
Abstract
Study Design
Retrospective review of a prospectively collected national database
Objectives
To determine the association between preoperative serum albumin levels and perioperative adverse events (AEs) following vertebral corpectomy and posterior stabilization for metastatic spine disease.
Methods
The 2010 to 2019 American College of Surgeons’ National Surgical Quality Improvement (ACS-NSQIP) database was used to identify all patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease. Receiver operative characteristic (ROC) curve analysis was used to determine preoperative serum albumin cut-off values for predicting perioperative AEs. Low preoperative serum albumin was defined as serum albumin below this cut-off value.
Results
A total of 301 patients were included in the study. ROC curve analysis demonstrated serum albumin < 3.25 g/dL as a cut-off value for predicting perioperative AEs. The low serum albumin group had a higher overall perioperative AEs (P = .041), longer post-operative LOS (P < .001), higher 30-day reoperation rate (P = .014), and a higher in-hospital mortality rate (P = .046). Multivariate analysis demonstrated that low preoperative serum albumin was associated with higher perioperative AEs.
Conclusions
Low serum albumin level is associated with higher perioperative AEs, longer postoperative LOS, and higher rates of 30-day reoperation and in-hospital mortality among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease. Strategies to improve preoperative nutritional status in patients undergoing this procedure may improve these perioperative outcome measures within this surgical population.
Level of Evidence
III
Introduction
Hypoalbuminemia is a marker for poor nutritional status and has been associated with increased perioperative AEs following elective spine surgeries.1-3 Serum albumin is a laboratory value included within the comprehensive metabolic panel (CMP) and can be obtained cost-effectively during a routine preoperative visit among patients undergoing surgery. Although costlier, serum prealbumin has been shown to be a more specific indicator of overall nutritional status than albumin and numerous recent studies report a stronger association between low serum prealbumin with post-operative AEs following spine surgery.4-9 However, particularly among patients with an oncologic diagnosis, it is well-documented that both malnutrition and high cancer burden are strong clinical indicators of poor prognosis. 10 Serum albumin has been shown to be an indicator for both malnutrition and chronic inflammation in patients with high cancer burden; thus, is a particularly useful and cost-effective tool for predicting outcomes after various types of oncological surgery.11-14
Patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease have particularly high rates of perioperative adverse events (AEs).15-17 Although a recent study has shown that severe hypoalbuminemia (<2.5 g/dL) is associated with a 7-fold increase 30-day mortality among patients undergoing surgery for metastatic spine disease, no study has investigated the association between preoperative serum albumin levels and perioperative AEs following vertebral corpectomy and posterior stabilization for metastatic spine disease. 18 Furthermore, no prior studies have determined the cut-off value for predicting AEs following this procedure.
Thus, the primary objective of this study was to determine the association between preoperative serum albumin levels and perioperative AEs following vertebral corpectomy and posterior stabilization for metastatic spine disease. The secondary objectives were to determine the preoperative serum albumin cut-off value for predicting post-operative AEs, as well as to determine other variables associated with perioperative AEs.
Methods
This study was exempt from the local institutional review board and from informed consent due to the use of a publicly available national database.
Study Population
The 2010 to 2019 American College of Surgeons’ National Surgical Quality Improvement (ACS-NSQIP) database was used to identify all patients from the United States undergoing vertebral corpectomy and posterior stabilization for metastatic spine tumor. CPT codes utilized for the inclusion of patients undergoing vertebral corpectomy and posterior stabilization were a combination of: 63081, 63300-63306 and 22840, 22842-22844. ICD-9 and ICD-10 codes utilized for the inclusion of patients with the diagnosis of metastatic spine tumor were: 198.3, 198.4, 198.5, C79.49, C79.5, C79.51, C79.52, and C79.4. The exclusion criteria were patients who underwent corpectomy or posterior stabilization alone and a diagnosis of a primary spinal neoplasm.
