
Abstract
Study design
Retrospective cohort study.
Objective
To identify risk factors and predictive models for proximal junctional kyphosis (PJK) in a long-term follow-up of patients with adult degenerative scoliosis (ADS) following posterior corrective surgeries.
Materials and Methods
A consecutive 113 ADS patients undergoing posterior corrective surgery between January 2008 and April 2019 with minimum 2-year follow-up were included. All patients underwent preoperative, postoperative, and final follow-up by X-ray imaging. Multivariate logistic analysis was performed on various risk factors and radiological predictor models.
Results
PJK was identified radiographically in 46.9% of patients. Potential risk factors for PJK included postoperative thoracic kyphosis (TK) (P < .05), final follow-up Pelvic Tilt (PT) (P < .05), PT changes at final follow-up (P < .05), age over 55 years old at the surgery (P < .05), theoretical thoracic kyphosis–actual thoracic kyphosis mismatch (TK mismatch) (P < .05) and theoretical lumbar lordosis–acutal lumbar lordosis mismatch (LL mismatch) (P < .05). As for the predictive models, PJK was predictive by the following indicators: preoperative global sagittal alignment ≥45° (Model 1), postoperative pelvic incidence–lumbar lordosis mismatch (PI–LL)≤10° and postoperative PI–LL overcorrection (Model 2), and TK+LL≥0° (Model 3) (P < .05). Postoperative TK mismatch (OR = 1.064) was independent as risk factors for PJK, with the cut-off values respectively set at −28.56° to predict occurrence of PJK.
Conclusion
The risk of radiographic PJK increases with an age over 55 years old and higher postoperative TK. In addition, postoperative TK mismatch is an independent risk factor for developing PJK. All three predictive models could effectively indicate the occurrence of PJK.
Keywords
Introduction
Adult degenerative scoliosis (ADS) refers to a spectrum of disabling curves that results in sagittal imbalance and occurs specifically after skeletal maturity. 1 The main pathogenesis of ADS is the degeneration of the intervertebral discs and facet joints. On top of compromising patient’s life quality, ADS inflicts a significant health burden on elderly patients in current aging society and has become a focus of clinical concern. 2 For patients with severe ADS, optimal surgical correction is essential in improving clinical outcomes and preventing sagittal decompensation.
Proximal junctional kyphosis (PJK) is a common complication after posterior instrumentation corrective surgery for ADS correction. The proximal junction is between the caudal endplate of the upper instrumented vertebra (UIV) and the cephalad endplate of the vertebra that is two levels above the UIV. 3 Lowe et al defined PJK as proximal junctional sagittal Cobb angle >10° and at least 10° greater than the preoperative measurement.4,5 According to previous literatures, the radiological incidence of PJK is varied and ranges from 6% to 50%.6,7
Varied risk factors have been considered to be associated with the occurrence of PJK, including age at surgery >55 years, low bone mineral density, obesity, preoperative comorbidities, fusion to sacrum, high preoperative lumbar lordosis (LL), and thoracic kyphosis (TK). 6 The Scoliosis Research Society (SRS) Schwab classification also proposed that coronal curve types and spinopelvic modifiers (SVA, PT, PI–LL) contributed to a strong correlation with postoperative prognosis in ADS patients, including the occurrence of PJK. 8 Besides, several radiological predictive models for PJK have been found in previous studies, including global sagittal alignment (GSA), TK+LL, and pelvic incidence—lumbar lordosis (PI–LL).9-11
However, to the best of our knowledge, the risk factors and predictive radiographical models of PJK are still yet to be defined, when one takes in to account the patient, radiographical, and surgical factors together. The present study was thus designed to identify risk factors associated with development of PJK and to evaluate three proposed predictive models for PJK. Based on our findings, we aimed to further provide clinical recommendations on current operational strategy for preventing PJK.
Materials and Methods
The present study was approved by the Institutional review board of the authors’ affiliated institution (IRB number: M2021239). A retrospective review of the medical records and radiographs was conducted for 113 ADS patients from a single institution. All patients received posterior corrective surgeries performed by the senior author between 2008 and 2019. Patients were eligible for inclusion if they (a) were diagnosed with ADS; (b) were treated with posterior corrective surgery; (c) were at least 50 years old; (d) completed radiographical follow-up at a minimum of three time points (preoperatively, immediately after the operation, and at the last follow-up). Patients with less than 2-years follow-up and incomplete radiographical records were excluded from the study.
Data Collection and Radiographic Measurements
We reviewed patient charts and radiographs, and recorded the following demographic and clinical data for each patient: age, sex, and body mass index (BMI). Surgical data such as surgical approach and UIV were also recorded. Preoperative, postoperative, and final follow-up full-length standing spine radiographs were measured and evaluated by a single observer. Spinal measurements were performed through the Picture Archiving and Communication System. They included sagittal vertical axis (SVA), sacral slope (SS), lumbar lordosis (LL), thoracic kyphosis (TK), pelvic incidence (PI), and pelvic tilt (PT). Theoretical values of TK and LL were calculated according to the formulas proposed by Sebaaly et al: LL = .67PI+23.7 and TK = .15PI+43 11 . In addition, we calculated the mismatch values of theoretical TK and LL minus their actual values. Coronal Cobb angles were also measured.
We focused on 3 predictive models which combined both spinal and pelvic parameters to assess sagittal alignment. The predictive models were defined and calculated respectively:
Model 1: GSA was calculated as a predictor. Normal GSA was defined as less TK+PI+LL than 45°, as suggested by the study of Rose et al. 12
Ideal age-specific alignment criteria for PI–LL.
