
Abstract
Study Design
Retrospective multicenter study
Objectives
To investigate changes over a 10-years period in the profile of cervical spine and spinal cord injuries among the elderly in Japan.
Methods
The current multicenter study was a retrospective analysis of inpatients aged ≥65 years, suffering cervical fracture (CF) and/or cervical spinal cord injury (CSCI). We analyzed 1413 patients’ epidemiology (from 2010 to 2019). Moreover, 727 patients who underwent surgical treatment were analyzed in 2 groups: the early (2010-2014) and late period (2015-2019).
Results
Both the number of patients and number of surgical patients showed a significant increasing trend (P < .001), while the mean age, the distribution of injury levels and paralysis severity, and the proportion of surgical indications remained the same. The number of surgical patients doubled from 228 to 499 from the early to late periods. Posterior surgery was the most common approach (90.4%), instrumentation surgery with screws increased significantly, and the range of fusion was significantly longer in the late period (2.1 vs 2.7 levels, P = .001). Significantly worsening neurological symptoms were recorded in the late period (1.3% vs 5.8%, P = .006), with C5 palsy being the major one. Otherwise, perioperative, major, and other complications, including mortality, did not differ significantly in incidence.
Conclusions
Both the number of elderly CF and/or CSCI patients and number of patients undergoing surgery increased dramatically over the decade without any change in profile. Instrumentation surgeries with screws increased, without an increase in systemic complications.
Keywords
Introduction
With the growing elderly population worldwide, the incidence of cervical spine and spinal cord injuries in elderly individuals is continually increasing. Thus, these injuries have become a major social issue.1-5 Elderly individuals are at risk of falls, 6 and they present with fatal injuries caused by minor trauma.7,8 Not only cervical fractures (CFs) with instability but also cervical spinal cord injuries (CSCIs) may require surgical treatment. In general, older patients commonly present with comorbidities and frailty, and they are more likely to develop postoperative adverse events.9-11 Therefore, several issues can impede surgical treatment in these patients.
