
Abstract
Study Design
Single-center retrospective cohort study
Objectives
Type II odontoid fractures occur disproportionately among elderly populations and cause significant morbidity and mortality. It is a matter of debate whether these injuries are best managed surgically or conservatively. Our goal was to identify how treatment modalities and patient characteristics correlated with functional outcome and mortality.
Methods
We identified adult patients (>60 years) with traumatic type II odontoid fractures. We used multivariate regression controlling for patient demographics, Glasgow Coma Scale (GCS) score, Charlson Comorbidity Index (CCI), modified Rankin Scale (mRS) score, modified Frailty Index (mFI-5 and mFI-11), fracture displacement, and conservative vs operative treatment.
Results
Of the 59 patients (mean age 77.9 years), 24 underwent surgical intervention and 35 underwent conservative management. Operatively managed patients were younger (73.4 vs 80.6 years, P < .001) and had higher degree of fracture displacement (3.5 vs 1.0 mm, P = .002) than conservatively managed patients but no other differences in baseline characteristics. Twenty-four patients (40.7%) died within the study period (median time to death: 376 days). There were no differences between treatment groups in functional outcomes (mRS or Frankel Grade) or mortality (33.3% in operative group vs 45.7%, P = .34). There was a statistically significant correlation between higher presentation mRS score and subsequent mortality on multivariate analysis (OR = 2.06, 95% CI 1.04-4.10, P = .039), whereas surgical intervention, age, GCS score, CCI, mFI-5, mFI-11, sex, and fracture displacement were not significantly correlated.
Conclusions
Mortality after type II odontoid fractures in elderly patients is common. mRS score at presentation may help predict mortality more accurately than other patient factors.
Introduction
The incidence of cervical fractures is biphasic in distribution, most commonly affecting individuals between 20 and 30 or 70 and 80 years old.1-3 In the younger population, high-energy trauma is the most common cause, whereas the elderly are susceptible to low-energy trauma due to age-related changes in bone density. Of all cervical spine injuries in older patients, C2 fractures are the most common, with type II odontoid fractures of the Anderson D’Alonzo Classification 4 representing the most prevalent subtype.1,5,6
Type II odontoid fractures occur at the base of the odontoid process and are inherently unstable. These injuries disproportionately affect the elderly population, who are at higher risk of subsequent morbidity and mortality. 7 Globally, there is an expected increasing life expectancy over the next decades with the population of individuals over 80 years old in North America alone anticipated to double by 2050. 8 As these numbers rise, the incidence of these fractures will increase. Thus, developing an appropriate treatment algorithm is essential. Despite the relatively common nature of these injuries, there continues to be debate as to whether Type II odontoid fractures are best managed surgically or conservatively in this elderly population.