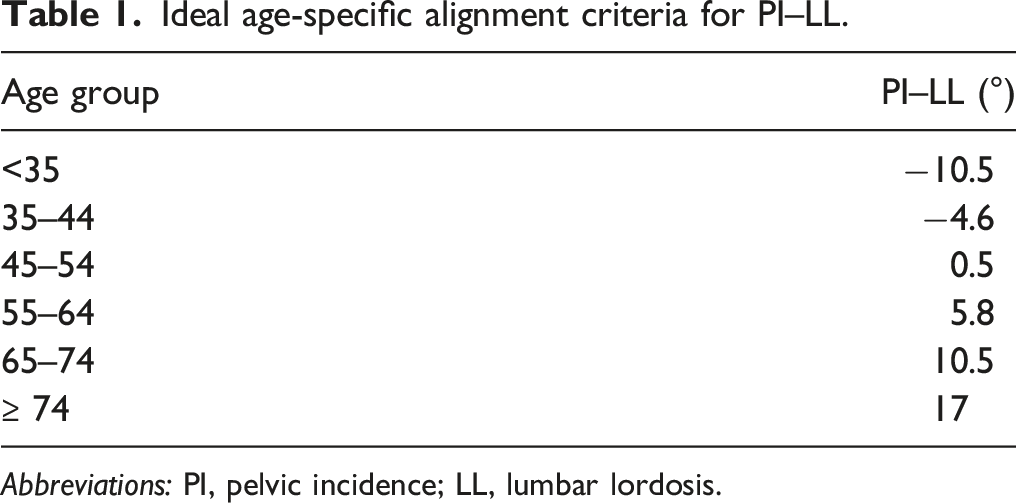
Abbreviations: PI, pelvic incidence; LL, lumbar lordosis.
Model 3: the predictor was the sum of thoracic kyphosis and lumbar lordosis (TK+LL), according to the approach proposed by Mendoza–Lattes.
10
Normal TK+LL was defined as less than
Proximal junctional kyphosis was defined at the final follow-up radiograph as described by Glattes: proximal junctional Cobb angle greater than 10° and at least 10° greater than the corresponding preoperative measurement. The presence of both criteria was necessary to be considered abnormal. 16
Statistical Analysis
Data was analyzed with SPSS 23.0. Continuous variables with normal distribution were presented as mean ± standard deviation, continuous variables with skewed distribution were presented as median (lower quartile, upper quartile), and categorical variables were expressed as frequency or percentages. Independent t test and Mann–Whitney U-test were used to analyze the differences in continuous variables between groups. Fisher’s exact test and
Results
Prevalence and Characteristics of PJK Patients
There were 94 female and 19 male patients. The average age at the time of surgery was 60.8
Comparison of patient characteristics and surgical factors between PJK and non-PJK group.
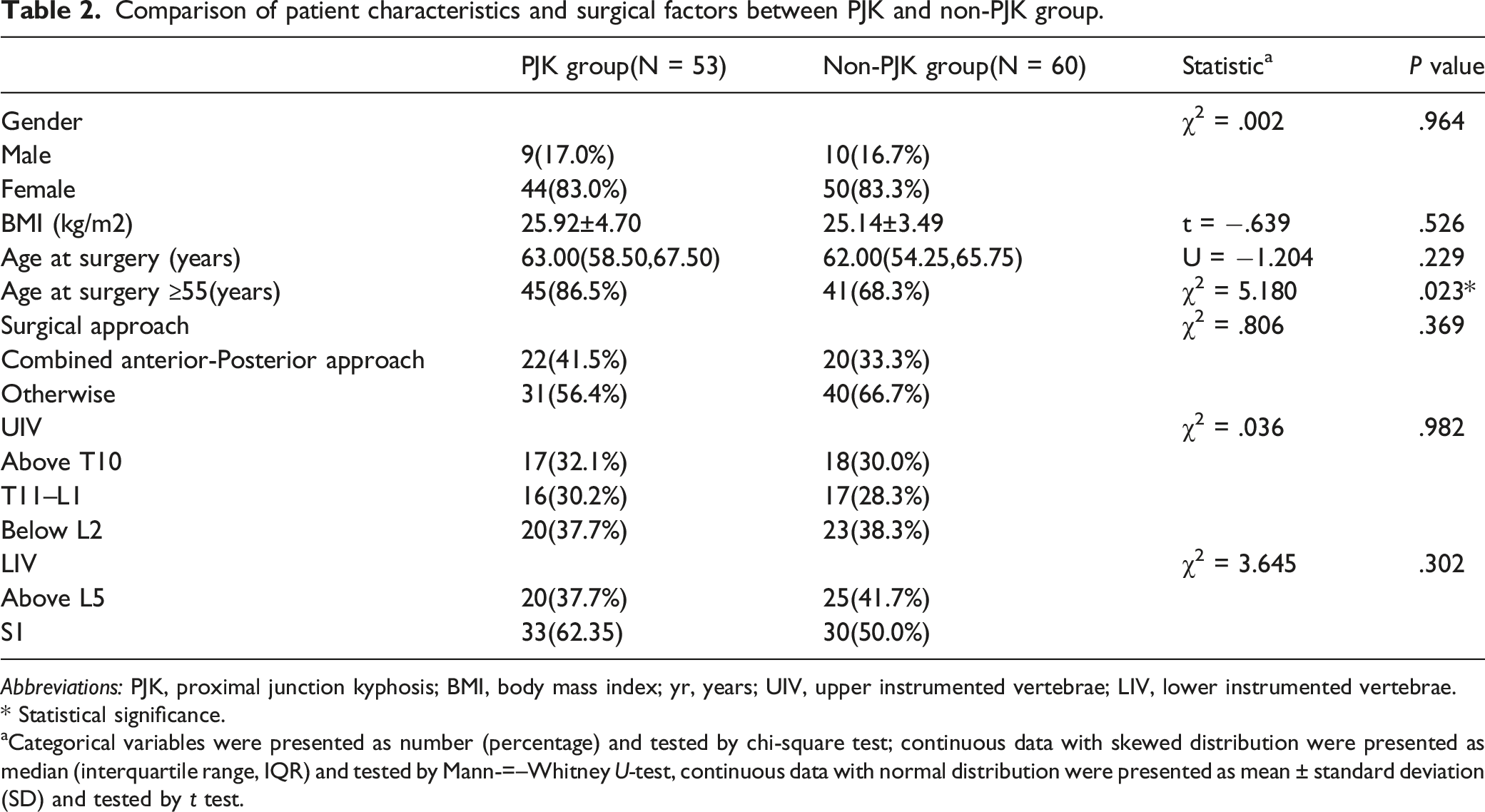
Abbreviations: PJK, proximal junction kyphosis; BMI, body mass index; yr, years; UIV, upper instrumented vertebrae; LIV, lower instrumented vertebrae.
