
Abstract
Study design
National cross-sectional study.
Objective
Thoracic kyphosis (TK) is related to sagittal parameters as pelvic tilt (PT), lumbar lordosis (LL) and pelvic incidence (PI). The equation TK = 2 (PT+LL–PI) was validated for adolescents. The purpose of this study was to investigate if this equation correctly predicts TK regardless of age.
Methods
Sagittal alignment parameters were assessed on full spine radiographs of 2599 individuals without spine pathology (1488 females, 1111 males). Calculated TK (CTK) = 2 (PT+LL–PI) and measured TK (MTK) were compared by calculating the gap and using a linear regression between both parameters. Subgroup analyses were performed for gender, age, TK groups (≤20°, 21°-40°, 41°-60°, >60°), and PI groups (<45°, 45°-60°, >60°).
Results
Average values in the total population were: MTK 45.0°, CTK 36.9°. Average TK gap was 8.1°, 5.2° in females (intercept 11.7, slope .61) and 11.9° in males (intercept 7.1, slope .58). The mean gap was 3.6° for 15-34 years, 5.7° under 15 years and it increased progressively after 35 years with a maximum of 19.9° over 80 years. The gap also increased with the amount of MTK: -3.5° for TK<20° up to 17.3° for TK >60°. Differences in gaps were minor between PI groups. The intercept was smallest and slopes >.6 for PI <45° and TK ≤20°.
Conclusion
The formula TK=2 (PT+LL-PI) yielded moderate accuracy for adolescents and young adults, but did not fit for over 35 years and under 15. The amount and variance in TK increased in elderly subjects, which made the formula less accurate.
Background
The range of physiologic thoracic kyphosis (TK) is very large and values can therefore vary from 10° to 55° in healthy subjects. 1 This reflects that individual TK is linked to the spinopelvic alignment type, which is related to pelvic incidence (PI). 2 Furthermore, TK might vary with age, gender, and ethnicity.3-6 Therefore, there is not one optimal TK value for all, but a specific value for each subject. 7 The most comprehensive way to measure TK is from the cervico-thoracic inflection point to the thoraco-lumbar inflection point, ie global TK (GTK).1,2,5-9 The latter is characterized by limit vertebrae, the number of vertebrae (NTV), and the position of the thoracic apex of kyphosis (TA), which is the mid-point of GTK. The horizontal line through the TA separates GTK into proximal TK (PTK) and distal TK (DTK).1,2,5-9 All these parameters are poorly investigated, and might vary according to the spinopelvic alignment type.2-6
Defining the accurate thoracic shape is crucial when planning surgical correction of spinal deformity 7 , as the surgical modifications of TK have a significant impact on non-instrumented levels.8-11 Postoperative hypo- or hyperkyphosis might increase the risk for proximal junctional kyphosis (PJK) and proximal junctional failure.10,11 The setting of thoracic rod curvature in patients operated on for hyperkyphosis, adolescent idiopathic scoliosis, and adult spinal deformity (ASD), might therefore be planned in accordance to spinopelvic alignment parameters.7,10-15 Thus, it is suitable to define target values for TK that fit with each patient’s sagittal alignment type, in order to bend the rods accordingly.7,13-18
The geometrical relationship between TK and spinopelvic parameters has been investigated using the formula TK=2 (PT+LL-PI). 18 Calculated TK (CTK) was deemed accurate for adolescents, assuming that PTK and DTK were similar in healthy young subjects. 18 However, TK increases with age3,4,19 and it remains unclear to what extent this formula might be applied to an elderly population when planning adult spinal deformity correction.
The study hypothesis is that the equation TK=2 (PT+LL-PI) may vary according to age and gender, as thoracic and spinopelvic alignment change over time.
The primary objective was to test the formula on a large multicenter cohort from children to elderly subjects without spinal pathology, with respect to gender, amount of TK, and PI. The secondary aims were to describe the distribution between PTK and DTK, the position of the TA, and the NTV.
Methods
Institutional review board approval (FC/2019-91) was obtained for this retrospective cross-sectional study on full spine radiographs that were prospectively collected in a national French spine registry involving 16 centers. Sagittal radiographs (EOS Imaging, Paris, France) performed from September 2019 to March 2020 were collected on 2599 individuals (1488 females, 1111 males) aged from 5 to 93 years. Radiographs were performed for minor limb length inequality below 2 cm, spondylolysis, scoliosis screening in children and adolescents with positive family history. In adults, radiographs of patients with mild or moderate common low back, neck or radicular pain were also included. Exclusion criteria were: spinal deformity (scoliosis >10°, Scheuermann’s kyphosis, thoracolumbar kyphosis, and spondylolisthesis higher than grade 1), traumatic or osteoporotic fractures, spinal tumors or metastases, spondylodiscitis, neuromuscular diseases, previous spine surgery (except microdiscectomy), and limb length inequality exceeding 2 cm. Intervertebral disc degeneration, facet joint osteoarthritis and degenerative spondylolisthesis did not represent exclusion criteria, as they belong to the normal aging process. Spino-pelvic parameters were automatically measured after manual identification of segmental anatomical landmarks on sagittal radiographs by a trained operator per center using KEOPS software (SMAIO, Lyon, France). Each reconstruction was then checked by an independent senior spine surgeon from another center to minimize inter-rater errors. This method has been described as reliable and superior to manual measurements.