Data Collection
Preoperative demographic data including gender, age, American Society of Anesthesiologist (ASA) class, comorbidities, and functional status were collected. Preoperative laboratory values including serum albumin, serum creatinine, white blood cell (WBC) count, and platelet count were also obtained. Intraoperative data including duration of surgery and the location of corpectomy were also collected. Perioperative outcome measures were also obtained. Primary outcome measures included perioperative AEs including post-operative anemia requiring transfusion, cardiac arrest, myocardial infarction, sepsis, wound complication (wound dehiscence and deep wound infection), cerebrovascular accident (CVA), acute kidney injury (AKI), pneumonia, urinary tract infection (UTI), unplanned reintubation, and venous thromboembolism (VTE). Secondary outcome measures included post-operative length of stay (LOS), discharge disposition (home, facility, or unknown), 30-day readmission rates, 30-day reoperation rates, and in-hospital mortality rates.
Statistical Analysis
Data analysis was performed using SPSS statistical software (Version 25.0; SPSS, Inc, Chicago, IL). Two-tailed student t-test was used to analyze continuous data and the Chi-Sqre or Fisher’s exact test was used to analyze categorical data. The Mann-Whitney U test was utilized for continuous variables with non-normal distribution. A P value < .05 was considered statistically significant. Receiver operative characteristic (ROC) curve analysis and Youden index were used to determine preoperative serum albumin cut-off values for predicting perioperative AEs. Low preoperative serum albumin was defined as serum albumin below this cut-off value. The area under the ROC curve (AUC) as well as the corresponding 95% confidence interval (CI) was used to measure the overall validity. The odds ratio (OR) with 95% CI was calculated for comparing perioperative outcomes. Univariate and multivariate logistic regression modeling were used to determine the association of demographic variables and preoperative laboratory values with perioperative AEs.
