
Abstract
Study Design
Multicenter, prospective cohort
Objectives
Malalignment following adult spine deformity (ASD) surgery can impact outcomes and increase mechanical complications. We assess whether preoperative goals for sagittal alignment following ASD surgery are achieved.
Methods
ASD patients were prospectively enrolled based on 3 criteria: deformity severity (PI-LL ≥25°, TPA ≥30°, SVA ≥15 cm, TCobb≥70° or TLCobb≥50°), procedure complexity (≥12 levels fused, 3-CO or ACR) and/or age (>65 and ≥7 levels fused). The surgeon documented sagittal alignment goals prior to surgery. Goals were compared with achieved alignment on first follow-up standing radiographs.
Results
The 266 enrolled patients had a mean age of 61.0 years (SD = 14.6) and 68% were women. Mean instrumented levels was 13.6 (SD = 3.8), and 23.2% had a 3-CO. Mean (SD) offsets (achieved-goal) were: SVA = −8.5 mm (45.6 mm), PI-LL = −4.6° (14.6°), TK = 7.2° (14.7°), reflecting tendencies to undercorrect SVA and PI-LL and increase TK. Goals were achieved for SVA, PI-LL, and TK in 74.4%, 71.4%, and 68.8% of patients, respectively, and was achieved for all 3 parameters in 37.2% of patients. Three factors were independently associated with achievement of all 3 alignment goals: use of PACs/equivalent for surgical planning (P < .001), lower baseline GCA (P = .009), and surgery not including a 3-CO (P = .037).
Conclusions
Surgeons failed to achieve goal alignment of each sagittal parameter in ∼25-30% of ASD patients. Goal alignment for all 3 parameters was only achieved in 37.2% of patients. Those at greatest risk were patients with more severe deformity. Advancements are needed to enable more consistent translation of preoperative alignment goals to the operating room.
Introduction
Adult spinal deformity (ASD) is a heterogeneous diagnosis with a broad range of etiologies and manifestations that all have in common malalignment of the spine.1,2 ASD is a major healthcare issue due to its growing incidence as Western populations continue to age. The prevalence of ASD has been estimated to be as high as 60% in the older population. 3 Patients with symptomatic ASD can have profound health impact, including back and leg pain, weakness, myelopathy, and disability and mobility issues.4-7 Although nonoperative treatments may sufficiently treat or temporize symptoms in some patients with symptomatic ASD, for others these measures fail to provide sufficient or durable relief. 8 Multiple reports have documented the potential for operative treatment to provide significant improvement for symptomatic ASD, including many that have directly compared nonoperative and operative treatment approaches.5,6,9-16
The general goals of surgery for ASD include reducing pain and disability and improving quality of life through decompression of neural elements and restoration of appropriate spinopelvic alignment. Over the past two decades, the importance of the sagittal plane has been increasingly recognized, with reports of significant correlations between health-related quality of life (HRQL) measures and sagittal vertical axis (SVA), T1 pelvic angle (TPA), pelvic tilt (PT), and pelvic incidence to lumbar lordosis mismatch (PI-LL).17-19 Achievement of appropriate sagittal spino-pelvic alignment has also been shown to be important for reduction of mechanical complications, including instrumentation failure and proximal junctional kyphosis (PJK), that can result in major revision surgery.20-25
Although the definition of ASD is inherently based upon the presence of malalignment and multiple studies have shown that correcting this malalignment is important for patient-reported outcomes and for the mechanical stability of the reconstruction, there remains considerable controversy with regard to optimal strategies and goals for spinal realignment in ASD surgery.24-28 Regardless of the favored alignment strategy and goals, the surgeon has increasingly sophisticated software available to aid in planning the specific surgical treatment and in assessing anticipated resulting spinal alignment.29-34 Despite the ability for surgeons to preoperatively generate alignment goals and a specific surgical strategy, it remains unclear whether preoperative alignment goals are consistently achieved in the operating room. The objective of this study was to prospectively assess how often the operating surgeon’s preoperative goals for sagittal alignment following complex ASD surgery were achieved on first follow-up standing radiographs. A secondary objective was to assess for clinical, radiographic, and operative factors that may be associated with achievement of these alignment goals.
Methods
Study Design and Population
This is a multicenter, prospective cohort study conducted to assess the outcome of complex ASD among those who underwent surgical treatment at 13 centers across the United States. This study is registered through ClinicalTrials.gov (NCT04194138). All study participants signed informed consent, and the study received institutional review board approval (Presbyterian/St Luke’s Medical Center, HCA-HealthONE IRB #1241485-12). Eligible patients had a diagnosis of adult congenital, degenerative, idiopathic, or iatrogenic spinal deformity with plan for operative treatment. In addition, for this study of complex ASD, patients were required to meet any of the following criteria: (1) radiographic criteria (PI-LL ≥25°, TPA ≥30°, SVA >15 cm, thoracic scoliosis≥70°, thoracolumbar/lumbar scoliosis≥50°, or global coronal alignment>7 cm); (2) procedural criteria (posterior spinal fusion >12 levels, 3-column osteotomy (3-CO), or anterior-column reconstruction (ACR); or (3) geriatric criteria (age >65 years and minimum 7 levels of spinal instrumentation during surgery). Exclusion criteria included active spinal infection or neoplasm, deformity due to acute trauma, neuromuscular conditions, syndromic scoliosis, inflammatory arthritis/autoimmune diseases, and pregnancy. Decisions regarding surgical indications, clinical and radiographic evaluation, surgical procedure and approach, and instrumentation were at the discretion of the operating surgeon. The specific study objective of assessing achievement of goal alignment was proposed and required data fields included on case report forms prior to initiation of patient enrollment.
Data Collection
At preoperative baseline and postoperative follow-up, demographic, clinical, radiographic, and operative data were collected using standardized forms. Prior to surgery, the operating surgeon documented sagittal alignment goals for each patient, including SVA, PI-LL, and TK. As a requirement for a site to enroll a patient in the study, these goals had to be submitted to the central data repository prior to surgery.
Full-length standing (head to toe) anteroposterior and lateral EOS radiographs were obtained for all patients at the time of enrollment and at follow-up visits. Radiographs were analyzed at a central site using validated software (Spineview, ENSAM Laboratory of Biomechanics, Paris, France). 34 Coronal Cobb angles, PT, PI-LL mismatch, SVA, TPA, global coronal alignment (GCA), and thoracic kyphosis (TK) were assessed using standard techniques. Patients were classified based on the SRS-Schwab adult thoracolumbar spinal deformity classification.35-37
Enrolling surgeons were queried with regard to whether they use specific surgical planning tools and whether they employ specific goal alignment criteria in planning their ASD surgeries. Surgery planning tools were grouped into either commercially available planning software (e.g., Surgimap) specifically designed for spine surgery planning or generic imaging workstations (e.g., PACS). Goal alignment criteria were reported as the specific system used (e.g., age-adjusted alignment, 27 Global Alignment and Proportion [GAP] Score, 24 or Roussouly classification 25 ) or as patient-individualized alignment criteria if a surgeon indicated that no specific criteria were used but rather goals were individualized to the patient.
Data Assessment and Statistical Analysis
Statistical analysis was performed using IBM SPSS (version 28.0). Descriptive statistics were reported using means and standard deviations (SD) for continuous variables and frequencies with percentages for categorical variables. Pearson chi-square test was used to compare categorical variables and Student t-test for continuous variables. Continuous data were assessed using the Kolmogorov-Smirnov test for normality. Correlations between continuous variables were assessed using Pearson correlation coefficients. Univariate analyses were performed to assess for associations between demographic, clinical, operative, and radiographic parameters and whether alignment goals were achieved for SVA, PI-LL, and TK. Multivariate logistic regression models included all variables with P < .10 from the univariate comparisons. All tests were two-tailed, with a significance level of P-value < .05.
Goal alignment parameters, as determined by the operating surgeon prior to surgery, were compared with achieved alignment based on radiographs obtained at 6-week follow-up after surgery. Although surgeons were required to provide their alignment goals as specific numbers (not ranges), the surgeon did not have to achieve the exact numbers in order for it to be considered a favorable match between goal and achieved alignment. Goals were compared with achieved alignment and the overall mean and SD for all patients were calculated for the offset (achieved minus goal) for each radiographic parameter. Goal alignment was considered attained if the offset was within ±1 SD of the achieved.
