
Abstract
Study Design
A prospective cohort study.
Objectives
To report a new index, the realigned K-line, for predicting surgical outcomes after laminoplasty in patients with degenerative cervical myelopathy (DCM).
Methods
One hundred twenty-eight patients with DCM undergoing laminoplasty were enrolled from January 2018 to April 2021 in our department. A realigned K-line was defined as the line connecting the midpoints of the spinal cord between C2 and C7 on realigned T1-weighted magnetic resonance imaging. The minimum interval between the anterior compression factors of the spinal cord and the realigned K-line (INTrea), and the modified K-line (INTmod) were measured. A logistic regression analysis was performed to identify factors associated with unsatisfactory surgical outcomes. The receiver operating characteristic (ROC) curve and the area under the curve (AUC) was applied to evaluate the reliability of the multivariate logistic regression model.
Results
Univariate analysis showed that the score for the bladder function section of the Japanese Orthopedic Association Cervical Myelopathy Evaluation Questionnaire, numeric rating scale scores for arm pain, and INTrea might be related to the Japanese Orthopaedic Association (JOA) recovery rate (RR) not achieving the minimal clinically important difference (MCID) (P < .05). Only INTrea (odds ratio = .744, P < .05) was an independent preoperative factor related to the JOA RR not achieving the MCID (area under the curve, .743). A cutoff of 5.0 mm for INTrea had an accuracy of 71.9% and specificity of 80.3% for predicting the JOA RR not achieving the MCID.
Conclusions
INTrea is an independent preoperative risk factor related to the JOA RR not achieving the MCID in patients with DCM. A cutoff point of 5.0 mm is most appropriate for alerting spine surgeons to a high likelihood of the JOA RR not achieving the MCID.
Keywords
Introduction
Laminoplasty is an effective and relatively safe non-fusion operation for the treatment of degenerative cervical myelopathy (DCM), and its long-term neurological recovery is promising.1-7 Laminoplasty mainly drifts the spinal cord backward through a “bow-string effect” based on cervical lordosis, thereby achieving indirect decompression of the compressed spinal cord.8,9
Several preoperative factors have been reported to compromise the efficacy of this indirect decompression.10-13 Preoperative kyphosis and significant anterior compression of the spinal cord, such as cervical disc herniation and ossification of the posterior longitudinal ligament (OPLL), can lead to residual anterior compression of the spinal cord (ACS) after laminoplasty. These studies independently evaluated the 2 aforementioned factors but did not consider their combined effect on postoperative clinical outcomes. Fujiyoshi et al. 14 first analyzed these 2 factors on a neutral lateral radiograph and combined them into 1 parameter, which they named the K-line, that they used to select the surgical approach in patients with OPLL. However, anterior compression factors of the spinal cord, such as intervertebral disc herniation and spur formation, are unclear on plain radiographs.
Magnetic resonance imaging (MRI) is optimal because it has better visibility than plain radiography and can achieve accurate cervical sagittal parameters. Taniyanna et al. 15 reported a modified K-line connecting the midpoint of the spinal cord between C2 and C7 on preoperative T1-weighted MRI (T1MRI). Their results showed that the minimum interval (INTmin) between the modified K-line and anterior compression factors is an important prognostic indicator of postoperative ACS. However, the value of INTmin is easily affected by the curvature of the cervical spine; the study did not include the effects of gravity and load-bearing on cervical curvature, and the Cobb angle on supine MRI scans may be lower than that on plain radiographs.15,16 Moreover, the supine posture with a coil on the neck during MRI may lead to a different curvature of the cervical spine. The advent of upright MRI has made it possible to address these problems. However, upright MRI is a new technique that has not yet become routine compared with conventional MRI, and few imaging centers in the world perform upright MRI. In brief, MRI is still a practical and convenient tool for K-line measurement and may be used for postoperative prediction, but further study is needed for better accuracy. Using plain radiographs as references may be a solution; however, to our best knowledge, there is no reference to sagittal parameters of the cervical spine on plain radiographs in reports of the modified K-line.
Previous studies have reported that Surgimap allows surgeons to simulate sagittal correction and graphically present the expected sagittal alignment.17,18 The present study aimed to report a new index, the realigned K-line, for predicting the surgical outcomes after laminoplasty in patients with DCM and to validate the hypothesis that cervical curvature will affect the measurement of INT.
Methods
Ethics Statements
This study was implemented and reported in line with the Standard Protocol Items: Recommendations for Interventional Trials 2013 Statement. 19 It was also approved by our institutional review board (number: GDREC2017293H). Written informed consent was obtained from all patients before collecting their clinical and radiological information.
Study Design and Population
Patients who underwent laminoplasty under the diagnosis of multilevel DCM and who had complete imaging data were consecutively enrolled in this prospective cohort study from January 2018 to April 2021. The exclusion criteria were as follows: (1) patients with a history of other neurological diseases that may affect their neurological function, such as stroke, Parkinson's disease, or poliomyelitis, and (2) previous cervical surgery. All patients were followed for >1 year. Preoperative MRI and X-ray data, clinical outcome measurements (the Japanese Orthopaedic Association [JOA] score, Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire [JOACMEQ] score, and numeric rating scale (NRS) scores of neck and arm pain) were collected.
Operative Technique
All surgeries were performed by a single senior surgeon. We conducted laminoplasty as described in previous studies.20-22 The patients were operated on in a prone neutral position, and then the C3 to C7 laminae were exposed by dissection of both paracervical muscles through a posterior midline incision. A high-speed air-burr drill was used to create grooves at the junction of the lamina and facet joints, and the ventral cortex of each lamina was cut. Instead of being cut, the ventral cortex of the other lamina was grooved as a hinge, and the cut lamina of the opposite lamina was raised and secured in an expanded position with titanium miniplates and screws. The laminoplasty procedure was plated alone, and no bone graft or fusion equipment was placed on the hinge or open side.