Results
Demographics and Preoperative Laboratory Values of the Study Population.
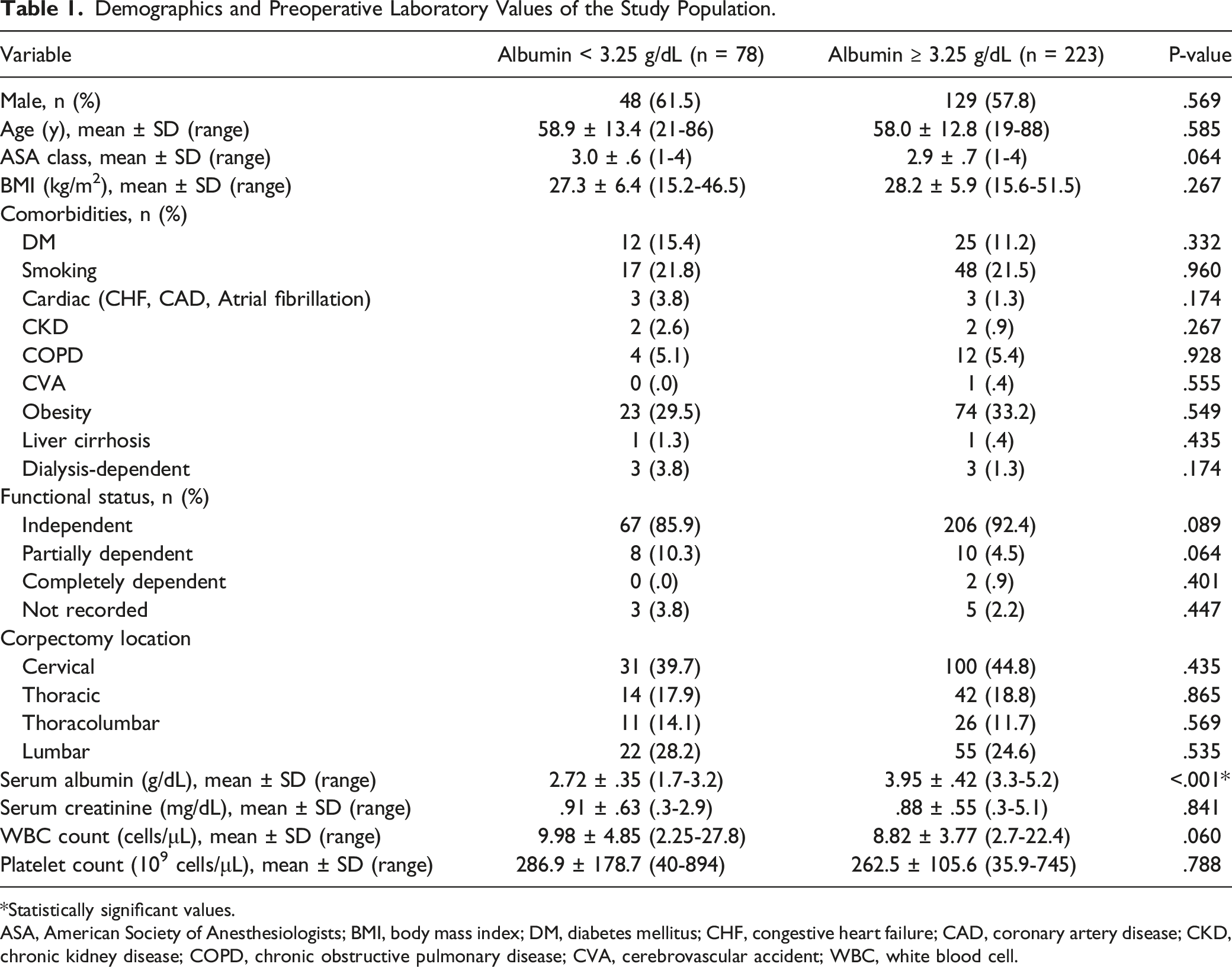
*Statistically significant values.
ASA, American Society of Anesthesiologists; BMI, body mass index; DM, diabetes mellitus; CHF, congestive heart failure; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; WBC, white blood cell.
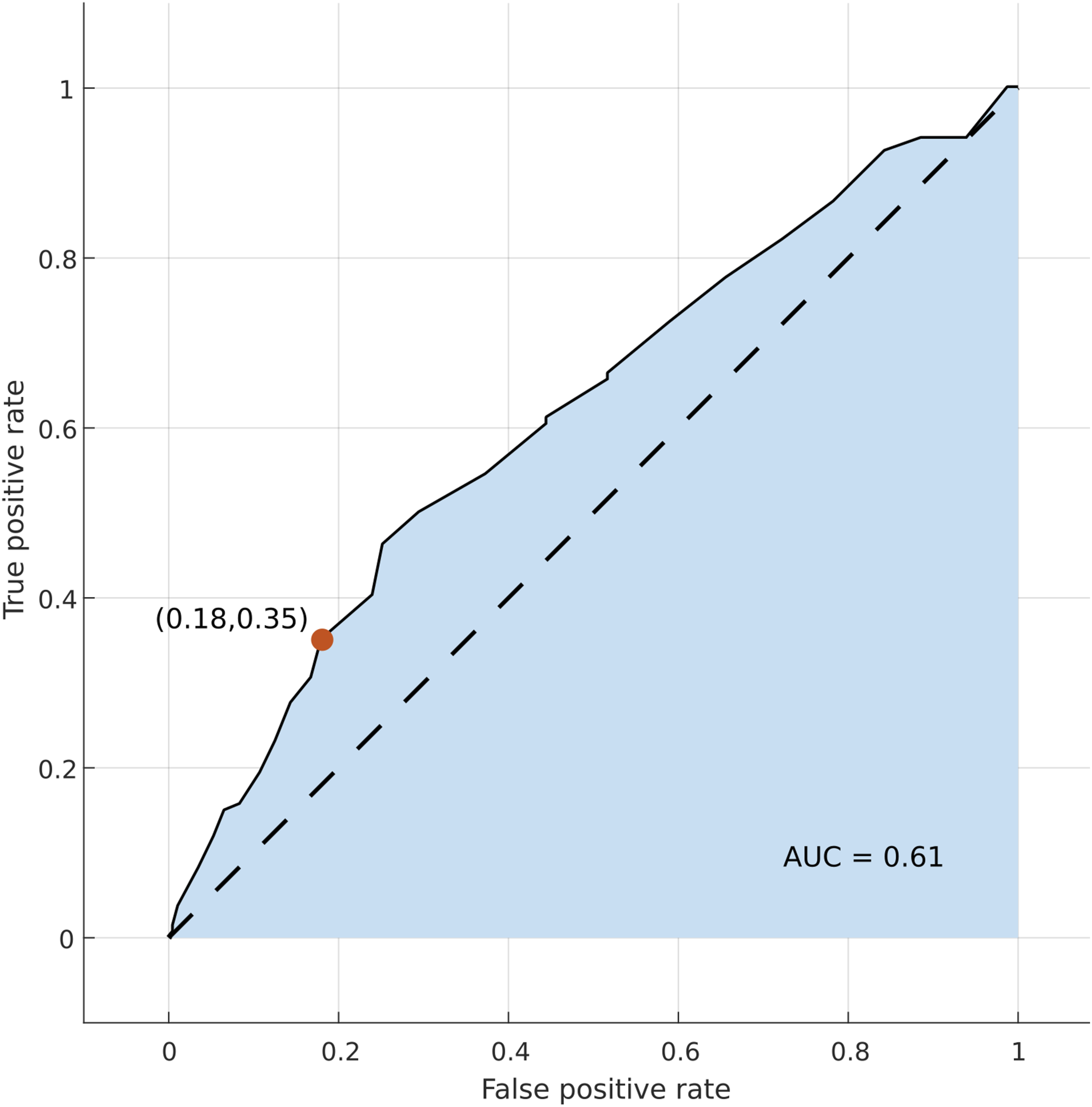
ROC curve of preoperative serum albumin predicting perioperative AEs. The AUC was .61 (P = <.001). Serum albumin < 3.25 g/dL maximized the power of serum albumin as a predictor for perioperative AEs.
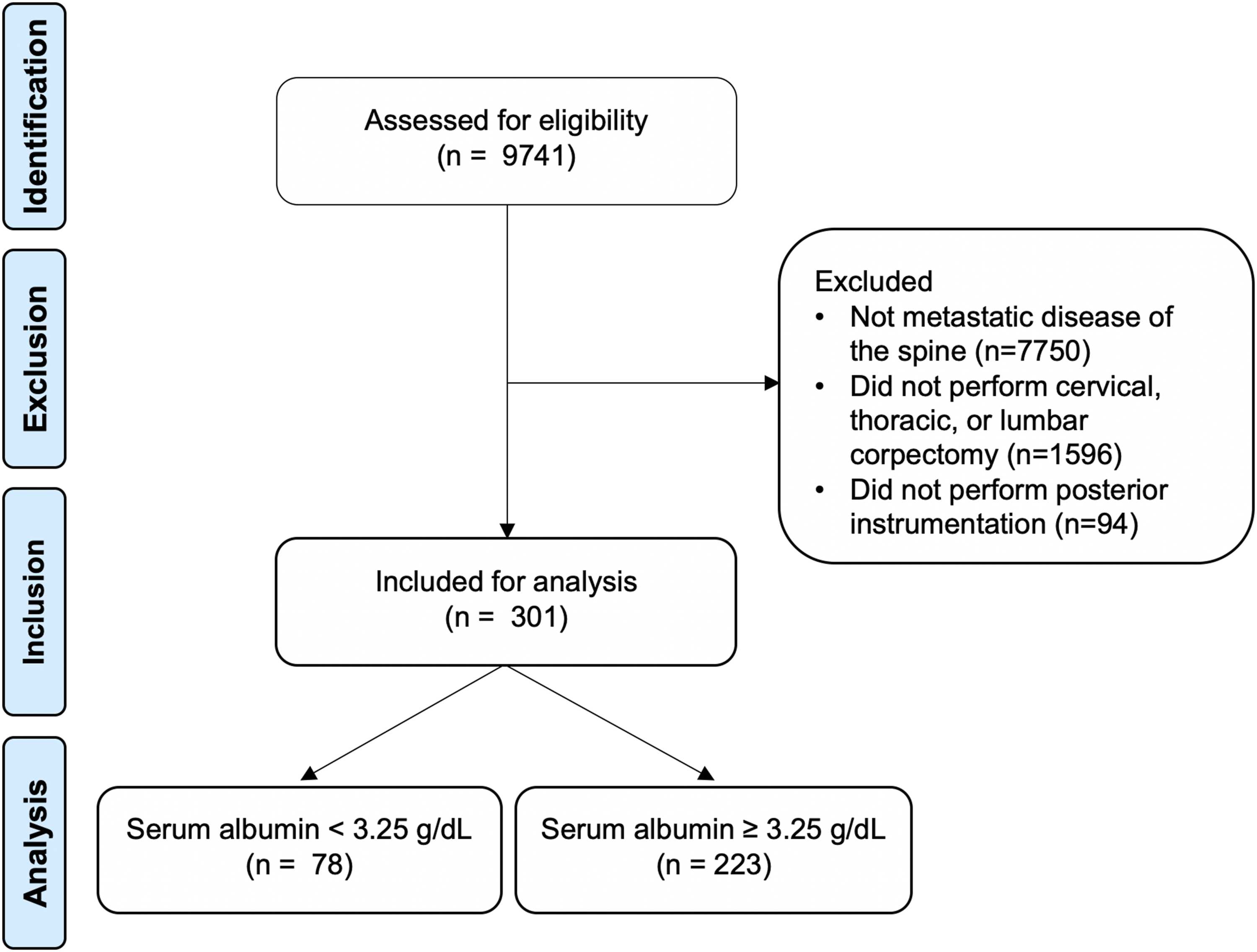
Study flow diagram.
Comparison of Perioperative Outcomes.
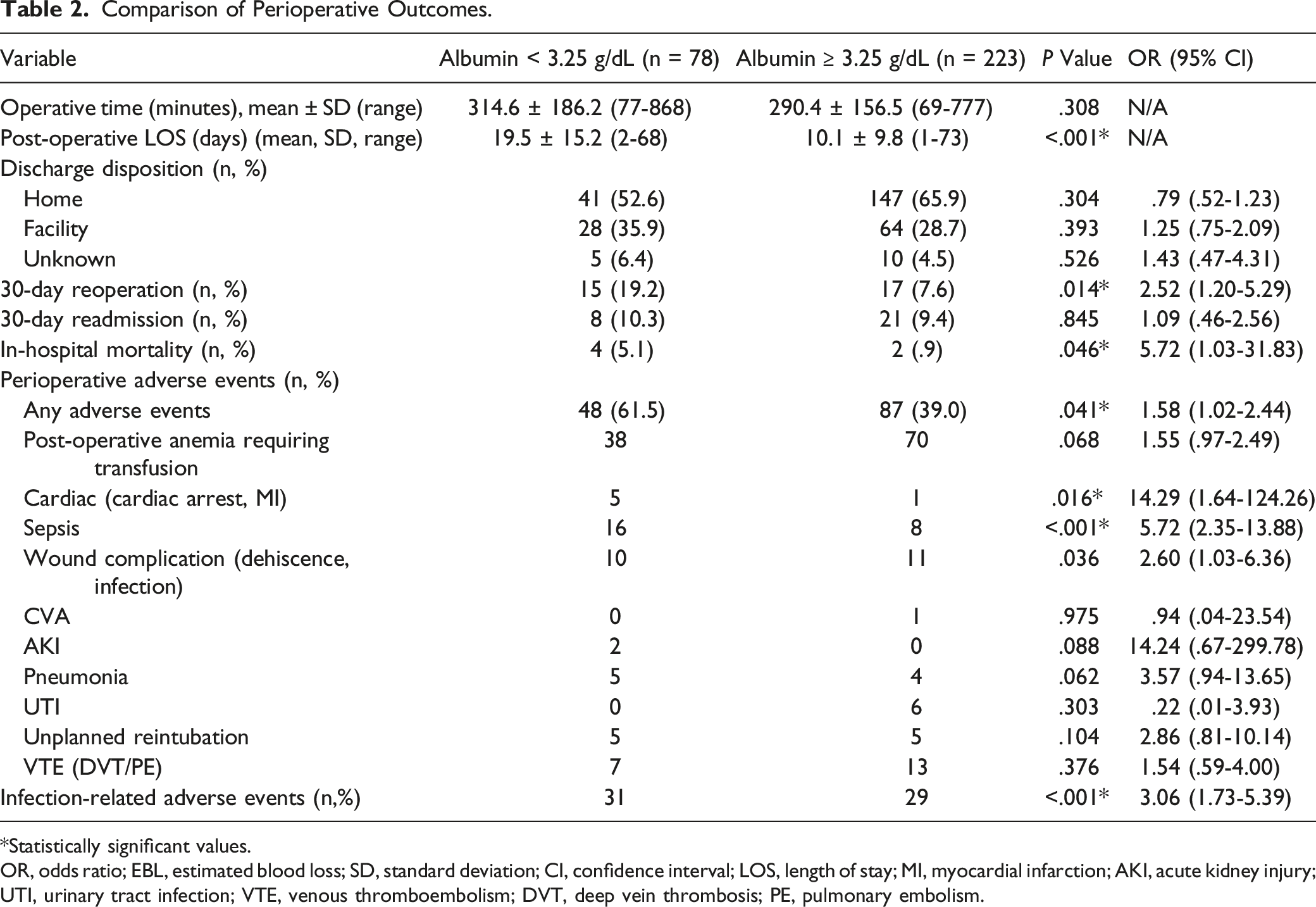
*Statistically significant values.
OR, odds ratio; EBL, estimated blood loss; SD, standard deviation; CI, confidence interval; LOS, length of stay; MI, myocardial infarction; AKI, acute kidney injury; UTI, urinary tract infection; VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism.