Results
Patient Population
Baseline Demographic/Clinical, Baseline Radiographic, and Operative Parameters for 266 Adults with Spinal Deformity. a
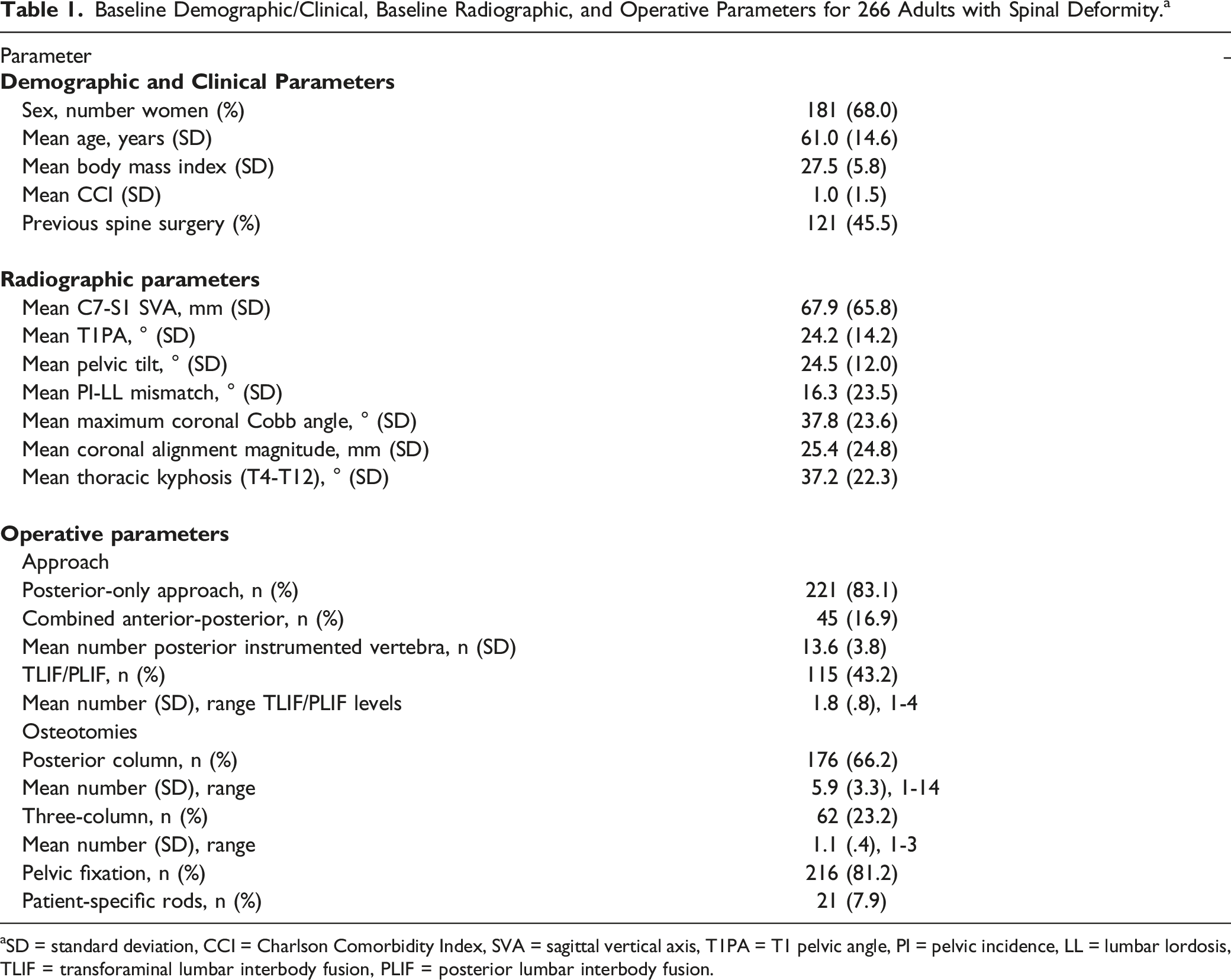
aSD = standard deviation, CCI = Charlson Comorbidity Index, SVA = sagittal vertical axis, T1PA = T1 pelvic angle, PI = pelvic incidence, LL = lumbar lordosis, TLIF = transforaminal lumbar interbody fusion, PLIF = posterior lumbar interbody fusion.
Summary of 266 Adults Treated Surgically for Spinal Deformity, Stratified by Surgeon, Surgery Planning Tools and Alignment Criteria Used by the Surgeon, and Whether the Respective Surgeon’s Sagittal Alignment Goals were Achieved. a
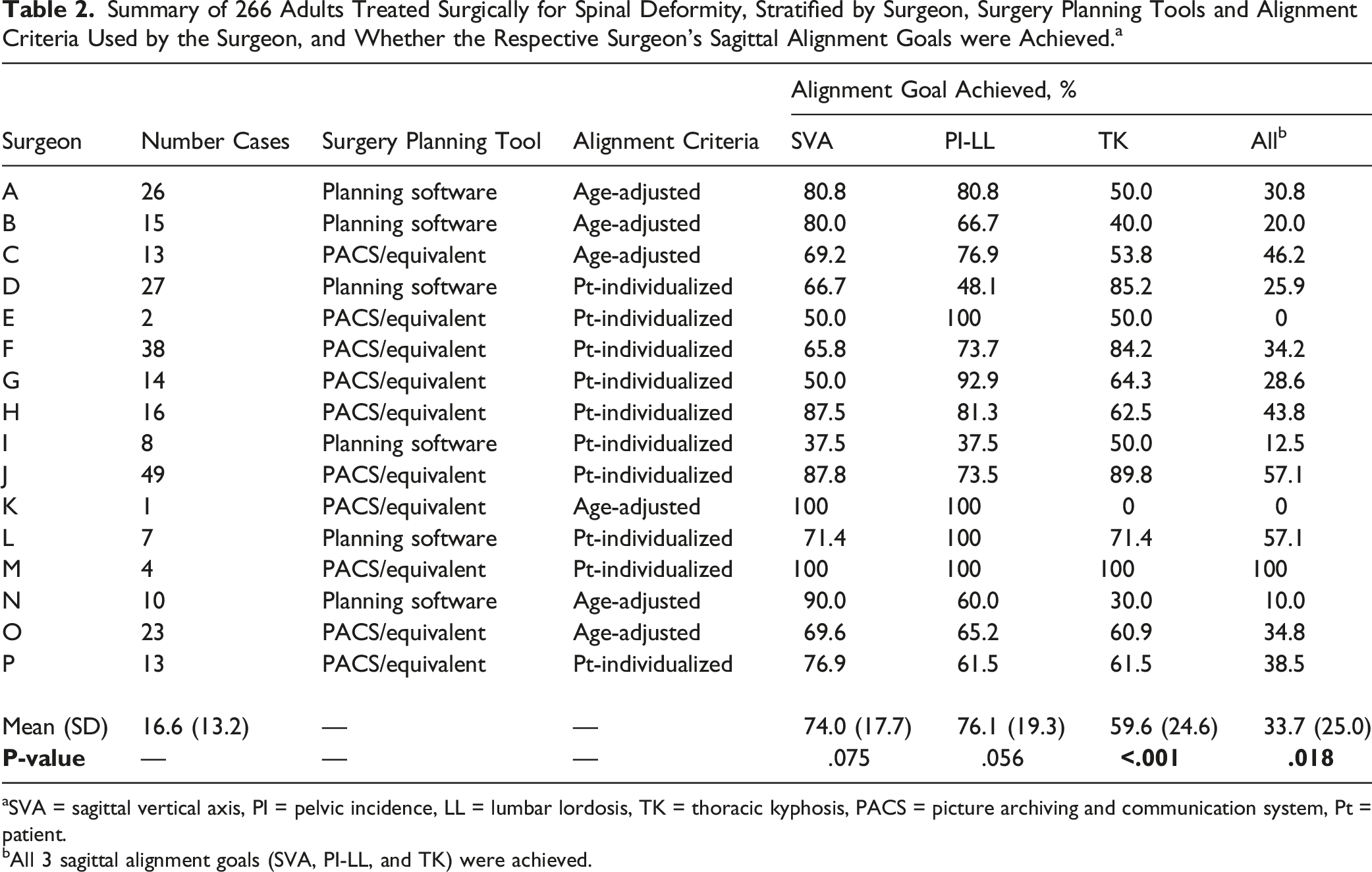
aSVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis, PACS = picture archiving and communication system, Pt = patient.
bAll 3 sagittal alignment goals (SVA, PI-LL, and TK) were achieved.
