
Abstract
Study Design
Retrospective case control study.
Objectives
To determine the role of TXA when used as topical soaked sponges (tTXA) on peri-operative blood loss and changes in hemoglobin following posterior spinal fusion (PSF) for neuromuscular and syndromic scoliosis (NMS).
Methods
A single center review of NMS patients who underwent PSF was conducted. The initial set of patients where no tTXA (control) was used were compared to consecutive NMS patients in whom tTXA was used. In the tTXA group, sponges soaked in 1g TXA in 500 mL normal saline were packed in the wound instead of dry sponges. Estimated blood loss (EBL) was calculated intraoperatively using a standard way. Pre-operative, intra-operative and immediate post-operative variables were collected and compared between the 2 groups.
Results
33 patients were included (mean age- 13.5 yrs., BMI- 21, 17 patients in tTXA and 16 patients in control group). Pre-op demographic and radiographic variables were similar between the 2 groups. EBL, EBL per level, EBVL, operative time and number of levels fused were similar in both groups. tTXA group received less intra-operative pRBC transfusion as compared to the control group (150 ± 214 vs 363 ± 186 cc, P = .004). No difference was noted in post-op blood transfusion and drain output for 3 days in both the groups. tTXA group had lesser hospital (5.1 vs 8.9 days) and ICU length of stay (2 vs 4.2 days) and fewer immediate post-operative complications (23.5 vs 52.9%) compared to the control group but not statistically significant (P > .05).
Conclusion
Administration of tTXA-soaked sponges is an effective and safe method to reduce intraoperative blood transfusion requirements in the correction of spinal deformity in patients with NMS.
Introduction
Despite advances in surgical and anesthetic techniques, scoliosis surgery is still associated with significant intraoperative blood loss (IBL). This is especially a special concern in pediatric patients with NMS due to their smaller blood volume, subclinical coagulation function abnormality, antiepileptic medications, osteoporotic bone quality, and vascular smooth muscle dysfunction as seen in certain muscular dystrophies.1-5 In a series of 114 patients with NMS, Jia et al 6 reported 55% with massive IBL, defined as > 30% estimated blood volume loss 6 Factors associated with massive IBL included the number of levels fused >12, BMI <16.8 kg/m2, age >15 years, and surgical time >4.4 hours. Similarly, Brenn et al compared cerebral palsy patients with idiopathic scoliosis patients undergoing PSF and although the clotting parameters were within normal limits there were significant differences at baseline. 7 Once 15% of blood volume loss had occurred in the cerebral palsy patients, the prothrombin time (PTT) and partial thromboplastin time became abnormal. Their findings suggested a functional abnormality of platelet aggregation in cerebral palsy patients. Blood loss can result in changes in physiological fluid shifts, coagulopathy, antibiotic dilution, and the need for transfusions. Allogenic transfusions, although potentially lifesaving, may be associated with infections, hemolytic reactions, and immune modulations, increased hospital stay, and consequently increased cost, especially in the NMS cohort. Therefore, it is important to continue to investigate newer modalities to prevent blood loss.
Numerous blood preservation techniques, including patient positioning, normovolemic hemodilution, intra-operative red-blood cell salvage, use of systemic hemostatic agents (Tranexamic acid (TXA), Aprotinin, desmopressin, recombinant factor VIIa), topical hemostatic agents (thrombin, Collagen-based, cellulose-based, and gelatin-based hemostatic products), and lastly operative techniques including all bovie dissection, frequent wound packing, use of bone wax, gelatin sponges are commonly used during spinal fusion surgery. Many systematic reviews have examined the efficacy and safety of systemic TXA in reducing peri-operative blood loss in both adult and pediatric populations undergoing spinal surgeries.8-10 TXA competitively blocks the lysine-binding site of plasminogen. The plasminogen system is the major proteolytic pathway responsible for the dissolution of blood clots and due to this mechanism of action, there exists a theoretically increased risk of developing venous thromboembolic (VTE) complications including deep venous thrombosis, pulmonary embolism, cerebral thrombosis, and acute renal cortical necrosis.11-13 This has prompted several groups to explore the efficacy of applying TXA topically in the surgical wound to reduce perioperative blood loss.
