
Abstract
Study Design
Retrospective review of a prospective randomized trial.
Objectives
To compare outcome scores and fusion rates in patients with and without pedicle screw-associated facet joint violation (FJV) after a single-level lumbar fusion.
Methods
Clinical outcomes data and computed tomography (CT) imaging were reviewed for 157 patients participating in a multicenter prospective trial. Post-operative CT scans at 12-months follow-up were examined for fusion status and FJV. Patient-reported outcomes (PROs) included Oswestry Disability Index (ODI) and Visual Analog Scale (VAS) for leg and low back pain. Chi-square test of independence was used to compare proportions between groups on categorical measures. Two-sample t-test was used to identify differences in mean patient outcome scores. Logistic regression models were performed to determine association between FJV and fusion rates.
Results
Of the 157 patients included, there were 18 (11.5%) with FJV (Group A) and 139 (88.5%) without FJV (Group B). Patients with FJV experienced less improvement in ODI (P = .004) and VAS back pain scores (P = .04) vs patients without FJV. There was no difference in mean VAS leg pain (P = .4997). The rate of fusion at 12-months for patients with FJV (27.8%) was lower compared to those without FJV (71.2%) (P = .0002). Patients with FJV were 76% less likely to have a successful fusion at 12-months.
Conclusion
Pedicle screw-associated violation of the adjacent unfused facet joint during single-level lumbar fusion is associated with less improvement in back pain, back pain-associated disability, and a lower fusion rate at 1-year after surgery.
Keywords
Level of Evidence: 3
Introduction
Lumbar spine pedicle screws are the most commonly utilized implants for providing immediate spinal stability during fusion surgery. Ideal pedicle screw positioning includes avoiding violation of any adjacent unfused facet joints. Nevertheless, inadvertent screw malposition and screw-associated violation of adjacent facet joints (FJV) remains a potential complication of the procedure regardless of whether surgery is performed in open fashion or with minimally invasive techniques and despite the use of intraoperative imaging or surgical navigation.1-11 Given the proximity of the lumbar vertebral pedicle to the proximal facet joint, FJV occurs almost exclusively at the level of the proximal as opposed to the distal unfused spinal segment, and the rate of FJV in previous series has been reported as ranging from 2.8-100%.1,2,12-16 Although previous studies have suggested that FJV is associated with worse post-operative patient reported outcomes (PROs) in terms of low back pain and disability,17-19 there is no published data regarding the potential impact of FJV on postoperative radiologic fusion rates. The goal of this study was to compare both PROs as well as one-year postoperative computed tomography (CT)-based fusion rates in patients undergoing single-level posterior instrumented fusion surgery with and without FJV.
Materials and Methods
Patient Population and Clinical Outcome Scores
This is a retrospective analysis of a subpopulation from a multicenter prospective randomized placebo-controlled trial of patients undergoing single-level posterior instrumented lumbar fusion for degenerative lumbar disease. The Exogen trial (clinical-trials.gov NCT00744861: Ultrasound as Adjunct Therapy for Increasing Fusion Success after Lumbar Surgery) involved 26 IRB approved participating sites and sought to determine if post-operative ultrasound would increase the rate of radiographic fusion. The trial was terminated after interim analysis showed no difference in radiographic fusion or outcomes between study groups. This unique dataset includes CT studies at 6- and 12-months post-operatively in addition to patient-reported outcome measures.
Inclusion criteria were age greater than 18 years and patients with single-level lumbar degenerative disease. To be included patients were required to have radiographic evidence of instability, facet joint or endplate osteophytosis, thickened facet joint capsule, annulus or ligamentum, disc herniation, decreased disc height, facet joint degeneration, and/or vacuum phenomenon. This retrospective review includes a subpopulation of 157 patients from the original cohort of 310 patients prior to early termination of the study. Patients were only included in this study if they had a complete CT study at 12-months of follow-up. All patients underwent a single-level TLIF and/or PLF with local autograft, of which the techniques have been previously reported.20,21 All pedicle screws were implanted utilizing a posterior midline approach and conventional open free-hand technique with assistance of intra-operative fluoroscopy to confirm acceptable screw positioning. Levels treated included L2-L3 to L5-S1. Patient-reported outcome scores included ODI, VAS leg pain, and VAS back pain at 1-year follow-up. Informed consent was not required after IRB review of study protocol.