Expected functional status and mortality are vital considerations when contemplating treatment options and selecting surgical candidates. Various scores such as the Charlson Comorbidity Index (CCI), 9 modified Rankin Scale (mRS) score, 10 and modified Frailty Index (mFI-5 and mFI-11)11,12 have been developed to stratify a patient’s condition, aid in determining a patient’s candidacy for surgery, and predict outcome. We, therefore, performed a retrospective review that included patient demographics, treatment modality, and multiple patient comorbidity and frailty indices, which were then controlled for in a multivariate model to identify factors associated with functional outcome and mortality.
Methods
Study Design and Patient Population of Interest
After receiving institutional review board approval with a waiver of informed consent (IRB#115230), we performed a retrospective single-institution cohort study comprising tertiary-care hospital record data from August 2015 to July 2020. Health records, including death reports, were available for at least 2 years after presentation for each patient. Clinical and radiographic follow-up ranged from 2 days (in the case of in-hospital death) to 4.3 years. Patients included for analysis were over the age of 60 years with traumatic type II odontoid fractures as defined by the Anderson and D’Alonzo classification method. 4 Variables of interest relating to fracture presentation included patient age at presentation, mechanism of injury, sex, body mass index (BMI), fracture displacement (category and distance of displacement), operative intervention related to odontoid fracture, and neurologic deficit at presentation. Fifty-nine patients met criteria for inclusion and were categorized into 2 groups based on operative or nonoperative management. Twenty-four patients were treated operatively while 35 were treated with conservative measures. Patients who were initially treated nonoperatively but went on to surgery were evaluated in the “conservatively managed” group throughout the study. The STROBE guidelines were used for reporting of this study.
Functional Status and Comorbidity/Frailty Variables of Interest
Functional status and comorbidity variables of interest included presenting mRS score, CCI, Glasgow Coma Scale (GCS) score, and mFI-5 and -11. The CCI is a validated measure of patient comorbidity 9 that has been used previously to predict mortality after odontoid fractures in the elderly.13-15 The mFI-5 11 and mFI-11 16 are validated frailty indices developed from the American College of Surgeons National Surgical Quality Improvement Program database to predict mortality after surgical procedures; these have been used previously to assess frailty in elderly patients with odontoid fracture.17,18
Outcomes of Interest
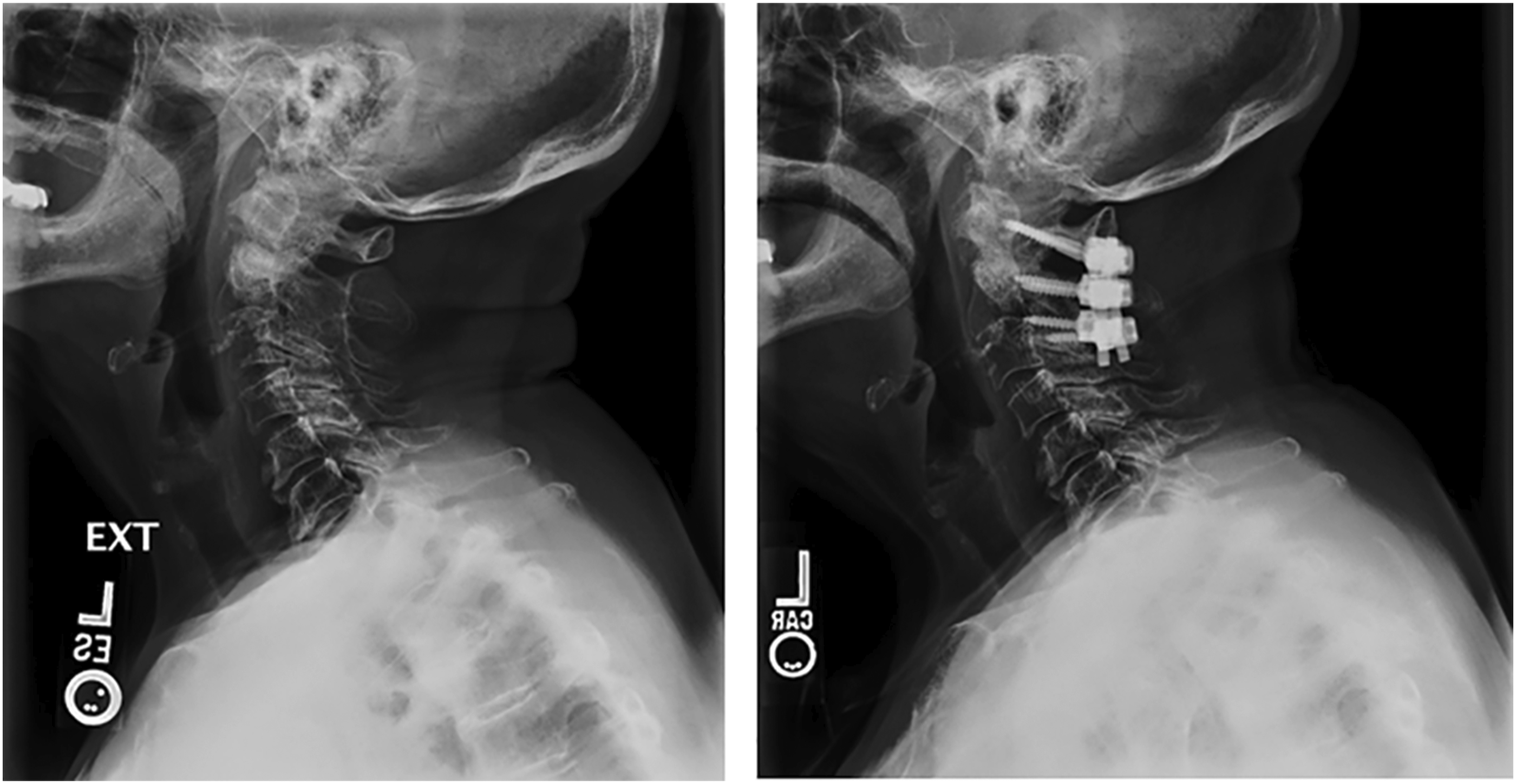