20
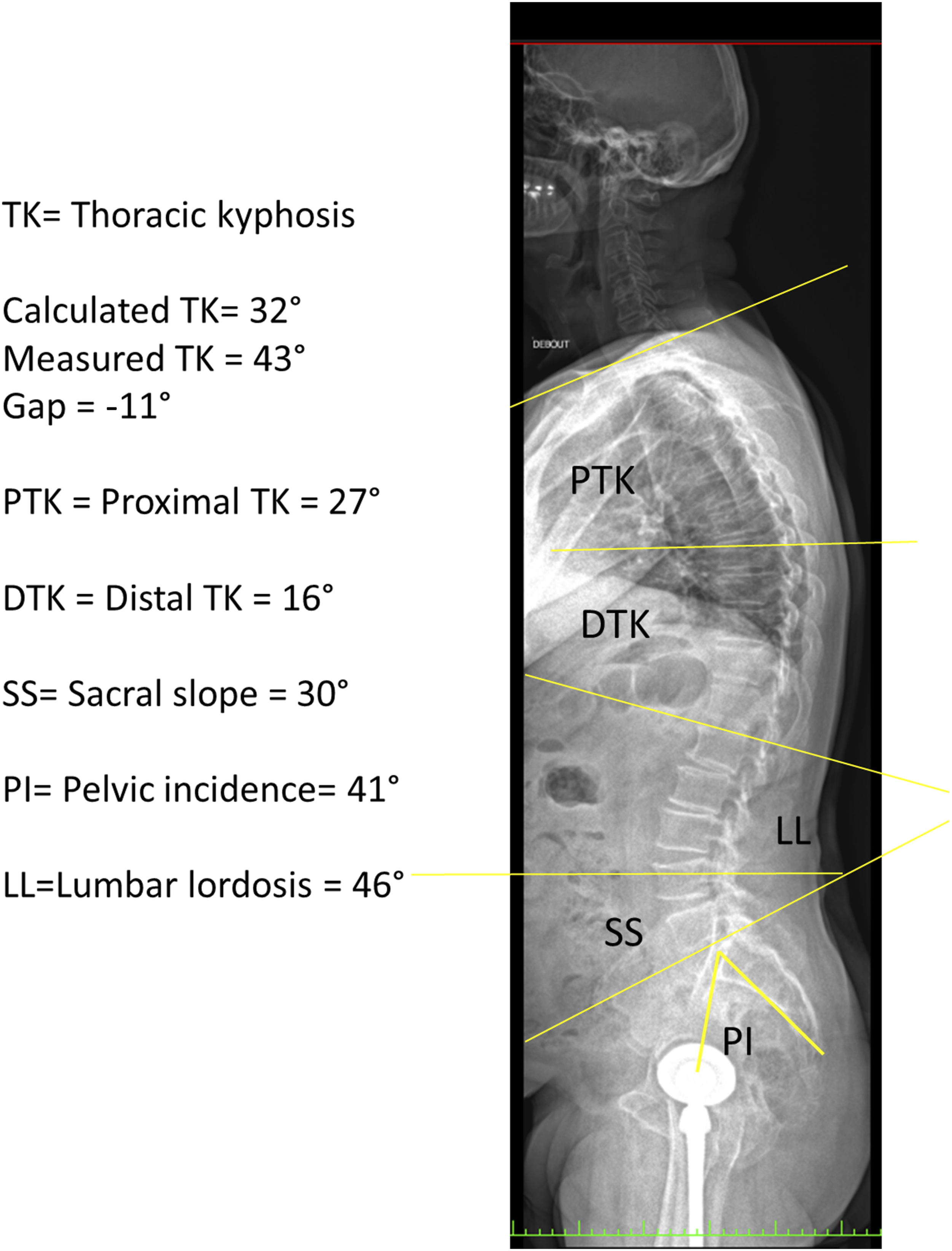
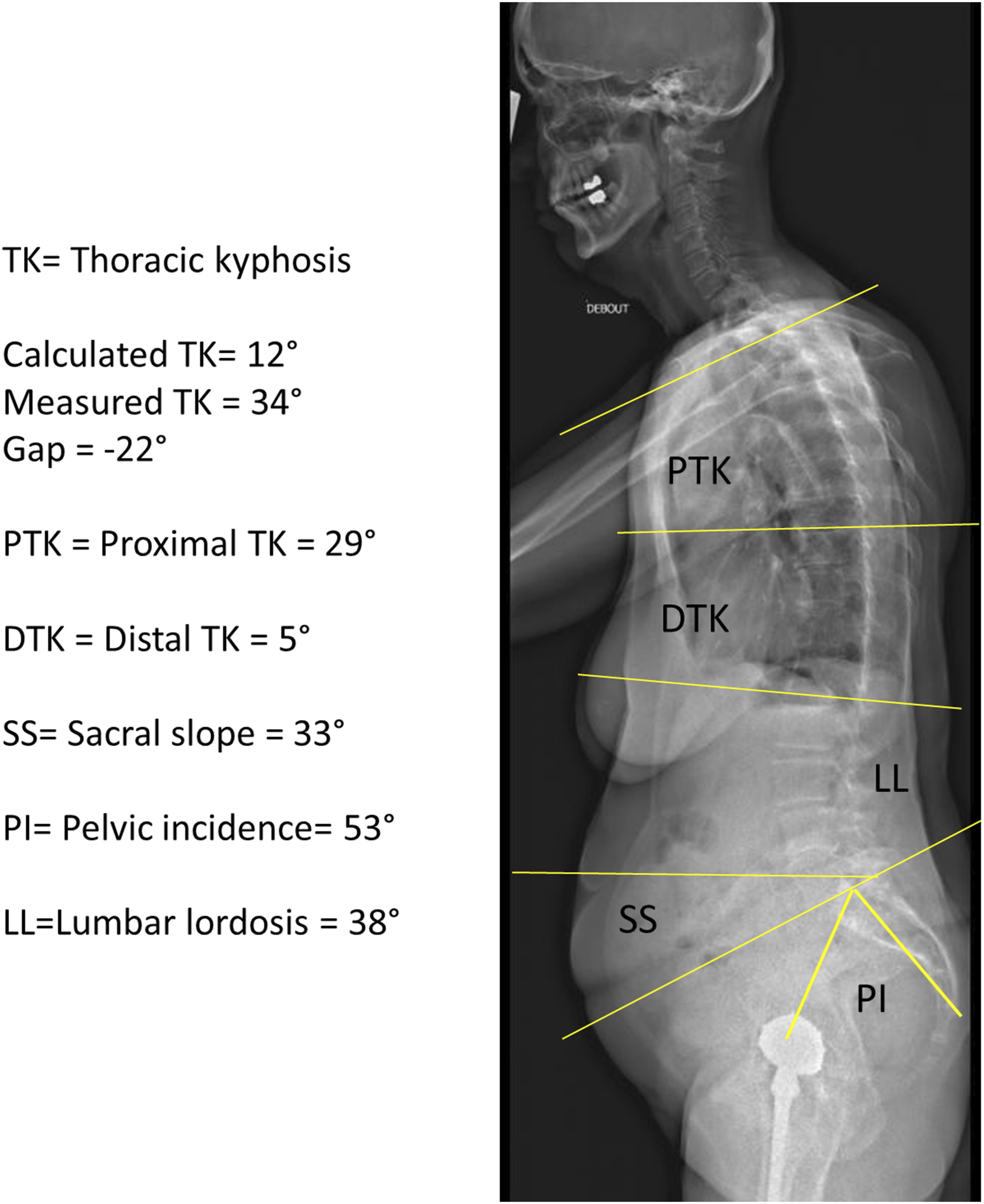
PI, PT, and sacral slope (SS) were assessed as usual (Figures 1-3).
2
GTK was measured between cervico-thoracic and thoraco-lumbar inflection points. PTK and DTK were assessed as previously described.2,8,9 Global LL was measured between the thoracolumbar inflection point and S1 endplate.2,8,9 Kyphosis was expressed as positive and lordosis as negative value. NTV and the TA were determined. Sagittal full spine radiograph, 22-year-old female. TK: Thoracic kyphosis. Calculated TK= 46°, Measured TK = 42°, Gap = 4°, PTK = Proximal thoracic kyphosis = 23°, DTK = Distal thoracic kyphosis = 19°, SS = Sacral slope = 42°, PI = Pelvic incidence= 46°, LL = Lumbar lordosis = 62°. Sagittal full spine radiograph, 