Epidemiological changes in aging, CFs and spinal cord injuries, such as the number of elderly patients with CF and/or CSCI requiring surgical treatment, changes in injury morphology, and changes in the degree of paralytic complications, are unclear. Aging and Health, which reflects the growing elderly population worldwide, was the theme of World Health Day 2012. Japan became a super-aging society in 2006. That is, more than 20% of its population is aged over 65 years, and the rate of aging is unparalleled worldwide. 12 Since the aging population will continue to increase in several countries in the future, 13 epidemiological studies in Japan can present important implications regarding future medical care ahead of other nations. In addition, the safety of surgical treatments in elderly patients is an important issue. Hence, the efficacy of novel spinal surgical techniques and medical systems is not fully elucidated.
We hypothesized that not only the number of patients but also their age will increase over time, and that the number of spinal surgeries but not the incidence of perioperative complications will increase. The current nationwide, retrospective, multicenter study aimed to validate the longitudinal epidemiology of CF and/or CSCI and to investigate changes in surgical treatment modalities and the incidence of perioperative complications in elderly patients during a 10-years period in Japan.
Methods
Patient Population
The current retrospective multicenter study was conducted by the Japan Association of Spine Surgeons with Ambition (JASA) group, and it included inpatients aged 65 years or older who sustained CF and/or CSCI between 2010 and 2020. In total, 33 health care facilities were included in the database (Appendix Table A). The study protocol was approved by the Institutional Review Board (no. 3352-1) of each of the 25 representative institutions. Because this was a retrospective study, informed consent was not required for submission. The optout of this study was posted on the website (and title https://web.sapmed.ac.jp/orsurg/guide/hj0g2h00000007ax-att/pgsps60000000g3l.pdf and https://web.sapmed.ac.jp/orsurg/guide/hj0g2h00000007ax-att/pgsps60000000g3l.pdf) and we did not receive any inquiries. The minimum follow-up period was 3 months, and 1512 patients were enrolled in the database.
Due to the apparent paucity of data in 2020, 1413 patients for the injury period from 2010 to 2019 were included in the initial patient population, and epidemiological analyses were then performed. During this period, 842 patients underwent surgical treatment. Patients whose surgical procedure was unknown (n = 2) and those whose treatment plan was changed from conservative treatment to surgery more than 1 month after admission (n = 113) were excluded from the analysis. Therefore, 727 patients were included in the analysis (Figure 1). To compare data trends over time, the year of injury was classified into the early period (2010-2014) and the late period (2015-2019). Flowchart of patient inclusion.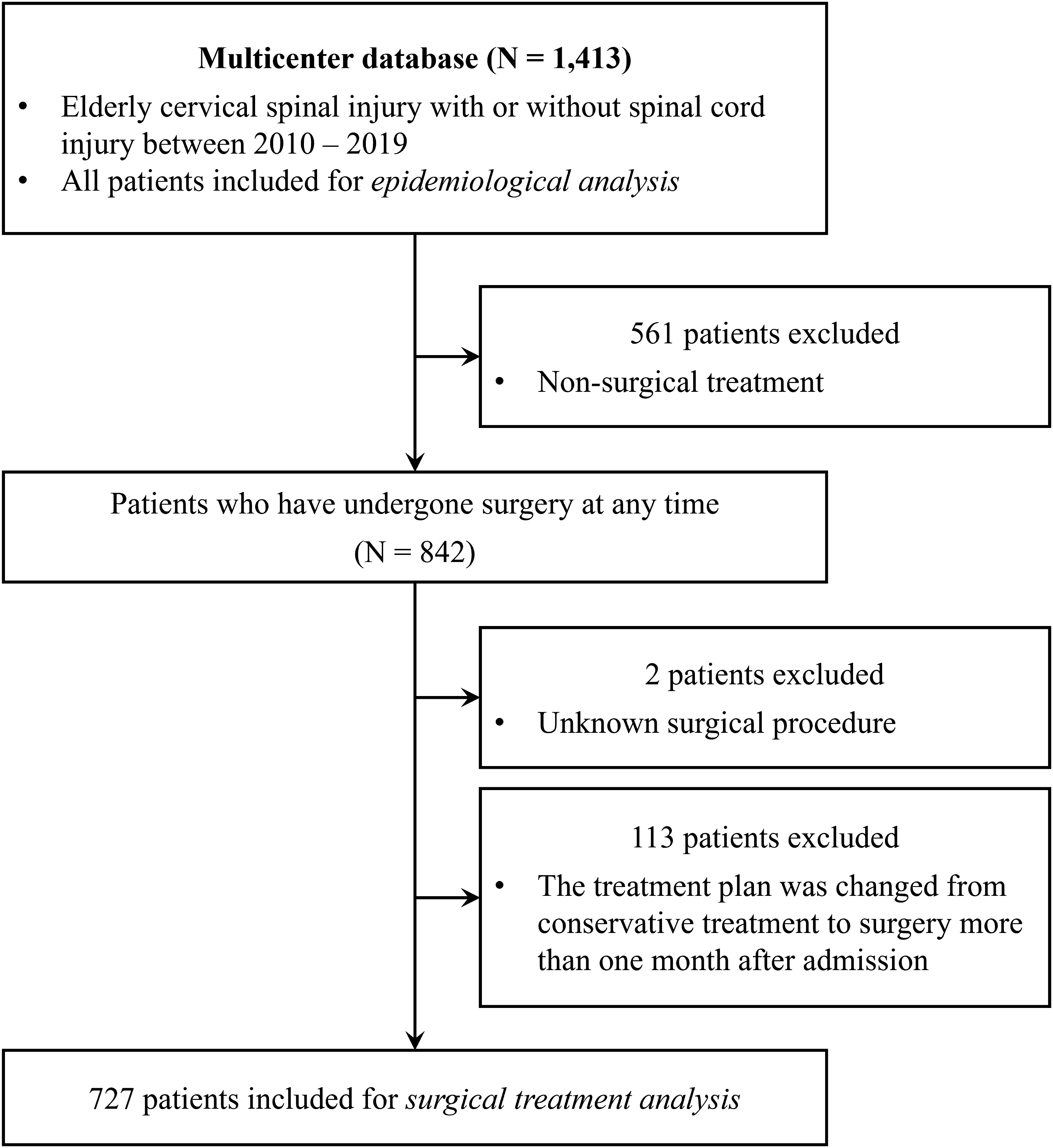
