12 <50 (OR:.17, 95% CI:.05-.5, both P < .05) were significant predictors of a lower likelihood of DJK. Receiver operator curve AUC using age, T1S match, TS-CL match, LL-TK match, cSVA <3.7 cm, and T4-T12 <50 predicted DJK with an AUC of .91 for DJK by 2Y, and .88 for DJF by 2Y.
Conclusion
These findings suggest post-operative radiographic alignment is strongly associated with distal junctional kyphosis. When utilizing age-adjusted realignment in addition to newly developed thresholds, a suggested post-operative cSVA target of 3.7 cm and thoracic kyphosis less than 50, it is possible to substantially reduce the occurrence of distal junctional kyphosis and distal junctional failure.
Introduction
Cervical deformity frequently produces major disability, manifesting through neurological deficits, axial and upper extremity pain.1-5 The differing presentations of cervical deformity make identifying the etiology difficult. Previous research has sought to devise classifications that properly stratify the severity of deformity across novel cervical parameters.6,7 Yet, when compared to the realignment schema in adult spinal deformity surgery, less progress has been made and poor outcomes continue to plague the postoperative course of cervical deformity corrective surgery.6-9
The goals of adult cervical deformity (ACD) corrective surgery are to improve patient outcomes through restoration of ideal alignment and horizontal gaze.3-5 Due to advances in surgical technology and peri-operative management and planning, post-operative cervical deformity patients have experienced substantial clinical improvement. By utilizing post-operative radiographic alignment, age-specific spinopelvic parameters can be applied to designate age-specific realignment thresholds for adult spinal deformity (ASD). These thresholds are critical for more precise pre-operative planning to ensure better patient experiences and clinical results. The age-specific values for spinopelvic sagittal parameters can be measured as PI-LL (mismatch between pelvic incidence and L1-S2 lumbar lordosis), PT (pelvic tilt), SVA (global alignment measured via the sagittal vertical axis), TPA (T1 pelvic angle). 1 More cervical-specific parameters can also be applied to evaluate postoperative changes, such as the C2-C7 coronal Cobb angle, cSVA (cervical sagittal vertical axis), T1 slope, C2 slope, and TS-CL (T1 slope minus cervical lordosis). 2 These parameters can be assessed from baseline and post-operative radiograph analyses to evaluate for the development of Distal Junctional Kyphosis (DJK) or Distal Junctional Failure (DJF), post-cervical deformity correction surgery.
The most common type of deformity in the cervical spine is kyphosis, which can be associated with degenerative, iatrogenic, neuromuscular pathologies, myelopathy and post-laminectomy syndrome. 6 DJK is a primary clinical consequence when correcting for cervical deformity, and can result in failed realignment and revision surgery.6,7 The development of DJK is radiographically defined as a loss of alignment at one or two levels distal to the lowest instrumented vertebra. This is typically due to a fixation failure, adjacent level fracture, or spondylolisthesis, and can progress into a DJF.
We propose that post-operative radiographic alignment can be utilized in the prediction of the development of distal junctional kyphosis, post-cervical deformity correction surgery. Our analysis will be based on the application of age-adjusted realignment measures to develop thresholds for post-operative patients, to better predict the development of DJK and DJF.