Post-Operative Assessment of Facet Joint Violation and Fusion
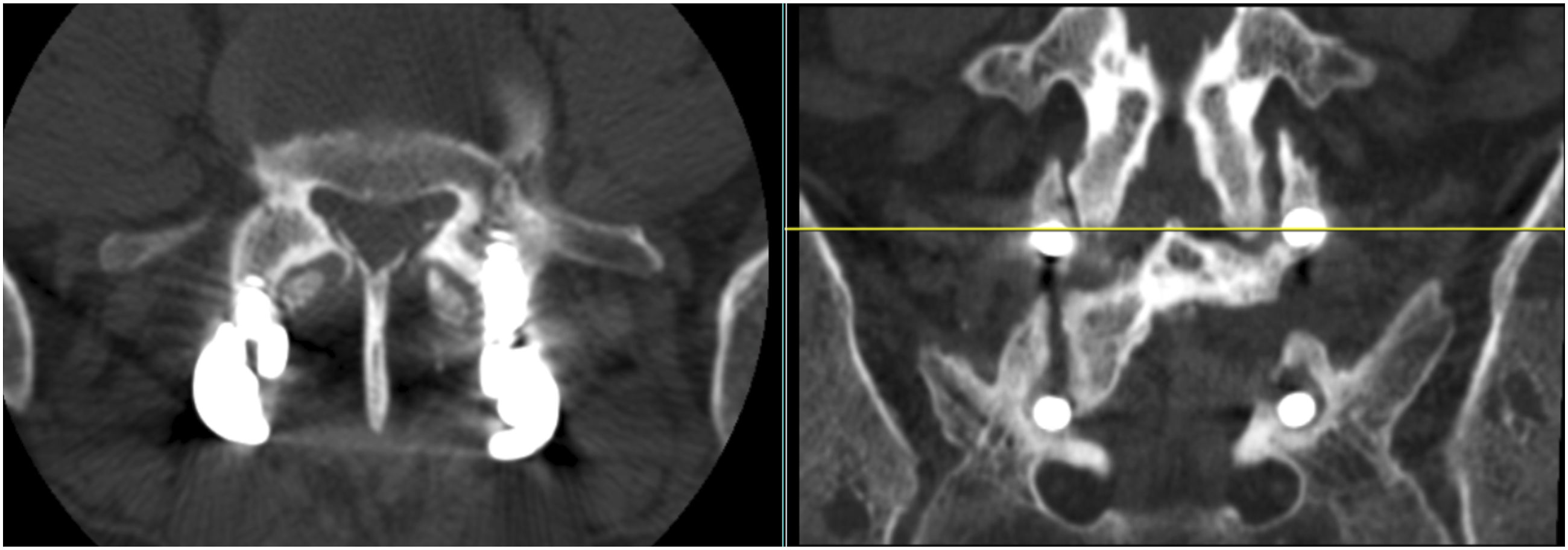
Lumbar CT was performed at 6- and 12-months following surgery. Pedicle screw violation of facet joints was assessed from the 6-month post-operative CT, or on the 12-month CT study if a 6-month CT was unavailable. FJV was defined as the appearance of any portion of the screw, including screw threads, within the anatomic facet joint space between adjacent opposing vertebral articular facets (Figures 1 and 2). Radiographic fusion rates were determined based on 12-month CT studies utilizing thin-cut axial bone windows and sagittal and coronal reconstructions. Evidence of bridging trabecular bone on multiple sequential images defined successful fusion. Radiographic fusion of any single region, including posterolateral, interbody, and facet joints, was considered an adequate post-operative fusion, as reported in our prior studies.20,21 CT studies were evaluated by two separate reviewers with final determination of any discrepancies made by the corresponding author, a fellowship-trained Orthopaedic Spine surgeon. Axial (left) and sagittal (right) CT