Demographic Characteristics of the Patients and Operative Data
Data on age, sex, presence of comorbidities, and use of medications were recorded and the 5-item modified frailty index14,15 (mFI-5) was calculated. Data on fracture, dislocation, CSCI, ASIA impairment scale, and incidence of mortality during hospitalization were recorded. Information about the number of surgical waiting, surgical procedure, number of fused vertebrae, operative time, estimated volume of blood loss, reoperation, postoperative worsening of neurological symptoms, incidence of other perioperative complications, and instruments used in the posterior fusion surgeries was collected.
The surgical procedures were selected based on the discretion of the spinal surgeon at each institution. Moreover, they were categorized as posterior approach decompression (eg, laminoplasty), posterolateral fusion (PLF), PLF with decompression, anterior surgery (eg, anterior cervical discectomy and fusion), and combined anterior and posterior surgery. The range of fusion in fusion surgeries was recorded. The instruments used in posterior fusion were categorized and recorded as pedicle screws (PS), lateral mass screws (LMS, including paravertebral foramen screws 16 ), and others (eg, wiring and plate systems) (with duplicates).
Patients received acute rehabilitation care to the full extent possible postoperatively. Patients with stable wounds and general conditions were discharged. However, if the condition was extremely difficult to be managed at home, the patient was transferred to another hospital for continuous rehabilitation and nursing care.
Statistical Analysis
Data were presented as mean ± standard deviation for continuous variables and as numbers and percentages for categorical variables. Statistical analyses were performed using R version 4.1.0 (http://www.R-project.org) using the Wilcoxon rank-sum test, Fisher’s exact test, Pearson’s chi-squared test, Jonckheere-Terpstra trend test, and Cochran-Armitage test. A P value of <.05 was considered statistically significant.
Result
Epidemiological Trends
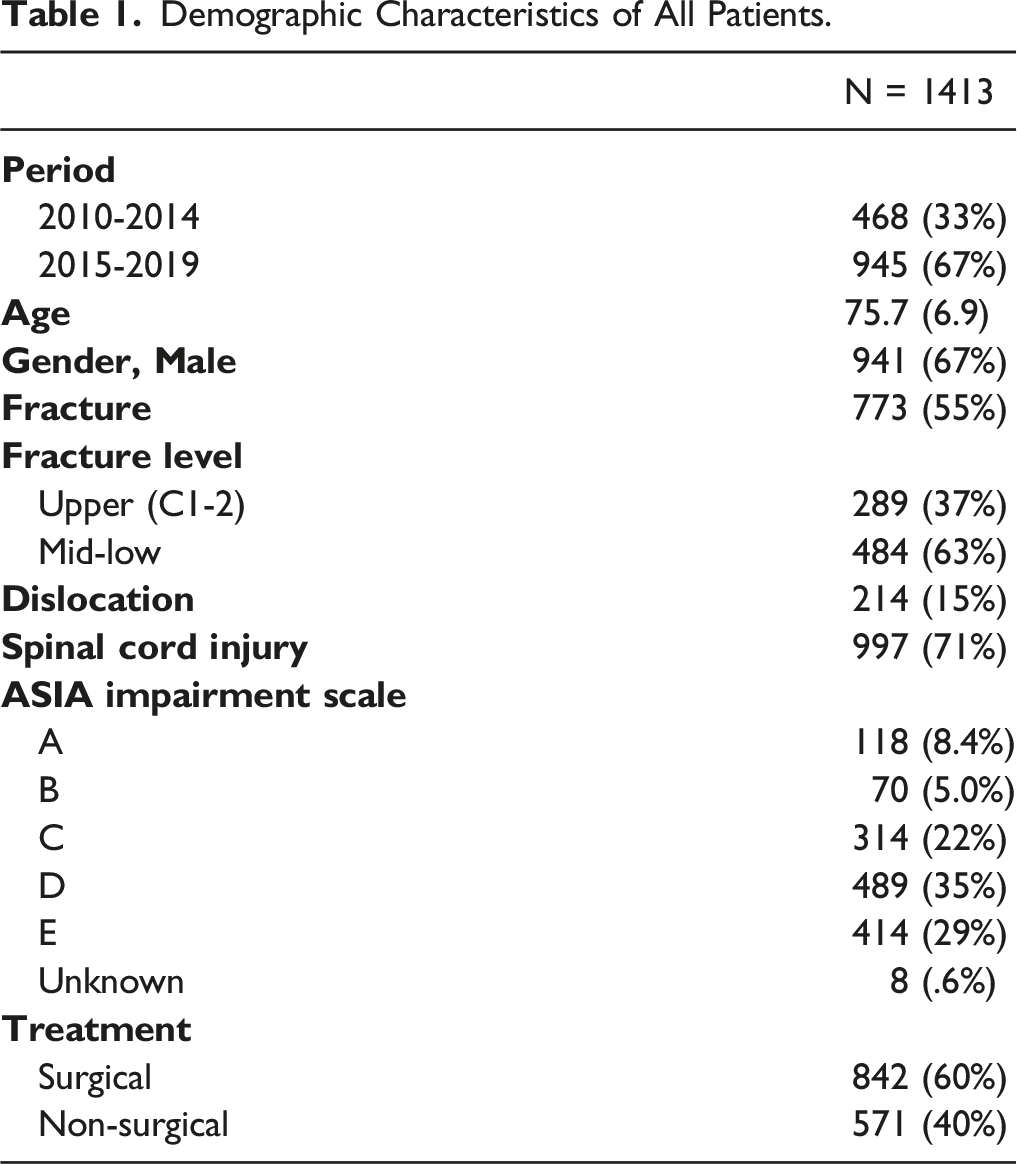
Demographic Characteristics of All Patients.
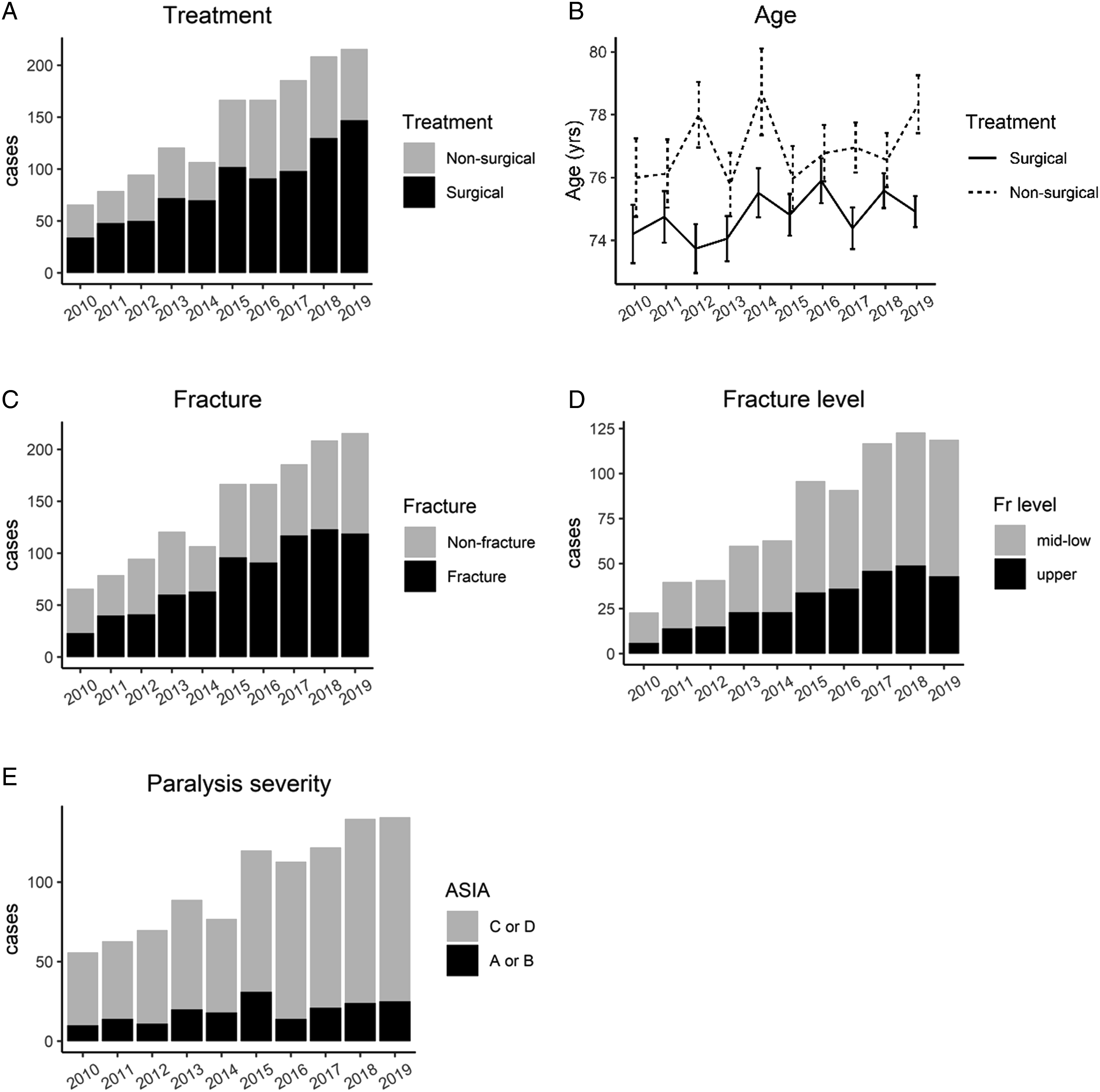
Epidemiological trends in all patients.