Definition of the Realigned K-line
To draw the realigned K-line, we first realigned the cervical alignment on MRI, with sagittal alignment on an X-ray as a reference. A previous study showed that the midpoints of the spinal cord at C2 and C7 are fixed before and after laminoplasty.
23
Among the intervals between the modified K-line and anterior compression factors of the spinal cord at each segment in the magnetic resonance (MR) image, only the lowest interval (INTmin) was significantly correlated with neurological improvement after laminoplasty.
23
Based on this theory, we selected 3 points on the mid-sagittal MR image as the anchor points for realignment: A. the midpoint of the spinal canal at C2, B. the midpoint of the spinal canal at C7, and C. the posterior edge of the intervertebral space at the most severely compressed segment. Then, we drew 2 lines between AC and BC, and the intersection of these 2 lines created an angle (∠ACB), which correlated with the curvature of the cervical spine. In the same way, we drew the aforementioned 2 lines and the angle (∠A'C'B') on the X-ray of the same patient. We used the simulated osteotomy function of Surgimap software
18
(New York, NY, USA) to process the MR image into a realigned MRI scan so that the included angle between the realigned MRI (∠ACB) was equal to that angle on the X-ray (∠A'C'B'). Therefore, the relative positional relationship within the 3 anchor points was similar between the realigned MRI scan and preoperative X-ray. Finally, we drew a K-line on the realigned MRI scan as previously described and called it the “realigned K-line.” Based on the realigned K-line, we defined INTrea as the minimum interval between the realigned K-line and anterior compression factors on the realigned MRI scan (Figure 1(A)-(C)). Schematic drawings of the “realigned K-line.” A: The most severely compressed segment is C5/6 on MRI. The 3 anchor points are as follows: A) the midpoint of the spinal canal at C2, B) the midpoint of the spinal canal at C7, and C) the posterior edge of the intervertebral space at the most severely compressed segment. The intersection of line AC and line BC forms an angle (∠ACB). The modified K-line is defined and the INTmod is measured. B: In the same way, draw the 2 aforementioned lines and the angle (∠A'C'B') on the X-ray of the same patient. C: A simulated osteotomy is performed on the T1MRI using Surgimap software (we refer to the MRI scan after a simulated osteotomy as the “realigned MRI scan”) so that the ∠ACB on the realigned MRI scan is equal to the ∠A'C'B' on the X-ray. The realigned K-line is defined and the INTrea is measured. The C2-7 lordosis angle (CL, the cobb angle between the inferior endplate of C2 to the inferior endplate of C7) was measured on MRI, radiography, and realigned MRI, respectively. MRI, magnetic resonance imaging; T1MRI, T1-weighted magnetic resonance imaging; INTrea, the minimum interval between the realigned K-line and anterior compression factor; INTmod, the minimum interval between the anterior compression factors of the spinal cord and the modified K-line.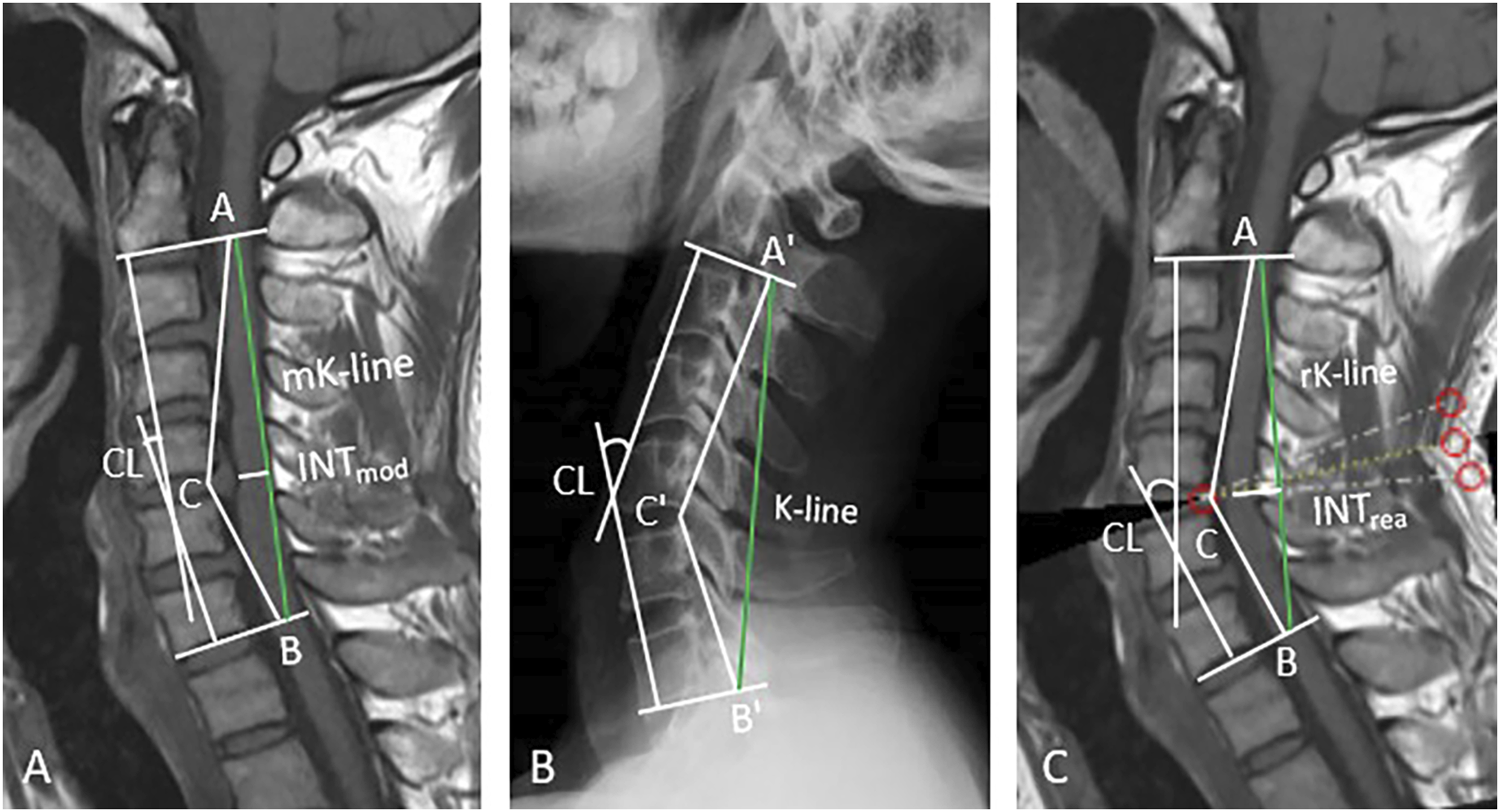
Measurements
Radiological Measurements
We created a realigned MRI scan with all preoperative MRI scans, and INTrea and INTmod were measured. The cervical lordotic angle (C2–C7 Cobb angle) was measured using radiography, MRI, and realigned MRI to confirm the efficacy of this method. Moreover, INTrea was measured separately on 50 randomly selected realigned MRI scans by 2 independent spine surgeons to evaluate inter-observer reliability, and then 1 of the observers analyzed the remaining images. The same observer measured INTrea twice on 50 randomly selected realigned MRI images, at 2-week intervals, to evaluate intra-observer reliability.