Outcomes of interest were obtained at different follow-up intervals based on available hospital documentation. Mortality was determined for all patients >2 years after initial presentation as summarized by hospital and death records and did not rely on neurosurgical follow-up. Clinical outcomes were obtained from neurosurgery clinic notes. Patients with imaging obtained more than 30 days postoperatively were assessed for radiographic fracture stability relative to the initial imaging, which was defined as no new odontoid displacement or abnormal motion on radiographic imaging (Figures 1 and 2). Fourteen patients did not have repeat imaging more than 30 days after presentation and were therefore excluded from the fracture stability analysis (median imaging follow-up duration 116 days, IQR 249). Radiographic findings of stability were corroborated with the surgeon’s imaging interpretation recorded in final clinic follow-up notes. Other outcomes of interest included related readmission, discharge disposition, Clavien Dindo score
19
at most recent clinic follow-up for patients who underwent surgical intervention, need for intensive care unit (ICU) stay, length of stay, Frankel grade
20
at last clinic follow-up, and post-intervention chronic pain and chronic opioid use. Lateral cervical x-rays from an 84-year-old woman who presented after a ground-level fall and was found to have a displaced, unstable type II odontoid fracture. She was managed in a collar and was determined to have achieved a stable nonunion at final radiographic follow-up. Left panel: lateral cervical x-ray obtained on presentation. Right panel: x-rays obtained after 12 weeks in a cervical collar. Lateral cervical x-rays from an 82-year-old woman who presented after a ground-level fall and was found to have a displaced type II odontoid fracture. She was treated with a C1-C3 posterior spinal fusion and achieved a stable bony fusion at final radiographic follow-up. Left panel: preoperative lateral cervical x-ray. Right panel: postoperative lateral cervical x-ray demonstrating bridging bone within previous fracture site, suggesting fusion.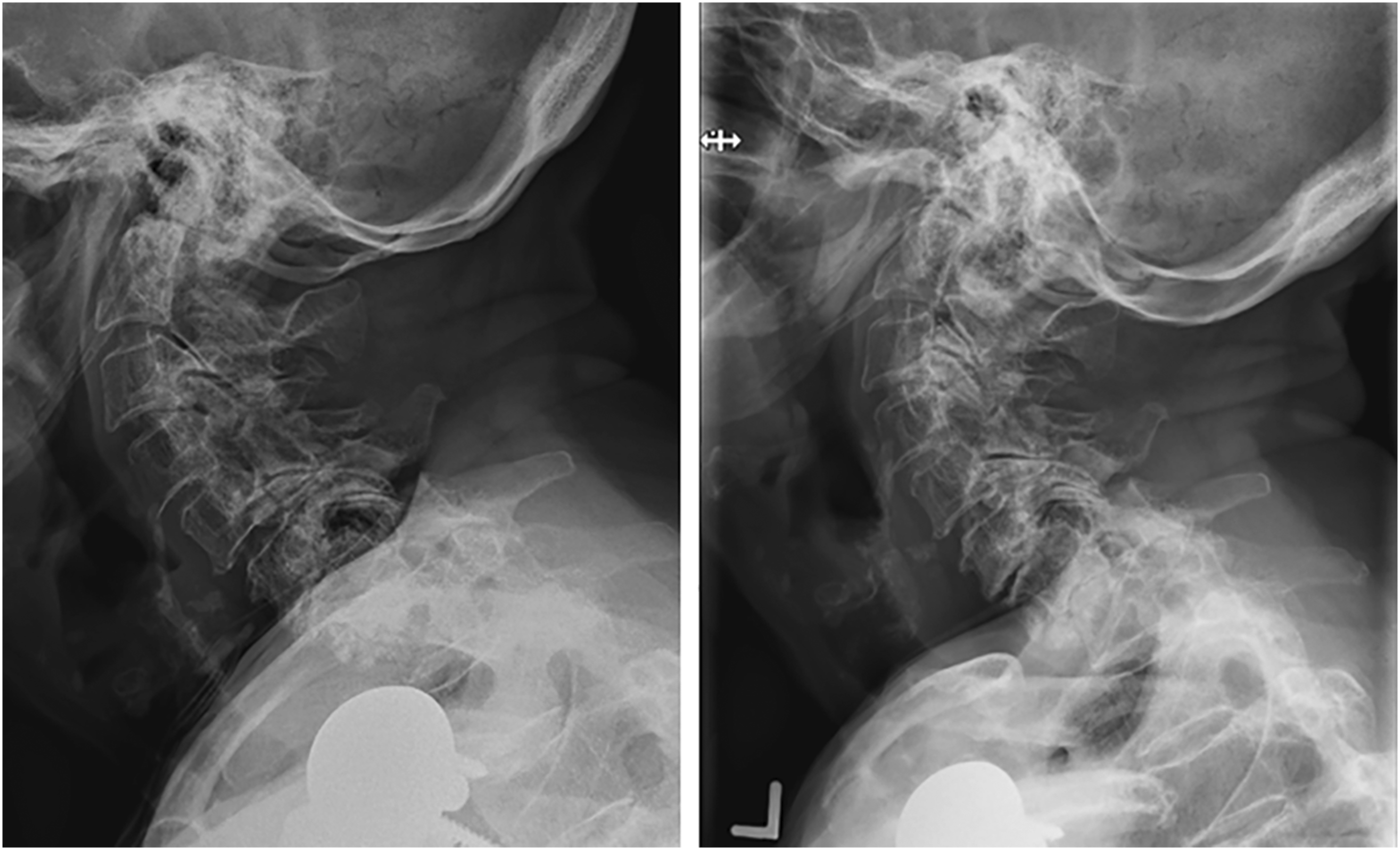
Statistical Analysis
Descriptive statistics were performed for all baseline patient characteristic variables, with categorical variables expressed as n (%) and continuous variables expressed as mean ± standard deviation (SD). A univariate analysis was performed to compare patients undergoing operative vs nonoperative fracture management. Patients <75 and ≥75 years of age were also compared using a univariate analysis. In both univariate analyses, Fisher’s exact test was used for categorical variables, and Student’s t-test was used for continuous variables. Variables that were independently associated with mortality at last clinical follow-up were identified with a multivariate binary logistic regression analysis. A receiver operating characteristic (ROC) curve was generated to assess model predictive power with calculation of the corresponding area under the curve (AUC). Alpha for significance was set to P < .05. All analyses were performed using SPSS v. 27 (IBM, Armonk, NY).
Results
Demographic and Comorbidity Variables for the Whole Cohort.
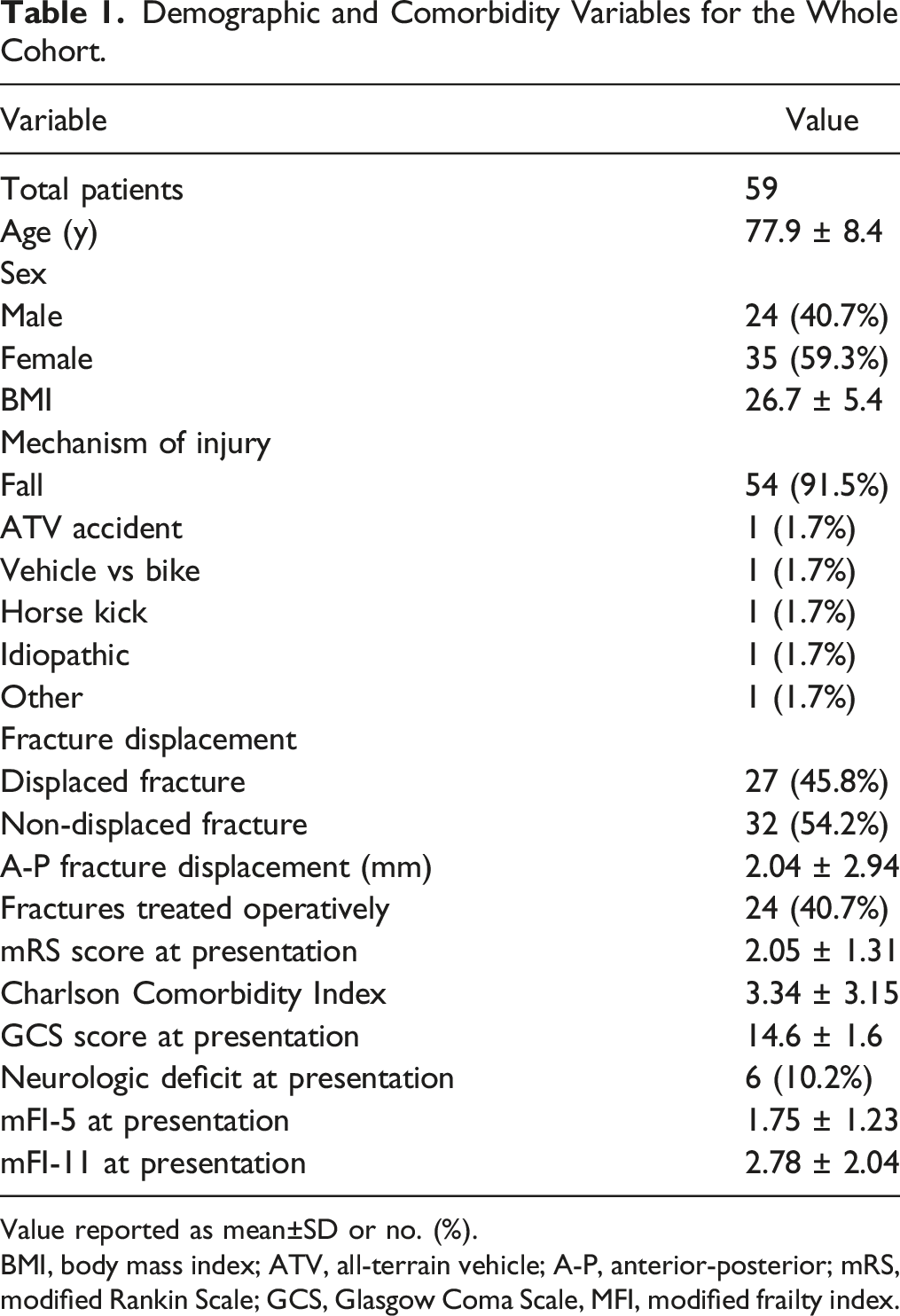
Value reported as mean±SD or no. (%).
BMI, body mass index; ATV, all-terrain vehicle; A-P, anterior-posterior; mRS, modified Rankin Scale; GCS, Glasgow Coma Scale, MFI, modified frailty index.