Topical administration of TXA in the form of an irrigating solution prior to closure and drug-eluting wafers has shown promising results in reducing peri-operative blood loss as shown in recent systematic reviews and meta-analyses.14,15 Our group has previously demonstrated that topical TXA reduces intra‐operative blood loss and transfusion requirements in patients with adolescent idiopathic scoliosis. 16 Given its relatively cheap cost and potential benefits in reducing blood loss and associated costs with surgery, TXA is a promising tool for surgeons to provide more cost-effective care for their patients. The purpose of this study was to determine the role of topical soaked sponges (tTXA) on peri-operative blood loss and changes in hemoglobin following PSF for NMS which has not been explored.
Materials and Methods
Study Design
Following Institutional Review Board approval, we identified 34 consecutive patients with NMS aged ≤18 years who underwent PSF between June 2018 and January 2022. For the purpose of this study, we defined NMS as scoliosis caused due to neuro-muscular and syndromic conditions as described later in the results section. Informed consent was not required as it was a retrospective chart review. Patients in whom blood transfusion was unacceptable due to religious reasons and revision surgeries were excluded. The first 17 patients identified in this study had dry sponges packed in their surgical wound during the surgical procedure. Since November 2019, we started a protocol of using sponges soaked in TXA solution (1 g in 500 mL normal saline) to pack the surgical wounds. Since then, an additional seventeen NMS patients were identified and included in this study. Sponges were packed following exposure, during osteotomies and while placing screws in the non-working field. Standardized perioperative blood conservation techniques were utilized in all 34 patients. This included, hypotensive anesthesia, all bovie dissection, use of gelatin sponges and bone wax, use of cell-saver and use of iv TXA at 50 mg/kg loading and 10 mg/kg/hr. maintenance. Data from one patient from the control group was excluded for post-operative analysis as the patient had a serious post-operative complication and was admitted to the hospital for 69 days due to his medical condition. Out of three fellowship trained spinal deformity surgeons, 2 surgeons were present for all the procedures, one of the surgeons was constant for all the procedures and the second surgeon were alternated by rest of the 2 surgeons . Prior to incision, all patients received a bolus of 50 mg/kg of tranexamic acid, followed by a continuous infusion of 5 mg/kg. Cell saver was used throughout the procedure to capture blood loss. Hemoglobin was measured preoperatively and monitored throughout the intraoperative and postoperative periods.
Data Collection
Patient demographics (age, gender, body mass index, diagnosis, and co-morbidities); radiographic variables (curve type, coronal Cobb angles, apical vertebra translation, pelvic obliquity); surgical variables [number of fusion levels, operative time, estimated blood loss (EBL), estimated blood loss per level (EBL per level), percent estimated blood volume loss (% EBVL), intraoperative packed red blood cell (Intra-op pRBC), fresh frozen plasma (FFP), cell saver, total fluids] and perioperative outcomes [complications, length of stay in ICU, hospital length of stay, intraoperative and postoperative transfusions, postoperative hemoglobin (Hb) days 1-3, and postoperative drain output] were determined. Any thrombo-embolic adverse events were collected up to 30 days post-surgery. EBL was calculated using the blood volume collected in the cell saver and the weight of blood collected on soaked sponges, considering the amount of saline irrigation used. EBV was calculated using the Nadler equation 17 and % EBVL was calculated as EBL/EBV × 100. At our institute, we initiate blood transfusion anytime when the Hb falls < 8 g/dl intra-operatively. All data was collected by 2 dedicated spine research fellows.
Statistical Analysis
Frequency distributions were obtained for demographics and perioperative complications. Control and tTXA groups were compared using Fisher exact tests for categorical variables and independent sample t-tests for continuous variables. Mean values are presented as mean ± standard deviation. P-values of <.05 were considered significant. Mean values are presented as Mean ± SD. All statistics were performed using SPSS software (IBM SPSS statistical package, version 25)
Results
Demographics and Preoperative Radiographic Variables
Demographics and Pre-operative Characteristics of 33 Patients With Neuromuscular Scoliosis Included in Our Cohort.