Demographic Characteristics of Patients who Underwent Surgery.
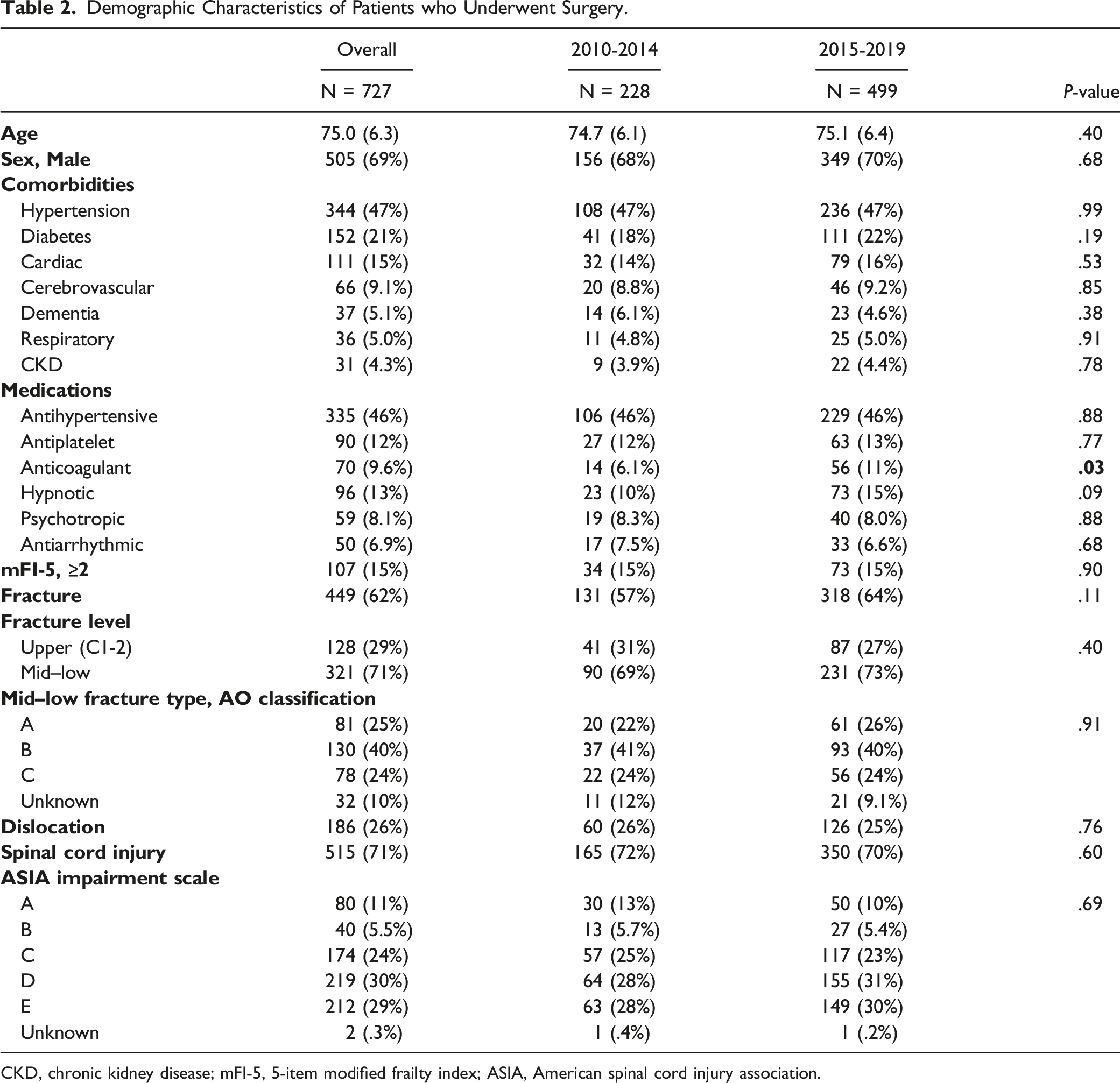
CKD, chronic kidney disease; mFI-5, 5-item modified frailty index; ASIA, American spinal cord injury association.
Surgical Treatments
Summary of Surgical Treatment.