There are 2 ways to measure the INTrea. The first method is to realign at the most severely compressed segment on the mid-sagittal MRI, copy the relative position relationship between the K-line and the posterior edge of intervertebral space at the most severely compressed segment from radiography to MRI, and then measure INTrea. The second method is to realign the cervical curvature at each segment on the mid-sagittal MRI to restore the true cervical curvature, and then measure INTrea. The first method is simple and can obtain the relative position relationship between the K-line and the posterior edge of the intervertebral space at the most severely compressed segment, making the measurement of INTrea more accurate than the second method. The second method can better restore cervical curvature, but it is more complex than the first method. We randomly selected 50 patients to compare the 2 methods. (Supplementary File 1, Fig 1).
Clinical Measurements
The JOA score, JOACMEQ score, and NRS scores of neck and arm pain were used to evaluate the neurological outcomes before and after laminoplasty. The JOA recovery rate (RR) was evaluated using the Hirabayashi method as follows: RR = [postoperative JOA score – preoperative JOA score]/[17–preoperative JOA score] × 100%. 24 The JOACMEQ defines effective treatment as when (1) the post-treatment score increases by ≥ 20 points compared to the pretreatment score, or (2) the pretreatment score is < 90 points and the post-treatment score is ≥ 90 points. Patients with pre-and post-treatment scores ≥90 were excluded from further analysis. 25 The efficacy rate was calculated as follows: [(number of patients judged “effective”)/[(total number of patients in the group) − (number of patients whose pre- and post-treatment scores are both ≥90)].
The minimal clinically important difference (MCID) was defined as the smallest change that can be recognized as “clinically meaningful” by a patient, to evaluate the success of interventions. A previous study demonstrated that the minimum clinically important recovery rate was 52.8%. 26 In this study, we used 52.8% as a reference criterion to measure whether the changes in the JOA scores were significant enough to make a clinical difference. The patients were classified into 2 groups: the JOA RR achieved the MCID (minimal change group) and JOA RR did not achieve the MCID (no change group). We also evaluated the therapeutic effect based on whether the changes in JOACMEQ scores met the criteria for effective treatment.
Statistical Analysis
Numerical variables are described as mean ± standard deviation (SD), and the differences were analyzed using a Student's t-test. Categorical variables are shown as frequencies and percentages, and differences were compared using the Pearson’s chi-squared test or Fisher’s exact test. Multivariate logistic regression analysis was performed to identify potential independent preoperative factors correlated with the JOA RR not achieving the MCID. Preoperative factors with P-values < .1 in univariate analyses were entered into the multivariate analysis. The intraclass correlation coefficient (ICC) was calculated to evaluate the inter-observer and intra-observer reliabilities of INTrea. A receiver operating characteristic (ROC) curve was used to measure the reliability of the multivariate logistic regression model. The area under the ROC curve (AUC) was used to test the overall ability of the multivariate logistic regression model to predict the JOA RR not achieving the MCID.
The minimum sample size for this study was 70, according to Flahault et al. (with a sensitivity and specificity of 90% and consideration that the lower 95% confidence limit should not be < .75). 27 Owing to the small amount of missing data, no imputation was performed.
All statistical analyses were performed using SPSS statistical software, version 26 (IBM Corp, Armonk, NY, USA). Statistical significance was defined as a P-value < .05.