* Statistical significance.
aCategorical variables were presented as number (percentage) and tested by chi-square test; continuous data with skewed distribution were presented as median (interquartile range, IQR) and tested by Mann-=–Whitney U-test, continuous data with normal distribution were presented as mean ± standard deviation (SD) and tested by t test.
Comparison of radiographical parameters between PJK and non-PJK group.
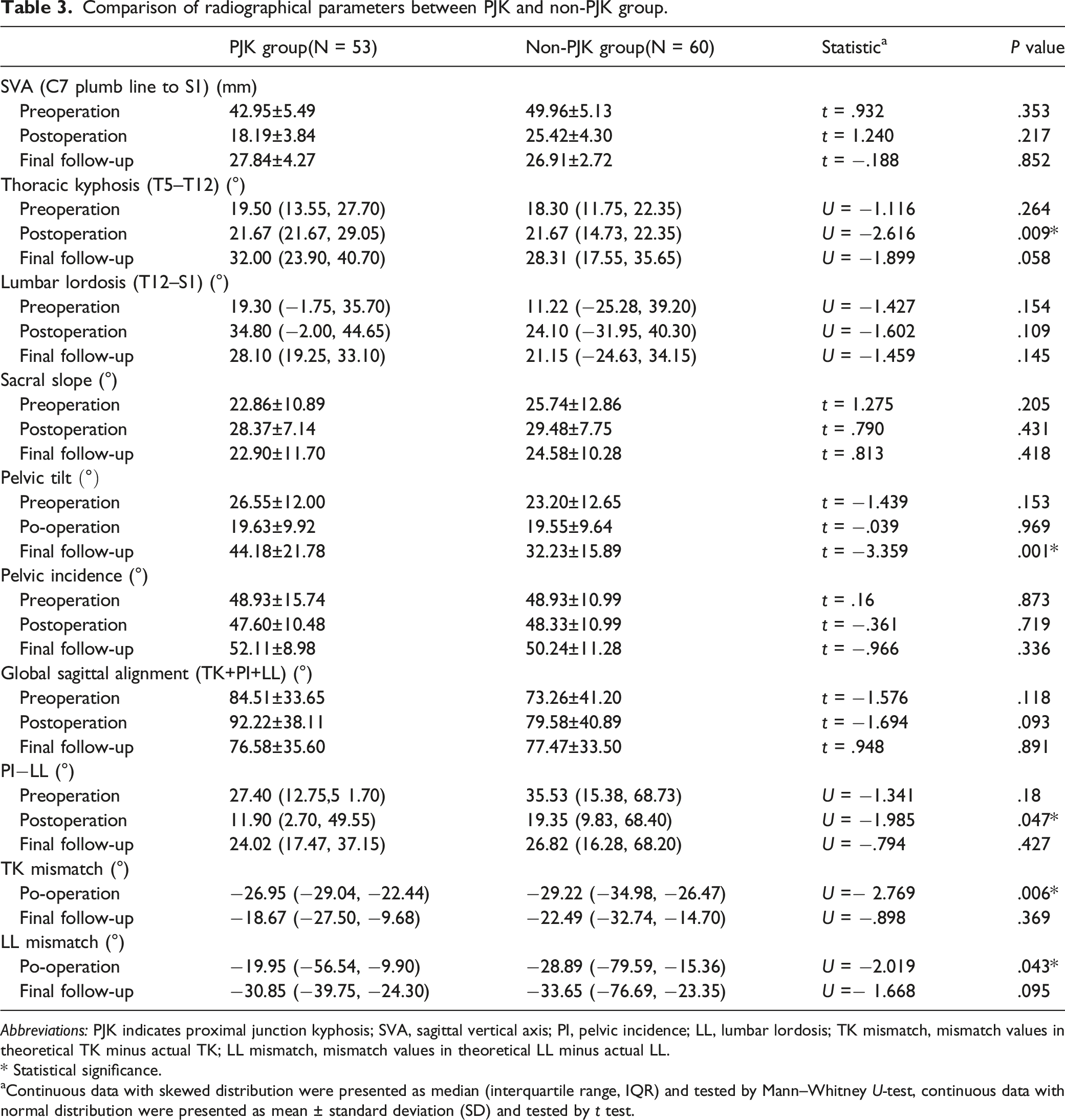
Abbreviations: PJK indicates proximal junction kyphosis; SVA, sagittal vertical axis; PI, pelvic incidence; LL, lumbar lordosis; TK mismatch, mismatch values in theoretical TK minus actual TK; LL mismatch, mismatch values in theoretical LL minus actual LL.
* Statistical significance.
aContinuous data with skewed distribution were presented as median (interquartile range, IQR) and tested by Mann–Whitney U-test, continuous data with normal distribution were presented as mean ± standard deviation (SD) and tested by t test.