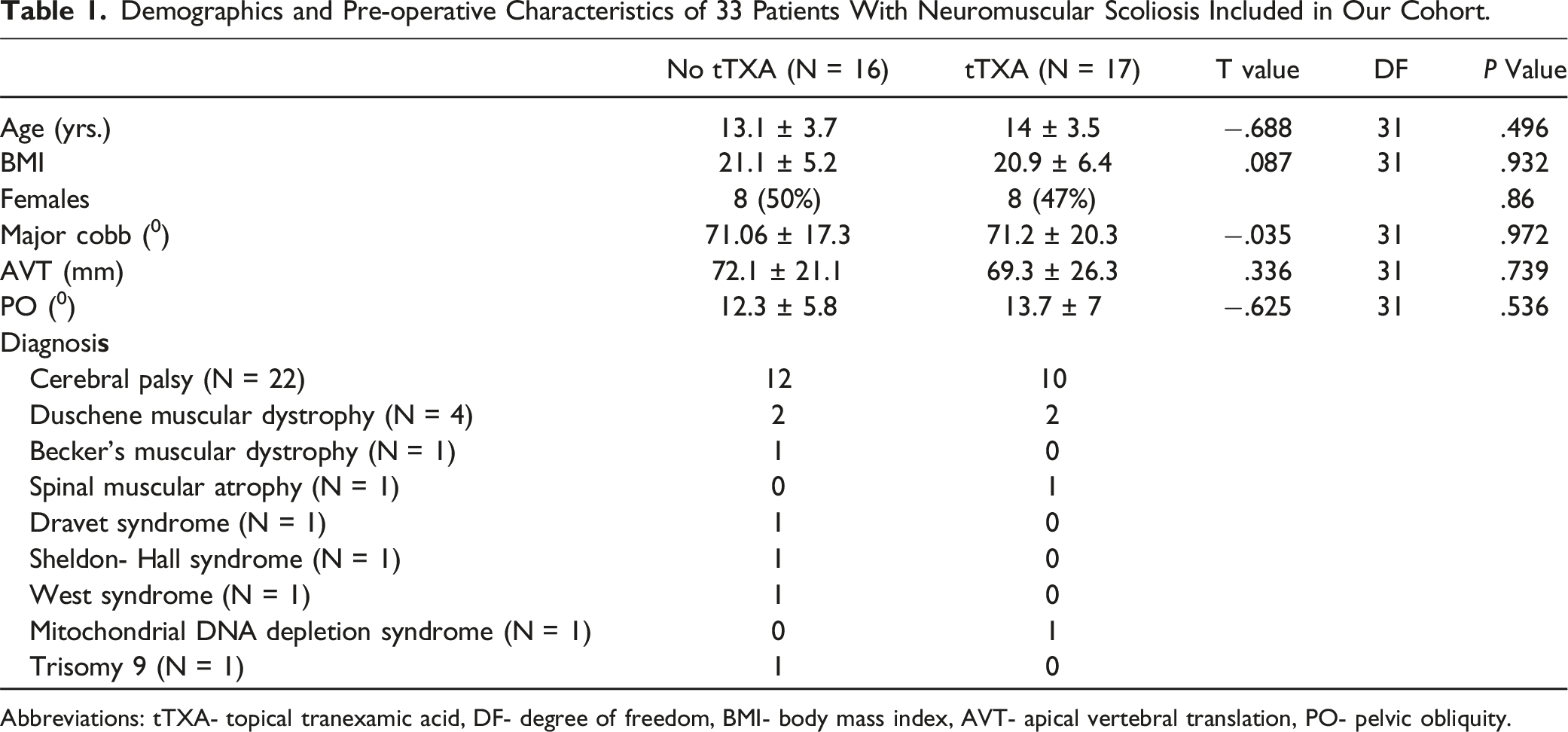
Abbreviations: tTXA- topical tranexamic acid, DF- degree of freedom, BMI- body mass index, AVT- apical vertebral translation, PO- pelvic obliquity.
Surgical Variables and Intra-operative Outcomes
Comparison of Intra-operative Variables Between the tTXA and Control Groups of Neuromuscular Scoliosis Patients Included in Our Study.