Results
Characteristics of the study Participants
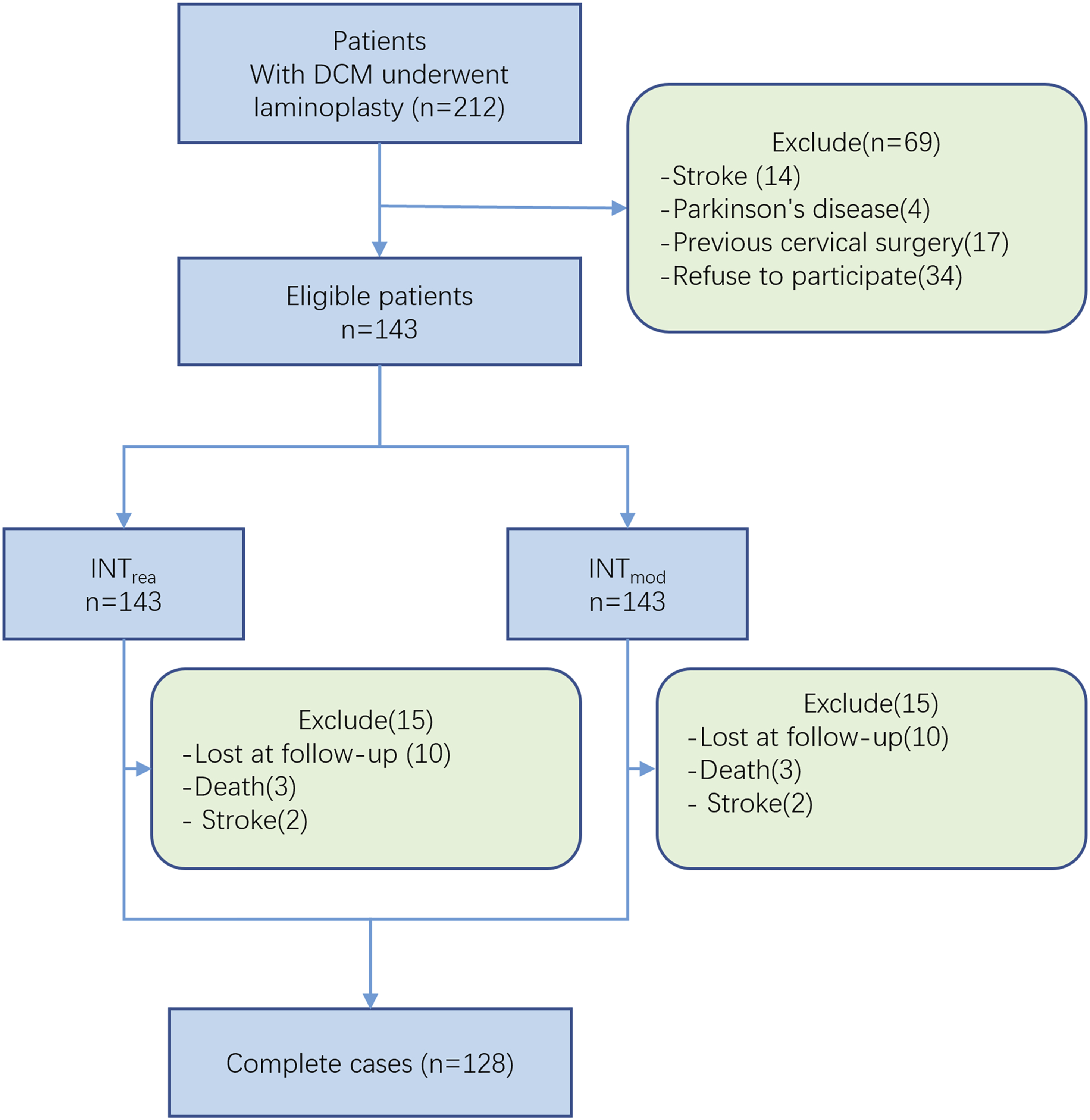
A total of 143 patients who met the inclusion criteria during the study period were enrolled. During the follow-up period, 3 patients died and 2 had a stroke after surgery. Another 10 patients were lost to follow-up. Thus, 15 patients were excluded, leaving 128 patients for the primary analysis (Figure 2). Table 1 shows the patients’ baseline demographic and clinical characteristics. Flow-chart of patient inclusion. Baseline demographic and clinical characteristics of the 128 patients.