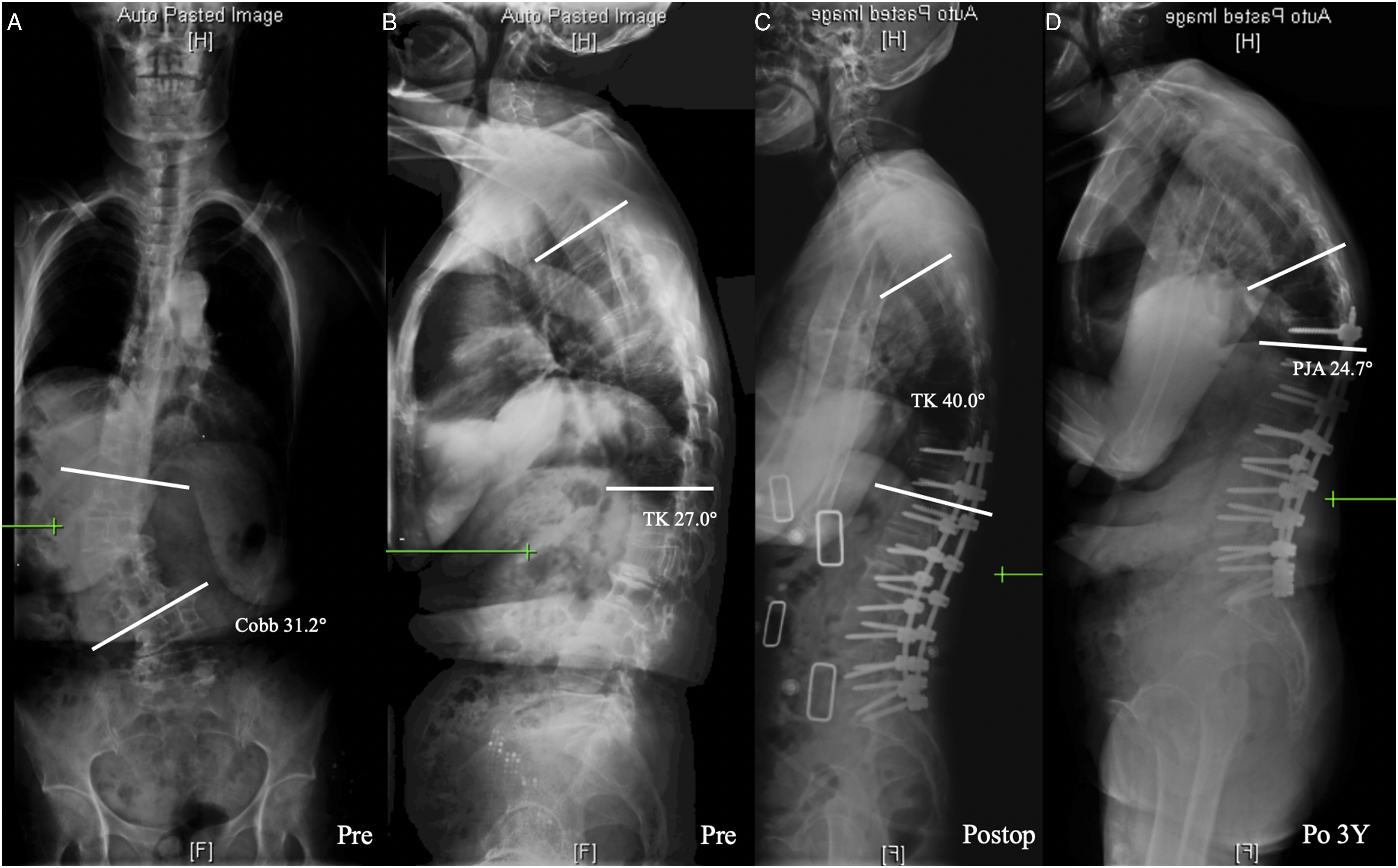
According to the formulas LL = .67PI+23.7 and TK = .15PI + 43, as proposed by Sebaaly, we also calculated the theoretical values of LL and TK and their gaps with actually their observed values. The mismatch of LL, that is, the difference between average theoretical LL and observed postoperative LL, in the non-PJK group was significantly higher than that in the PJK group (P = .043). Likewise, the mismatch of TK, that is, the difference between average theoretical TK and observed postoperative TK, in the non-PJK group was also found higher than that in the PJK group (P = .006, Table 3) (Figure 1 and 2). 64-year-old woman presenting with degenerative lumbar scoliosis and sagittal imbalance (Cobb angle 19.9°, TK 3.2°, LL −1.7°, SS 21.9°, PT13.9°, PI 36.1°) (A, B). We performed posterior iliac screw fixation on T10–S2. Postoperative Thoracic Kyphosis was 17.4° while the theoretical TK was 47.8°, indicating a large mismatch (C).postoperative 3-year whole spine lateral radiograph showing normal sagittal balance without occurence of proximal junctional kyphosis (proximal junctional kyphosis angle 5.6°) at final follow-up (D). 