Materials and Methods
Study Inclusion Criteria
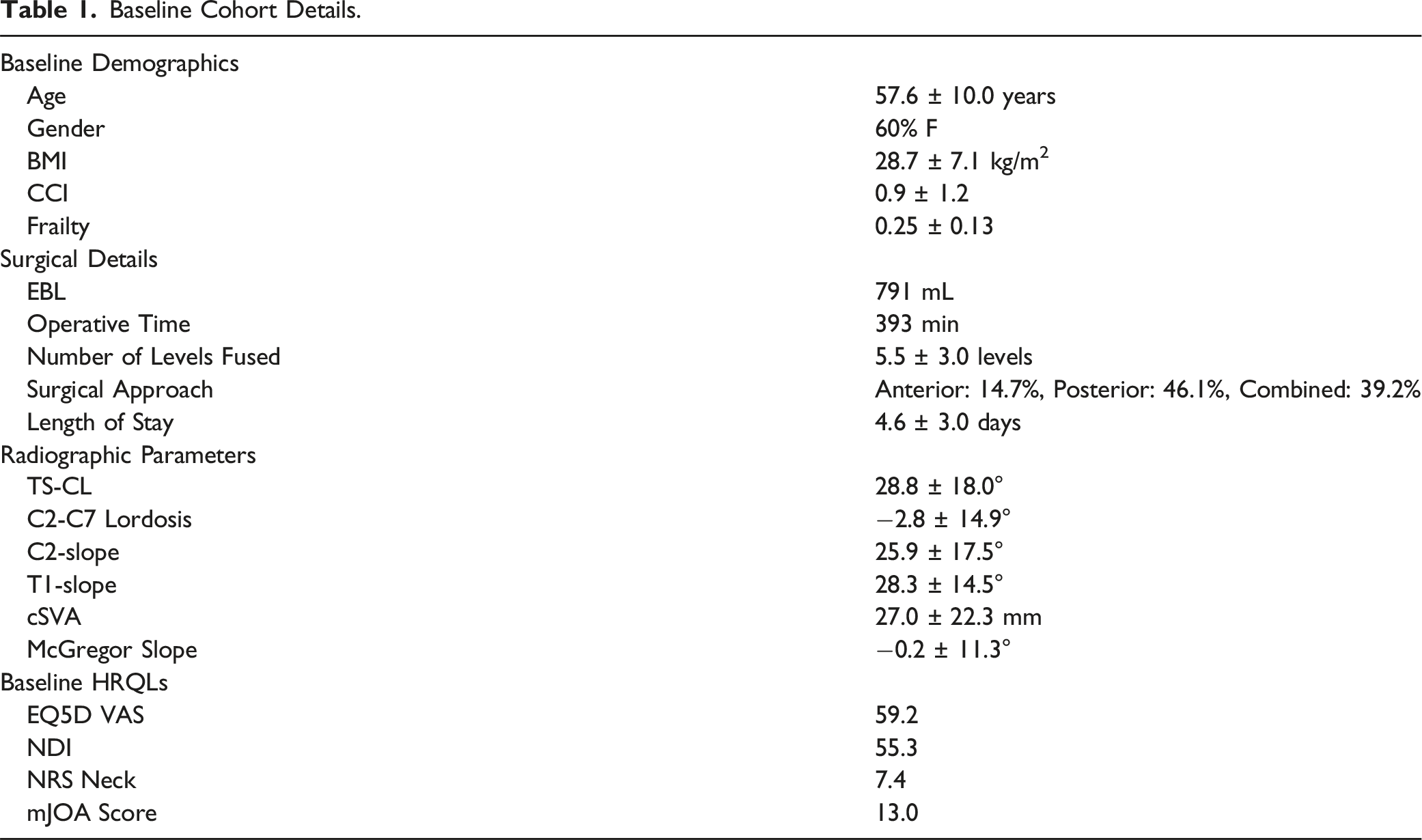
Baseline Cohort Details.
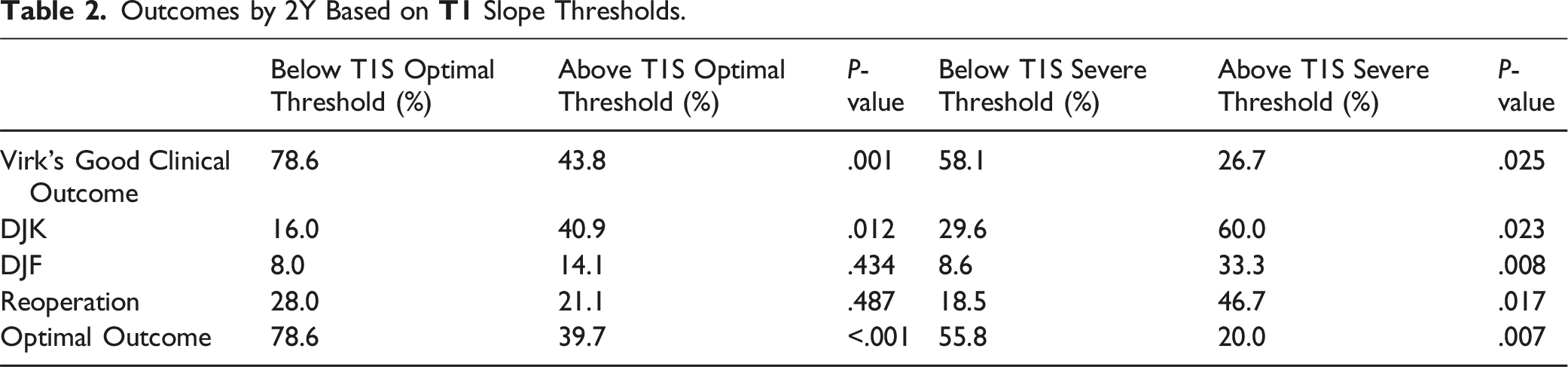
Outcomes by 2Y Based on
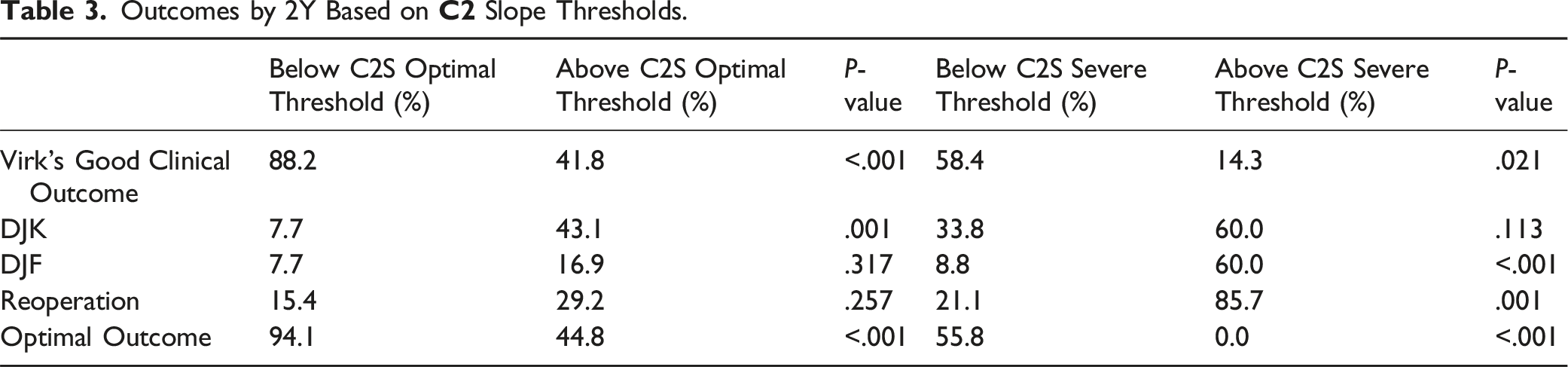
Outcomes by 2Y Based on
Outcomes by 2Y Based on Both Slope Thresholds.

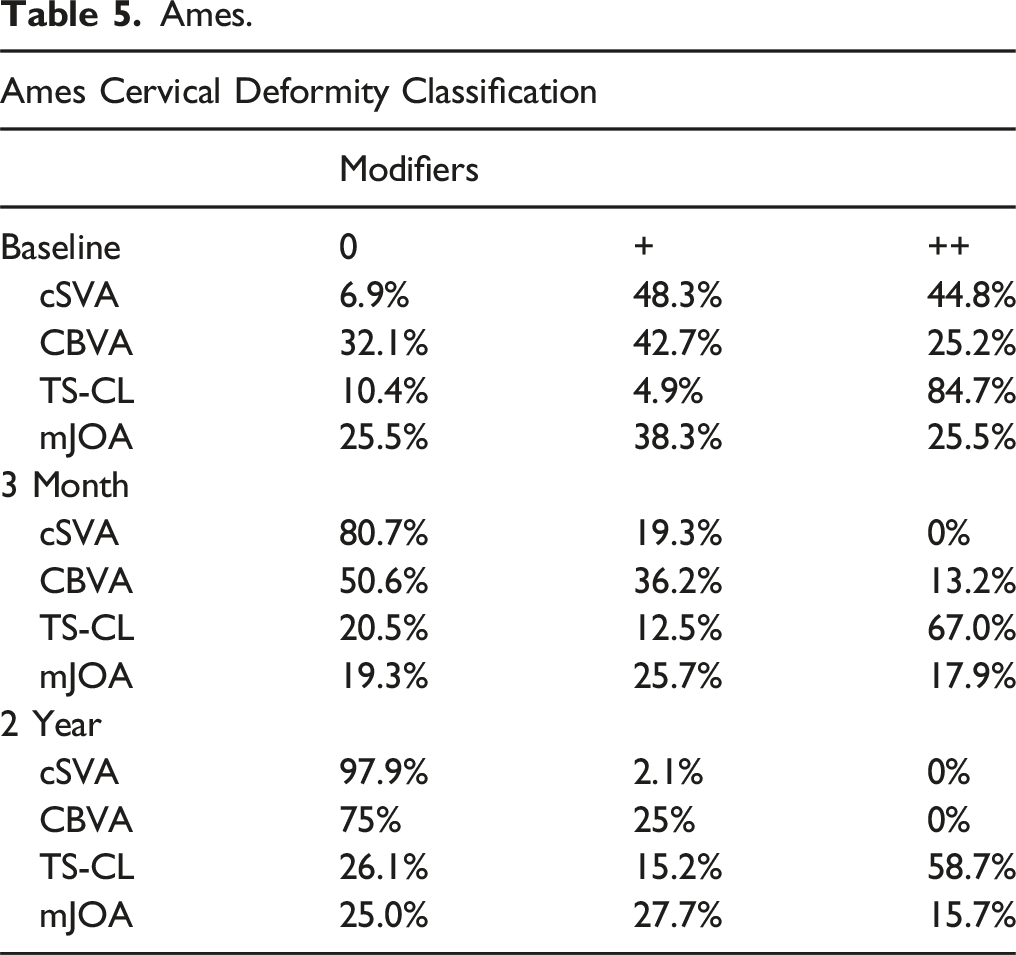
Ames.
Data Collection
Demographic data included age, gender, body mass index (BMI), history of prior cervical fusion, frailty index per the modified cervical deformity frailty index by Passias et al (mCD-FI), and baseline comorbidities incorporated into a score known as the Charlson Comorbidity Index (CCI).12,13 Surgical data collected included number of levels fused, estimated blood loss, operative time, surgical approach, decompression type (discectomy, foraminotomy, corpectomy, laminectomy), and osteotomy type (Smith-Peterson, incomplete/complete facet), as well as perioperative details such as length of stay, admission to the surgical intensive care unit (SICU), and disposition status upon discharge. Complication assessments were made based on review of imaging, patient reports, and clinical follow-up.