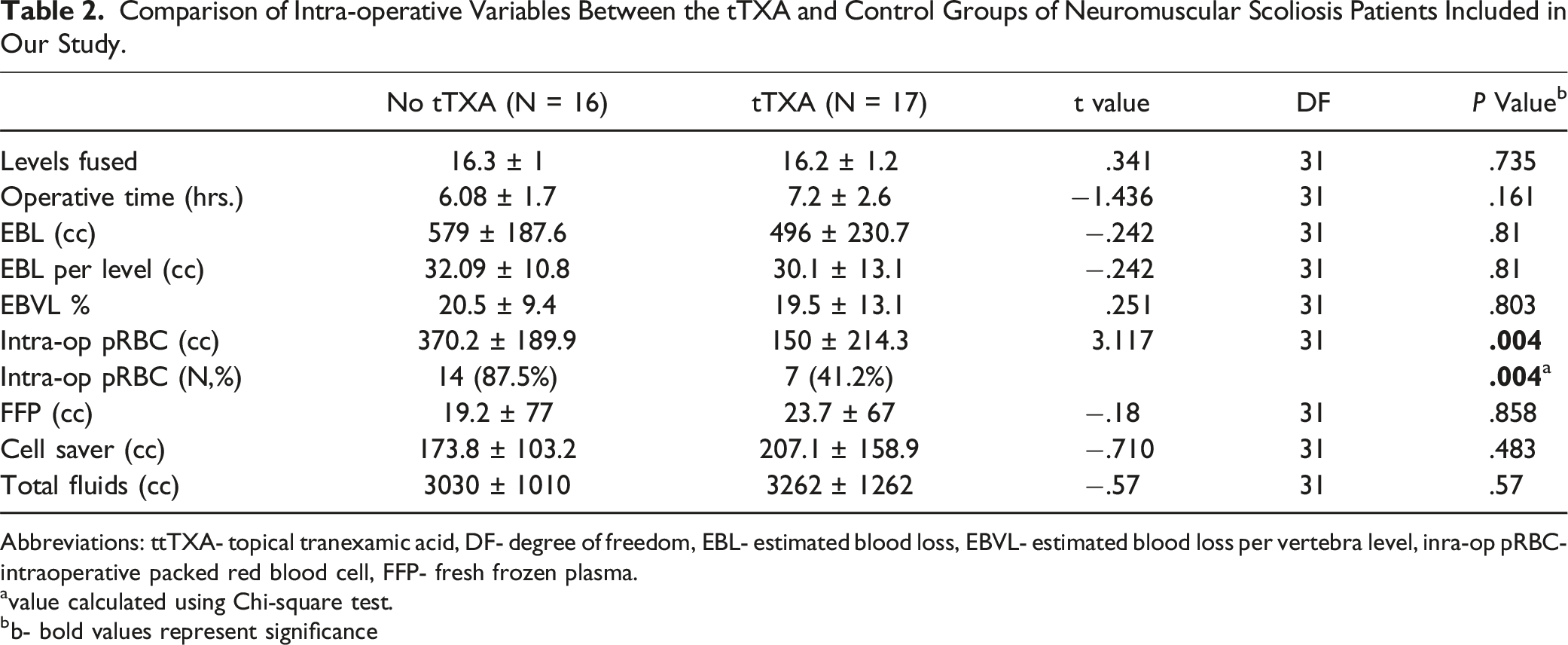
Abbreviations: ttTXA- topical tranexamic acid, DF- degree of freedom, EBL- estimated blood loss, EBVL- estimated blood loss per vertebra level, inra-op pRBC- intraoperative packed red blood cell, FFP- fresh frozen plasma.
avalue calculated using Chi-square test.
bb- bold values represent significance
Post-operative Outcomes
Comparison of Immediate Post-operative Variables Between the tTXA and Control Groups of Neuromuscular Scoliosis Patients Included in Our Study.
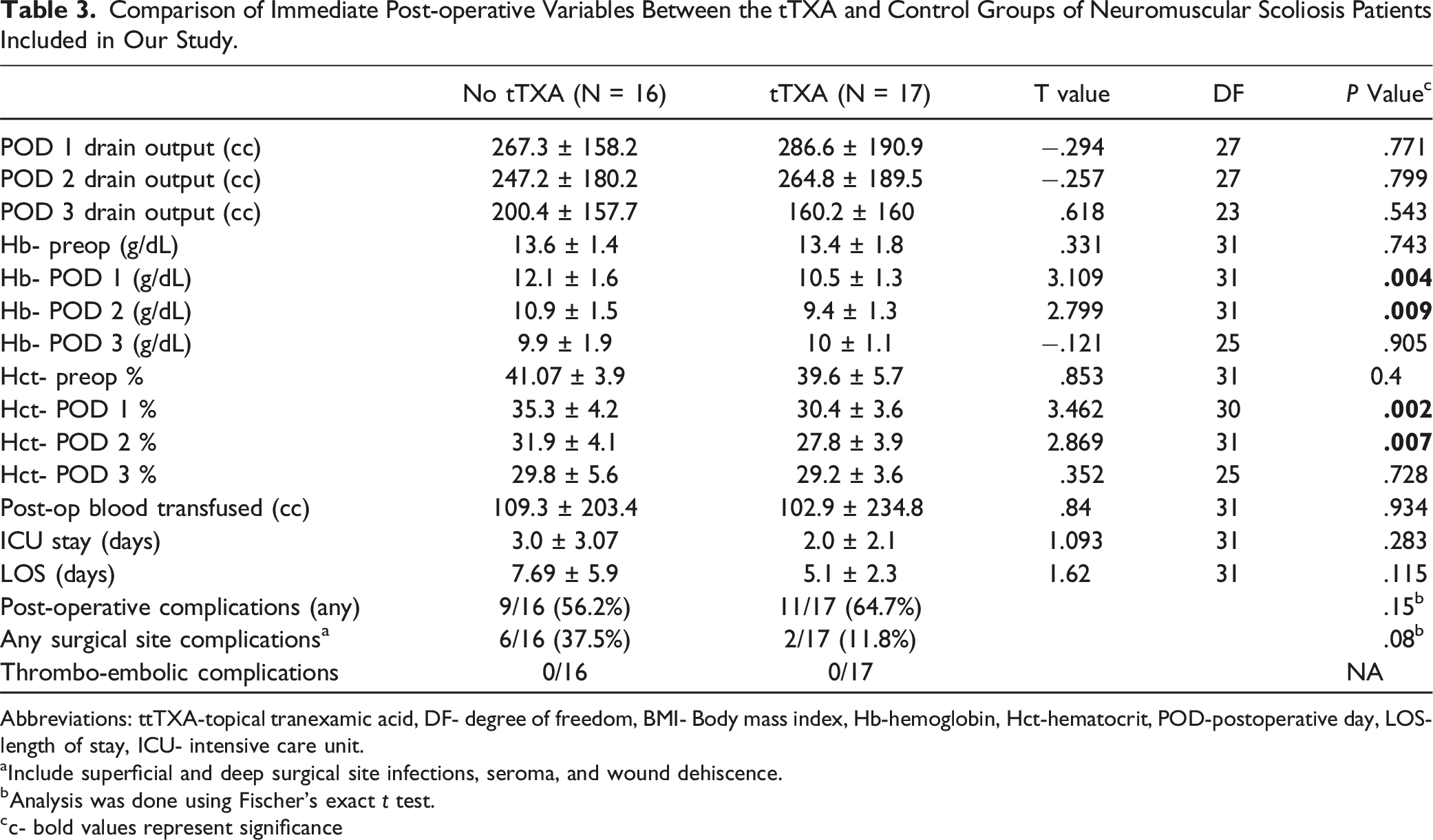
Abbreviations: ttTXA-topical tranexamic acid, DF- degree of freedom, BMI- Body mass index, Hb-hemoglobin, Hct-hematocrit, POD-postoperative day, LOS- length of stay, ICU- intensive care unit.
aInclude superficial and deep surgical site infections, seroma, and wound dehiscence.
bAnalysis was done using Fischer’s exact t test.
c- bold values represent significance
Discussion
Neuromuscular scoliosis is a complex deformity often associated with massive blood loss. The use of systemic tranexamic acid (TXA) has been very successful in spinal deformity surgeries as demonstrated by numerous clinical trials. More recently, many groups have explored the role of topical TXA administered in various forms across multiple surgical specialties in reducing peri-operative blood loss. The plasma concentration of topically applied TXA has shown to be approximately 90% less than when the medication is administered systemically. 