63-year-old woman presenting with degenerative lumbar scoliosis and major sagittal imbalance (Cobb angle 31.2°, TK 27.0°, LL −23.1°, SS 25.5°, PT30.2°, PI 54.8°) (A, B). She was operated with posterior instrumentation on T10–S1. Postoperative Thoracic Kyphosis was 40.0° while the theoretical thoracic kyphosis was 50.65°(C). 3 years postoperatively (final follow-up), she presented a proximal junctional kyphosis with a proximal junctional kyphosis angle of 24.7°(D). Compared with the non-proximal junctional kyphosis subject presented in Figure 1, she had a higher postoperative thoracic kyphosis which was closer to the theoretical value. Our findings suggested a necessity for developing personalized orthopedic plan against adult degenerative scoliosis patients specifically.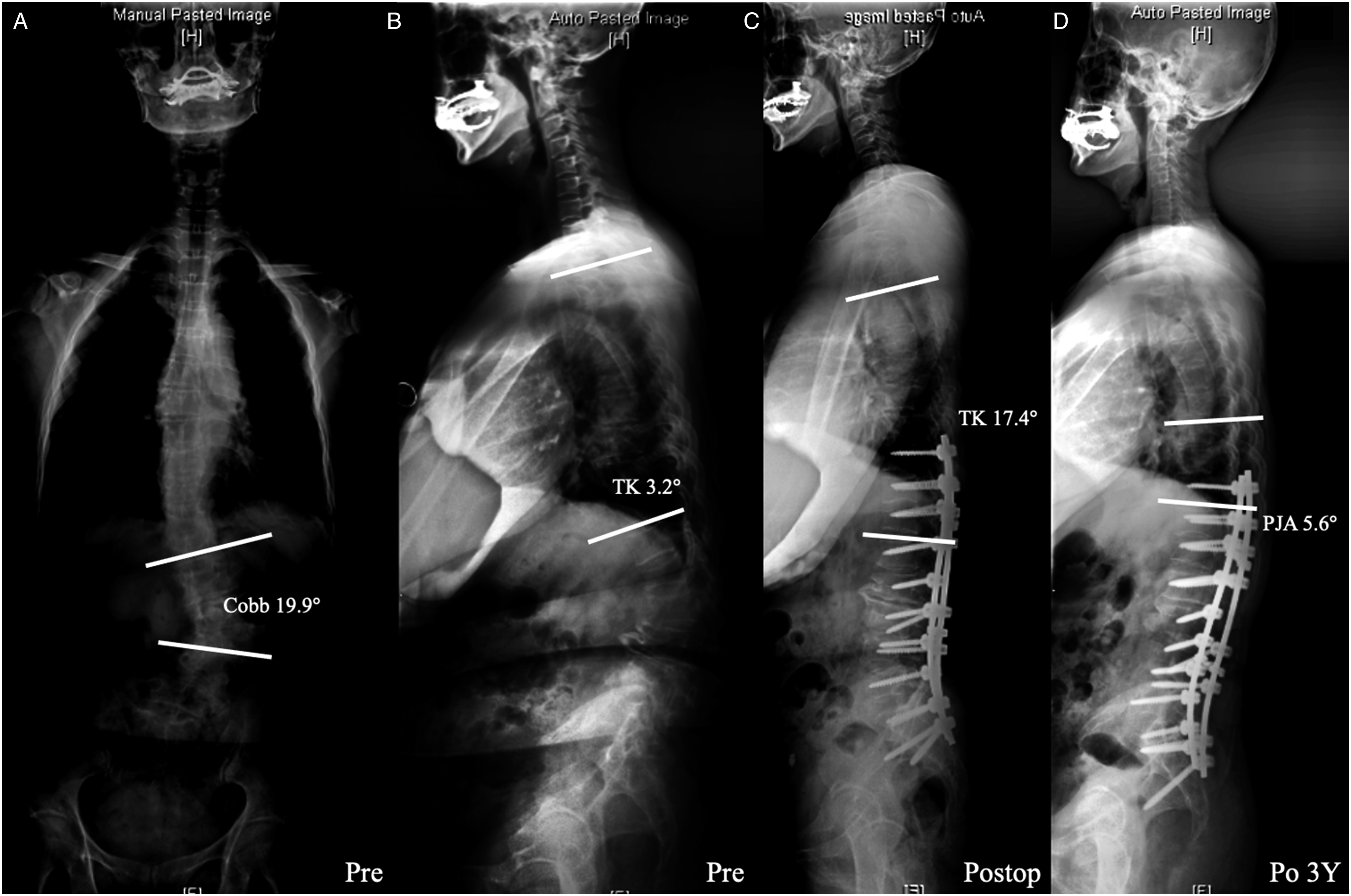
Comparison of radiographical parameter changes between PJK and non-PJK groups.
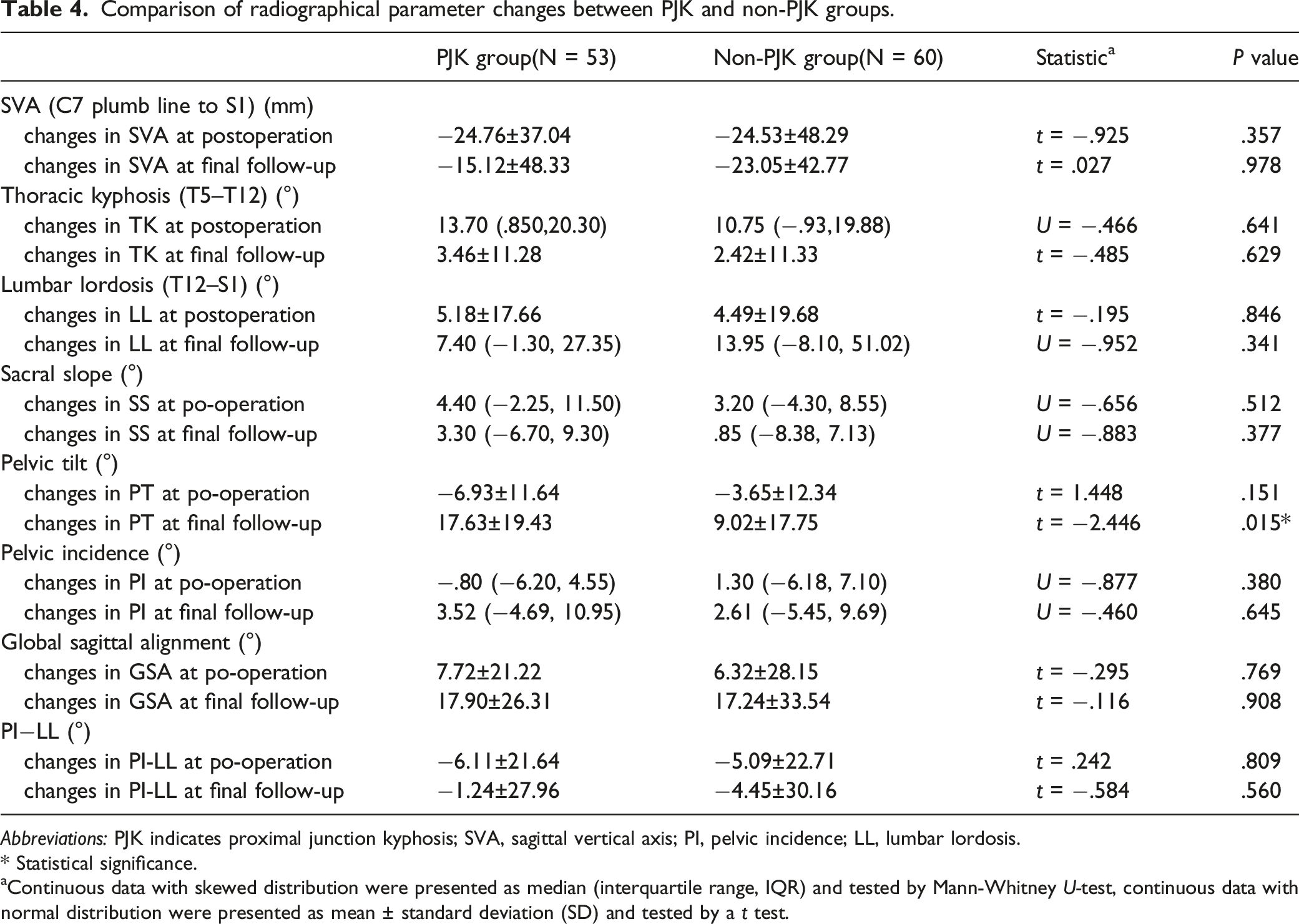
Abbreviations: PJK indicates proximal junction kyphosis; SVA, sagittal vertical axis; PI, pelvic incidence; LL, lumbar lordosis.