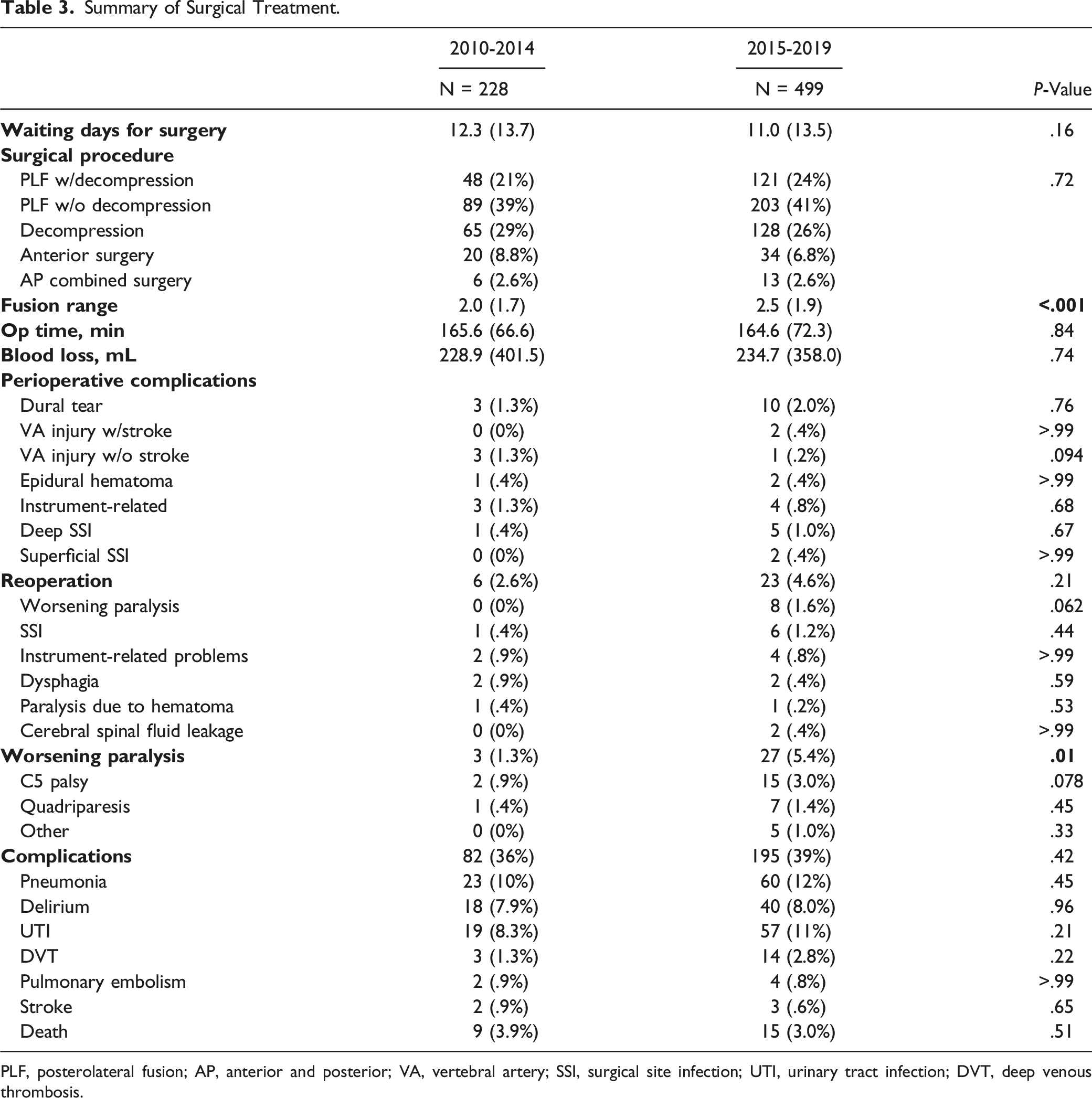
PLF, posterolateral fusion; AP, anterior and posterior; VA, vertebral artery; SSI, surgical site infection; UTI, urinary tract infection; DVT, deep venous thrombosis.
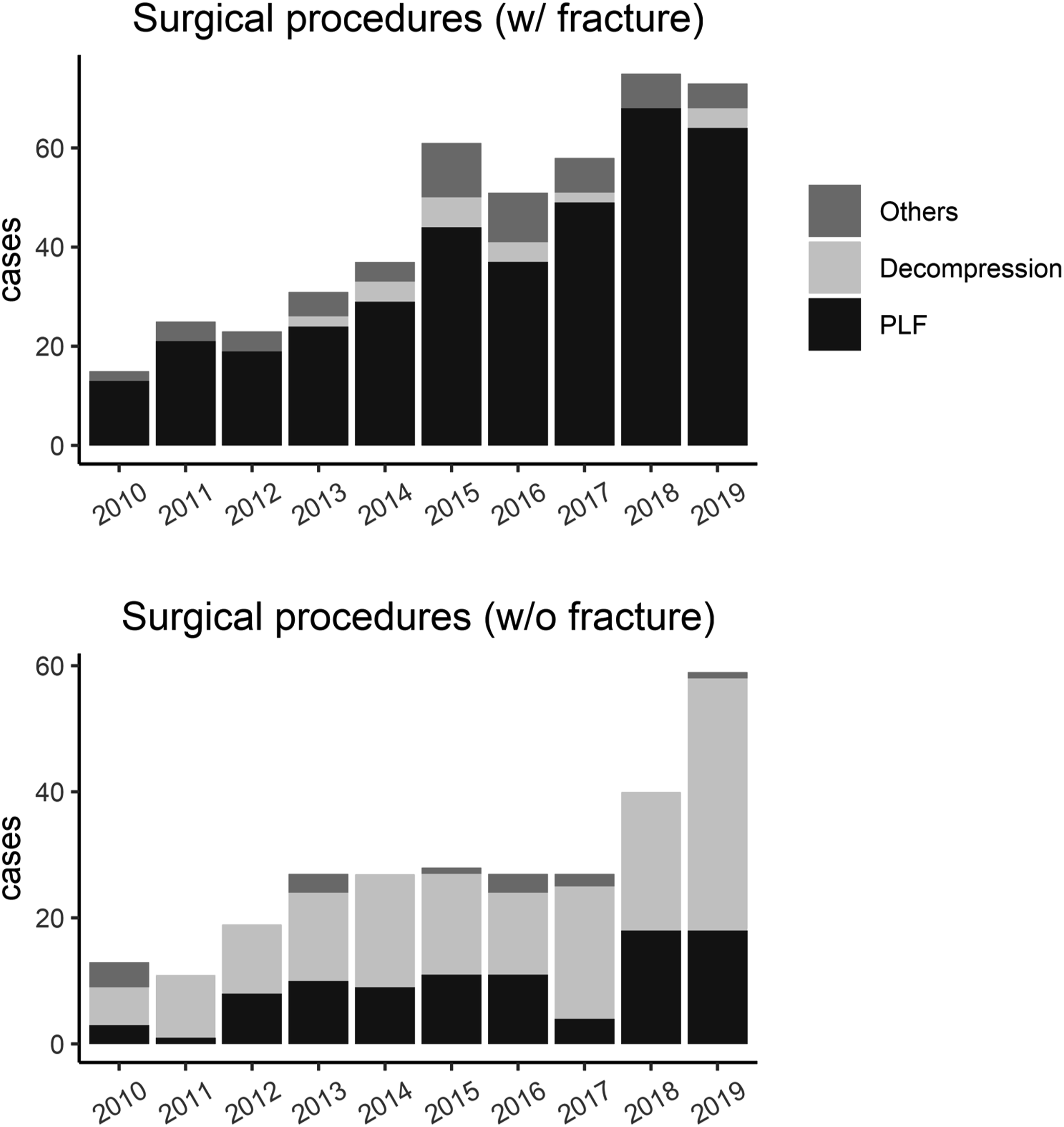
Surgical procedures according to the presence of fracture.