Achievement of Sagittal Alignment Goals
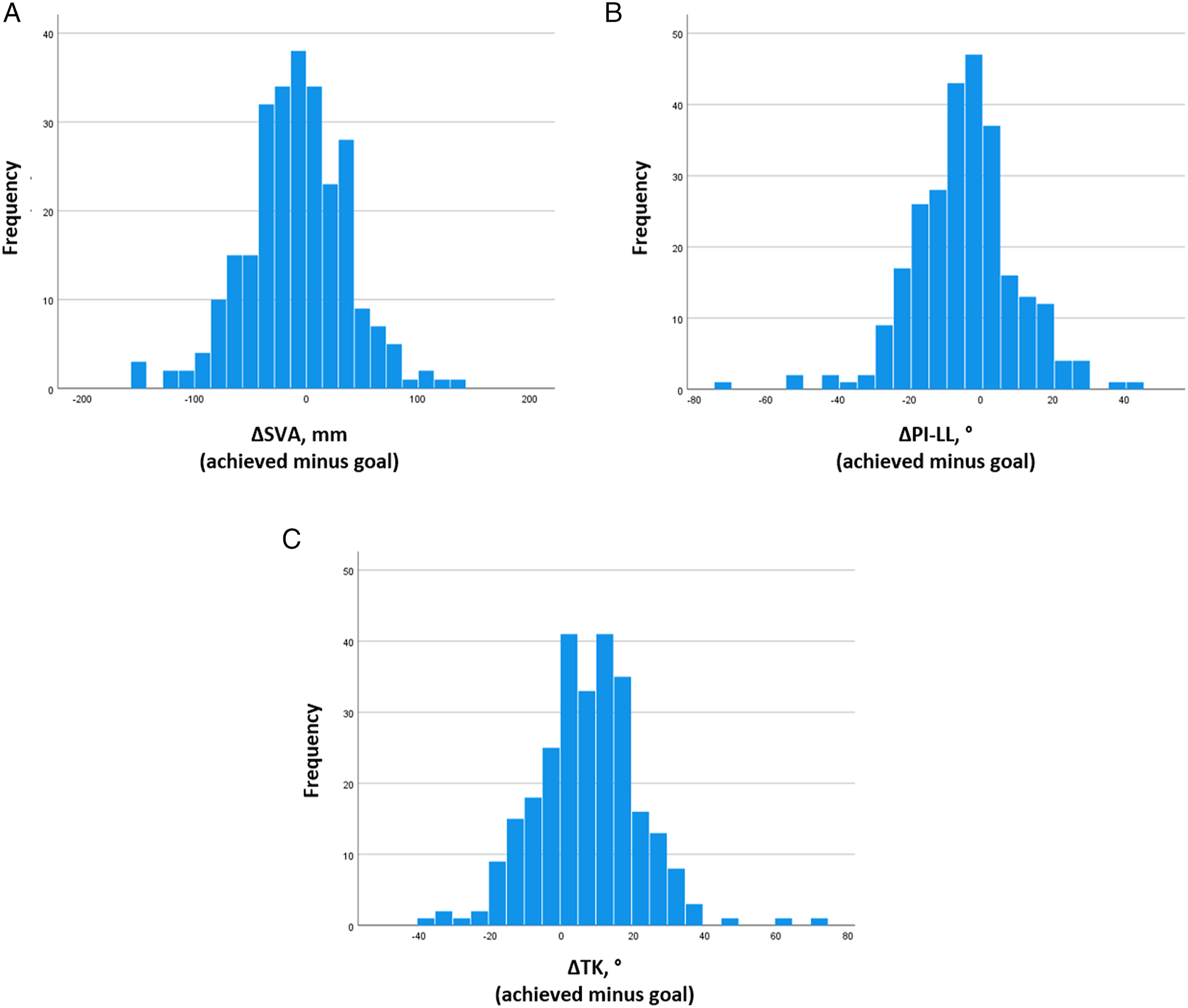
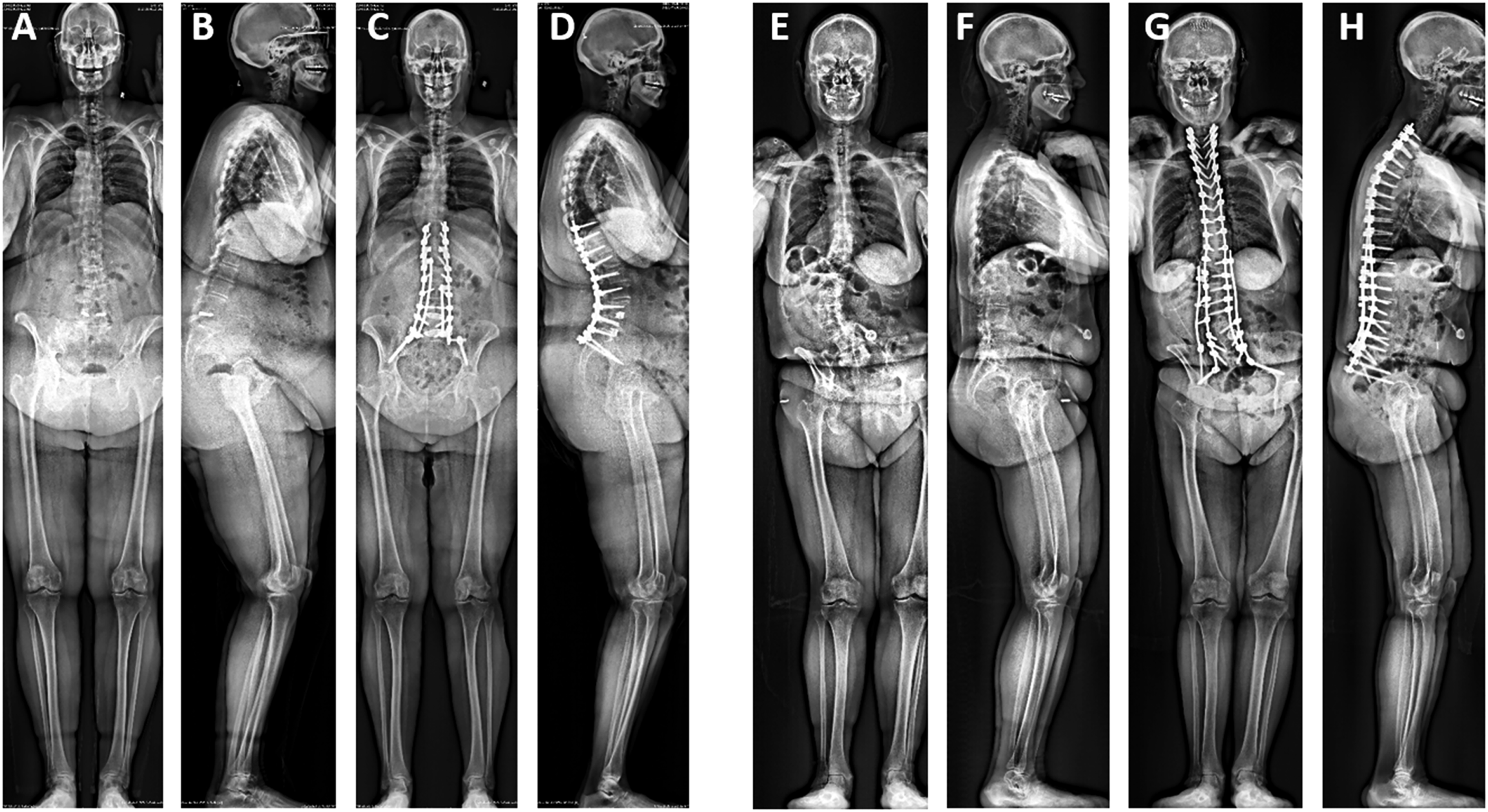
Weak to moderate correlations were observed between goal and achieved alignment for each of the parameters assessed (Figure 1). Histograms of the difference between achieved postoperative alignment and the respective surgeon’s preoperative goal alignment for SVA, PI-LL, and TK are shown in Figure 2. The mean offsets (achieved-goal) for each parameter were: SVA = -8.5 mm (SD = 45.6 mm), PI-LL = -4.6° (SD = 14.6°), and TK = 7.2° (SD = 14.7°). These SDs were used to establish windows for acceptable achievement of goal alignment. Thus, for a surgeon to have been considered to have achieved SVA goal alignment, the achieved SVA would have to be within ±45.6 mm of the goal. Similarly, for the PI-LL and TK measures, the achieved alignment would have to be within ±14.6° and ±14.7° of preoperative goal alignment, respectively. Based on these criteria, goal alignment for SVA, PI-LL, and TK was achieved in 74.4%, 71.4%, and 68.8% of patients, respectively. Goal alignment for all three parameters was achieved in 37.2% of patients. Two patient examples are shown in Figure 3, one with a patient for whom all 3 sagittal alignment goals were achieved and another for whom none of the 3 sagittal alignment goals were achieved. For each contributing surgeon, the rates of achieving goal alignment are summarized in Table 2. These rates significantly differed across surgeons for TK (P < .001) and for combined assessment of all 3 parameters (P = .018). Scatter plots of achieved vs goal sagittal alignment and baseline sagittal alignment vs difference between goal and achieved alignment for 266 adult spinal deformity patients treated surgically. Shown are plots for SVA (A), PI-LL (B), and TK (C). SVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis. Histograms summarizing the distribution of 266 patients treated surgically for adult spinal deformity based on difference between the surgeon’s preopertaive goals for sagittal alignment and the achieved postoperative alignment. Shown are plots for SVA (A), PI-LL (B), and TK (C). SVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis. Patient examples illustrating alignment goals. The first patient is a 66-year-old woman with global sagittal malalignment for whom all sagittal alignment goals were achieved. Shown are preoperative antero-posterior (AP, A) and lateral (B) and 6-week postoperative AP (C) and lateral (D) full-body radiographs. Preoperative alignment measures were: sagittal vertical axis (SVA) of 166 mm, pelvic incidence to lumbar lordosis mismatch (PI-LL) was 52°, and thoracic kyphosis (TK) was 9°. The surgeon’s alignment goals were: SVA = 45 mm, PI-LL = 10°, and TK = 50°. Alignment on imaging at 6-weeks following surgery was: SVA = 11 mm, PI-LL = -2°, and TK = 43°. The second patient is a 61-year-old woman with degenerative lumabr scoliosis for whom none of the sagittal alignment goals were achieved. Shown are preoperative AP (E) and lateral (F) and 6-week postoperative AP (G) and lateral (H) full-body radiographs. Preoperative