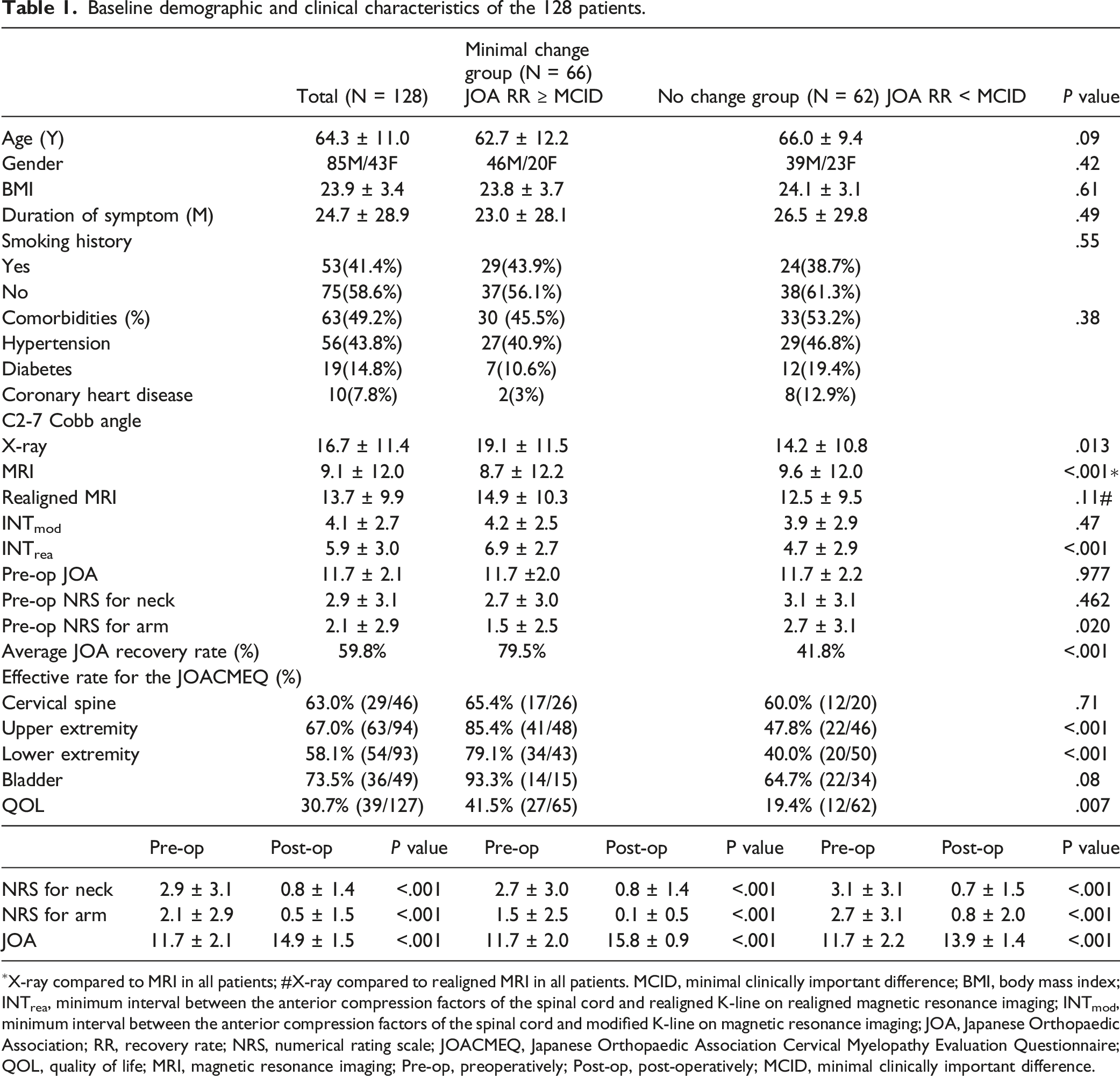
The study population of 128 patients included 85 men (66.4%), with a mean (±SD) age of 64.32 (±11.0) years. Sixty-six patients (51.6%) who achieved the MCID were classified into the minimal change group and 62 patients (48.4%) who did not achieve the MCID were classified into the no change group. None of the patients had worse neurological outcomes postoperatively than preoperatively. The C2–C7 Cobb angles were found to be nearly equivalent between the realigned MRI and X-ray images and were strongly correlated (r = .953, P < .0001).
Reliability of the Realigned K-line
Inter- and intra-observer reliabilities for the INTrea measurements.
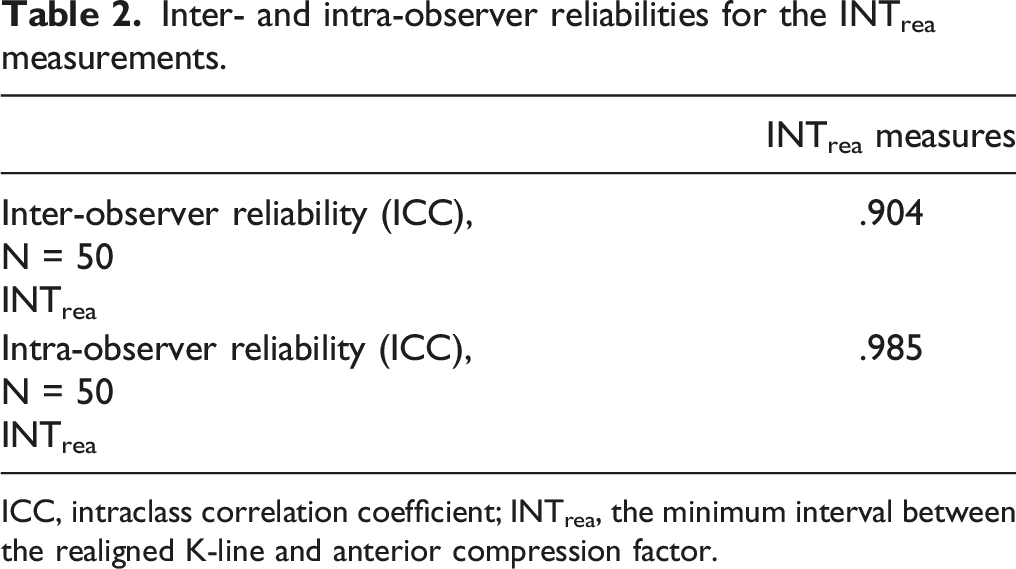
ICC, intraclass correlation coefficient; INTrea, the minimum interval between the realigned K-line and anterior compression factor.
Additionally, we found no significant difference in the INTrea values and C2-7 Cobb angles obtained by realigning at the most severely compressed segment and realigning the cervical curvature at each segment. However, it is simpler to realign at the most severely compressed segment than at each segment, and a relative position relationship between the K-line and the posterior edge of the intervertebral space at the most severely compressed segment can be obtained. Therefore, our method of realigning at the most severely compressed segment is simple and feasible (Supplementary File 2, Table 1).