Outcome Variables for the Entire Cohort.
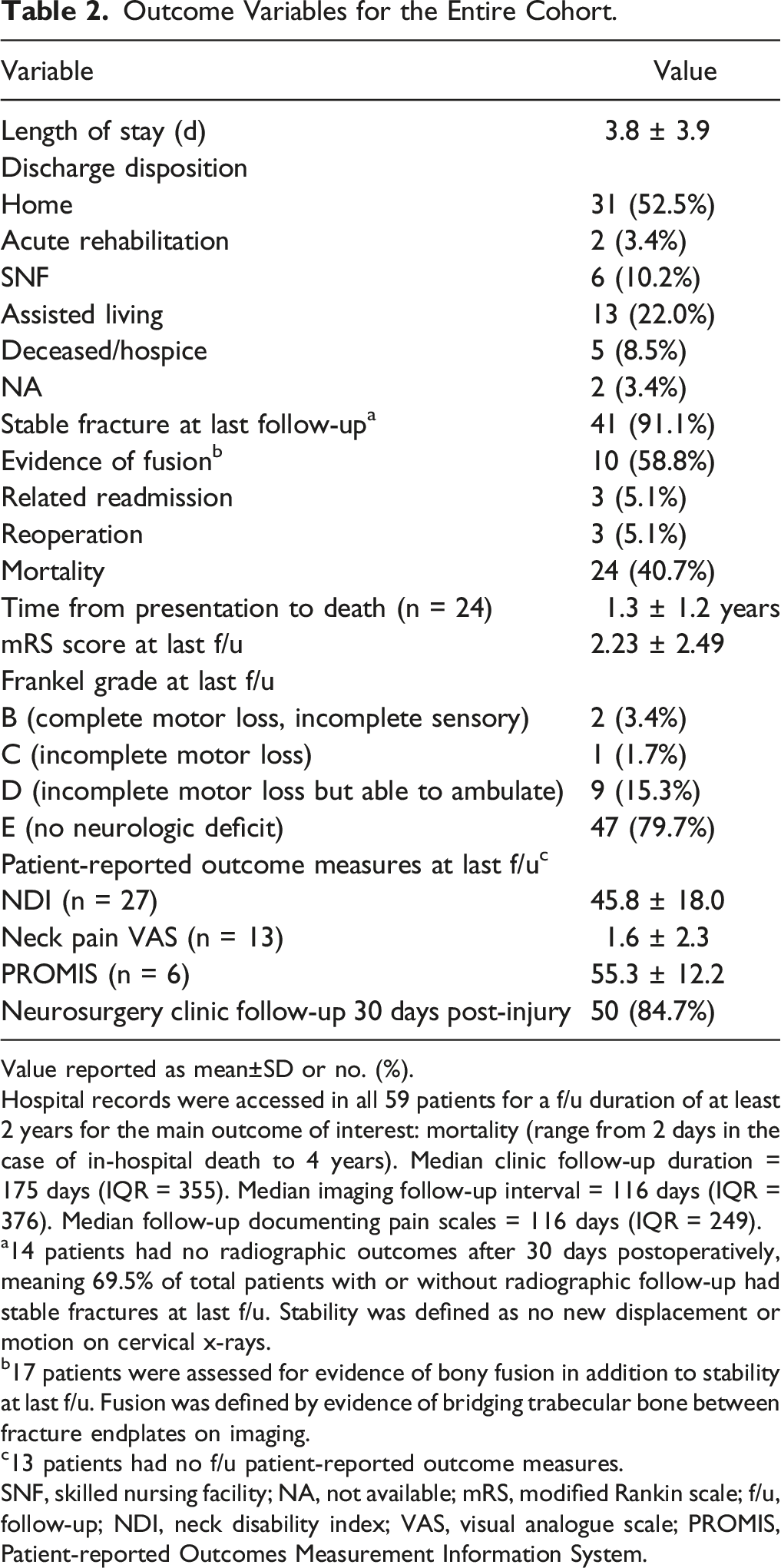
Value reported as mean±SD or no. (%).
Hospital records were accessed in all 59 patients for a f/u duration of at least 2 years for the main outcome of interest: mortality (range from 2 days in the case of in-hospital death to 4 years). Median clinic follow-up duration = 175 days (IQR = 355). Median imaging follow-up interval = 116 days (IQR = 376). Median follow-up documenting pain scales = 116 days (IQR = 249).
14 patients had no radiographic outcomes after 30 days postoperatively, meaning 69.5% of total patients with or without radiographic follow-up had stable fractures at last f/u. Stability was defined as no new displacement or motion on cervical x-rays.
17 patients were assessed for evidence of bony fusion in addition to stability at last f/u. Fusion was defined by evidence of bridging trabecular bone between fracture endplates on imaging.
13 patients had no f/u patient-reported outcome measures.
SNF, skilled nursing facility; NA, not available; mRS, modified Rankin scale; f/u, follow-up; NDI, neck disability index; VAS, visual analogue scale; PROMIS, Patient-reported Outcomes Measurement Information System.
Three patients (5.1%) had a related readmission. One patient treated with rigid bracing fell without his collar, leading to reinjury of his neck three months after initial presentation. Two surgical patients had a related readmission: one presented three months postoperatively with hardware failure and the second returned within 30 days for altered mental status thought to have occurred in the setting of postoperative medications. The patient who experienced hardware failure underwent reoperation. Two patients (5.7%) who were initially managed conservatively underwent subsequent operative intervention for treatment failure in the form of ongoing clinically significant fracture instability. According to institutional and outside records, 24 patients (40.7%) died. Death occurred at an average of 1.3 years after initial presentation for these 24 patients. At last clinical follow-up, the majority of patients had no neurologic deficit (79.7%), and 15.3% were at least able to ambulate. Thirty-nine (66.1%) patients in our cohort had standardized pain scales recorded at a median of 116 days (IQR = 249) postoperatively. The average neck disability index was 45.8 (SD ± 18; n = 27), mean neck pain visual analog scale score was 1.6 (SD ± 18; n = 13), and mean Patient-Reported Outcomes Measurement Information System (PROMIS) form v1.0 pain interference score was 55.3 (SD ± 18; n = 6).
Comparison of Characteristics for Operatively vs Nonoperatively Managed Patients.