alignment measures were: SVA = 52 mm, PI-LL = 41°, and TK = 20°. The surgeon’s alignment goals were: SVA = 40 mm, PI-LL = 20°, and TK = 40°. Alignment on imaging at 6-weeks following surgery was: SVA = 100 mm, PI-LL = 38°, and TK = 25°.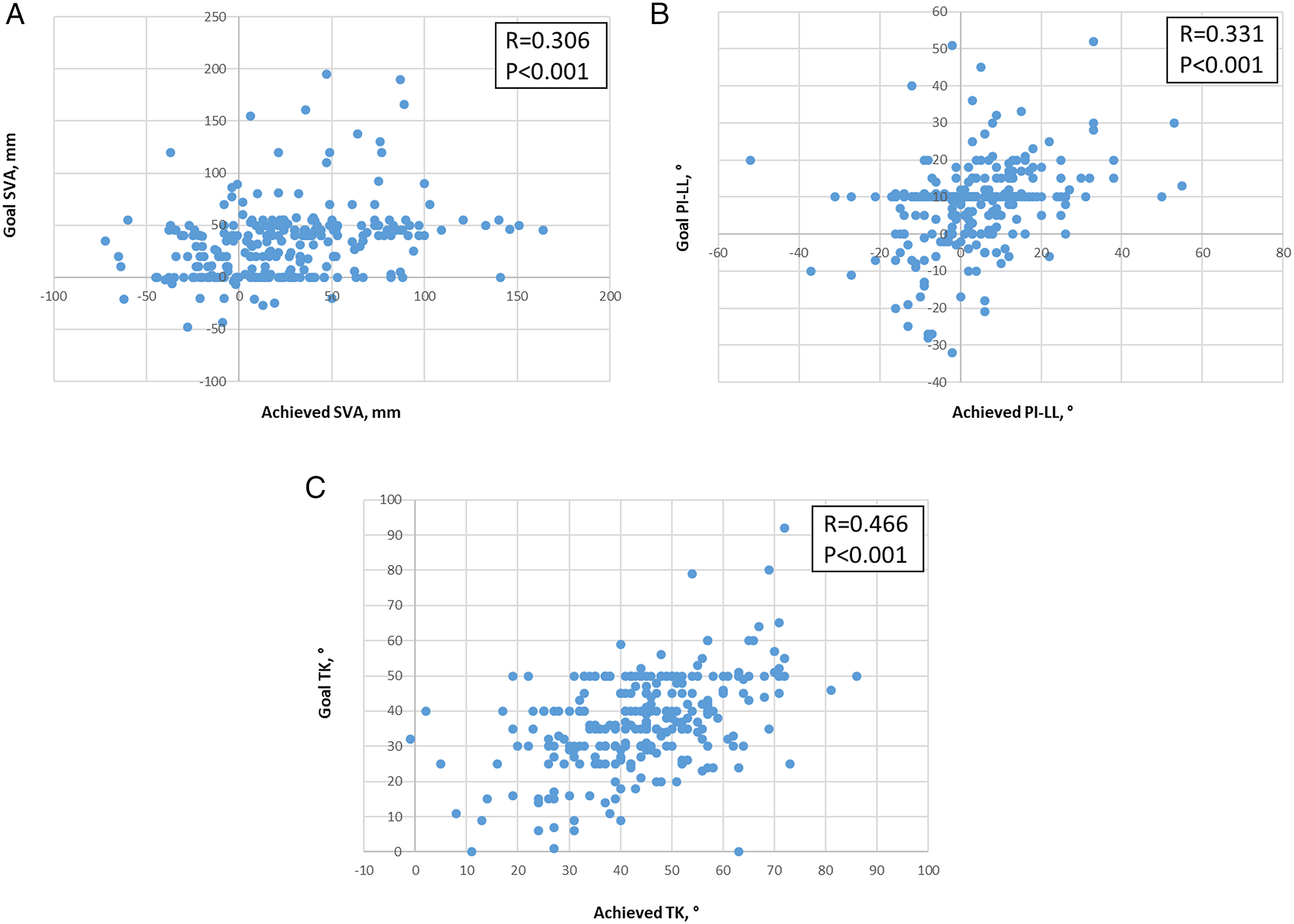
Factors Associated With Achievement of Sagittal Alignment Goals
Demographic/Clinical, Radiographioc, and Operative Parameters for 266 Adults With Spinal Defomity Stratified Based on Whether the Indiviudal Surgeon’s Sagittal Alignment Goals Were Achieved. a
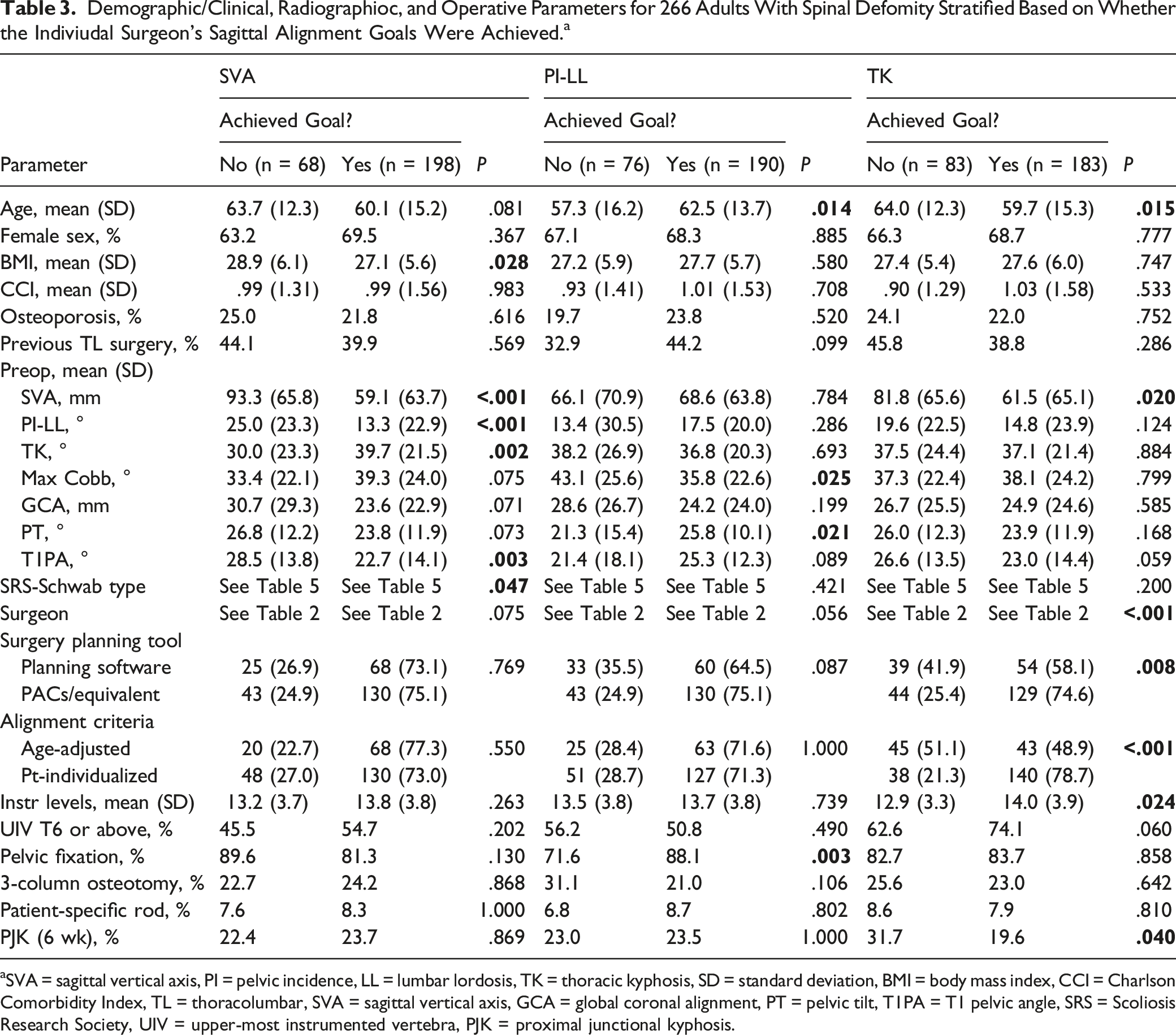
aSVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis, SD = standard deviation, BMI = body mass index, CCI = Charlson Comorbidity Index, TL = thoracolumbar, SVA = sagittal vertical axis, GCA = global coronal alignment, PT = pelvic tilt, T1PA = T1 pelvic angle, SRS = Scoliosis Research Society, UIV = upper-most instrumented vertebra, PJK = proximal junctional kyphosis.
Demographic/Clinical, Radiographioc, and Operative Parameters for 266 Adults with Spinal Defomity Stratified Based on Whether all Sagittal Alignment Goals of the Indiviudal Surgeon were Achieved. a
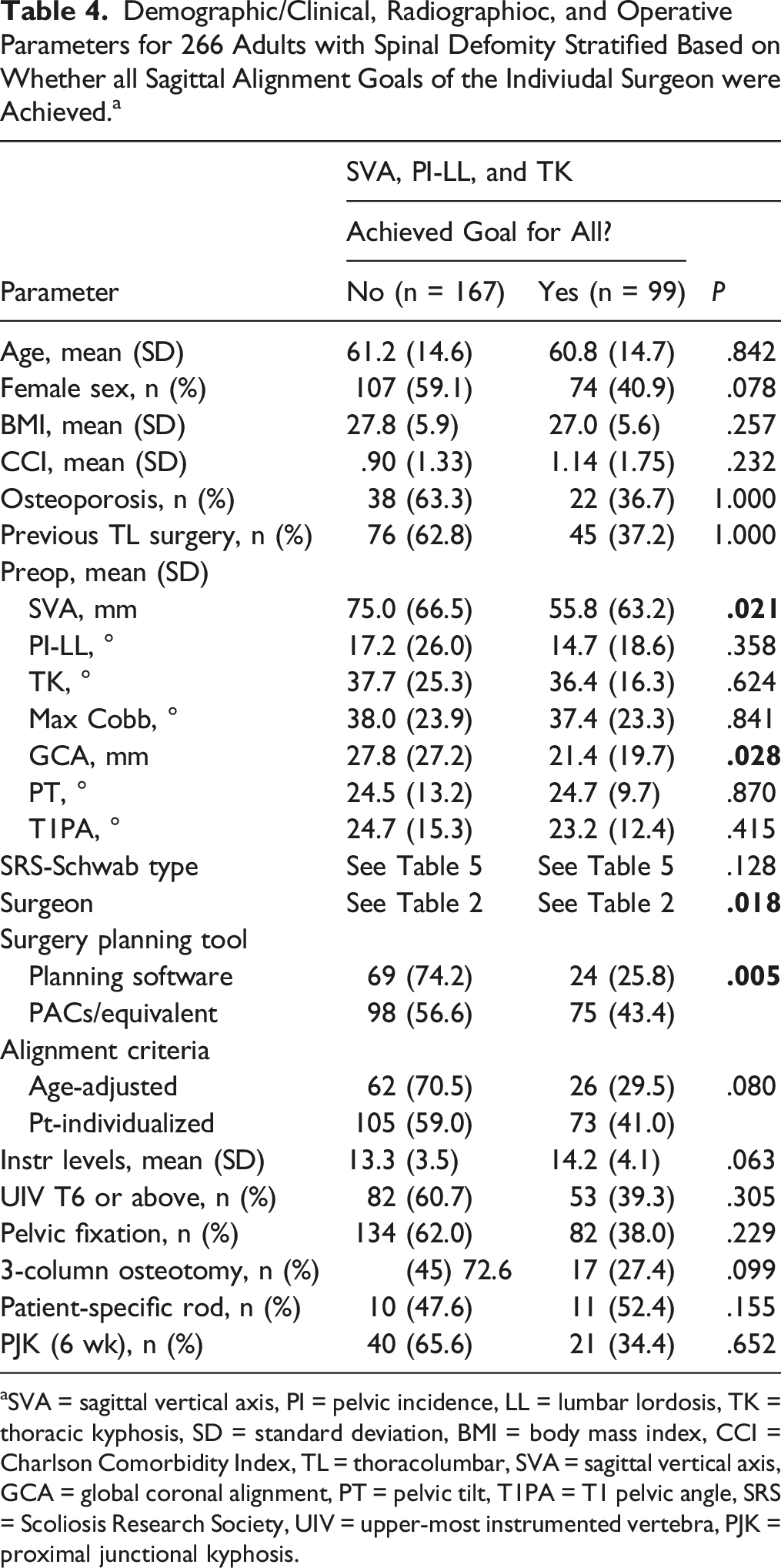
aSVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis, SD = standard deviation, BMI = body mass index, CCI = Charlson Comorbidity Index, TL = thoracolumbar, SVA = sagittal vertical axis, GCA = global coronal alignment, PT = pelvic tilt, T1PA = T1 pelvic angle, SRS = Scoliosis Research Society, UIV = upper-most instrumented vertebra, PJK = proximal junctional kyphosis.