* Statistical significance.
aContinuous data with skewed distribution were presented as median (interquartile range, IQR) and tested by Mann-Whitney U-test, continuous data with normal distribution were presented as mean ± standard deviation (SD) and tested by a t test.
To further examine the predictive models, the actual values of specific parameters were calculated and compared to their theoretical values in terms of each measurement:
Comparison of predictive models between PJK and non-PJK group.
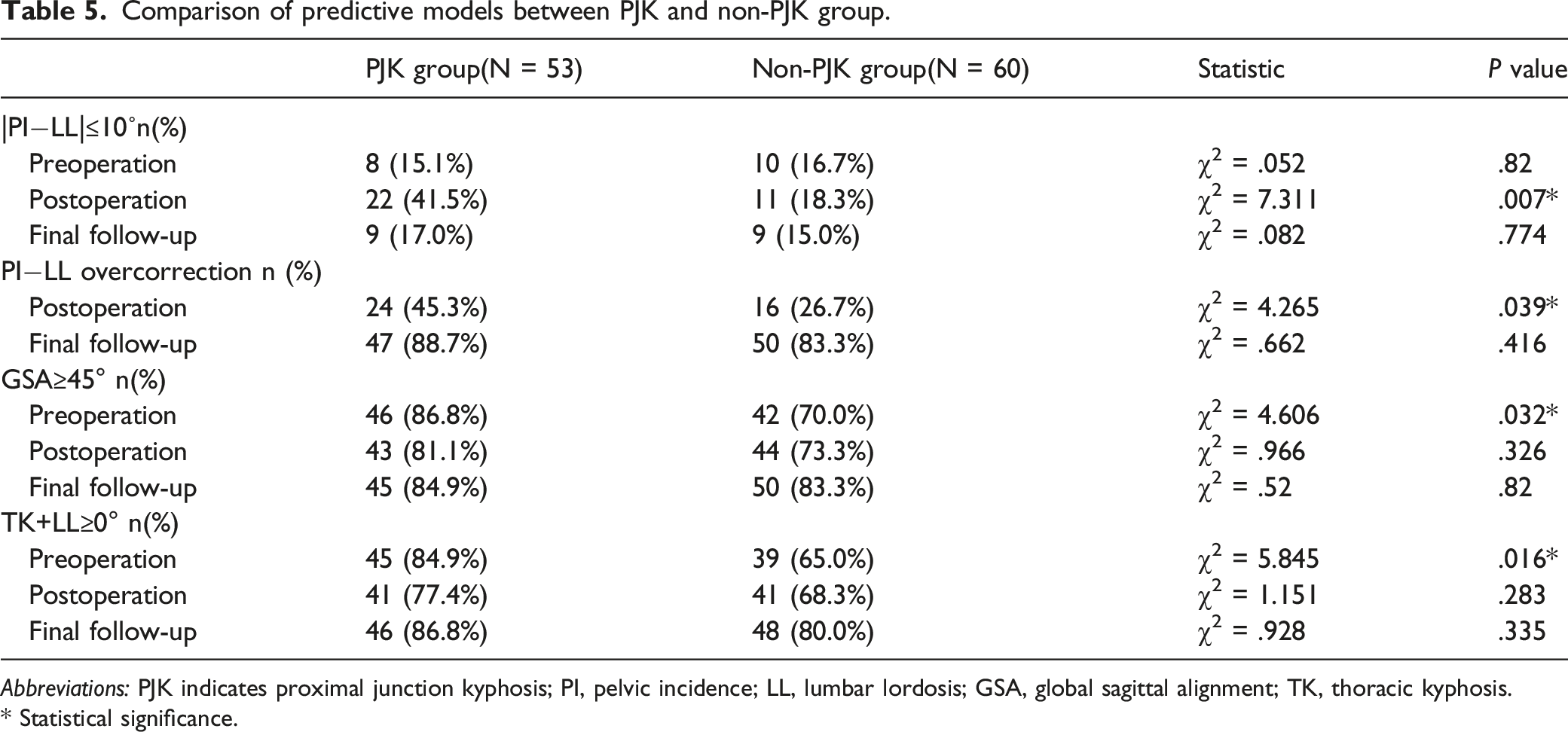
Abbreviations: PJK indicates proximal junction kyphosis; PI, pelvic incidence; LL, lumbar lordosis; GSA, global sagittal alignment; TK, thoracic kyphosis.
* Statistical significance.
Model 2: The average postoperative PI
Model 3: The average preoperative TK+LL was 29.79°. Moreover, 84.9% of PJK group was associated with positive TK+LL preoperation, compared to the 65.0% of non-PJK group (P = .016) (Table 5).
Risk Indicators
Risk factors for PJK in ADS patients identified through multivariate analysis.
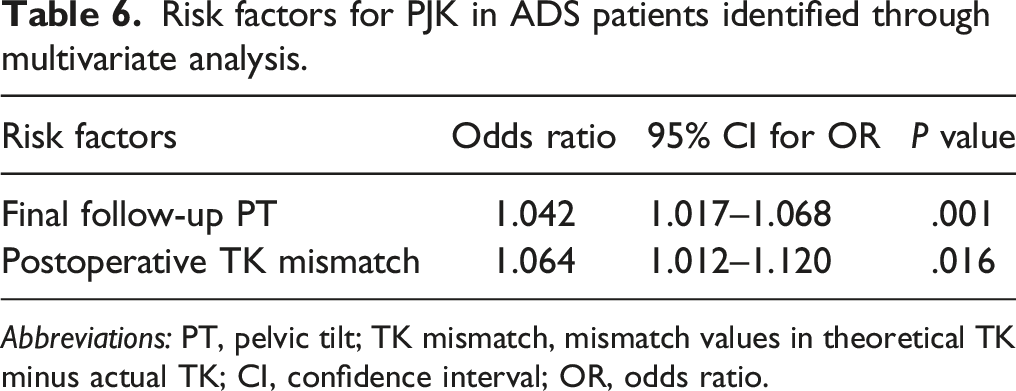
Abbreviations: PT, pelvic tilt; TK mismatch, mismatch values in theoretical TK minus actual TK; CI, confidence interval; OR, odds ratio.