images of an L4-5 PLF demonstrating facet joint violation by the left L4 pedicle screw with gross violation of the L3-4 facet joint articular surface. Axial (left) and coronal (right) CT images of an L5-S1 posterior fusion construct demonstrating both facet joint impingement and facet joint violation. There is right sided L4-5 facet joint impingement with right L5 pedicle screw within 1mm of the articular surface. In addition, there is left L4-5 facet joint violation by the left L5 pedicle screw.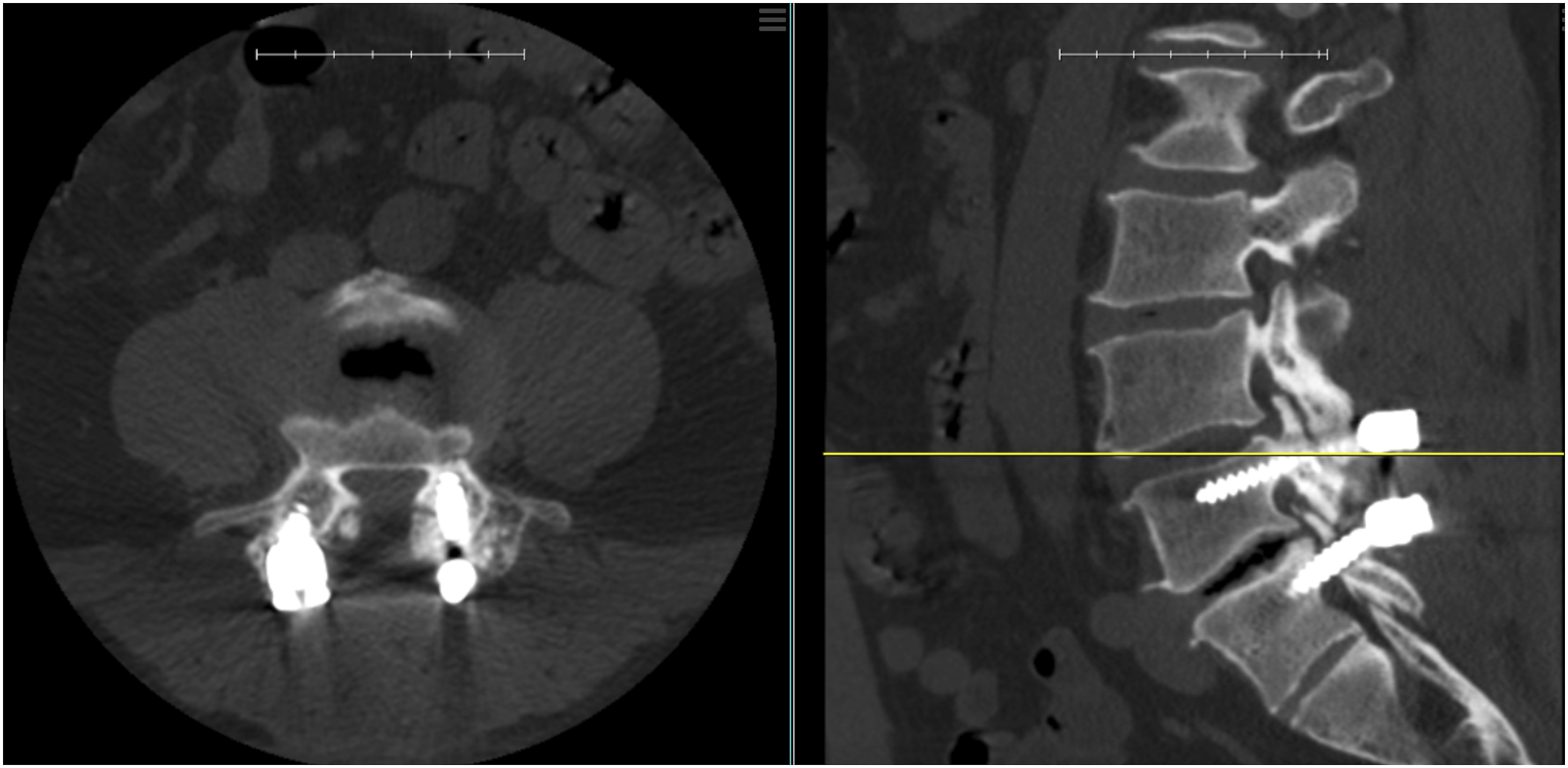
Statistical Analysis
Descriptive statistics are presented for patient-reported outcomes measures, incidence of pedicle screw violation of facet joints, and incidence of radiographic fusion at follow-up. Two-sample t-test was used to identify differences in mean patient-reported outcome scores between baseline and follow-up. Chi-square test was used to compare proportions between groups on categorical measures. Multiple logistic regression models were performed to determine variables associated between FJV and successful fusion. Significance was set to P < .05.
Results
Patient demographics and characteristics by group.