Crude and adjusted odds ratios of AEs for serum albumin and other potential risk factors.
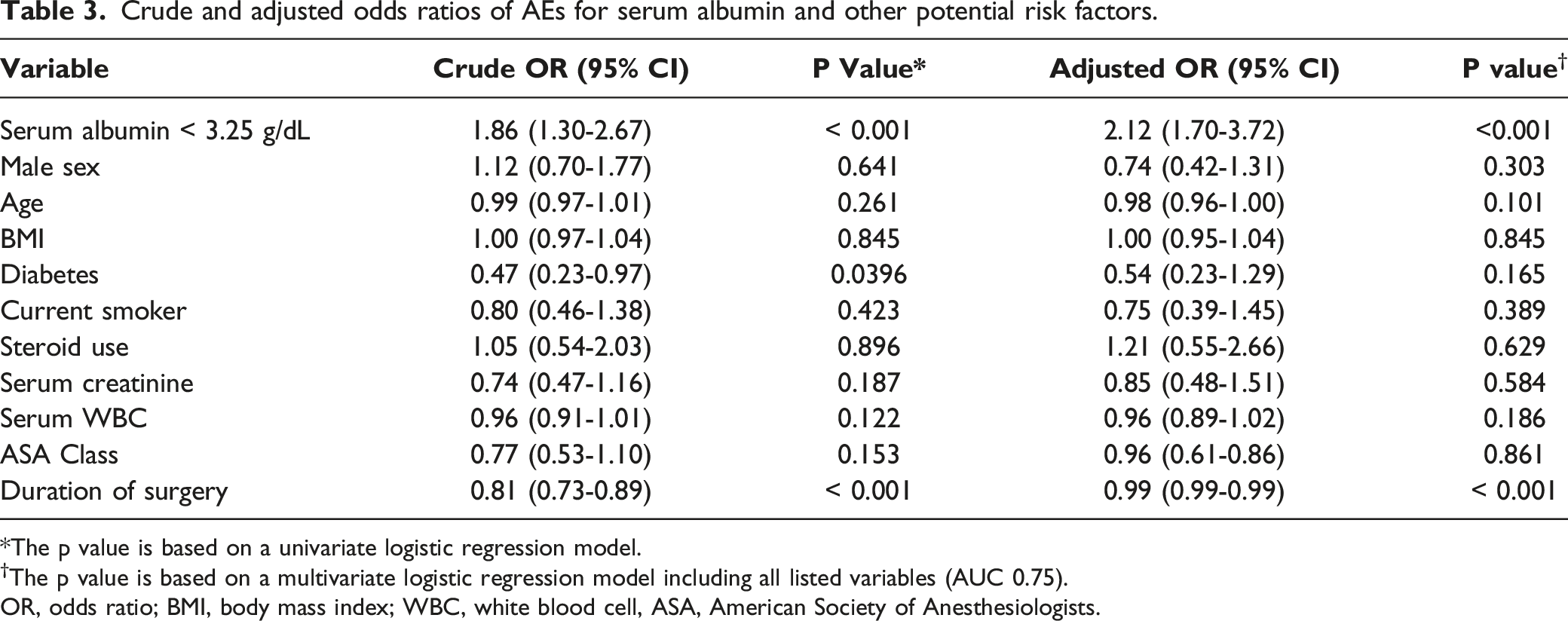
*The p value is based on a univariate logistic regression model.
†The p value is based on a multivariate logistic regression model including all listed variables (AUC 0.75).
OR, odds ratio; BMI, body mass index; WBC, white blood cell, ASA, American Society of Anesthesiologists.
Discussion
In this study, we investigated the utility of preoperative serum albumin as a predictor of perioperative AEs among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease. Our analysis demonstrated that the cut-off serum albumin for predicting perioperative AEs within the patient population was < 3.25 g/dL. Comparison between patients with low serum albumin levels defined as patients below this cut-off value with patients at or above this cut-off value demonstrated that low serum albumin levels is associated