Radiographic Assessment
Baseline and up to 2-year postoperative radiographs were measured using validated software programming (SpineView; ENSAM Laboratory of Biomechanics, Paris, France) at a single academic center.14-16 Cervical sagittal alignment and balance were evaluated using C2-7 Cobb angle for cervical lordosis (CL: angle between the lower endplates of C2 and C7), C2 slope, T1 slope (T1S), cervical sagittal vertical axis (cSVA: C2 plumbline offset from the posterosuperior corner of C7), and the mismatch between T1 slope and CL (TS-CL). Global sagittal alignment was assessed via the C7-S1 sagittal vertical axis (SVA), the mismatch between pelvic incidence and lumbar lordosis (PI-LL), pelvic tilt (PT), and thoracic kyphosis (T4-T12; TK).
Alignment classifications were also assessed. Baseline and postoperative alignment at three months and two years post-operatively in age adjusted cervical alignment, the Passias cervical deformity classification, Ames, and overall global using Global Alignment and Proportionality score (GAP).
Assessment of Distal Junctional Kyphosis and Failure
Distal junctional kyphosis, per previous literature, was defined per physician note or radiographically as DJK angle (kyphosis between the superior endplate of the lowest instrumented vertebra [LIV] and the inferior endplate of the second distal vertebra [LIV-2]) >15°, or DJK with reoperation.
Definition of Age-Adjusted Realignment Criteria
For each patient, the age-adjusted alignment targets were calculated based on prior literature values. Age-specific realignment thresholds were generated from radiographic spino-pelvic parameters, patient age, and physical component score (PCS), via linear regression analysis. Formulas for LL-TK, T1S, and TS-CL were generated as follows


Statistical Analysis
Multivariable logistic regression was used to identify 3-month predictors of DJK. Conditional inference tree (CIT) machine learning was used to determine threshold cutoffs. A P-value lower than .05 would be recognized as reaching significance. Radiographic predictors were combined in a model to determine predictive value using area under the curve (AUC) methodology. “Match” refers to ideal age-adjusted alignment. All analyses were performed using SPSS.