To further evaluate the effectiveness of the two parameters in indicating PJK, we performed ROC curves and calculated the Youden index to figure out the best cut-off points. The ROC curve was painted based on the division of PJK group and non-PJK group (Figure 3). We found that the best cut-off values for indicating PJK were final follow-up PT = 39.05° (AUC = .676, sensitivity = 64%, specificity = 68%) and postoperative TK mismatch = −28.56° (AUC = .651, sensitivity = 74%, specificity = 58%). Receiver operating characteristic curve to find the optimal cut-off points of final follow-up Pelvic Tilt and postoperative thoracic kyphosis mismatch to predict proximal junctional kyphosis.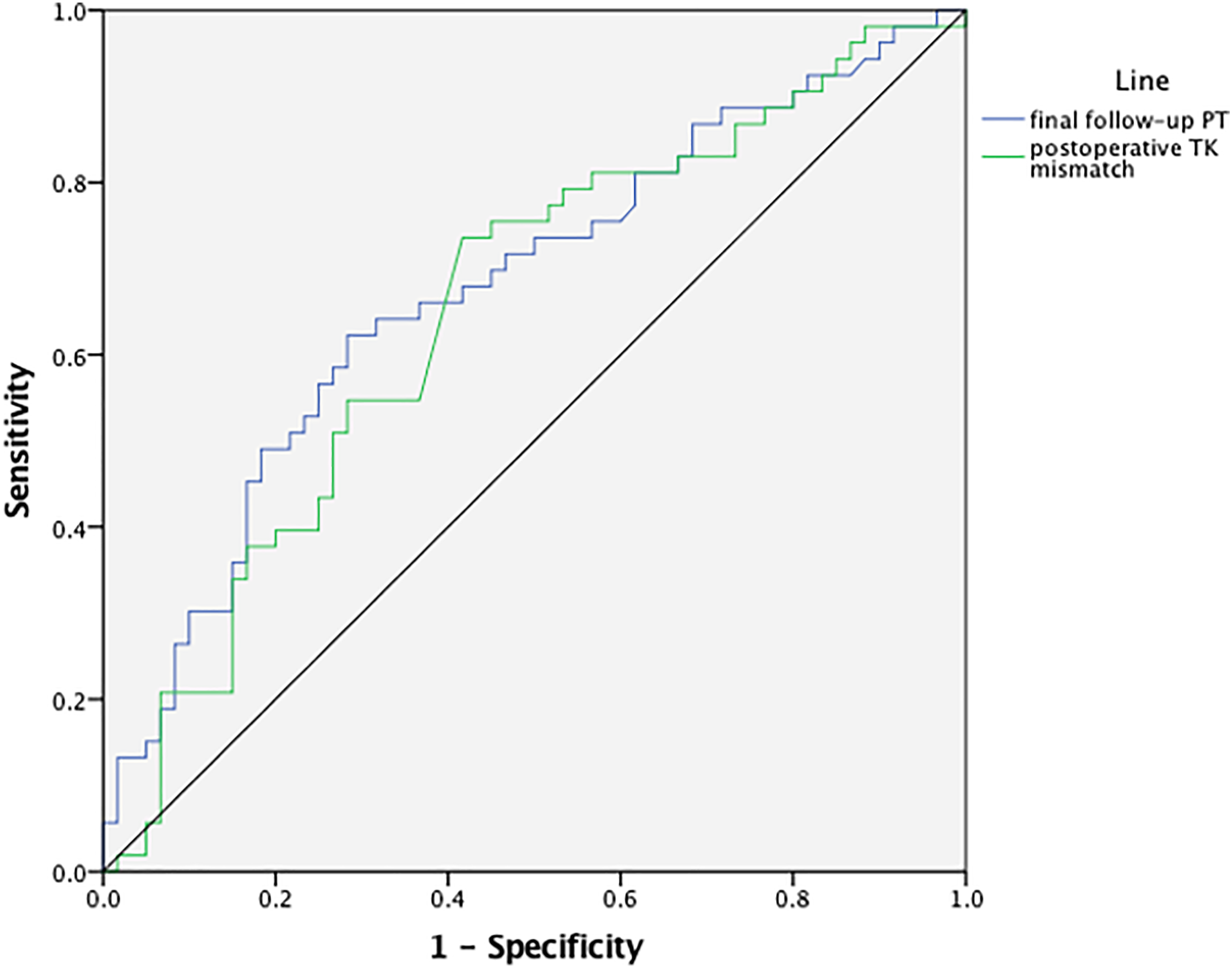
Discussion
Proximal junctional kyphosis has been identified as a common complication in patients undergoing corrective surgeries for adult spinal deformities. 17 As reported by Bridwell, this condition may progress with deterioration of sagittal alignment with an apex, and may lead to compromised balance in the sagittal plane, vertebral collapse, and, in some cases, neurological symptoms. 18
This study reviewed 113 ADS patients with a 46.9% prevalence of PJK, which was similar to the incidence described in previous studies.19,20 Existing literatures suggested that the development of PJK is associated with a variety of baseline characteristics, surgical parameters, and radiographical parameters.6,7 Nonetheless, related indicators for predicting the occurrence of PJK are still controversial without a comprehensive examination. Therefore, the present study systematically evaluated potential risk factors for PJK as well as 3 radiological predictive models.
Existing evidence has pointed to age as a risk factor for PJK. 21 As reported by Liu et al, patients who were older than 55 years at the surgery were more liable to developing PJK compared to younger patients. 6 In addition, Kim et al suggested that advanced age correlated with a high prevalence of revision surgeries for PJK. 22 Consistent with previous findings, our study revealed a higher prevalence of PJK among patients over 55 years old (52.3%), as contrasted to the 28% among the younger patients, which indicated advanced age as a risk factor for PJK. Age dependents disc and facet joint degeneration also led to the development of spinal extension musculature in the older adult patients. These degenerative factors might affect the sagittal balance of patients, which may eventually lead to PJK. 17
There were also some radiographical variables identified as potential risk factors for PJK. According to Buell et al, postoperative TK was significantly associated with developing PJK. 23 The present study also demonstrated that greater postoperative TK may serve as risk factors for PJK. This could be explained by the increased junctional stress at the proximal end of UIV caused from large thoracic kyphosis. In patients with a hyperkyphotic thoracic spine, the compensatory mechanism often fails with weak back muscle strength caused by surgery. 24 Besides, we postulated that a relative higher postoperative TK implied a substantial correction after surgery, which may cause a reciprocal kyphosis at the proximal junction. 25 We further suggested a necessity of monitoring TK intraoperatively to prevent PJK.