70-year-old male. TK: Thoracic kyphosis. Calculated TK= 32°, Measured TK = 43°, Gap = −11°, PTK = Proximal thoracic kyphosis = 27°, DTK = Distal thoracic kyphosis = 16°, SS = Sacral slope = 30°, PI = Pelvic incidence = 41°, LL = Lumbar lordosis = 46°. Sagittal full spine radiograph, 81-year-old female. TK: Thoracic kyphosis. Calculated TK = 12°, Measured TK = 34°, Gap = −22°, PTK = Proximal thoracic kyphosis = 29°, DTK = Distal thoracic kyphosis = 5°, SS= Sacral slope = 33°, PI= Pelvic incidence= 53°, LL=Lumbar lordosis = 38°.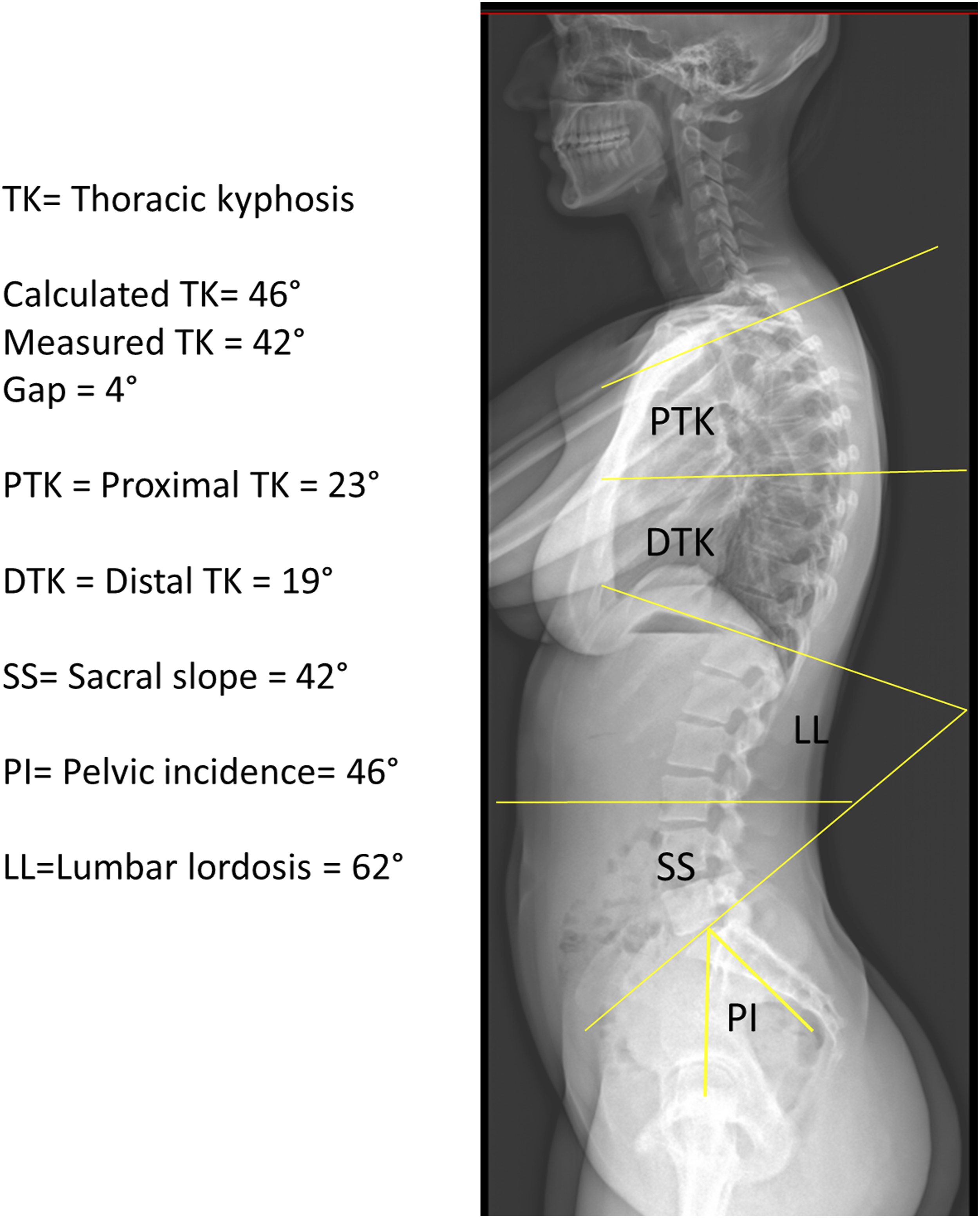
Statistical evaluation was performed with R Software Version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). Radiographic parameters were presented as mean values ± standard deviation. To test the hypothesis, CTK was calculated as follows: CTK = 2 (PT + LL - PI). Measured TK (MTK) and CTK were compared by calculating the difference as follows: TK gap = CTK - MTK. Subgroup analyses were performed for sex, age groups (5 to 9, 10 to 14, 15 to 19, 20 to 34, 35 to 49, 50 to 64, 65 to 79, over 80 years), TK groups (≤20°, 21°-40°, 41°-60°, >60°), and PI groups (<45°, 45°-60°, >60°). A linear regression was used to compare the distribution of MTK and CTK. Results of linear regressions were presented as intercept and slope according to the equation MTK = intercept + CTK slope. An intercept close to 0 and the slope close to 1 indicted a similar TK value distribution for MTK and CTK and optimal prediction by the formula. Conversely, the predictability of CTK decreased as the intercept increased and the slope decreased.