Results
Cohort Overview
We included 140 CD patients in the present study. The mean age of the cohort was 61.3 years, 67% were female, mean BMI of 29 kg/m2, and mean CCI of 0.96 ± 1.3. Examination of surgical details revealed a mean levels fused of 7.6 ± 3.8, and average estimated blood loss (EBL) of 824 mL. By surgical approach, 51.3% had osteotomies, 17.9% of the cohort underwent an anterior-only approach, 47.1% a posterior-only, and 35% underwent combined anterior-posterior approach.
Baseline Radiographic Parameters
The mean baseline radiographic parameters were as follows: PT of 17.7 ± 8.9°, PI-LL of −2.0 ± 14.0°, SVA of −9.9 ± 58.9 mm, T2-T12 kyphosis (TK) of −41.5 ± 25.5°, C2-C7 lordosis of −2.8 ± 14.9°, T1-slope (T1S) of 28.3 ± 14.5°, TS-CL of 28.8 ± 18.0°, C2-Slope (C2S) of 25.9 ± 17.5°, cSVA of 27.0 ± 22.3 mm, C2-T3 Cobb angle of −8.3 ± 16.4°, and McGregor’s slope of −0.2 ± 11.3° (Table 1).
Post-Operative Radiographic Parameters
At 3 months postoperatively, the cohort had a mean C2 slope of 22.8 ± 13.9° and a T1-slope (T1S) of 34.7 ± 14.0°. By 2 years postoperatively, both parameters had slightly decreased with a C2 slope of 19.8 ± 9.7° and a T1-slope (T1S) of 30.7 ± 12.6°.
Radiographic Categorization
For Ames classification descriptors at baseline 54% were type C, 27% were type CT, 15% type T, and the lowest group was type S at 3%. Significant improvement in Ames modifiers were seen post-operatively. (Table 5). Age-adjusted analysis depicted under correction was significantly correlated with development of DJK and DJF (P < .05). Passias cervical deformity classification depicted.
Patient Reported Outcomes
Preoperatively NDI was 55, mJOA was 13, NRS neck was 7.4 and EQ5D VAS was 59. This improved postoperatively and was found to be 43.6 for NDI, mJOA was 14, NRS neck improved to 5.0, and EQ5d VAS 72.
Complications
Regarding complications, overall, 54.7% had complications. 28.2% developed DJK, and 11.8% developed DJF, with 23% reoperation and 14.8% failure. Minor complications were seen in 24%, while major were in 25%. Dysphagia was present in 3%, while 17% had neurological complications. The rates of DJK did not differ by surgical approach (anterior 20%, posterior 30.3%, combined 24.5%, P = 0.149)
Multivariable Analysis
Parameters and complication correlates at three months was conducted with multivariable analysis controlling for age, and baseline deformity, followed by CIT found three month cSVA <3.7 cm (OR: .2, 95% CI:.06-.6), and TK T4-T12 <50 (OR:.17, 95% CI:.05-.5, both P < .05) were significant predictors of a lower likelihood of DJK.
Prediction of Three-Month Alignment on Occurrence of DJK and DJF
Receiver operator curve AUC using age, T1S match, TS-CL match, LL-TK match, cSVA <3.7 cm, and T4-T12 <50 predicted DJK with an AUC of .91 for DJK by 2Y, and .88 for DJF by 2Y.
Discussion
Patients suffering from cervical deformity (CD) can undergo corrective surgery as a means to achieve a higher quality of life in both physical presentation, and pain experience. Many encouraging results have been published on the short-term outcomes of CD corrective surgery, but not as much has been evaluated for long-term patient experience and clinical presentation. 1 Although corrective surgery has been shown to have many beneficial clinical outcomes, there are often associated complications, depending on the complexity of the case, which can result in further spinal deformity. 2 Encouraging results have demonstrated that the use of post-operative radiographic analysis can be used to better predict the development of complications, such as DJK and DJF.17-21
Our research proposes the use of age-adjusted realignment thresholds in post-operative CD patients, to better evaluate for the progression of DJK, via established radiographic spinal parameters. This is an important contribution to the understanding of CD-corrective surgery outcomes, because it investigates radiographic age-adjusted thresholds which can better predict the development of DJK post-operatively. In our study 140 patients met the inclusion criteria, with an average age of 60 years, majority being female and overweight. Nearly half (47.1%) of the patients underwent a posterior approach, with a little more than half (51.3%) undergoing a three-column osteotomy and under 1L estimated blood loss during surgery. In terms of mechanical complications, 33 patients (23.6%) developed DJK, 11 patients (9%) developed DJF that required return to OR. A 3-month post-operative analysis, controlling for age and baseline deformity, demonstrated that of the patients who developed DJK and DJF from ACD corrective surgery, showed that a cSVA <3.7 cm (OR: 0.2, 95% CI: 0.06-0.6), TK T4-T12 <50 (OR: 0.17, 95% CI: 0.05-0.5, both P < 0.05) were significant predictors for a lower likelihood of DJK.