Relationship between preoperative factors and the JOA RR not achieving the MCID
Regarding prognostic indicators of clinical outcomes after laminoplasty, our results revealed that INTrea was significantly correlated with the JOA RR. Univariate analyses showed that there were significant differences between the 2 groups regarding the C2-7 Cobb angle on radiography, score of the bladder function section of the JOACMEQ, preoperative NRS score for arm pain, and INTrea (all, P < .05).
Results of logistic regression analysis of the preoperative risk factors for the JOA RR not reaching the MCID.
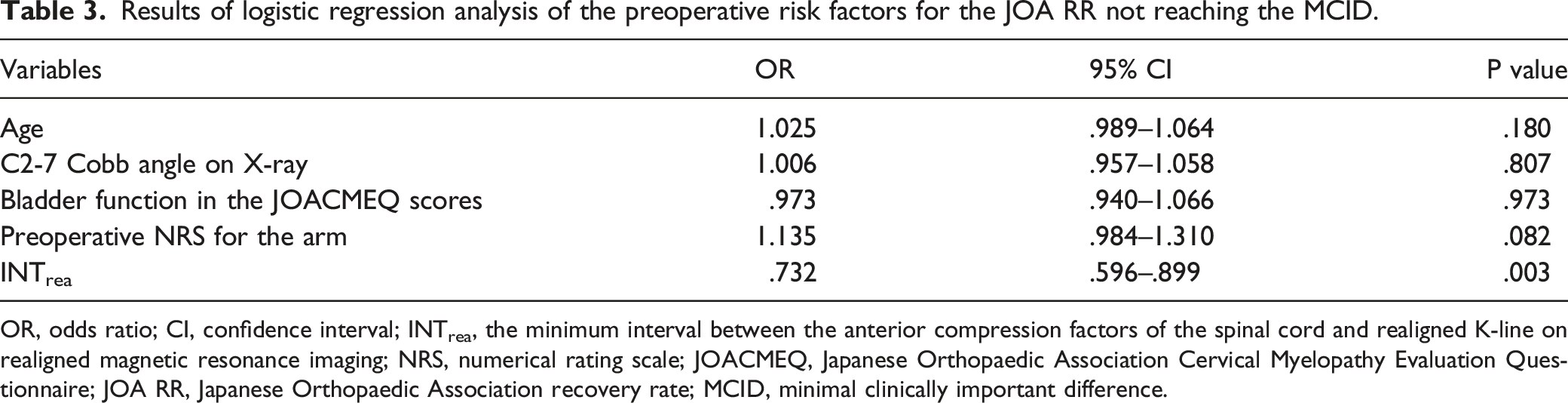
OR, odds ratio; CI, confidence interval; INTrea, the minimum interval between the anterior compression factors of the spinal cord and realigned K-line on realigned magnetic resonance imaging; NRS, numerical rating scale; JOACMEQ, Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire; JOA RR, Japanese Orthopaedic Association recovery rate; MCID, minimal clinically important difference.
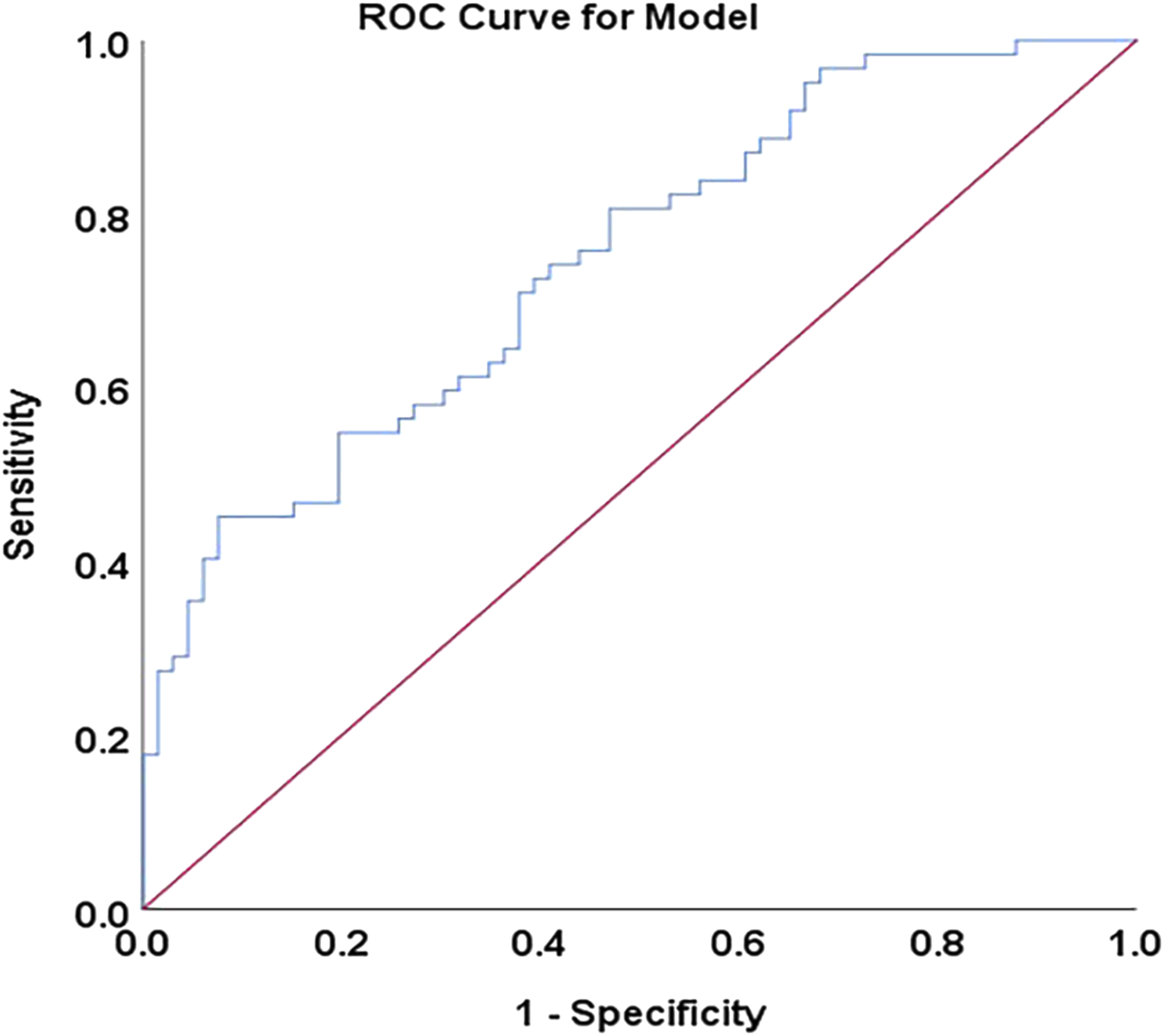
ROC curve of the multivariate logistic regression model. The AUC of .745 indicates a fair ability to discriminate the JOA RR not reaching the MCID. ROC, receiver operating characteristic; AUC, area under the receiver operating characteristic curve; JOA, Japanese Orthopaedic Association; RR, recovery rate; MCID, minimal clinically important difference.