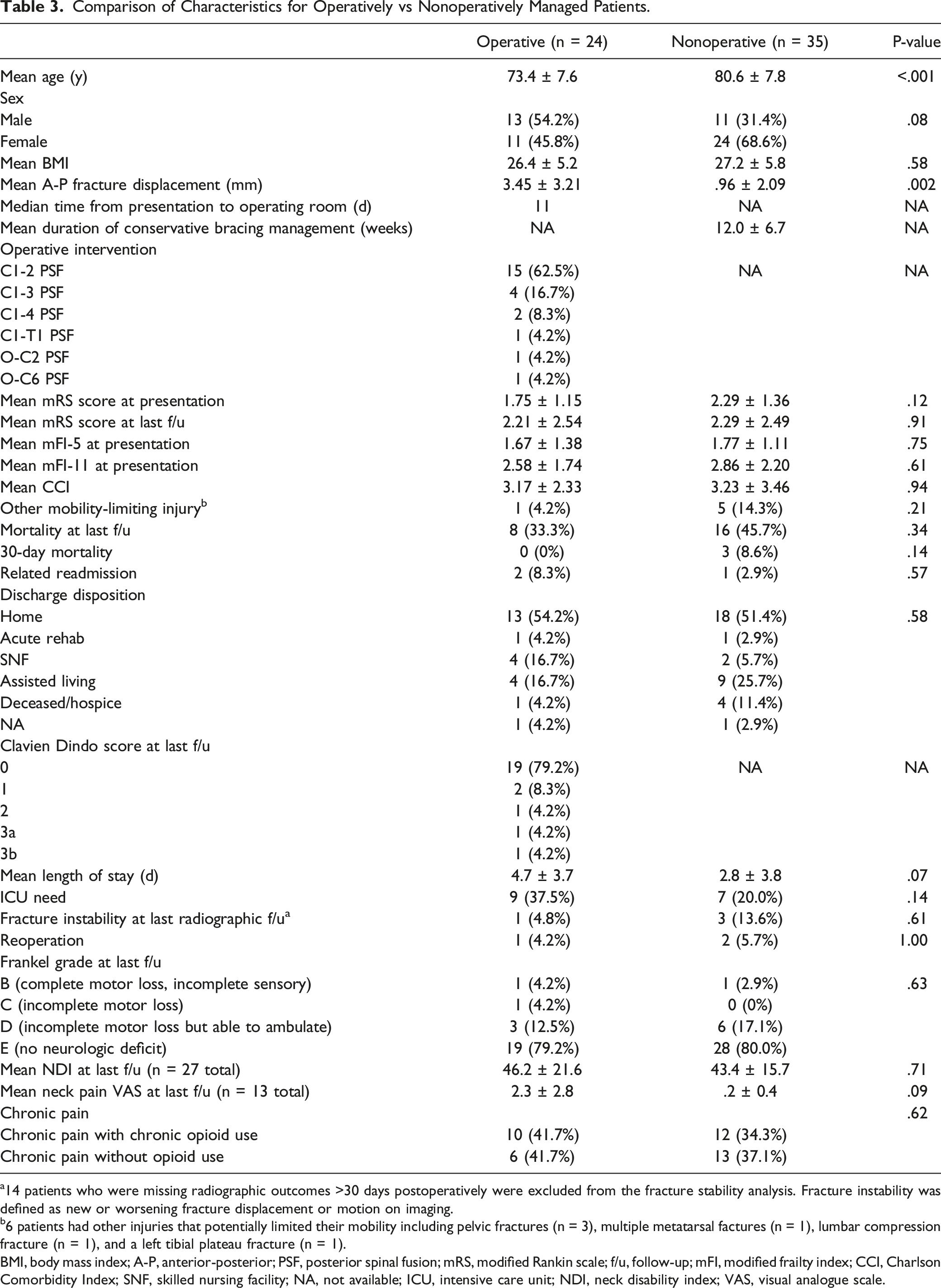
14 patients who were missing radiographic outcomes >30 days postoperatively were excluded from the fracture stability analysis. Fracture instability was defined as new or worsening fracture displacement or motion on imaging.
6 patients had other injuries that potentially limited their mobility including pelvic fractures (n = 3), multiple metatarsal factures (n = 1), lumbar compression fracture (n = 1), and a left tibial plateau fracture (n = 1).
BMI, body mass index; A-P, anterior-posterior; PSF, posterior spinal fusion; mRS, modified Rankin scale; f/u, follow-up; mFI, modified frailty index; CCI, Charlson Comorbidity Index; SNF, skilled nursing facility; NA, not available; ICU, intensive care unit; NDI, neck disability index; VAS, visual analogue scale.
Operative patients were more likely to return for a related readmission (16.7% vs 2.9%), but this difference was not statistically significant (P = .148). Fracture instability as noted in the surgeon’s final follow-up note occurred in one operatively managed patient (4.2%) and three conservatively managed patients (13.6%) (P = .609). Two patients in the conservatively managed group and one in the operative group underwent subsequent surgery in the cervical spine (5.7% and 4.2%, respectively, P = 1.0). BMI, mRS score at presentation, mRS score at last clinic follow-up, mFI-5 at presentation, mFI-11 at presentation, CCI, the presence of other mobility-limiting injuries, mortality, discharge disposition, ICU need, length of stay, rate of fracture instability, Frankel Grade, neck pain, and the presence of chronic pain and chronic opioid use were not different between the treatment groups at last clinic follow-up.
Patient Characteristics and Outcomes Dichotomized Around the Age of 75.