SRS-Schwab curve types for 266 adults with spinal deformity stratified based on whether the indiviudal surgeon’s sagittal alignment goals were achieved. a
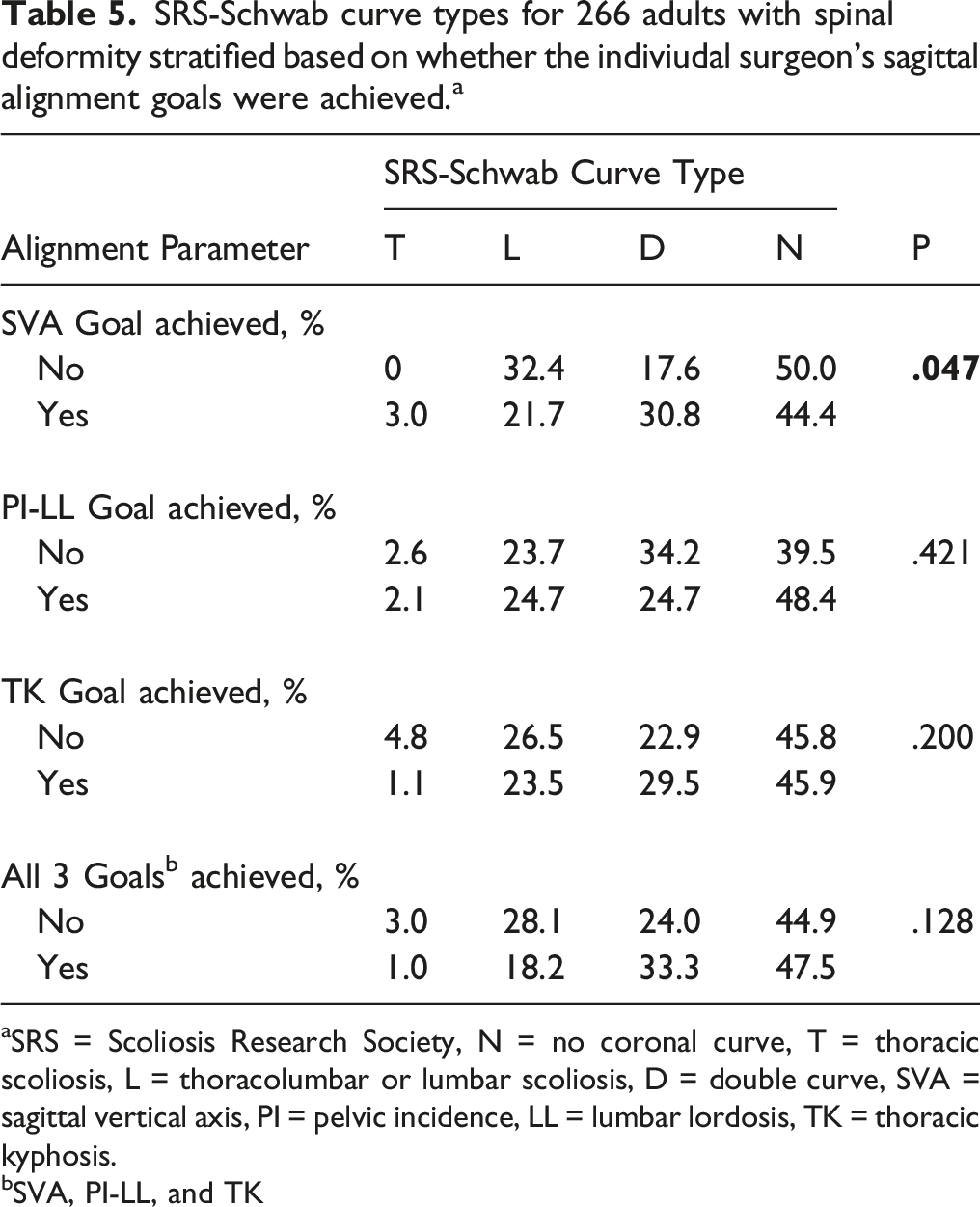
aSRS = Scoliosis Research Society, N = no coronal curve, T = thoracic scoliosis, L = thoracolumbar or lumbar scoliosis, D = double curve, SVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TK = thoracic kyphosis.
bSVA, PI-LL, and TK
Factors associated with a greater likelihood of achieving goal PI-LL mismatch included greater patient age (62.5 years vs 57.3 years, P = .014), lower baseline maximum coronal Cobb angle (35.8° vs 43.1°, P = .025), greater baseline PT (25.8° vs 21.3°, P = .021), and use of pelvic fixation (88.1% vs 71.6%, P = .003) (Table 4).
Achievement of goal TK was significantly associated with lower patient age (59.7 vs 64.0, P = .015), lower baseline SVA (61.5 mm vs 81.8 mm, P = .020), operating surgeon (P < .001), use of PACS/equivalent for surgical planning (P = .008), use of patient-individualized alignment goals (P < .001), greater number of instrumented vertebral levels (14.0 vs 12.9, P = .024), and lack of PJK on 6-week postoperative imaging (19.6% vs 31.7%, P = .040) (Table 4).
On univariate analysis, factors associated with successful achievement of all 3 assessed sagittal alignment goals (SVA, PI-LL, and TK) included lower baseline SVA (55.8 mm vs 75.0 mm, P = .021), lower GCA (21.4 mm vs 27.8 mm, P = .028), operating surgeon (P = .018), and use of PACS/equivalent for surgical planning (P = .005) (Table 4).
Multivariate Analysis of Factors Associated with Acheivement of Sagittal Alignments Goals Following Surgery for Adult Spinal Deformity. a
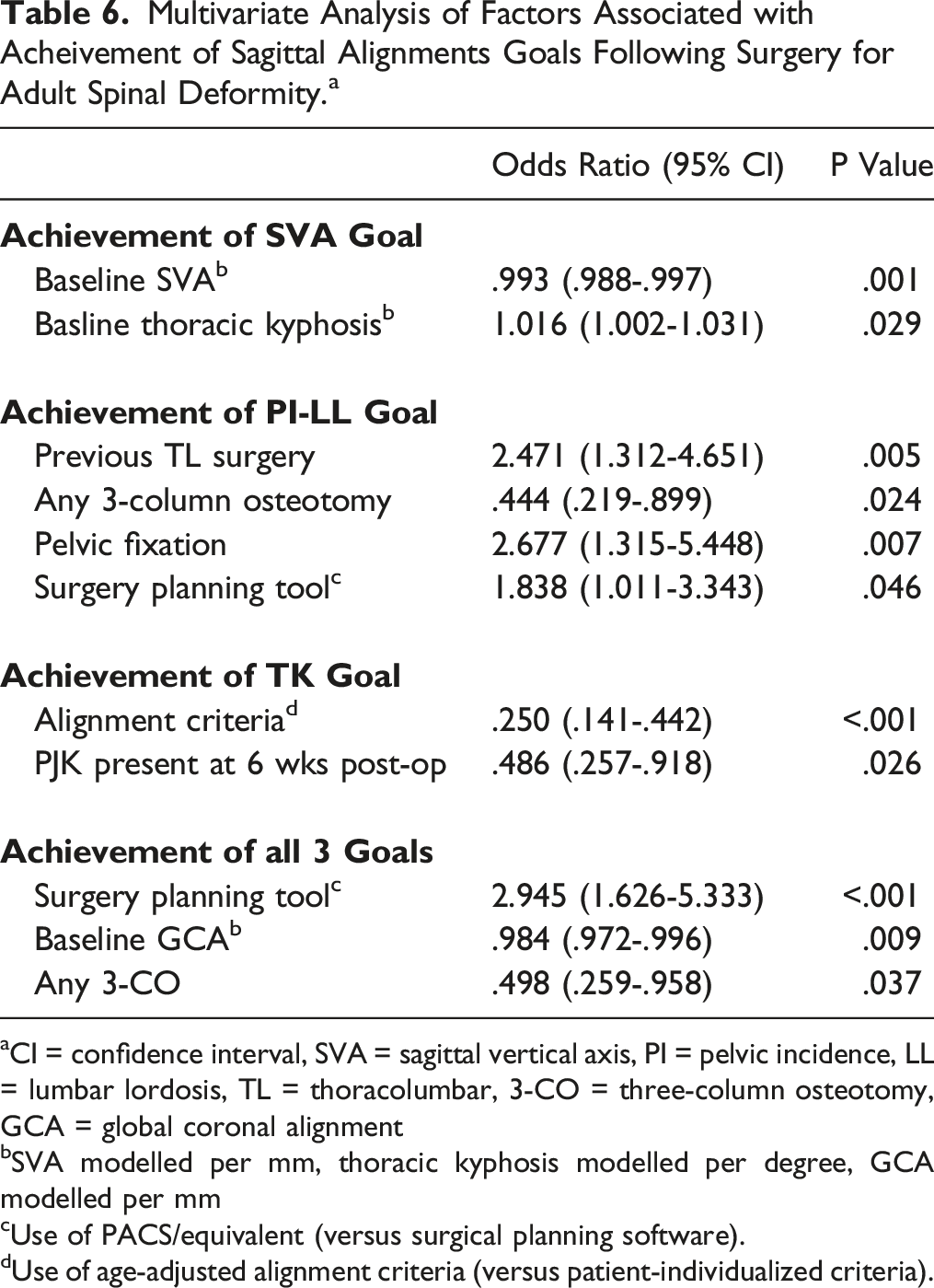
aCI = confidence interval, SVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis, TL = thoracolumbar, 3-CO = three-column osteotomy, GCA = global coronal alignment
bSVA modelled per mm, thoracic kyphosis modelled per degree, GCA modelled per mm
cUse of PACS/equivalent (versus surgical planning software).