Moreover, the ROC curve analysis for INTrea showed an AUC of .718 (95% confidence interval [CI] = .628-.807, P < .001; Supplementary File 1, Figure 2). The cut-off value of INTrea for the JOA RR not achieving the MCID was 5.0 mm, with a sensitivity of 62.9% (95% CI = 49.7%–74.6%), specificity of 80.3% (95% CI = 68.3%–88.7%), positive predictive value of 75.0% (95% CI = 60.8%–85.5%), and negative predictive value of 69.7% (95% CI = 58.0%–79.5%).
Regarding the postoperative clinical outcomes, we found that 66 patients (51.6%) achieved the MCID. Seventy-six (59.5%) patients had an INTrea value ≥5.0 mm. Compared with patients with an INTrea value >5.0 mm, patients with an INTrea <5.0 mm had a higher risk of the JOA RR not achieving the MCID after laminoplasty (OR: 6.913, 95% CI = 3.119-15.323, P < .001; Supplementary File 2, Table 2).
We also investigated the predictive performance of INTrea for effective treatment after surgery based on whether the changes in the JOACMEQ scores met the criteria for effective treatment. ROC curve analysis of INTrea showed that INTrea could predict ineffective treatment of upper extremity function, with an AUC of .748 (95% CI = .659-.836, P < .001; Supplementary File 1, Figure 3).
Discussion
To our knowledge, this is the first study to realign the cervical curvature on MRI by simulating osteotomy, measuring the sagittal parameters, and discussing the relationship between these parameters and the surgical outcomes after laminoplasty. The major result of the present study was finding that INTrea may be an independent preoperative factor related to the JOA RR not reaching the MCID. In addition, we confirmed the hypothesis that the measurement of INT on mid-sagittal MRI requires the addition of true curvature information of the cervical spine.
The postoperative prognosis of patients treated with laminoplasty for DCM can be affected by various clinical factors.28-32 To better predict the clinical efficacy of laminoplasty, Fujiyoshi et al. 14 developed the K-line on lateral neutral radiographs. However, anterior compression factors of the spinal cord such as intervertebral disc herniation and spur formation, are poorly visible on plain radiographs. 23 In contrast, MRI has better visibility than plain radiographs and can accurately measure cervical sagittal parameters. Taniyanna et al. 15 developed a modified K-line on T1MRI and demonstrated that an INTmin value of 4.0 mm can predict residual anterior compression of the spinal cord after laminoplasty with 80% sensitivity and 80.6% specificity.
Although MRI offers better soft tissue imaging than plain radiography, it is rarely able to maintain the cervical spine in a neutral position during MRI, and the cervical curvature can easily change when patients move from an upright position to a supine position. Moreover, the supine posture with a coil on the neck during MR may lead to a different curvature of the cervical spine. An abnormal cervical curvature will not only compromise the effect of indirect decompression but also affect the minimum interval value and thus the accuracy of its prediction of postoperative clinical efficacy. Taniyanna et al. 15 also found an effect of the aforementioned factors on the cervical curvature. They believe that there was a significant correlation between the C2–C7 Cobb angle on MRI and that on plain radiography; therefore, their findings were not affected. However, a recent study reported that despite the significant correlation between the C2–C7 Cobb angle on supine MRI and that on plain radiography, the mean measurement of the C2–C7 Cobb angle was still statistically different between MRI and plain radiography. 33 Several studies have reported that supine MRI is not a substitute for plain radiography for assessing cervical alignment.16,34,35 Our study also revealed that the mean C2–C7 Cobb angle was different between radiography and MRI. The advent of upright MRI has made it possible to address these problems. However, upright MRI is a new technique that has not yet become routine compared with conventional MRI, and few imaging centers in the world perform upright MRI. In short, MRI is a practical and convenient tool for K-line measurement and may be used for postoperative prediction, but further study is still needed for better accuracy. To consider the influence of gravity and load bearing on cervical curvature while eliminating the effect of neck coil on cervical curvature, we realigned the cervical curvature on MRI by simulating osteotomy with the X-ray as a reference, so that the cervical curvature on the realigned MRI scan was similar to the cervical curvature on the radiograph. The results revealed that the C2–C7 Cobb angle was nearly equivalent between the realigned MRI scan and X-ray.