18 However, several outstanding questions remain unanswered regarding the application of tTXA in pediatric spine surgeries, especially in children with medically complex neuro-muscular conditions. Our study reports that the use of topical TXA as TXA-soaked sponges packed intra-operatively throughout the procedure is associated with decreased need for intra-operative transfusions during PSF for children with NMS.
Existing literature on the use of tTXA in spine surgeries primarily focuses on its effect on post-operative blood loss and transfusion rates when used as an irrigating solution prior to the end of the procedure.19,20 However, considering the continuous nature of osseous and epidural bleeding during spinal deformity surgery, it is important to investigate modalities of intra-operative application of tTXA for continuous effect. In 2017, Xu et al reported their results of a randomized control trial to see the efficacy of tTXA sponges compared to gelatin sponges in adult patients with lumbar degenerative conditions undergoing PSF. 21 They reported that there was no difference in intra-operative blood loss between the 2 groups. Additionally, the tTXA group received less amount of blood transfusions compared to the gelatin sponge group, however, it is not mentioned if this transfusion was intra- or post-operative. Our study demonstrated that although EBVL% was lower in the tTXA group, this did not reach significance (P > .05). However, the tTXA group received significantly lower intra-operative blood product transfusions compared to the control group not only in terms of quantity but also in terms of frequency.