Results
Measured and calculated thoracic kyphosis
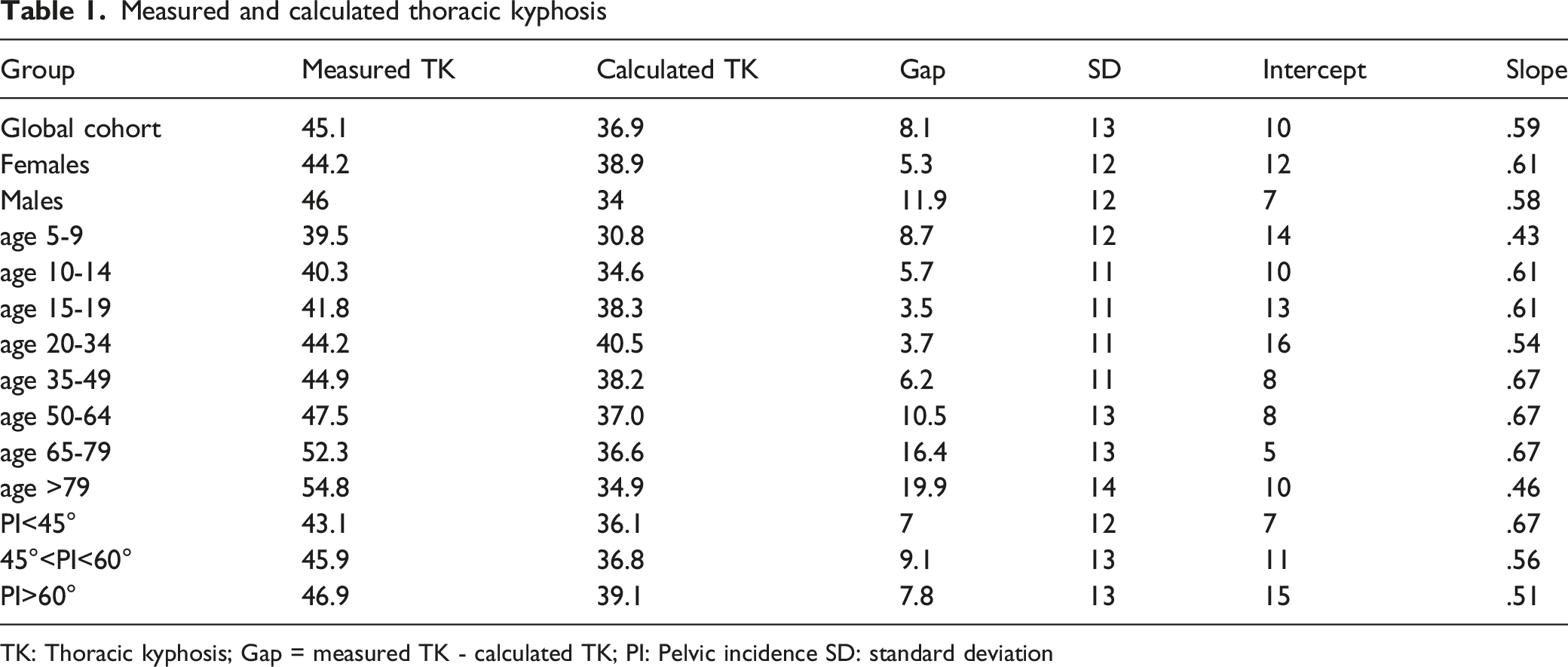
TK: Thoracic kyphosis; Gap = measured TK - calculated TK; PI: Pelvic incidence SD: standard deviation
When considering the formula, the mean TK gap was 8° in the global population with respective values of 5° (intercept 11.5, slope .62) for females and 12° (intercept 7.0, slope .59) for males.
The smallest TK gaps were measured in the age groups 15-19 years (3°) and 20-34 years (4°). Under the age 15 years, the mean gap was 6°. The gap progressively increased after the age of 35 years and it reached a maximum of 20° after 80 years (Table 1).
Consistently, the intercept was highest in children younger than 10 years and elderly subjects over 80 years with a slope <.5. Moreover, the gap increased with the amount of MTK: -3.5° for MTK<20° to 17.3° for MTK >60°. On the other hand, differences in gaps were minor between PI groups. The intercept was smallest and slopes >.6 for PI <45°, and MTK ≤20° (Table 1). Representative cases are shown in Figures 1-3.
