
Abstract
Study Design
Mutlidisciplinary consensus recommendations for patients suffering from multiple myeloma (MM) involvement of the spinal column by the Spine Section of the German Association of Orthopaedic and Trauma Surgeons.
Objective
To provide a comprehensive multidisciplinary diagnostic and therapeutic approach and to summarize the current literature on the management of pathological thoracolumbar vertebral fractures in patients with multiple myeloma.
Methods
Multidisciplinary recommendations using a classical consensus process provided by radiation oncologists, medical oncologists, orthopaedic- and trauma surgeons. A narrative literature review of the current diagnostic and treatment strategies was conducted.
Results
Treatment decision has to be driven by a multidisciplinary team of oncologists, radiotherapists and spine surgeons. When considering surgery in MM patients, differing factors compared to other secondary spinal lesions have to be included into the decision process: probable neurological deterioration, the stage of the disease and prognosis, patient’s general condition, localization and number of the lesions as well as patient’s own wishes or expectations. Aiming to improve quality of life, the major goal of surgical treatment is to preserve mobility by reducing pain, secure neurological function and stability.
Conclusion
The goal of surgery is primarily to improve quality of life by restoring stability and neurological function. Interventions with an increased risk of complications due to MM-associated immunodeficiency must be avoided whenever feasible to allow early systemic treatment. Hence, treatment decisions should be based on a multidisciplinary team that considers patient’s constitution and prognosis.
Introduction
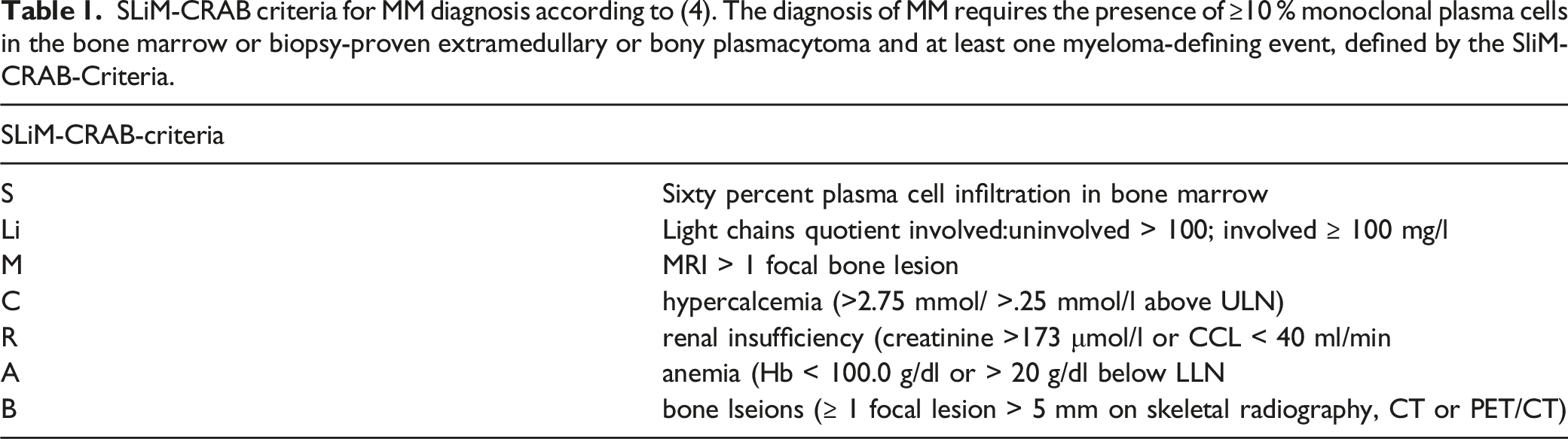
SLiM-CRAB criteria for MM diagnosis according to (4). The diagnosis of MM requires the presence of ≥10 % monoclonal plasma cells in the bone marrow or biopsy-proven extramedullary or bony plasmacytoma and at least one myeloma-defining event, defined by the SliM-CRAB-Criteria.
The incidence of MM in Europe has been reported to be about 6/100,000/year. 5 The median age at the time of diagnosis is around 70 years and the disease occurs slightly more often in men than in women. The absolute 5-year survival is about 40%, the 10-year survival about 30%. 6 Considering demographic changes in ageing societies, there will be an estimated increase of cases by 30% until 2040. 6 More than half of the patients suffer at least from one pathological fracture. 7 While systemic oncological treatment is needed to induce remission and long-term disease control, pathological vertebral fractures need to be addressed surgically in some constellations. The goal of surgery is primarily to improve quality of life by restoring stability and neurological function. Interventions with an increased risk of complications due to MM-associated immunodeficiency must be avoided whenever feasible. Hence, treatment decisions should be based on a multidisciplinary team that considers patient’s constitution and prognosis. This review aims to provide a comprehensive multidisciplinary diagnostic and therapeutic approach and to summarize the current literature on the management of pathological thoracolumbar vertebral fractures in patients with multiple myeloma.
Material and Methods
To achieve a multidisciplinary recommendation, a nominal group process was chosen to summarize expert opinions including medical oncologists, radiation oncologists, trauma- and orthopaedic surgeons. Using this consensus technique, a comprehensive practical diagnostic and treatment algorithm was stepwise developed.
In parallel, a narrative literature was used to include common practice into the nominal treatment process. A Medline-research was chosen to identify the relevant MM literature.