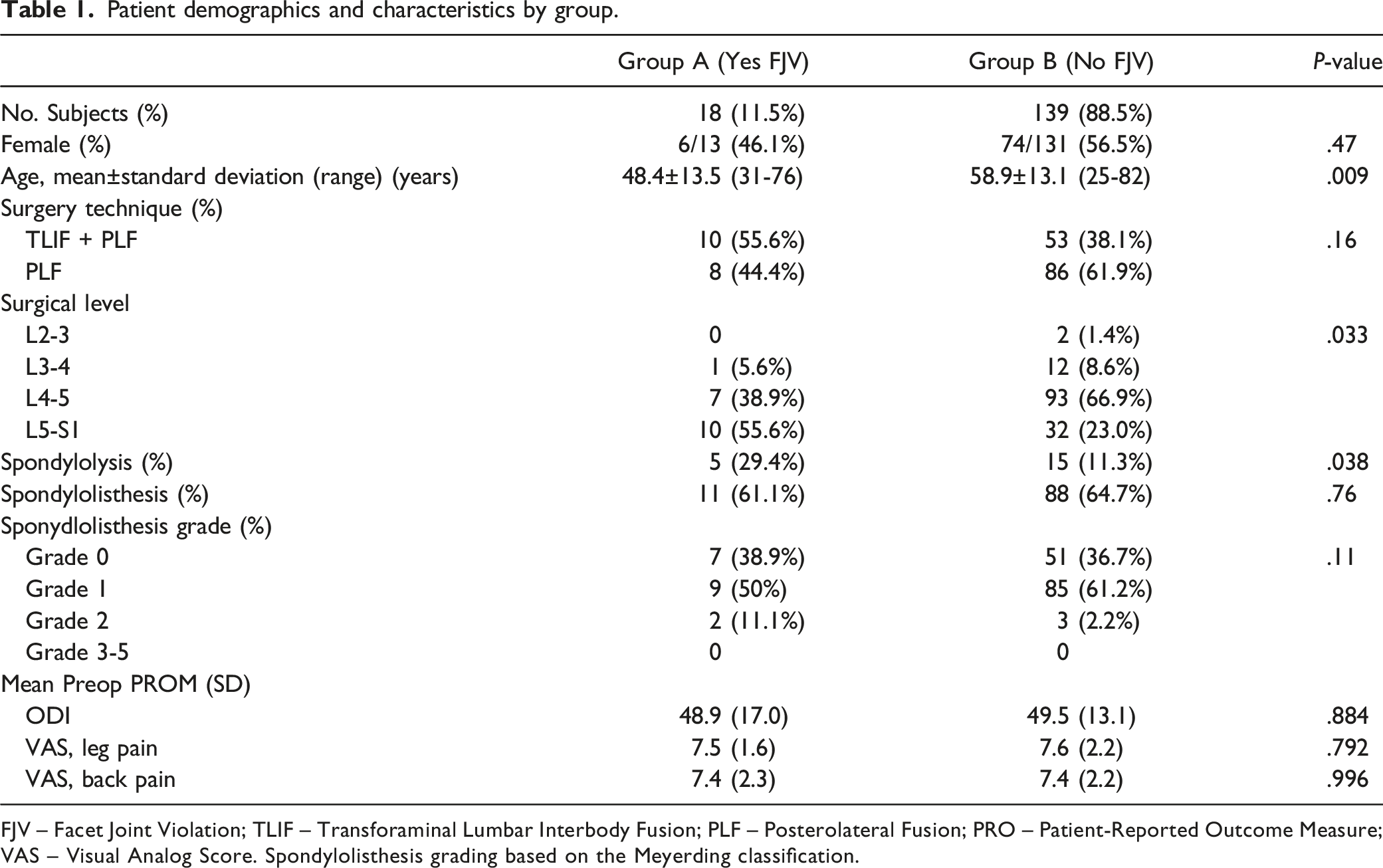
FJV – Facet Joint Violation; TLIF – Transforaminal Lumbar Interbody Fusion; PLF – Posterolateral Fusion; PRO – Patient-Reported Outcome Measure; VAS – Visual Analog Score. Spondylolisthesis grading based on the Meyerding classification.
Patient-Reported Outcome Scores
Fusion Rates and Mean Outcome Scores at 12-Months Follow-Up.