Thoracic apical vertebra: count and % per group
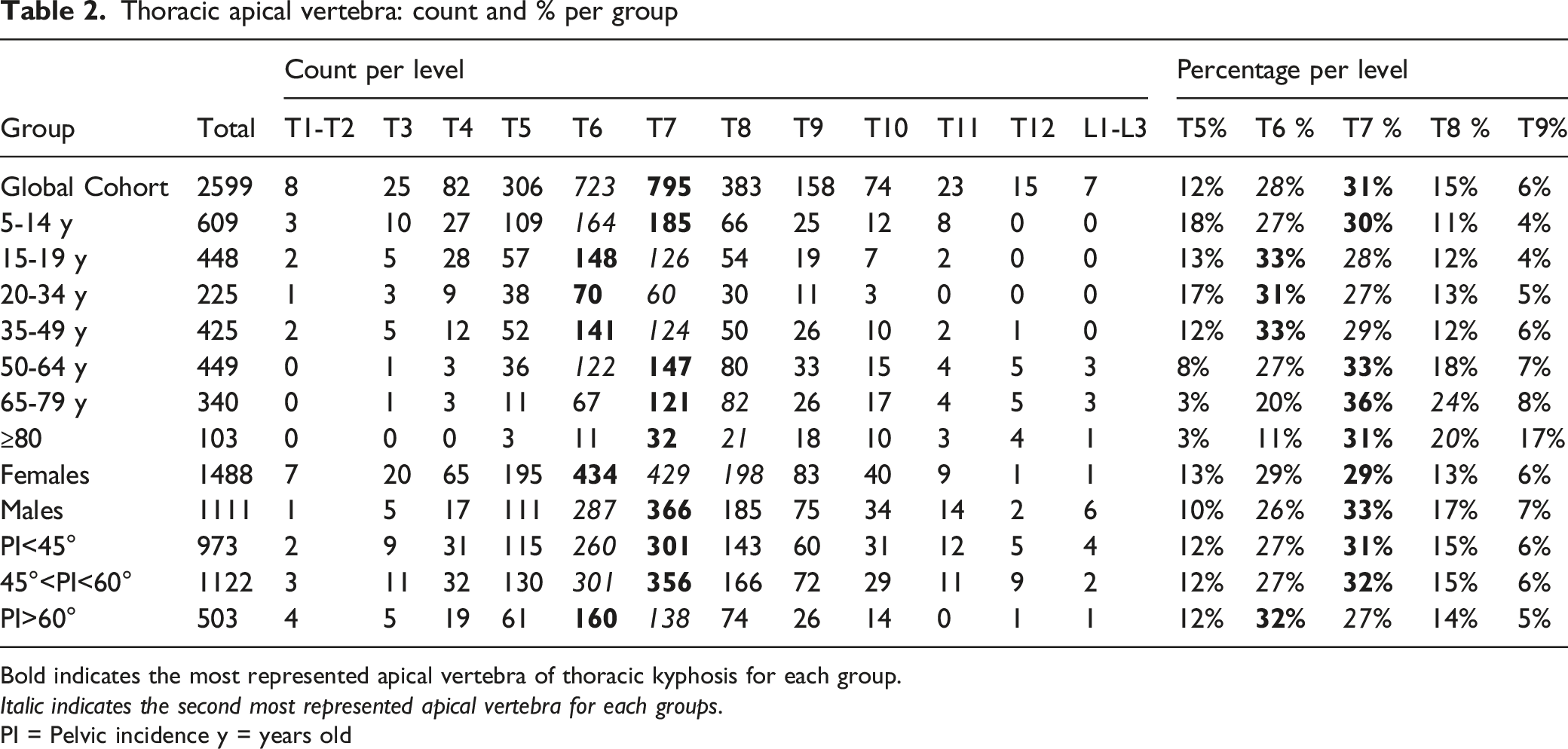
Bold indicates the most represented apical vertebra of thoracic kyphosis for each group.
Italic indicates the second most represented apical vertebra for each groups.
PI = Pelvic incidence y = years old
Number of vertebrae of global thoracic kyphosis
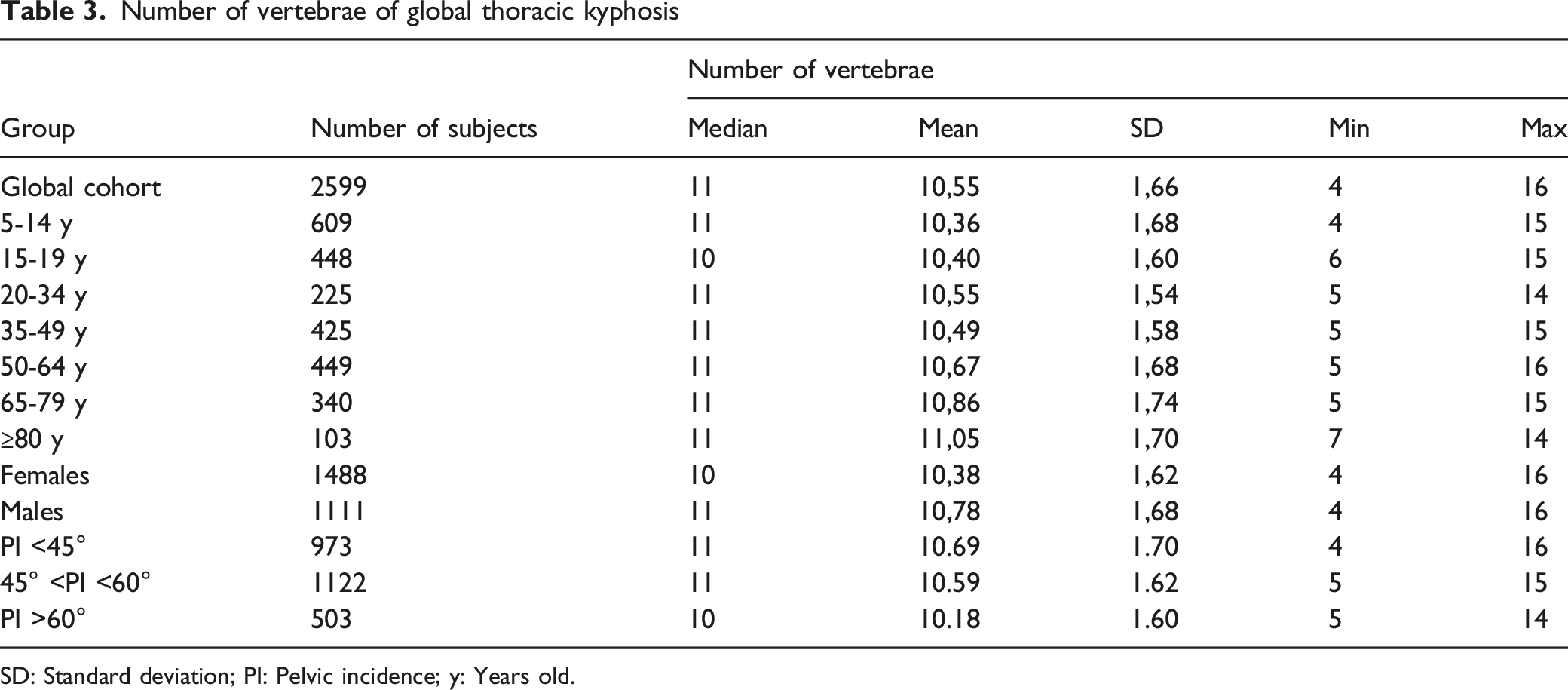
SD: Standard deviation; PI: Pelvic incidence; y: Years old.
Discussion
Our results suggest a moderate relationship between lumbo-pelvic and thoracic alignment in healthy subjects between 15 and 34 years. This finding confirms the previous study by Clément et al on 100 adolescents. 18 However, the predictions obtained from the current study using the formula TK=2 (PT+LL-PI) seem to be less accurate than that found by Clément et al, despite a larger series. Therefore, TK needs to be individually assessed while adjusting on age and PI. Nevertheless, for lack of a more precise indication, the formula TK=2 (PT+LL-PI) can be used to calculate the target TK in thoracic spinal deformity surgery of adolescents and young adults with an acceptable margin of error (average <4°), especially for patients with low pelvic incidence. On the opposite, the formula is less accurate in adults between 35 and 49 years with a mean error of 6°, and not applicable above 50 years, due to increase of TK with aging. Other parameters of the equation also vary over age: LL decreases and PT increases as degenerative changes occur in the lumbar spine, whereas PI also tends to increase in the elderly.21-23 This reflects the typical modifications of sagittal parameters with age, as previously described.19,21-25