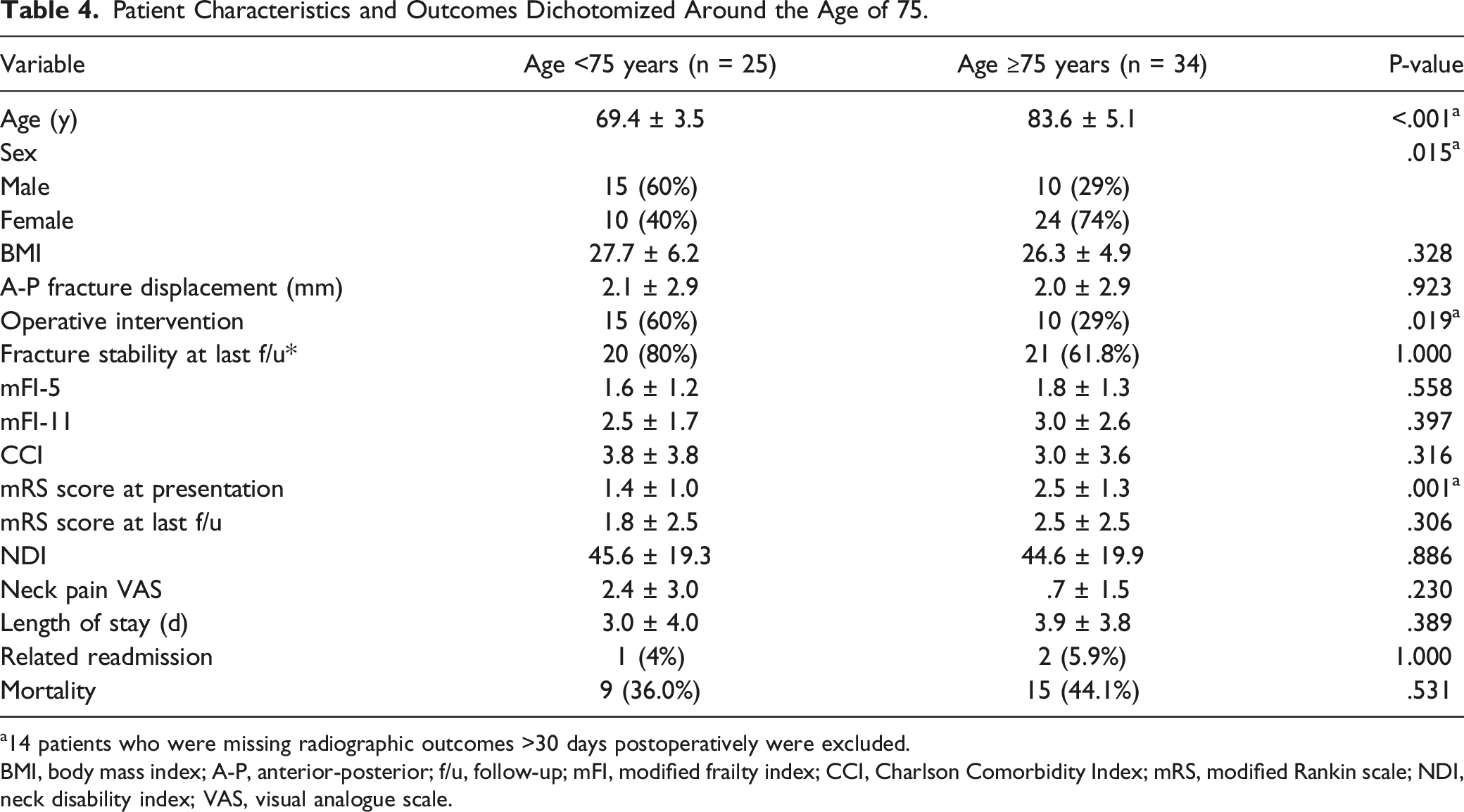
14 patients who were missing radiographic outcomes >30 days postoperatively were excluded.
BMI, body mass index; A-P, anterior-posterior; f/u, follow-up; mFI, modified frailty index; CCI, Charlson Comorbidity Index; mRS, modified Rankin scale; NDI, neck disability index; VAS, visual analogue scale.
Binary Logistic Regression Multivariate Analysis of Variables Associated With Mortality.
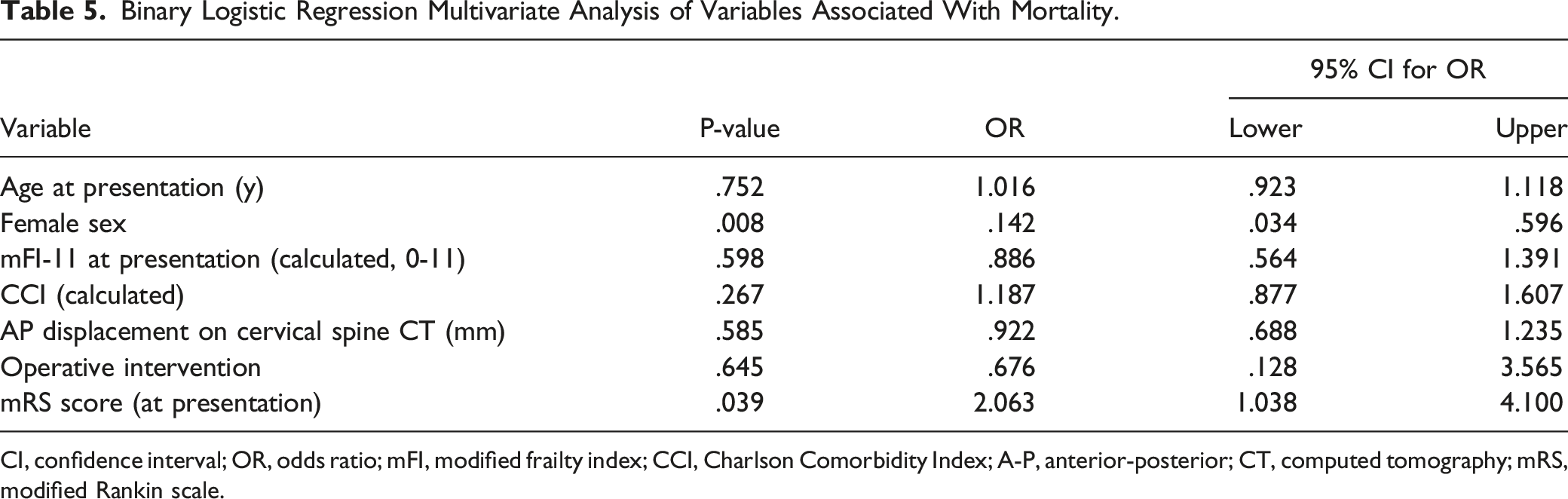
CI, confidence interval; OR, odds ratio; mFI, modified frailty index; CCI, Charlson Comorbidity Index; A-P, anterior-posterior; CT, computed tomography; mRS, modified Rankin scale.