FJV – Facet Joint Violation; ODI – Oswestry Disability Index; VAS – Visual Analog Scale.
Mean patient reported outcomes by group.
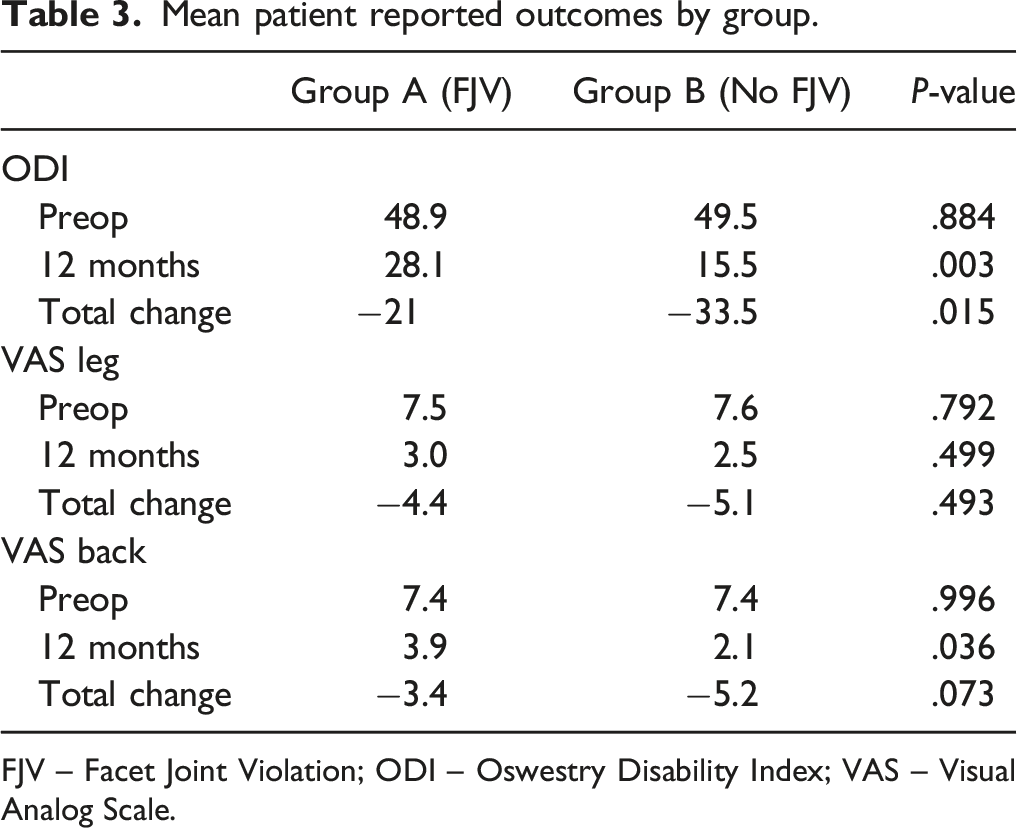
FJV – Facet Joint Violation; ODI – Oswestry Disability Index; VAS – Visual Analog Scale.
Facet Joint Violation and Rate of Fusion
Logistic regression models on adjusted association between FJV and Fusion (n = 127).
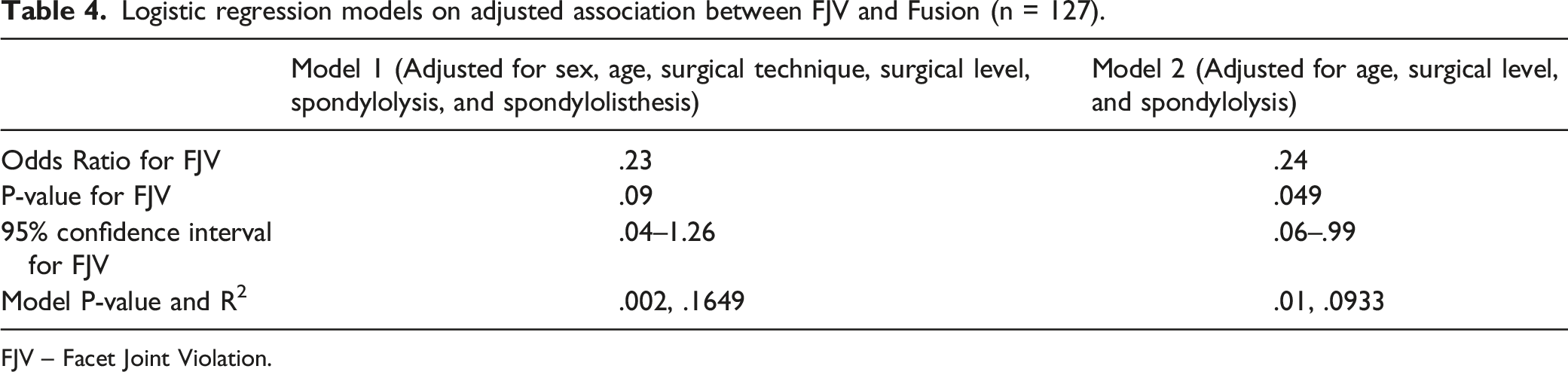
FJV – Facet Joint Violation.