dUse of age-adjusted alignment criteria (versus patient-individualized criteria).
Discussion
One of the primary goals of surgery to address ASD is to sufficiently correct spino-pelvic malalignment in order to improve HRQL, including pain and function, and to reduce the risks of mechanical complications, including instrumentation failure and PJK.17,19-25,38 Despite an ever-growing sophistication of surgical planning tools available to ASD surgeons, the present study demonstrates a significant gap in the ability of surgeons to translate these preoperative alignment goals to the operating room and ultimately achieve the goal alignment. Our analysis shows that surgeons failed to achieve goal alignment for each of the assessed sagittal parameters in ∼25-30% of operated ASD patients, and achieved goal alignment for all 3 sagittal parameters (SVA, PI-LL, and TK) in only 37.2% of operated ASD patients. The mean offsets (achieved minus goal) for all patients were −8.5 mm, −4.6°, and +7.2° for SVA, PI-LL, and TK, respectively, suggesting that surgeons had a tendency to undercorrect SVA and PI-LL and increase TK. Collectively, these findings highlight the need for further advances to enable more consistent translation of preoperative alignment goals to the operating room.
As a secondary objective, we aimed to explore whether specific clinical, radiographic, and operative factors could be associated with successful achievement of alignment goals. On multivariate analysis, a greater baseline SVA was independently associated with a lower likelihood of achieving goal SVA alignment following surgery, suggesting that the greater the severity of preoperative global sagittal deformity, the more challenging it was to achieve goal alignment. A greater baseline TK was also independently associated with increased likelihood of achieving goal SVA alignment. Although this may seem counterintuitive, it may reflect the complexities of thoracic compensation in the setting of global sagittal malalignment and the difficulties of predicting reciprocal changes in TK.22,39 The preoperative presence of low TK may or may not reflect compensation for global sagittal malalignment, and following surgical correction of sagittal malalignment, this low TK may persist or it may relax and increase the SVA. It is also possible that patients with a greater baseline TK were more likely to be fused to the upper thoracic spine and therefore the magnitude of the kyphosis was better controlled.
Four factors were independently associated with achievement of PI-LL goal alignment. Patients with previous thoracolumbar surgery were more likely to achieve goal PI-LL. This may be due to lumbar vertebral segments already being fused, which may facilitate a better estimate of final lumbar lordosis, barring extensive osteotomies to change the alignment. Similarly, patients with pelvic fixation were more likely to achieve goal PI-LL, and this may reflect a greater ability to control the final lumbar lordosis when instrumentation extends through the lumbar spine with sacro-pelvic fixation. Surgeons were less likely to achieve goal PI-LL alignment in cases in which a 3-CO was used. Deformities requiring a 3-CO are often those with the greatest PI-LL mismatch, and the marked release and powerful correction achieved through a 3-column release may introduce challenges in controlling the degree of LL correction achieved.40,41 Surgeons who used PACs/equivalent for surgical planning (versus commercially available spine-specific planning software) were more likely to achieve alignment goals. It may be that this approach produces better but more rigorous goals that are more challenging to achieve. Importantly, our findings do not suggest that surgeons should not use planning software.
Although several factors were associated with achievement of goal TK univariate analysis (Table 3), only two factors had independent association on multivariate analysis. Goal TK was significantly less likely to have been achieved if the patient developed early PJK. This may not be surprising and emphasizes the impact of this challenging complication. 42 Thoracic compensation and radiographic PJK are very common and often early occurrences following surgery for ASD and may be difficult to account for when planning goal alignment. Use of patient-individualized goals (versus age-adjusted alignment goals) was associated with greater likelihood of achieving goal TK. Notably, age-adjusted alignment goals do not specifically address TK,26,27 which may at least partially explain this association.
Factors independently associated with achievement of all 3 sagittal alignment goals were GCA, use of 3-CO, and surgical planning tools. Patients with more severe deformity at baseline, including global coronal malalignment (GCA) were less likely to achieve goal alignment for all 3 assessed parameters. This may simply reflect the greater challenges in releasing and correcting more severe deformities. Use of a 3-CO was also associated with a decreased likelihood of achieving all three alignment goals. Three-column osteotomies provide marked release of the spine and can enable a wide range of corrections, which may complicate the ability of the surgeon to achieve a specific planned realignment goal.41,43 Surgeons who used PACs/equivalent for surgical planning (versus commercially available spine-specific planning software) were more likely to achieve all 3 alignment goals. As noted previously, the reason for this association is not entirely clear but may reflect more aggressive realignment targets that could be more challenging to achieve when using spine-specific planning software.
Surgeons were required to provide specific alignment goals prior to surgery, but were allowed to be within a range of values in order to be classified as having successfully achieve the goal alignment. Since there are no such standardized ranges previously reported, we chose to use the standard deviation (±) of the offset (achieved minus goal) for each of the parameters across all patients in the study. This provided an arguably generous window for achievement of goal alignment. For the SVA, PI-LL, and TK, the windows were 9.1 cm, 29.2°, and 29.4°, respectively. Thus, the relatively low rates of achieving goal alignment, especially for all 3 parameters, cannot be attributed to overly rigid criteria for determining success.
Strengths of the present study include the prospective multicenter study design and relatively large number of patients. Limitations of the present study include the potential for selection, indication, and expertise bias to have influenced the results. Due to these limitations, it is possible that the findings may not be generalizable to all settings beyond the contributing centers. Patient-specific rods were used in only 21 patients, which limits the conclusions that can be drawn based on use of these implants. In addition, the surgical planning approach in the present study was based on usual care, 44 rather than standardizing the planning approach. Surgeons were allowed to choose whether to use specific software for surgical planning or to use commonly available generic imaging work stations. Surgeons were also allowed to choose how to determine the postoperative alignment goals, with some surgeons choosing to broadly apply standardized age-adjusted alignment goals, while others favored determination of goal alignment based on a patient-individualized approach. Although lack of a highly regimented approach to preoperative planning may be seen as a limitation, this strategy was intentionally chosen and is perceived as a strength, since this usual care approach provides a much better approximation of what actually occurs in practice, especially since the surgical planning approach is highly variable.