We also found that in a receiver operator curve using age, T1S match, TS-CL match, LL-TK match, cSVA <3.7 cm, and T4-T12 <50 predicted DJK with an AUC of 0.91 for DJK by 2Y, and 0.88 for DJF by 2Y. These findings show that there is a strong association between post-operative radiographic alignment and the development of DJK, and these thresholds can be used to help reduce the progression of DJK.
Although there have been many surgical advancements in CD corrective surgery, the reported rates of complications remain high.3-5 This is typically because of variability in surgical treatment, lack of readily defined radiographic intraoperative targets, and individual health issues affecting the patient such as frailty and bone quality. These factors can influence the development of DJK and DJF.6-8 Better understanding of both pre and post-operative factors that predispose patients to the development of DJK can help to prevent such complications and result in better outcomes for patients. A predictive model by Passias et al. was developed that was able to identify with an accuracy of 88% those individuals that were at risk of developing DJK following ACD corrective surgery. 6 However this model did not incorporate post operative radiographic alignment targets. Previous findings have demonstrated that CD patients with severe baseline malalignment were at increased risk of developing DJK irrespective of age-adjusted alignment radiographic alignment targets. 9 Our study, in comparison, utilized descriptive statistical analysis for characterization of the operative population and each cohort, followed by multivariable regression analysis for predictors of DJK. Conditional inference tree analysis was used to derive thresholds for operative radiographic targets. Then, ROC analysis was used to compare the efficacy of these predicted thresholds thereby showing that the radiographic targets established in our study are influenced by age adjusted metrics.
Other work has helped to develop composite alignment scores that are predictive of mechanical failures and the development of DJK, following ACDS based on offsets from age adjusted alignment targets. However, this method was predictive for the development of DJK at the 1 year post-op mark and included less patients than our study. 22
Likewise previous work analyzed various ACD procedures and patient malalignment to predict the incidence of DJK for up to 1 year. 23 Pre-operative C2-T1 tilt, cervical kyphosis, SVA and cervical lordosis were all shown be strong predictors of DJK at specific cut-off points. 23 However, this study did not incorporate age-adjusted alignment thresholds. The formulas in our study were generated from radiographic spino-pelvic parameters, patient age, and physical component score (PCS) via linear regression analysis based on previously published work.
This study has several notable limitations. The retrospective nature of this study could limit the findings and predispose to bias, including confounding by indication. The relatively small sample size might also create potential for restricted clinical variation and truncation in certain areas. The sample size also makes it difficult to ascertain significant findings from more granular analyses relative to the surgical approach. Additionally, ankylosing spondylitis is a notable etiology of ACD which was not present in our dataset. These patients require targeted surgical intervention specific to their needs, and the findings of this study may not be directly generalizable to this cohort of patients. Furthermore, as ACD is a heterogeneous condition, the radiographic parameters used to analyze ACD may lack precision. The statistical approach should also be viewed as exploratory, rather than definitive. There is also limited understanding of the clinical use of radiographic age-adjusted alignment measures as means to compare our findings to. Considering these issues, the findings presented here should be seen as hypothesis generating as opposed to clinically prescriptive. Further external validation in large-scale studies remains to be done before the results presented here can be considered truly clinically actionable.
Conclusions
There is a strong association between postoperative radiographic alignment and the development of DJK. When utilizing age-adjusted realignment in addition to newly developed thresholds, a suggested post-operative cSVA target of less than 3.7 cm and thoracic kyphosis less than 50°, it is possible to substantially reduce the occurrence of distal junctional kyphosis and distal junctional failure. Special attention to age, T1S, T1S-CL, LL-TK matching may also help guide early identification and prevention of DJK/DJF. Application of these thresholds can be used in future cervical deformity corrective surgery patients to better reduce the risk of complications such as DJK or DJF.
Footnotes
Author’s Note
Permission to reproduce Figure 1 and Figure 2 by Ames et al and Passias et al has been received.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.