Discussion
Although it is considered standard practice to attempt avoidance of FJV when placing pedicle screws during lumbar fusion surgery, multiple studies have demonstrated a persistent rate of FJV regardless of surgical technique and despite recent developments in intraoperative imaging, surgical navigation, and robotic assistance.1-11 Previously reported FJV rates have ranged from 2.8 to 100% and depend in large part on somewhat arbitrary definitions of FJV.1-3,13-16
The facet joint complex consists of the facet joint capsule and opposing superior and inferior articular facets from adjacent vertebrae. The broadest definition of FJV, including any pedicle screw placement within 1 mm of the articular facet, yields the highest rates of FJV but without any clinical or biomechanical evidence to support use of this cutoff. 1 The capsule is an integral component of the facet joint complex, and there is well-founded concern that capsule disruption may contribute to joint hypermobility or frank instability and accelerated adjacent segment degeneration and disease.22-24 However, marked hypertrophy of the proximal adjacent facet joint is commonly observed with expansive osteophyte formation that extends the capsule over potential pedicle screw starting points; and in such cases, a degree of capsule disruption is unavoidable. For the purposes of this study, we selected a practical definition of FJV, the appearance of screw threads between articulating surfaces of adjacent unfused facets, that is both readily identifiable on CT images and would inarguably lead to accelerated joint degeneration. It also represents a form of FJV that should technically be more avoidable.
Despite our narrower definition of FJV, this study still identified a relatively high rate (11.5%) of FJV in this prospective multicenter cohort of patients undergoing traditional open single-level posterior lumbar fusion, suggesting that this complication likely occurs at a much higher rate than generally suspected and that avoidance may be more challenging than assumed. Placement of pedicle screws at L5, especially in setting of L5-S1 spondylolisthesis, can be technically challenging and may have higher risk of FJV compared to more cephalad levels.2,3,13,15,17,25,26 Chronic exposure to pathologic biomechanical forces often leads to marked deformation of normal facet joint anatomy and overgrowth of bulky osteophytes, which can make identifying the anatomic start point more challenging and increase the risk of FJV. Our data confirms that the FJV rate is nearly three times higher among patients with spondylolysis (25% vs 9.5%). A nonsignificant but suggestive trend towards higher FJV rates was also observed with more severe grades of spondylolisthesis (P = .11). Prior studies suggest degenerative spondylolisthesis may be a risk factor for FJV.27,28 Additional factors including BMI ≥30 kg/m2 and the facet joint angle relative to the midline spinous process may be associated with increased rate of FJV, with prior studies suggesting a facet joint angle >40° as a cut off.3,26,29
Our data demonstrated significant postoperative improvement in PROs regardless of the occurrence of FJV (Table 3). The improvement in PROs at 12-months exceeded previously reported minimum clinically important difference (MCID) threshold values of 1.6 or 2.1 for VAS back pain, 1.7 or 2.8 for VAS leg pain, and 14.3 or 14.9 for ODI, as determined by Asher et al and Parker et al, respectively.30,31 However, consistent with previous studies,17-19 patients with FJV demonstrated significantly less improvement in ODI (28.1 vs 15.5; P = .003) and VAS back pain (3.9 vs 2.1; P = .036) at 12 months compared to patients without FJV. No difference in VAS leg pain scores (3.0 vs 2.5; P = .499) was observed.