In a recent meta-analysis on tTXA in spinal surgeries, Fatima et al. pooled data from 8 studies (N = 609) and concluded that there was a statistically significant difference in terms of post-operative blood loss (PBL), post-operative hemoglobin, operative time, post-operative transfusion rate, post-operative drain output and duration of hospital stay in patients treated with tTXA compared to the control group. 15 Our study did not show any significant difference in the drain output for 72 hours when tTXA sponges were used intra-operatively in NMS patients. We did not employ tTXA as an irrigating solution soaked in the wound prior to closure as most studies analyzed by Fatima et al. Also, due to the study design, we were unable to calculate the exact post-operative blood loss using the drain output and hematocrit of drain output as suggested by Ren et al. 20 In addition, the control group had higher mean Day 1 and day 2 hemoglobin and hematocrits compared to tTXA group. This can be explained by the fact that the control group received higher intra-operative blood product transfusions.
Previous research has demonstrated that patients who received topical TXA had significantly shorter hospital stays than the control group.20,21 Recently, Yerneni et al. conducted a meta-analysis with 5 studies including 218 patients to evaluate the effect of tranexamic acid (TXA) on postoperative blood loss and hospital stay in spine surgery. 14 Their pool results demonstrated that patients receiving topical TXA had significantly shorter hospital stays than the control group. Although the patients receiving tTXA in our study had shorter ICU and hospital stays than the control group, this difference was not statistically significant.
The potential increase in thromboembolic events is the primary concern when administering an antifibrinolytic medication. 11 Thus, topical TXA has grown in popularity due to its lower systemic absorption while still being effective in reducing blood loss and transfusion rates.16,22-24 In their systematic review and meta-analysis, Luo et al. emphasized that there is no meaningful difference in the incidence of infection, hematoma, DVT, and PE in patients receiving tTXA during spinal surgery. 25 Similar to previous studies, we did not find any thrombo-embolic adverse events with the use of tTXA for 30 days following PSF in our NMS cohort. Being an inexpensive medication, the utility of tTXA in NMS patients can be universal with an estimated cost of $ 12.11 per 1000 mg/10 mL vial at a wholesale cost as of October 2019. 26 Ehresman et al. revealed that intraoperative TXA reduces intraoperative blood loss and has a significant net cost benefit of $328.69 per patient undergoing long segmental spinal fusion surgery. 26
Our study had several limitations. The retrospective nature of our study makes it susceptible to selection bias. It is unfeasible to take into account all the different anesthesia practices over the last 4 years of our data collection period, although at our institution, the anesthesia protocol is relatively standardized. Another limitation of the present study is that different doses or methods of applying tTXA were not compared in this study. In addition, since all the patients included in our study are relatively medically complex, the post-operative transfusions were at the discretion of the intensivist’s care and therefore could not be standardized across the groups. Also, it can be reasonable to assume that certain blood transfusions could also be a result of over-aggressive fluid resuscitation which is quite hard to tease out in this retrospective study. Nevertheless, our study provides initial data on the use of tTXA continuously throughout the surgical procedure in a special medically complex group of patients with neuromuscular and syndromic scoliosis. Future randomized controlled trials are needed to establish an accurate dosage and the complication profile of tTXA in patients with NMS.
Conclusions
Administration of tTXA-soaked sponges is associated with reduced intraoperative blood transfusion requirements in the correction of spinal deformity in patients with neuromuscular and syndromic scoliosis. In addition, no increase in the risk of thromboembolic or other complications was observed in patients who received topical tranexamic acid during spinal deformity surgery due to NMS in this study.
Footnotes
Author Contributions
Osvaldo Conde, Subaraman Ramchandran, Ergin Coskun, Andrew Pierce, BS, Sassan Keshavarzi, Thomas Errico, and Stephen George contributed to the data acquisition, manuscript preparation, approved the version to be published and agree to be accountable for all aspects of work.
Declaration of conflicting interests
Dr. Thomas J. Errico is a speaker and consultant to Stryker. He also has royalties from Stryker and Altus Spine. Dr. Subaraman Ramchandran, Dr. Sassan Keshavarzi, Dr. Ergin Coskun, Andrew Pierce, Osvaldo Conde and Dr. Stephen George declare they have no financial or non-financial interests to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.