In a cohort of Japanese adults, average values of sagittal alignment parameters 24 were: 50° ± 11 for LL, 54° ± 11 for PI, 14° ± 8 for PT, and 39° ± 8 for SS. Our results were similar for SS, PI, PT, LL, whereas TK was higher in our cohort (45°±13 vs 36° ± 10). Furthermore, we found the most important increase of TK with aging in its proximal component (PTK) [25]. This asymmetric increase between PTK and DTK is poorly described in literature. Moreover, a higher PTK than DTK was observed in most cases and is therefore suggested when planning a thoracic spinal surgery. This is consistent with the previous study by Seebaly et al on a cohort of young asymptomatic adults 13 , who found mean DTK of 20° (18° in our series) while the mean PTK was of 26° (27° in ours series) with 6° of mean difference (9° in our series). When comparing our results with those described by Stagnara 26 (TK=37°) and Gelb 27 (TK=34°), we found a higher TK, which is probably related to different method of measurement: GTK in our study, whereas it was T4-T12 or T5-T12 TK in others. Conversely, our TK value was similar to that from the study of Jackson, who measured GTK as well. 28 LL was higher than that from Stagnara (mean 50°) 26 but lower than reported by Jackson (mean 61°) 28 and Gelb (mean 64°), 27 which probably reflects ethnic variance.