The incidence of perioperative complications did not differ significantly between the 2 periods (Table 3). In total, 29 patients underwent reoperation. There was no significant difference in terms of the reoperation rate between the 2 periods. However, reoperation for neurological symptom worsening was not performed in any of the patients in the early period and 8 patients in the late period (P = .06). Postoperative neurological deterioration was significantly more common in the late period than in the early period (P = .006), and the incidence of C5 palsy was relatively high in the late period than in the early period (n = 2 [.9%] in the early period and n = 15 [3.0%] in the late period, P = .078).
Summary of Posterolateral Fusion Surgery.
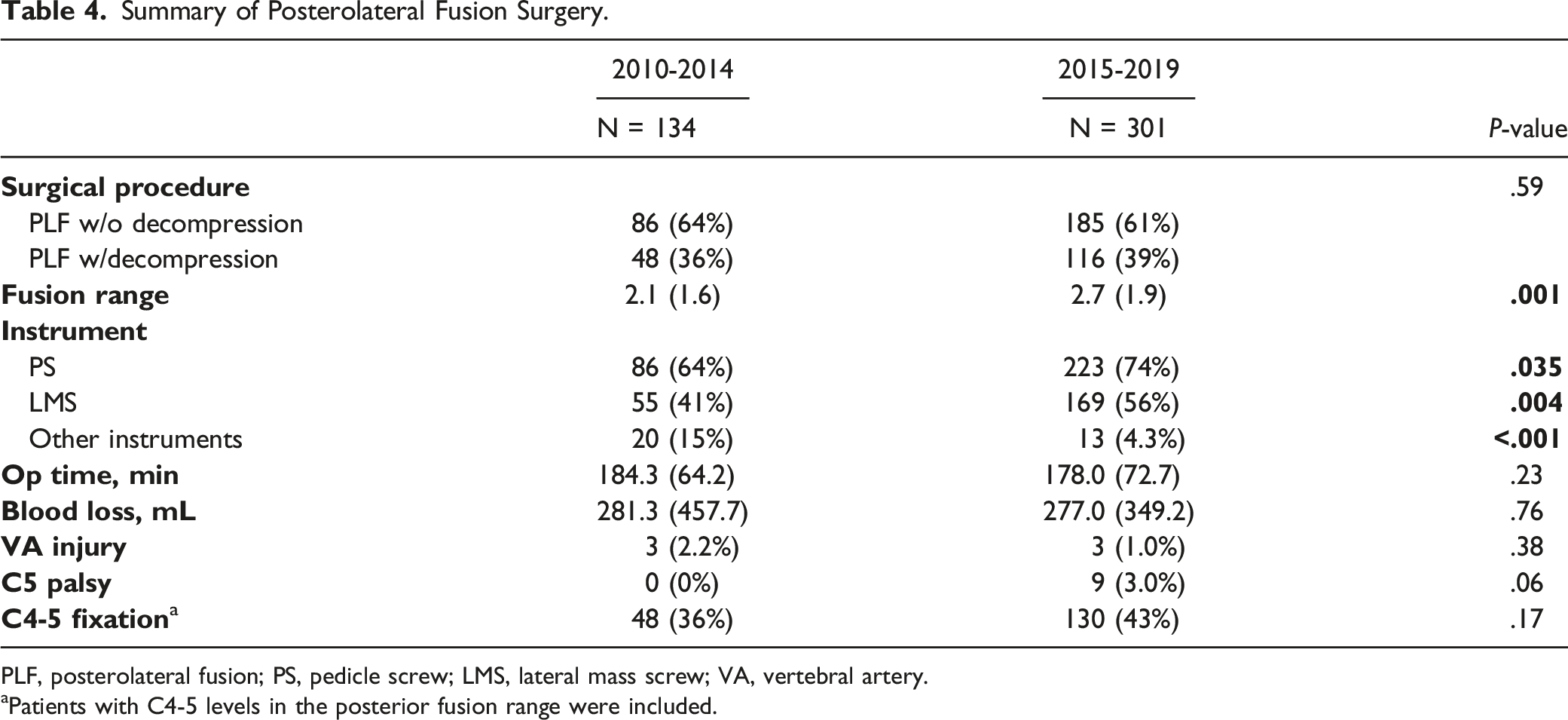
PLF, posterolateral fusion; PS, pedicle screw; LMS, lateral mass screw; VA, vertebral artery.
Patients with C4-5 levels in the posterior fusion range were included.
Outcomes
In total, 24 (3.3%; 9 [3.9%] in the early period and 15 [3.0%] in the late period, P = .51) patients were discharged after death. In total, 11 deaths (n = 3, respiratory failure; n = 1, pulmonary embolism; n = 1, myocardial infarction; n = 1, cerebral infarction; n = 1, massive gastrointestinal hemorrhage; n = 2, unknown; n = 1, cardiopulmonary arrest due to massive intraoperative hemorrhage; and n = 1, brainstem infarction due to intraoperative VA injury) were recorded within 1 month after surgery. Thus, 2 deaths (.29%) were directly attributed to surgery. There were no significant differences in the incidence of other major complications between the 2 periods (Table 3).