with higher perioperative AEs, longer postoperative LOS, and higher rates of 30-day reoperation and in-hospital mortality among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease
The preoperative serum albumin cut-off value was developed methodically using the ROC curve and Youden index for predicting perioperative AEs. Prior studies have develop cut-off values to define hypoalbuminemia and severe hypoalbuminemia; however, these are arbitrary values that may not be as useful for perioperative risk assessment within the patient population.1-3,18 Gelfand et al defined severe hypoalbuminemia as serum albumin ≤ 2.5 g/dL and found that patients with severe hypoalbuminemia who underwent operative intervention for metastatic spine disease had a 7-fold increased risk of 30-day mortality. 18 Although we found similar findings within our patient population, their methodology included patients undergoing any operative intervention for metastatic spine disease regardless of the complexity of the procedure. Our study specifically assessed patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease which have been shown to have particularly high rates of perioperative AEs.15-17
Perioperative risk stratification is becoming an important process particularly with patients with metastatic spine disease requiring complex spine surgeries that are known to have high perioperative complications. Although complications are known to be higher among metastatic cancer patients in general, specific variables that predict perioperative outcomes among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease remain largely unknown.1-3,18 In this study using a multivariate regression model, we found that preoperative serum albumin < 3.25 g/dL was associated with a higher risk for developing perioperative AEs. These findings were similar to results reported by Camino-Willhuber et al and Gelfand et al who both reported higher perioperative AEs among patients with hypoalbuminemia who underwent other types of spinal surgery.