Concerning pediatric subjects, the values of TK in the current cohort were globally lower than those of Cil et al 29 in a cohort from Turkey, but higher than those found by Boseker et al in the USA (average TK of 33°). 30 However, we observed a similar progression of TK from young children to skeletally mature adolescents as that reported by Cil et al (39° to 42° from our results, 45° up to 53° from Cil et al). 29 On the opposite, Boseker et al reported similar TK across ages in pediatric subjects. 30
The results from this study show slight differences between males and females, which is consistent with previous literature presenting contrasting influence of gender on TK. Indeed, some studies highlight a significant difference.3,24
Concerning the position of the TA, the current data are in contrast with those of Sebaaly et al, 13 who reported an average TA at T8 for mild PI and T9 for high PI. Other authors described TA at T7 as theoretical midpoint of the thoracic spine.18,31 The ideal TA position for each subject is still unknown, but the present results suggest that it is mostly located at T6 (especially for high PI subjects) and T7, sometimes at T5 or T8, whereas other locations remain rare. This is consistent with the findings of Pan et al 31 in Chinese adults, who found TA located at T7 ± 2 levels. Moreover, the level of TA tended to be more caudal in elderly subjects. Conversely, in children, the TA moved cranially with age, and was mostly located at T7 or T8. Additionally, aging can significantly affect the position of TA also during childhood.22,29 However, all studies reported a wide range of “physiological” TA.27,28 Therefore, it seems inappropriate to plan the same TA for all subjects during thoracic spinal surgery. However, it seems reasonable to avoid stopping a thoracic construct between T5 and T8 to decrease the risk of PJK. Unfortunately, our results do not allow better defining the ideal position of the upper instrumented level for hyperkyphosis or ASD correction.
Concerning the NTV, it was mostly between 10 and 11 from the current series, with slight increase across age groups.1,4 Moreover, a higher NTV was observed in low-incidence subjects and males, which is consistent with previous literature about spinopelvic alignment type 1 according to Roussouly et al.5,6
Strengths of this study include multicenter inclusions of a large number of subjects from a national registry. The main limitation of this study concerns its cross-sectional design, which implies an instantaneous picture of subjects without longitudinal assessment over a lifetime per subject. In addition, quality of life was not assessed, although various symptoms such as low-back or radicular pain could influence radiographic alignment. Indeed, many of our subjects were not healthy volunteers, but mostly patients with mild symptoms. Furthermore, anthropometric factors such as height, weight or ethnic origin were not considered, although they could influence sagittal alignment parameters.3,21 Moreover, the degenerative changes are an intrinsic phenomenon of aging and can influence sagittal alignment.22,23 Although severe degenerative changes leading to thoracolumbar deformity were excluded, it was arduous to define the exact threshold between the physiologic degenerative changes related to aging in the elderly and slight malalignment.
Conclusion
The formula TK=2 (PT+LL-PI) yielded moderate accuracy for healthy adolescents and young adults, but it did not fit for an adult population over 35 years and young children. The amount and variance in TK increased in elderly subjects, which made the formula less accurate. TK is not predictable from spinopelvic parameters above 50 years, since TK, PT and PI increase and LL decreases with age.
The TA was most frequently at T6 or T7, with low variations across age groups. The NTV was mostly between 10 and 11, with slight increase over age.
Footnotes
Acknowledgements
The authors thank Philippe Roussouly for technical support with the online database, and Dr Jean-Luc Clément for the primary scientific question. One of the authors (FS) performed this study in the framework of the International PhD in Innovation Sciences and Technologies, University of Cagliari, Italy.
Disclosures
Federico Solla received funding to attend meetings from Medicrea-Medtronic, Euros and Zimmer, and is a member of editorial board of BMC Musculosk Dis. Yann Philippe Charles is consultant for Stryker, Clariance, SpineVision, Philips and Ceraver; he received royalties and grants unrelated to this study from Stryker and Clariance. Vincent Lamas has no conflict of interest. Brice Ilharreborde is consultant for Zimmer Biomet, Medtronic and Implanet. Benjamin Blondel is associate editor for OTSR Elsevier-Masson and consultant for Medicrea, Medtronic, Implanet, Vexim Stryker and 3M. Solène Prost has no conflict of interest. Eloïse Bauduin has no conflict of interest. Féthi Laouissat is consultant for Spineart and SMAIO. Guillaume Riouallon is consultant for Medtronic, Stryker and NewClip; he received royalties from Euros. Stéphane Wolff has no conflict of interest. Vincent Challier is shareholder of Follow Health SA and consultant for Clariance. Ibrahim Obeid is consultant for Medtronic and Depuy Synthes; he received grants from DePuy Synthes unrelated to this study and royalties from Clariance, Alphatec and Spineart. Louis Boissière is consultant for Neo and Euros; he received grants from DePuy Synthes unrelated to this study. Emmanuelle Ferrero has no conflict of interest. Jean-Charles Le Huec is consultant for Medtronic and BD Bard; he received royalties and grants unrelated to this study from Medtronic. Stéphane Bourret has no conflict of interest. Joe Faddoul has no conflict of interest. Georges Naïm Abi Lahoud has no conflict of interest. Vincent Fière is consultant for Clariance; he received royalties from Medicrea and Clariance. Michiel Vande Kerckhove has no conflict of interest. Jonathan Lebhar has no conflict of interest. Hadrien Giorgi has no conflict of interest. Aymeric Faure has no conflict of interest. Erik André Sauleau has no conflict of interest. Sébastien Pesenti has no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.