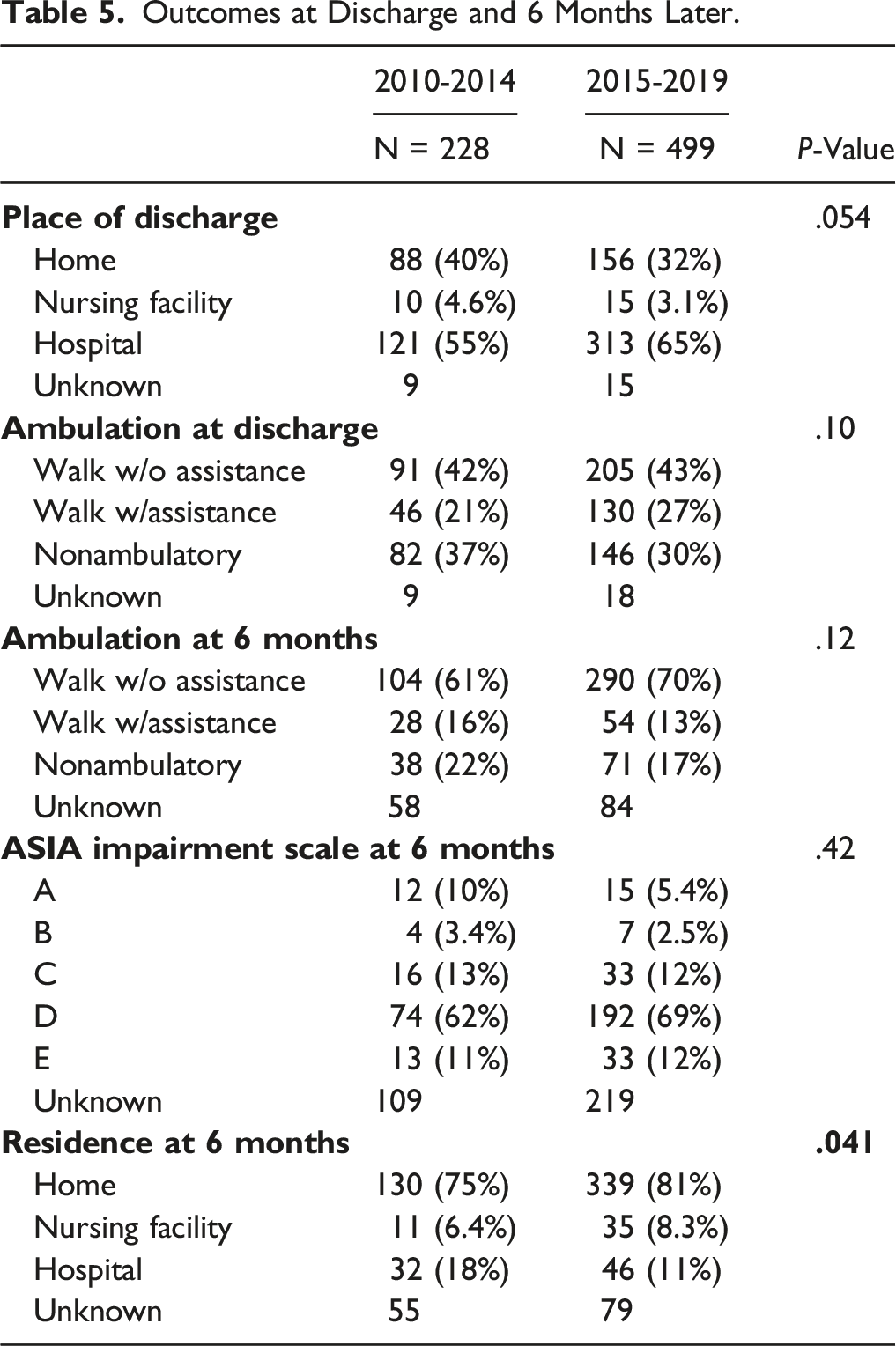
Outcomes at Discharge and 6 Months Later.
Discussion
This is the first study that examined the epidemiology and surgical treatment modalities of CF and/or CSCI in elderly patients during a 10-years nationwide study in Japan. The current study did not only conduct an epidemiological survey but also assessed the surgical treatment. Expectantly, the number of elderly patients with CF and/or CSCI and the number of patients undergoing surgery significantly increased. However, patient profiles such as age did not change remarkably. Approximately 90% of patients underwent posterior approach surgery, and the use of screws has increased. Moreover, there was a significant increase in the range of fusion. The incidence of perioperative mortality or fatal complications did not significantly differ.
The number of elderly patients with CF and/or CSCI increased over time. Interestingly, the mean age of the patients did not increase significantly in the surgical and non-surgical treatment groups. There was an increasing proportion of individuals with fractures; however, this does not indicate that most patients sustained fractures. The level of injury and the degree of paralysis did not significantly change. Thus, the change over the 10-year period was attributed to an increase in the number of patients. Although Japan has become a super-aged society unparalleled worldwide, 12 this situation is not unique in Japan, and several countries are moving toward the same social structure in the future. 13 In fact, cervical spine and spinal cord injuries in elderly patients will increase with the growing number of elderly people.1-5 Elderly people sustain CF and/or CSCI caused by minor trauma.7,8 This finding is owed to common factors, including the loss of physical and sensory abilities with aging, 17 which are associated with a higher risk of falls, and osteoporosis. Therefore, despite differences in social systems and racial differences, the results of this study represent not only the current situation in Japan but also important implications in other countries where the aging population can progress in the future.
Elderly individuals are frail,9-11 and the incidence of mortality is high in elderly patients with traumatic CSCI. 18 Thus, clinicians face difficulties in decision-making regarding the aggressiveness of treatments, including surgery, with consideration of the likelihood of recovery, survival, and risk of complications. There has been no significant difference in terms of mortality rate in elderly individuals with CF between the surgical and non-surgical groups in recent years. 19 McGee et al performed a retrospective study of patients with surgical spinal trauma (not limited to the elderly) using data obtained from 2015 to 2018. Results showed that the 30-days mortality rate of cervical spine injuries was 7.3%. 20 However, the current study showed that the mortality rate was only 3.3% (not limited to within 1 month) in elderly patients. Although 2 patients (.29%) died due to surgery, they were well within the acceptable risk range for the surgical treatment of elderly patients with CF and/or CSCI.
In the current study, systemic complications did not significantly decrease over time and occurred in 36% of patients in the early period and 39% of patients in the late period. Pneumonia was the most common systemic complication, similar to previous reports.21,22 Hartkopp et al 21 demonstrated that all-cause mortality decreased significantly from the first half (1953-1973) to the second half (1972-1992) of the observation period in spinal cord injury patients, and pulmonary emboli, sepsis, pneumonia, and uremia also decreased over time. On the other hand, in a study by DeVivo et al, 22 the highest mortality rates were for respiratory diseases since 2010, with no decrease in incidence since 1980. Patients in our study were relatively well managed despite their advanced age. For the frail elderly, prevention of systemic complications, such as pneumonia after spinal cord injury, may have reached its current limits.