According to previous study, a large TK was often accompanied with a large LL, which implies that the latter was also a risk factor for PJK. 22 Non-ideal LL might lead to an acute change in the sagittal alignment and eventually results in PJK as a compensatory response to restore sagittal balance. 26 Considering the essential role of TK and LL in keeping sagittal spinal balance, Sebaaly proposed to restore LL and TK to their theoretical ideal values based on PI, as calculated through the formulas LL = .67PI+23.7 and TK = .15PI+43 11 . After applying the two formulas to our subjects, we noted that observed postoperative TK and LL were closer to their theoretical values in the PJK group compared with non-PJK group. One possible explanation is that the construction of the formula was based on symptomatic subjects, whose sagittal parameters might have a different range from those of ADS patients. 27 For example, normal TK values were universally higher than observed TK values in the present study. However, a relative higher postoperative TK was found to be a potential risk factor for PJK among ADS patients. It is possible that excessive amount of sagittal balance correction against normal value would lead to a higher prevalence of PJK. Multivariable analysis further indicated that postoperative TK mismatch was an independent risk factor for PJK. Therefore, one should note that merely restoring TK and LL to their theoretical values based on normal population is insufficient to prevent the occurrence of PJK among ADS patients, and it is vital to develop a personalized orthopedic plan for a moderate correction.
Besides sagittal thoracolumbar parameters, pelvic parameters also have important implications for the postoperative development of PJK. In line with previous study, we found that a higher final follow-up PT was significantly associated with developing PJK. 14 Increased PT may be the primary cause of sagittal malalignment, it could also be explained as compensatory mechanisms for the forward incline of sagittal alignment caused by PJK.28,29 In the present study, the early occurrence of PJK in some cases precluded the ability to obtain a follow-up radiograph without the presence of PJK and the accompanying compensatory changes. Therefore, whether final follow-up PT is a risk factor for PJK or is a compensatory consequence of PJK needs further study. We suggested PT as an indicator for diagnosing PJK postoperatively with the cut-off value of 39.05°.
Finally, we calculated the three radiographical models to assess their efficacy for predicting PJK in ADS patients, based on preoperative, postoperative and final follow-up radiographs. All three radiographical models were found statistically predictive for the occurrence of PJK.
The first predictive model suggests that GSA (PI+LL+TK) greater than 45° implies the occurrence of PJK, as proposed by Rose et al. 12 The model was also supported by the study of Yagi et al, who found that 84% of patients in the PJK group were subject to non-ideal GSA (PI+LL+TK>45°) in the preoperative period. In line with these studies, our results suggested that preoperative GSA>45° was a risk factor for PJK. A possible account is that positive GSA may induce positive SVA and increase the stress for the proximal and distal junctions during the instrumentation, which may result in PJK. 7
The second predictive model was PI
It is possible that the postoperative PI–LL mismatch in the PJK group was generally overcorrected, which ultimately resulted in sagittal overcorrection and therefore PJK. Using the age-adjusted ideal PI–LL mismatch criteria proposed by Lafage, 15 we found that patients who developed PJK underwent significantly greater correction. Therefore, our data revealed that global alignment overcorrection was associated with a higher prevalence of PJK. Overcorrection of PI–LL mismatch have been proposed as potential risk factors leading to the development of PJK. Yang demonstrated that larger PI–LL mismatch could lower the risk of PJK. 33 More specifically, Kim et al suggested that excessive correction of the sagittal plane might lead to increased stress concentrations at the proximal end of the fusion. 16 Furthermore, they pointed out that patients with PI–LL mismatch <11° were more likely to have late-onset PJK that would require further surgeries. 34 Patients with an overcorrected PI-LL mismatch would unconsciously generate compensatory mechanisms to realign and correct the sagittal balance, which might lead to PJK. 35 Surgical plans should incorporate age-adjusted ideals to minimize the risk of PJK and increase the likelihood of sustainable realignment success.
The third predictive model, proposed by Mendoza-lattes et al, suggested that the sum of LL and TK is positively associated with the incidence of PJK. Mendoza-lattes reported that, for every 10 degrees of increase in preoperative TK+LL, the risk of developing PJK would increase by 140%. Our study also found that the PJK group had a higher prevalence of positive preoperative TK+LL, indicating that preoperative TK+LL>0°was a risk factor for PJK. The relationship between TK and LL plays a critical role in keeping sagittal balance, as TK largely depends on LL and the number of vertebras involved in the LL curve. 36 Our findings implied that the risk of PJK could be minimized by including sufficient correction of LL and TK in the surgical plans.
There are some limitations of this study. Firstly, as described above, causal relationship between pelvic tilt and PJK cannot be warranted with the cross-sectional data at final follow-up. Secondly, since our sample included more female patients, the results might be subject to gender-bias. Finally, it is a retrospective study with some inaccessible variables (such as bone density to study the effect of osteoporosis) and missing values. Therefore, we recommend further prospective studies that are adequately designed to examine our present conclusions.
Conclusion
For ADS patients who receive corrective surgeries, our study found that postoperative TK mismatch was an independent risk factor for PJK. In addition, the risk of radiographic PJK increases with an age over 55 years old and higher postoperative TK. All three predictive models can satisfactorily predict the occurrence of PJK. Respectively, the three models suggest three conditions to prevent postoperative PJK: 1) GSA less than 45°; (2) surgical overcorrection as indicated by PI–LL, and (3) positive sum of TK and LL. To summarize, our results stress the importance of restoring the global alignment balance to its ideal range and avoiding the overcorrection of sagittal balance in preventing postoperative PJK among ADS patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Note
The present study was approved by the Institutional review board of the authors’ affiliated institution (IRB number: M2021239)