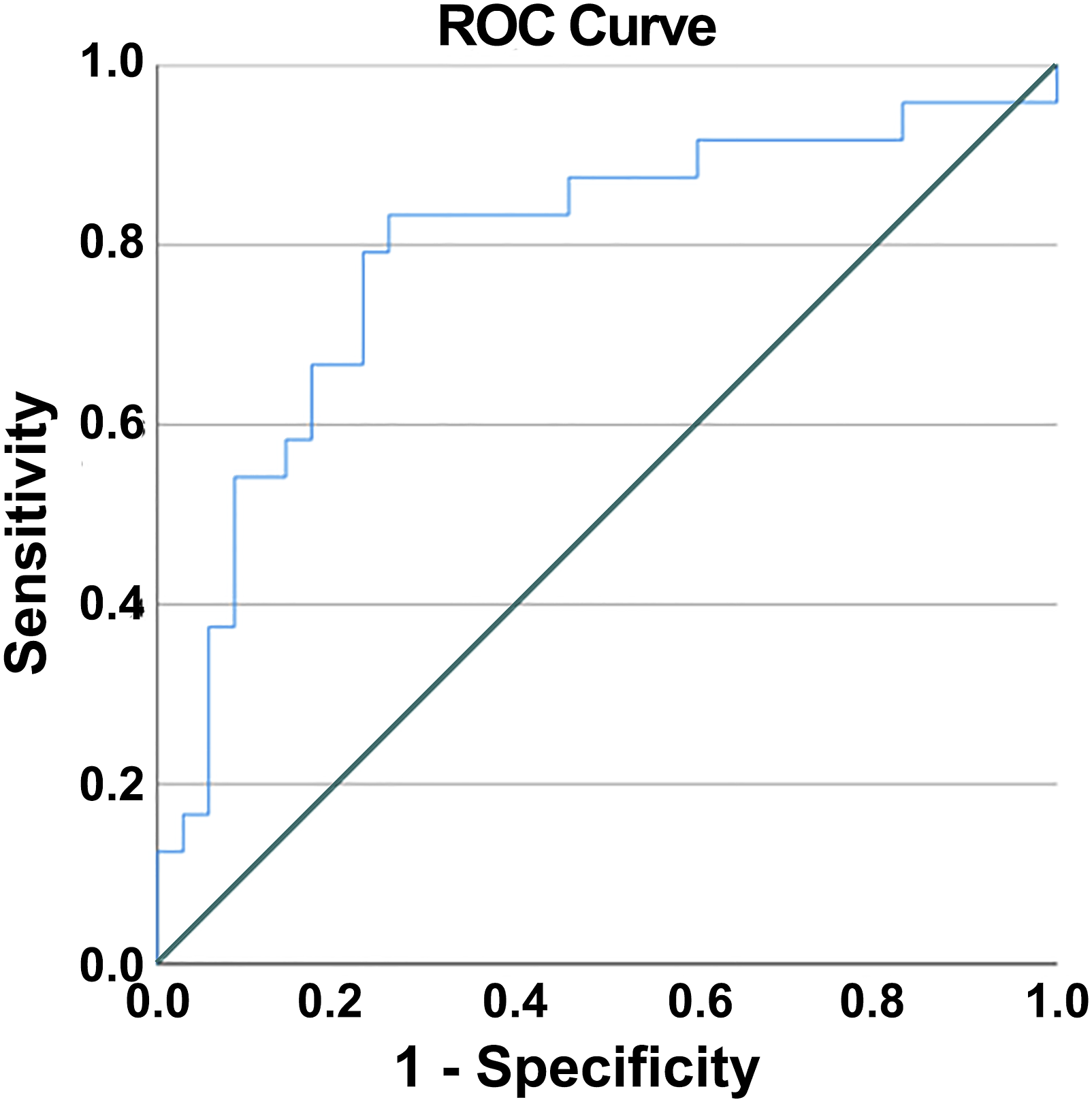
ROC analysis for the multivariate model. ROC area under the curve = .793.
Characteristics Among Patients Who Died by Last Follow-Up.
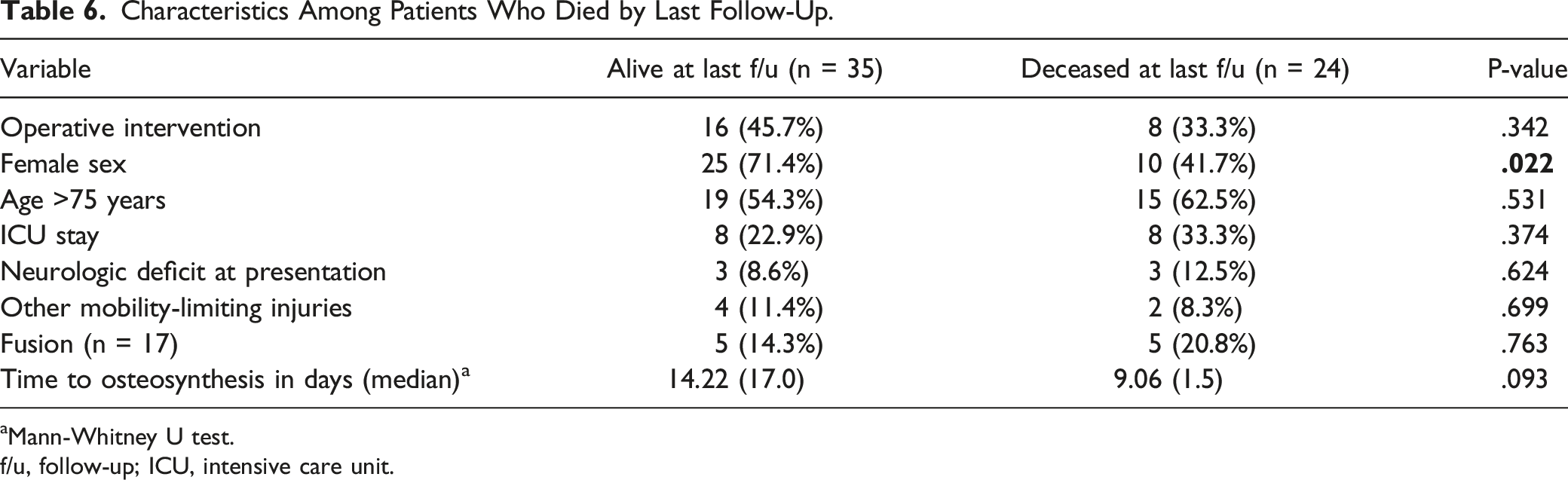
aMann-Whitney U test.
f/u, follow-up; ICU, intensive care unit.
Discussion
We studied the impact of patient factors and treatment on outcomes. Our multivariate analysis found that although treatment modality had no significant impact on all-cause mortality within the study period, mRS score at presentation was a significant predictor of patient mortality. In an aging population, the question of surgical vs conservative management of Type II odontoid fractures is of growing import.