Conclusion
Surgeons failed to achieve goal alignment of each sagittal parameter in ∼25-30% of ASD pts, with tendencies to undercorrect SVA and PI-LL and increase TK. Goal alignment for all 3 parameters was only achieved in 37.2% of patients. Those at greatest risk were patients with more severe deformity and those requiring more aggressive osteotomies. Use of spine-specific surgical planning software and use of age-adjusted alignment goals were associated with lower likelihood of achieving alignment goals. Importantly, our findings do not suggest that surgeons should not use planning software or age-adjusted alignment criteria. It may be that these approaches produce better but more rigorous goals that are more challenging to achieve. Further advancements are needed to enable more consistent translation of preoperative alignment goals to the operating room.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: reports consultancy fees from ZimVie, NuVasive, Cerapedics, and Carlsmed; receives royalties from Zimmer Biomet and Nuvasive; holds stock in Alphatec and NuVasive; receives research funding to his institution from DePuy Synthes, International Spine Study Group Foundation (ISSGF), and AOSpine; receives fellowship grant funding to his institution from AOSpine; serves on the Executive Committee of the ISSGF; and serves on the editorial boards of Journal of Neurosurgery Spine, Neurosurgery, Operative Neurosurgery, and Spine Deformity. is a consultant for ISSGF. is a consultant for Globus Medical and Alphatec; receives royalties from NuVasive; receives research support from ISSG; receives honoraria from DePuy Synthes, Stryker, and Implanet; and has leadership roles in ISSG and the Scoliosis Research Society. is a consultant for DePuy Synthes, Stryker, and Medtronic, SI Bone, and Agnovos; receives honoraria and a fellowship grant paid to an institution from AO Spine; and has leadership roles with AOSpine. Dr. Kim receives royalties from Zimmer Biomet, Acuity Surgical, and K2M-Stryker; is a consultant for NuVasive; receives research support from the ISSGF; is on advisory boards for Vivex Biology and Aspen Medical; and has other financial or non-financial interests with AOSpine. is a consultant for Medtronic, SpineWave, Terumo, and Royal Biologics; receives honoraria from Cervical Spine Research Society, Globus Medical, and Zimmer; serves on the editorial or governing board for Spine journal; and receives research support from Allosource. receives research support from Stryker, Biom’Up, Pfizer, the Alan L. & Jacqueline B. Stuart Spine Center, National Health Foundation, Cerapedics, Empirical Spine, Inc., TSRH, and Scoliosis Research Society; receives royalties from Acuity, Medtronic, and NuVasive; is a consultant for Acuity, DePuy, Medtronic, NuVasive, FYR Medical, and Stryker; receives honoraria from Baxter, Broadwater, NASS, and Pacira Pharmaceuticals; holds patents with Medtronic; participates on a data safety monitoring board or advisory board with Medtronic; has a leadership role in the National Spine Health Foundation; owns stock/stock options in Cingulate Therapeutics and FYR Medical; is an employee of Norton Healthcare, Inc.; and serves as a journal reviewer for Global Spine Journal, Spine Deformity, and The Spine Journal. and receives research/fellowship support from NuVasive, Medtronic, SeaSpine, SI Bone, and AONA; receives royalties from SI Bone, Nuvasive, Seaspine, Aesculap, and Globus Medical; is a consultant for Aesculap, NuVasive, SI Bone, SeaSpine, Spinal Elements, Biedermann-Motech, Silony, Neo Medical, Depuy, Medtronic, Carevature, and ControlRad; has received payment/honoraria from Radius; has patents with Globus, Spine Innovation, and SI Bone; has leadership role with San Diego Spine Foundation; and has stock/stock options with Alphatec, Nuvasive, Seaspine, and SI Bone. receives grants/research support from Medtronic and Orthofix; receives royalties from Spineart and Stryker; is a consultant for Stryker Spine, Spineart, and Medtronic; and has received payment for expert testimony from multiple law firms. is a consultant for NuVasive, Viseon, Carlsmed, SI Bone, and SeaSpine; holds patents with Stryker, NuVasive, and SeaSpine; has leadership roles with Global Spine Outreach and San Diego Spine Foundation; has stock or stock options with Alphatec, SeaSpine, and NuVasive; and receives royalties from NuVasive and K2M/Stryker. is a consultant for Globus, NuVasive, and Medtronic; receives royalties from Altus; receives grants from Medtronic; and has stock or stock options from One Point Surgical. Dr. receives travel expenses to teach at the ISSG-Medtronic Spine Course for fellows and residents; and has a leadership role with the Canadian Spine Society. receives grants/research support from Prosydiuan and NuVasive. receives honoraria from Wolters Kluwer; received support for travel from AO Spine; has leadership roles with Scoliosis Research Society and AO Spine; and receives research support from the Setting Scoliosis Straight Foundation and San Diego Spine Foundation. is a consultant for Stryker Spine; receives grant/research support from Medtronic, DePuy Synthes, and AOSpine; receives honoraria from Medtronic, Stryker Spine, DePuy Synthes, Scoliosis Research Society, and AOSpine; receives support for travel from AO Spine and Scoliosis Research Society; and is on an advisory board/panel for AOSpine Research Commission and Scoliosis Research Society Research Task Force; and is Chair of the AO Spine Knowledge Forum Deformity. owns stock in J&J; is a consultant for DePuy, Medtronic, Globus; receives royalties from Innomed, DePuy, and Globus; receives honoraria from AO Spine, Wright State, and LSU; serves on the board of directors of the Scoliosis Research Society; receives travel reimbursements from DePuy, Globus, Scoliosis Research Society; and has a voluntary relationship with the National Spine Health Foundation. is a consultant for MSD, Zimmer Biomet, and Mainstay Medical; receives royalties from Zimmer Biomet, Medtronic, and Stryker; owns stock in VFT Solutions and SeaSpine; is an executive committee member of ISSG. receives royalties from DePuy Spine, Globus, and Blue Ocean Spine; is a consultant for DePuy Spine, Globus, and Blue Ocean Spine; has a leadership role in the Scoliosis Research Society and International Spine Study Group Foundation; has stock or stock options in Progenerative Medical; and has received research support from DePuy Spine and ISSGF. receives royalties from Stryker, Biomet Zimmer Spine, DePuy Synthes, NuVasive, Next Orthosurgical, K2M, and Medicrea; is a consultant for DePuy Synthes, Medtronic, Medicrea, K2M, Agada Medical, and Carlsmed; receives research support from Titan Spine, DePuy Synthes, and ISSG; serves on the editorial board of Operative Neurosurgery; receives grant funding from SRS; serves on the executive committee of ISSG; is the director of Global Spinal Analytics; and is the safety and value committee chair of SRS. is a consultant for Medtronic, ABRYX, and Acuity Surgical; receives research/grant support from AOSpine, Scoliosis Research Society, and Setting Scoliosis Straight Foundation; receives royalties from Medtronic and Acuity Surgical; and receives other financial support from Broadwater, AOSpine, and Scoliosis Research Society. is a consultant for NuVasive, SI Bone, and Proprio; owns stock in NuVasive; holds patents with NuVasive; receives fellowship funding from Globus, Medtronic, and NuVasive; and receives royalties from NuVasive, Medtronic, and SI Bone; has leadership roles with SRS and CSRS; and receives study-related clinical or research support from DePuy Synthes and ISSGF. is a consultant for Zimmer Biomet, NuVasive, Cerapedics, Carlsmed, SeaSpine, and DePuy Synthes; owns stock in Alphatec and NuVasive; receives study-related clinical or research support from DePuy Synthes and ISSGF; receives non–study-related clinical or research support from DePuy Synthes, ISSGF, and AO Spine; receives royalties from Zimmer Biomet and NuVasive; and receives fellowship support from AO Spine. is a consultant for Alphatec, Stryker, and MiRus; receives honoraria from Stryker; holds patents with Stryker; receives study-related clinical or research support from Medtronic, Globus, NuVasive, Stryker, Carlsmed, and SI Bone; receives non–study-related clinical or research support from DePuy Synthes; and receives royalties from Stryker and NuVasive. report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medtronic, Globus, Stryker, SI Bone, and Carlsmed.
Trial Registration
This study is registered through ClinicalTrials.gov (NCT04194138).