In recent years, cervical spinal instrumentation with different types of screws, such as LMS and PS, is commonly used for the treatment of cervical spine disorders. Lateral mass screws 23 are relatively safe. However, this screw may have a relatively weak fixation force for patients with osteoporosis. In contrast, pedicle screws 24 have stronger pull-out strength than lateral mass screws.25–27 However, pedicle screws may damage the vertebral artery or the nerve root. 28 In recent years, the rapid spread of surgical support devices, such as navigation systems has led to safer cervical spine fusion using screws in Japan.29,30 This may be why screw instrumentation is being increasingly utilized in cervical spinal surgery in elderly individuals.
Rigid internal fixation with spinal instrumentation could reduce the range of fusion and simplify external fixation, thereby allowing early rehabilitation in the postoperative period and contributing to reduced postoperative complications. However, contrary to our expectations, the range of fusion increased, and the incidence of postoperative complications did not decrease. Fixation with screws was less rigid in elderly individuals because of osteoporotic issues. The data set does not provide direct information on the impact of instrumentation on the postoperative course because rehabilitation details were not available. However, the evolution of fixation methods alone did not reduce the incidence of complications in elderly patients with cervical spine trauma.
Next, whether the incidence of direct complications has increased due to instrumentation such as screws in the cervical spine was another concern in this study. Indeed, as previous reports have shown, 31 very few instrumentation-related VA injuries were documented in the current analysis. On the other hand, the causes of increased postoperative neurological adverse events in the late period are unclear. Although fixation methods other than screws may decrease the incidence of intraoperative complications, these may not be reliable for fixation particularly in elderly individuals who may have significant osteoporosis. Since complications associated with external fixation are also serious in cervical spine injuries,32,33 a technique with poor fixation should not be selected due to the risk of unnecessary complications. Surgery can be performed safely with a low complication rate due to the accumulation of knowledge, techniques, and recent advances in surgical support devices, and cervical fusion is a common procedure now. On the other hand, our study revealed an increased rate of postoperative neurologic adverse events. Thus, the surgery is by no means safe. We must weigh the advantages and disadvantages of surgical treatment, and ensure safe surgical procedures in conjunction with intraoperative neuromonitoring.
In addition, there was a possible increasing trend in the incidence of C5 palsy, a well-known complication after cervical spine surgery. The incidence of C5 palsy is significantly high in posterior approach surgery combined with fusion, and C4-5 fusion, which can achieve a more lordotic alignment in patients with a narrowed C5 intervertebral foramen due to degeneration, is a high risk procedure.34-38 Since all of the elderly population has some degenerative changes in the cervical spine,39,40 the current analysis included a population at high risk of C5 palsy after posterior fusion procedures. However, the incidence of C5 palsy was only 3.0%, even in the late period, which is comparable to or lower than that in previous studies.34-38 Therefore, we should refrain from discussing the association between C5 palsy and surgical treatment in elderly individuals with cervical spine and CSCI.
Despite a decrease in discharges to home in the late period compared to the early period of the current study, the number of patients living at home after 6 months increased. This may reflect the fact that patients who survived the acute phase were appropriately transferred to rehabilitation hospitals. Rehabilitation after CSCI is effective in the elderly. 41 Thus, the number of patients who live at home may have increased. Since the details of rehabilitation are not available from the present data, rehabilitation of elderly patients is a subject for further study.
Reducing this devastating trauma is very important. Fall prevention and environmental modification are critical for the prevention of cervical injuries in the elderly because falls, especially on the same level in the home, are the most common etiology of CSCI in the elderly.42,43 Furthermore, exercise to strengthen balance and muscles may reduce falls and subsequent cervical injuries. The Japanese Orthopaedic Association is generating awareness of this issue. 44
The current study had several limitations. First, selection bias might have existed because of the retrospective nature of this research. Second, this study was based on the results of a single country. Finally, our data set did not include younger patients. Therefore, the results of the present study may not be only specific to the elderly. Despite these limitations, this was the first large-scale study assessing the epidemiology and surgical treatment of CF and/or CSCI in elderly patients in Japan. Hence, the study results are highly indicative of the future healthcare of elderly people worldwide.
Conclusions
The number of elderly patients who sustained CF and/or CSCI and the number of patients who underwent surgery increased significantly. The mean age, distribution of injury levels and paralysis severity, and the rate of surgical indications did not change. Approximately 90% of patients underwent posterior approach surgery. In the late period, the use of screw instrumentation and the range of fusion increased significantly. The incidence of perioperative and other complications and mortality did not significantly differ between the 2 periods. Thus, the number of patients increased significantly over the 10-years period, and the number of instrumentation procedures increased. While appropriate treatment can return the majority of patients to their homes, a high rate of complications still occur.
Supplemental Material
Supplemental Material - Epidemiology of Cervical Fracture/cervical Spinal Cord Injury and Changes in Surgical Treatment Modalities in elderly Individuals During a 10-year Period: A Nationwide Multicenter Study in Japan
Supplemental Material for Epidemiology of Cervical Fracture/cervical Spinal Cord Injury and Changes in Surgical Treatment Modalities in elderly Individuals During a 10-year Period: A Nationwide Multicenter Study in Japan by Philipp Pieroh, Ulrich J.A. Spiegl, Anna Völker, Sven Märdian, Nicolas H. von der Höh, Georg Osterhoff, Christoph-E. Heyde; Spine Section of the German Society for Orthopaedics and Trauma in Global Spine Journal
Footnotes
Acknowledgments
We thank all members of the Japan Association of Spine Surgeons with Ambition (JASA) for collecting the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Thirty-three health care facilities were included in the database. The study protocol was approved by the Institutional Review Board (no. 3352-1) of each of the 25 representative institutions.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.