Surgical management of Type II odontoid fractures may involve anterior fixation of the odontoid process to the C2 vertebral body. The anterior approach is associated with higher rates of nonunion among older patients and is favored in minimally displaced fractures.21,22 C1-C2 posterior fusion boasts a superior rate of bony fusion, especially in the elderly, and minimizes complications like dysphagia compared with the anterior screw osteosynthesis approach.21,23,24 Patients treated conservatively may be placed in a semi-rigid cervical collar for 12 weeks or in halo immobilization. Surgical candidates in our cohort each underwent posterior fusion, and conservatively managed patients were in a rigid collar for an average of 12 weeks. In the literature, treatment success has historically hinged upon radiographic evidence of osseous fusion or assessments of subsequent morbidity and mortality.
Weighing expected outcomes is vital to surgical decision-making. Most of the literature on the management of type II odontoid fractures in the elderly has sought to answer the question of surgical vs conservative therapy. The results are mixed, and the subject remains controversial. Proponents of surgical intervention cite superior rates of bony fusion and decreased likelihood of treatment failure.23,25-28 They tend to agree that patients who are younger, have fewer comorbidities, and have significant fracture displacement are more likely to benefit from undergoing surgery over conservative management.6,21,29 Authors who argue for a selective conservative approach have indicated that surgery carries a potentially higher complication risk and provides equivalent functional outcomes.27,30-33 Some articles propose that functional status is more critical than radiographical evidence of bony fusion. 31 In addition, they claim that fibrous union resulting from conservative treatment provides sufficient stability for positive clinical outcomes.27,31,34 Patients in the present study achieved similar radiographical and clinical evidence of stability regardless of surgical intervention.
When dichotomized around the age of 75 years, older patients in our study had a higher mRS score at presentation but mortality did not differ between groups based on age alone. Of note, patients chosen for surgery in our cohort tended to be younger (73.4 y vs 80.6 y, P < .001). As discussed above, this patient selection pattern aligns with the favored practice as described in the current literature, which states that patients above the age of 80 years are less likely to benefit from surgery.7,24,32,33 Graffeo et al 7 demonstrated no survival benefit after surgical management of patients over the age of 80 years. Fan et al 24 showed that patients younger than age 70 years experience higher rates of union and lower rates of mortality after surgical intervention. Barlow et al 35 revealed that operative management of Type II odontoid fracture was cost-effective for elderly patients below the age of 84 years using $100,000/QALY. Above the age of 84 years, surgeries were comparatively more costly and less effective. In addition to the potential for higher complications, cost-effectiveness is a vital measure to consider when outcomes are seemingly equal. Our results and those of the authors cited above suggest that the older patients are at presentation, the more likely they are to be best served by conservative therapy.
Male sex was found to be statistically significantly associated with all-cause mortality after a Type II odontoid fracture. This finding agrees with the findings from a prior study by Chapman et al, 26 who identified an elevated mortality risk in males over females after odontoid fractures (52% vs 38%, P = .013). Similarly, a study reported in JAMA in 2009 found that that older males have a higher risk of mortality after any major fracture. 36
Evidence of fracture stability at final radiographic follow-up did not significantly differ between operatively and conservatively managed patients; however, individuals who underwent surgical stabilization in our cohort also had a statistically significantly larger degree of fracture displacement (3.45 vs .96 mm displacement, P = .002). Fractures with more significant displacement carry a lower likelihood of eventual osseous fusion and stable clinical outcomes without surgical intervention.21,37 The literature also suggests that patients with minimal fracture displacement more readily arrive at a clinically stable outcome with conservative therapy. 38
We found no relationship between treatment modality and functional outcome. In this case, other patient characteristics such as age and degree of fracture displacement should play a role in determining appropriate intervention. Additionally, patients may be stratified based on an assessment of neurologic deficits. Although no association between neurologic deficit and mortality was found in our study, Patel et al 39 have pointed out that patients who present with neurologic deficit are at an increased risk of death after Type II odontoid fractures.
Our study demonstrates that frailty and disability are vital to preoperative assessment. We recorded each patient’s mRS score, CCI, mFI-5, and mFI-11, which have proven utility in patient prognostication. Carlstrom et al. 18 demonstrated the utility of the mIF-5, modified CCI, and Davies frailty indices in predicting mortality and selecting operative vs nonoperative treatment for elderly patients with Type II odontoid fractures. Their results support our claim that assessing patient frailty in addition to age is critical in determining which patients will be best served by surgical intervention. Few other studies have focused the role of frailty in determining patient mortality after Type II odontoid fracture.26,40 To this literature, we add the utility of mRS score in the assessment of elderly patients with Type II odontoid fracture.
The use of mRS score to predict patient outcomes has been validated in other pathologies such as stroke. 41 Our multivariate regression revealed a correlation between a patient’s presenting mRS score and their mortality within the study period (OR 2.24, 95% CI 1.13-4.43, P = .020). mRS score may predict death after Type II odontoid fracture regardless of age, severity of fracture displacement, operative intervention, or neurological deficit. After initially selecting patients based on age, comorbidities, and degree of fracture displacement, we propose using a patient’s mRS score as a potential branch point in determining operative vs conservative management.
Limitations
This is a retrospective study representing the experience of a single institution. Patient death occurred most frequently at an outside facility, which limited our ability to accurately record the cause of death. Post-treatment radiographical assessment was often limited to x-ray, which is inherently less reliable than other imaging modalities when assessing stability and bony fusion. Pain scales were often not recorded upon presentation, limiting our analysis of pre- and post-intervention pain. Future studies will ideally use a randomized controlled design and include more patients across multiple institutions.
Conclusion
Type II odontoid fractures are disproportionately morbid in the elderly population. Choosing optimal candidates for either surgical or conservative management is essential. Patients in this cohort were selected for operative intervention in a manner consistent with the literature, which states that patients who are younger and experience a higher degree of fracture displacement may benefit from operative fracture treatment. Mortality, fracture stability, mRS score, mFI-5, mFI-11, CCI, and pain at last clinic follow-up did not differ based on treatment modality. Our study shows that male sex and an elevated mRS at presentation correlate with greater mortality risk after Type II odontoid fracture. Other frailty and comorbidity measures failed to predict outcome. Additional studies are needed to further characterize which patients are the best candidates for surgical or conservative interventions in the setting of Type II odontoid fracture.
Footnotes
Acknowledgments
We thank Kristin Kraus, MSc, for editorial support.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Dailey is a consultant for Zimmer Biomet Spine. Dr. Bisson is a consultant for MiRus, Stryker Spine, and nView and has equity interest in MiRus. The other authors have no potential conflicts to report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.