Next, we developed a realigned K-line on the realigned MRI and measured the minimum interval between the realigned K-line and anterior compression factors (INTrea). We then analyzed the relationship between preoperative factors and postoperative clinical outcomes. Based on the univariate analysis, we found that patients whose JOA RR did not reach the MCID tended to have a smaller preoperative C2-7 angle, smaller INTrea, worse bladder function according to the JOACMEQ score, and higher NRS score for arm pain. This result was similar to that of existing studies, where the minimum interval was significantly associated with the JOA RR.15,23,36 To investigate the independent preoperative factors for predicting the JOA RR not reaching the MCID, we conducted a multivariate logistic regression analysis, which revealed that only INTrea was a significant factor. To test the reliability of the multivariate logistic regression model, we used the ROC curve and its AUC, which could assess the ability of this model to predict the JOA RR not reaching the MCID. Our model showed an AUC of .746, indicating fair discrimination ability. Previous studies have shown that a prediction model would be considered reasonable with a value of >.7. 37 We analyzed the relationship between the preoperative INTrea value and JOA RR to assess what values of INTrea are best to prevent the JOA RR from not reaching the MCID. Based on the receiver operating characteristic curve, a cutoff value of 5.0 mm was found to predict the JOA RR not achieving the MCID. The result reveals that an INTrea value <5.0 mm may be a risk factor for the JOA RR not achieving the MCID. Compared with patients with an INTrea value >5.0 mm, patients with an INTrea value <5.0 mm had a higher risk of the JOA RR not achieving the MCID. Moreover, our results revealed that INTrea can predict ineffective treatment of upper extremity function based on the JOACMEQ score.
This study found that INTrea was an independent preoperative factor related to the JOA RR not reaching the MCID, but INTmod had no significant correlation with the postoperative JOA RR. However, Taniyanna et al. 23 believed that INTmin was closely related to the JOA RR after surgery. We believe that the reason for this difference is that we restored the true curvature of the cervical spine on MRI by referring to the X-ray before measuring INTrea. The intra- and inter-observer reliabilities of the INTrea measurement on realigned MRI were substantial, supporting that the INTrea measurement is a reliable and reproducible means of communication between different observers. Therefore, we suggest that clinicians restore the true cervical curvature on MRI before measuring the sagittal parameters used to predict clinical outcomes after laminoplasty. Realigning the cervical curvature by simulating osteotomy is a simple and easy method.
Our study has several limitations. Firstly, this was a single-center prospective study with a small number of patients. Therefore, a multicenter prospective study with a larger sample size is needed to further clarify the validity and practicability of INTrea for predicting the clinical outcomes of patients with DCM after laminoplasty. Second, owing to the different imaging principles of MRI and radiography, the magnification of the images is also different. The lines from the midpoint of C2 to the posterior edge of the intervertebral space at the most severely compressed segment and from the midpoint of C7 to the posterior edge of the intervertebral space at the most severely compressed segment could not be made identical on realigned MRI and radiography. However, because a significant correlation between the 2 lines on realigned MRI and radiography was observed in this series, the findings may still be considered significant (Supplementary File 3). Third, this study focused on the predictive performance of INTrea for clinical outcomes after laminoplasty. Furthermore, the most severely compressed segment on MRI does not always correspond to that responsible for cervical myelopathy. Therefore, we did not assess the predictive performance of INTrea for inadequate decompression of the segment responsible for cervical myelopathy. We will conduct further research on this aspect.
Conclusions
This study’s results suggest that INTrea may be an independent preoperative risk factor related to the JOA RR not achieving the MCID in patients with DCM. A more satisfactory clinical effect will be obtained after laminoplasty in DCM patients with an INTrea value >5.0 mm. On this basis, the realigned K-line may inform clinical decision-making and guide individualized treatments for DCM.
Supplemental Material
Supplemental Material - Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy
Supplemental Material for Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy by Qifei Duan, Guoyan Liang, Chong Chen, Yongyu Ye, Xiaoqing Zheng, Changxiang Liang and Yunbing Chang in Global Spine Journal
Supplemental Material
Supplemental Material - Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy
Supplemental Material for Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy by Qifei Duan, Guoyan Liang, Chong Chen, Yongyu Ye, Xiaoqing Zheng, Changxiang Liang and Yunbing Chang in Global Spine Journal
Supplemental Material
Supplemental Material - Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy
Supplemental Material for Accuracy of Realigned K-line for Predicting Surgical Outcomes After Laminoplasty in Patients With Degenerative Cervical Myelopathy by Qifei Duan, Guoyan Liang, Chong Chen, Yongyu Ye, Xiaoqing Zheng, Changxiang Liang and Yunbing Chang in Global Spine Journal
Footnotes
Acknowledgments
We thank Ke’er Wang for contributing to data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr. Guoyan Liang has received funding from the Guangdong Provincial Traditional Chinese Medicine Research Project (20221001) and Guangdong Provincial Medical Science and Technology Research Fund Project (B2022059). Dr. Chong Chen has received funding from the National Natural Science Foundation of China (82102636), Basic and Applied Basic Research Foundation of Guangdong Province (2020A1515110545), Guangzhou Municipal Science and Technology Project (202102020100) and Guangdong Medical Research Foundation (A2021301). Dr. Yunbing Chang has received funding from the Natural Science Foundation of Guangdong Province (2022A1515012557) and Guangzhou Science and Technology Program Key Projects (202103000053).
Ethical Approval
The Research Ethics Committee of the institute approved this investigation [No.GDREC2017293H] and all investigations were conducted in conformity with ethical principles of research.
Availability of Data
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.