Interestingly, our study also showed that a shorter length of operation was associated with a higher incidence of perioperative AEs. This contradicts multiple prior studies that demonstrates higher incidences of perioperative AEs with increased operative time.19-21 Our speculation is that patients that undergo vertebral corpectomy and posterior stabilization more quickly is associated with worse overall preoperative morbidities that requires minimizing time of general anesthesia and/or have a worse cancer-related prognosis requiring a palliative separation surgery and stabilization procedure alone vs a more curative en-bloc procedure. Future studies designed to observe the effects of this specific confounder that separates patients that underwent a partial corpectomy for separation surgery vs those that underwent a complete corpectomy may be beneficial for a better understanding of this result. Although statistically significant, this association was weak compared to serum albumin on multivariable analysis.
Currently, there are a variety of scoring systems utilized for preoperative evaluation of metastatic spine disease.22-26 Scoring systems as described by Tokuhashi et al and Tomita et al are widely used preoperative evaluation methods for predicting prognosis in metastatic spine disease.22-24 However, there are have been no scoring systems for predicting perioperative AEs within the 30-day post-operative period within this population. One scoring system described by Ghori et al incorporated serum albumin < 3.5 g/dL within their scoring parameters to better predict 1-year mortality among patients undergoing surgery for metastatic spine disease than the established modified Bauer score methodology.25,26 Thus, our study demonstrating a pre-operative serum albumin cut-off value of < 3.25 g/dL that predicts perioperative AEs is a novel finding that may be useful for additional preoperative evaluation and counseling regarding short-term outcomes.
There are limitations in our study. This is a retrospective review of the 2010-2019 ACS-NSQIP database that consists of a prospectively collected data of 301 patients from 603 hospitals within the United States, which may lead to selection bias and adversity of the collected data. This database merely collects data within a 30-day post-operative period; thus, we are unable to investigate the long-term association between pre-operative serum albumin levels and AEs within the surgical population. Although we included similar patient population within our study by using consistent CPT codes and ICD-9/ICD-10 codes, the cases are inevitably variable in nature and the aggregate result may not be reflective of all outcomes. Further studies demonstrating the external validity of this data as well as long-term follow-up may be necessary prior to its application in practice. Additional co-morbidities such as hepatocellular necrosis, liver metastasis, and specific diseases causing gastrointestinal malabsorption not included within the NSQIP database may also be contributors to hypoalbuminemia, which may be confounders that are unable to be investigated within this study. Finally, although this study demonstrates an association between low pre-operative serum albumin levels and perioperative AEs, it is yet unclear whether preoperative optimization and repletion of serum albumin will lead to decreased rates of AEs.
Despite these limitations, to our knowledge, this is the largest study that evaluates the relationship between preoperative serum albumin and perioperative AEs among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease. The strength of this study was the ability to methodically detect a serum albumin cut-off value for predicting perioperative AEs within this surgical population.
Conclusion
Low serum albumin level is associated with higher perioperative AEs, longer postoperative LOS, and higher rates of 30-day reoperation and in-hospital mortality among patients undergoing vertebral corpectomy and posterior stabilization for metastatic spine disease. Strategies to improve preoperative nutritional status in patients undergoing this procedure may improve these perioperative outcome measures within this surgical population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Takashi Hirase, Khaled Taghlabi, Jesus Cruz-Garza, and Amir Faraji has no conflicts of interests to disclose. Rex Marco has the following disclosures: DePuy, A Johnson & Johnson Company: Paid presenter or speaker Globus Medical: IP royalties. Comron Saifi has the following disclosures: Acquisition of Vertera Inc. by NuVasive’ Shares: Stock or stock Options. Alphatec Spine: Stock or stock Options. Nuvasive: Paid consultant. Restor3d: Stock or stock Options.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.