To our knowledge, there has been no published data regarding the potential association between FJV and fusion rates. Previous studies regarding FJV at the most proximal level of a construct have focused mostly on pain generation and accelerated adjacent segment degeneration and disease, with a recent meta-analysis demonstrating that FJV increased the risk of ASD with an OR of 30.3.4,7,32-36 Cardoso et al in a cadaveric study demonstrated that bilateral cranial FJV may lead to proximal segment instability. 32 As discussed in these prior studies,4,7,32-36 pedicle screw malposition associated with FJV may carry adverse biomechanical consequences in terms of implant stability or segmental immobilization. In our study, the lower fusion rate in the setting of FJV may be a reflection of surgical technique, perhaps in preparation of the fusion bed, discectomy prior to interbody graft insertion, and/or in application of local autograft. Indeed, 12-month postoperative CT imaging in our study confirmed that FJV was associated with an approximate 43% lower rate of radiologic fusion at 1 year. The possibility that FJV simply serves as a marker for spondylolysis was considered. However, even after controlling for spondylolysis, surgical level, and age, all variables found to be associated with FJV in univariate analysis, FJV was still found to be associated with significantly lower one-year fusion rate (P = .049).
The wide range of FJV rates previously reported in the literature may be due to arbitrary differences in the definition of FJV, but it is also likely due to variations in surgical technique, including minimally invasive approaches, use of intraoperative image-guidance, and robotic assistance. The effect size and even the positive or negative effect of these technical variables, however, remains an area of ongoing debate. Some studies have shown higher rates of FJV in percutaneous versus open techniques1,2,4-6; however, a systematic review of 881 patients from 4 studies by Wang et al in 2015 showed similar rates of FJV of 18.2% in the percutaneous group and 18.7% in the open group. 37 Several anatomic studies have suggested contrasting techniques to minimize the risk of FJV during both open and minimally invasive placement of pedicle screws.9,12,25,38,39 Considered together, the results highlight significant interindividual variability in lumbar spinal anatomy obviating adoption of any single strategy for screw placement based solely on visualization of local anatomic features.
The results from several prior studies have demonstrated improved accuracy of pedicle screw implantation and a reduced risk of pedicle screw-associated FJV when utilizing CT-based navigation 3 and robotic assistance.3,8-11,14,40 A systematic review by Fatima et al analyzed 7379 pedicle screws from 19 studies and demonstrated that proximal FJV was 92% less likely with robotic-assisted pedicle screw implantation versus conventional free-hand technique (OR .08, P < .00001). 10 A more recent study by Singhatanadgige et al found a FJV rate of 0 vs 8.4% when utilizing 3-D CT navigation vs without navigation (P = .01). 3 However, there are some conflicting reports in the literature, such as a review of 768 percutaneously placed pedicle screws comparing fluoroscopic visualization versus intra-operative 3D-CT navigation that found no difference in FJV with rates of 8.8% and 10.2%, respectively (P = .55). 11 The learning curve associated with the implementation of these new technologies is well recognized with reduced operative time, improved pedicle screw accuracy, and lower rate of intra-operative conversion from robotic to free-hand technique.41-45 Potential errors when utilizing navigation systems may arise during image acquisition, reference array motion, and registration of the imaging and equipment, which can be minimized with surgeon experience. 41
As a possible type of spinal implant malposition, FJV represents a common target of medicolegal action, and care must be taken to avoid overinterpretation of the results from this study. Taking reasonable measures to minimize the risk of FJV is an accepted surgical standard; however, the occurrence of FJV itself cannot be considered completely avoidable and represents an accepted risk of pedicle screw-based lumbar fusion. In the case of the current study, all screws were placed in an open fashion by experienced board-certified orthopaedic and neurosurgical spine specialists using intraoperative radiographic imaging but without surgical navigation or robotic assistance. The 11.5% FJV rate observed appears relatively high but is consistent with previous rates reported in the literature. Our finding that FJV is associated with less improvement for clinical outcomes in terms of postoperative back pain, back pain-related disability, and potentially lower fusion rates is concerning and supports the need for ongoing research on the impact of FJV. Despite some conflicting results in the literature, navigation and robotic-assisted pedicle screw placement may help to avoid violation of the cranial unfused facet joint during surgery.3,8-11,14 Although our analysis accounted for confounding factors such as patient age, spondylolysis, and level of surgery, there are likely additional confounding factors that could not readily be accounted for given our limited sample size and the retrospective nature of the study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval was obtained: [1752310-1] Outcomes in lumbar fusion with and without facet joint violation.