Results
Multidisciplinary Diagnostic and Treatment Algorithm
Figure 1 presents the multidisciplinary diagnostic and treatment algorithm. The different levels of the recommendations for diagnosis and subsequent therapy are described in the following diagnostic workup and treatment sections. Multidisciplinary diagnostic- and treatment-flowchart for patients suffering from pathological fractures due to multiple Myeloma (MM).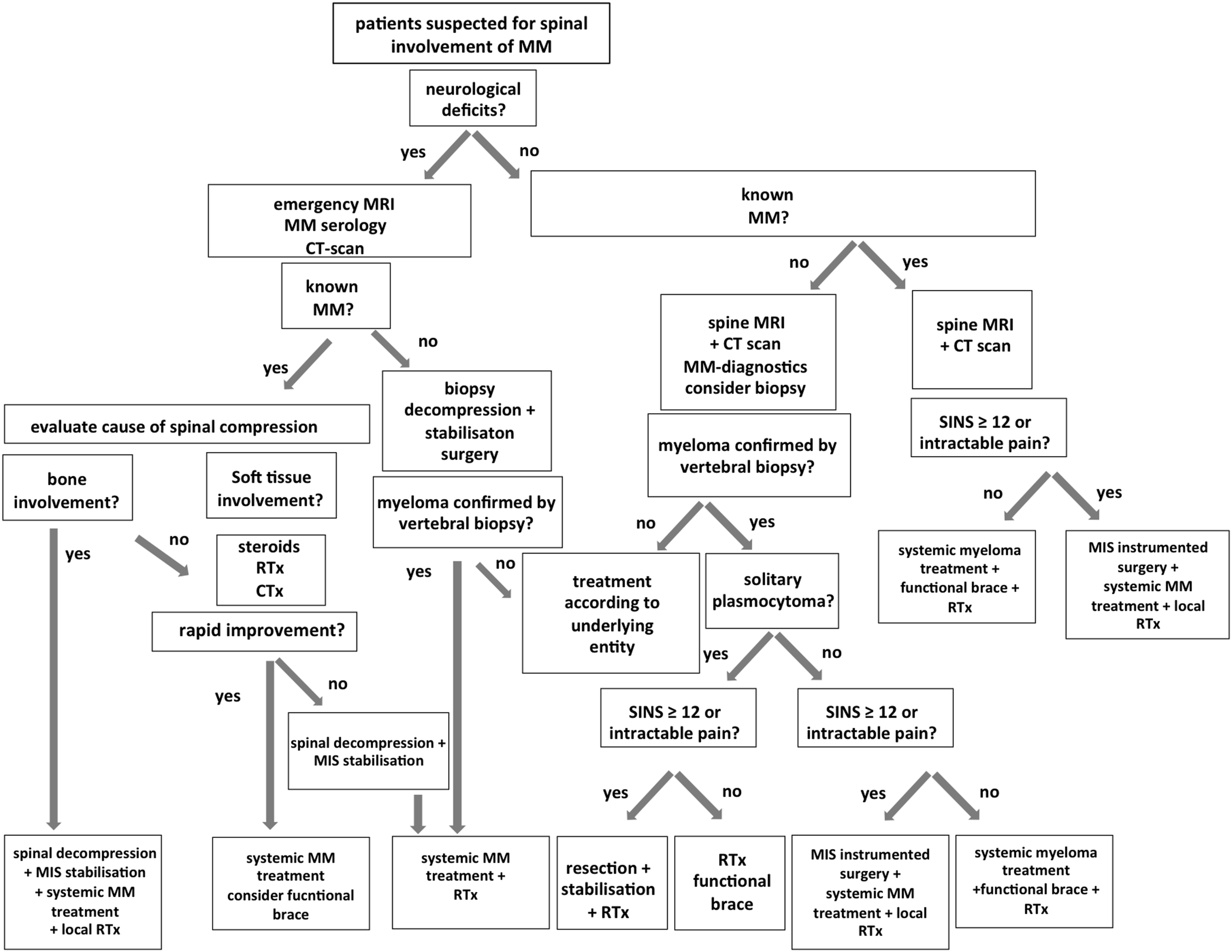
Diagnostic Workup
Clinical diagnostics
In the majority of patients with MM, clinical symptoms are nonspecific and have been lasting for a longer period. 8 Anaemia is reported to be present in 73% of patients, followed by unspecific bone pain in 58% and fatigue (32%). 9 Additionally, 25% of affected patients suffer from weight loss. The diagnosis of MM requires the presence of >= 10 % monoclonal plasma cells in the bone marrow or biopsy-proven extramedullary or bony plasmacytoma and at least one myeloma-defining event, defined by the SliM-CRAB-Criteria (See Table 1). Besides, most patients show typical laboratory findings including elevated levels of monoclonal protein in serum and/or urine protein electrophoresis, an abnormal free-light chain ratio and a positive immunofixation. Therefore, a standard work-up in patients with suspected myeloma includes a full differential blood cell count, serum-chemistry for kidney and liver function tests, albumin, calcium and previously described diagnostics for monoclonal protein in serum and urine. Apart, a bone marrow biopsy and an appropriate imaging survey are mandatory. 4 In a recent publication, different characteristics were shown to be predictive for MM vertebral collapse fractures. Stage 2 and 3 of the International Staging system (ISS) for Multiple Myeloma, patients’ gender, lower back pain, lower Houndsfield Units in a CT-scan, abnormal alignment and lytic lesions were all associated to a higher VCF incidence. 10
Imaging
(a) Spinal Neoplastic Instability Score (SINS) to estimate biomechanical stability in spinal tumor involvement according to (12), For patients with a total score ≥ 7, surgical intervention should be considered (b).
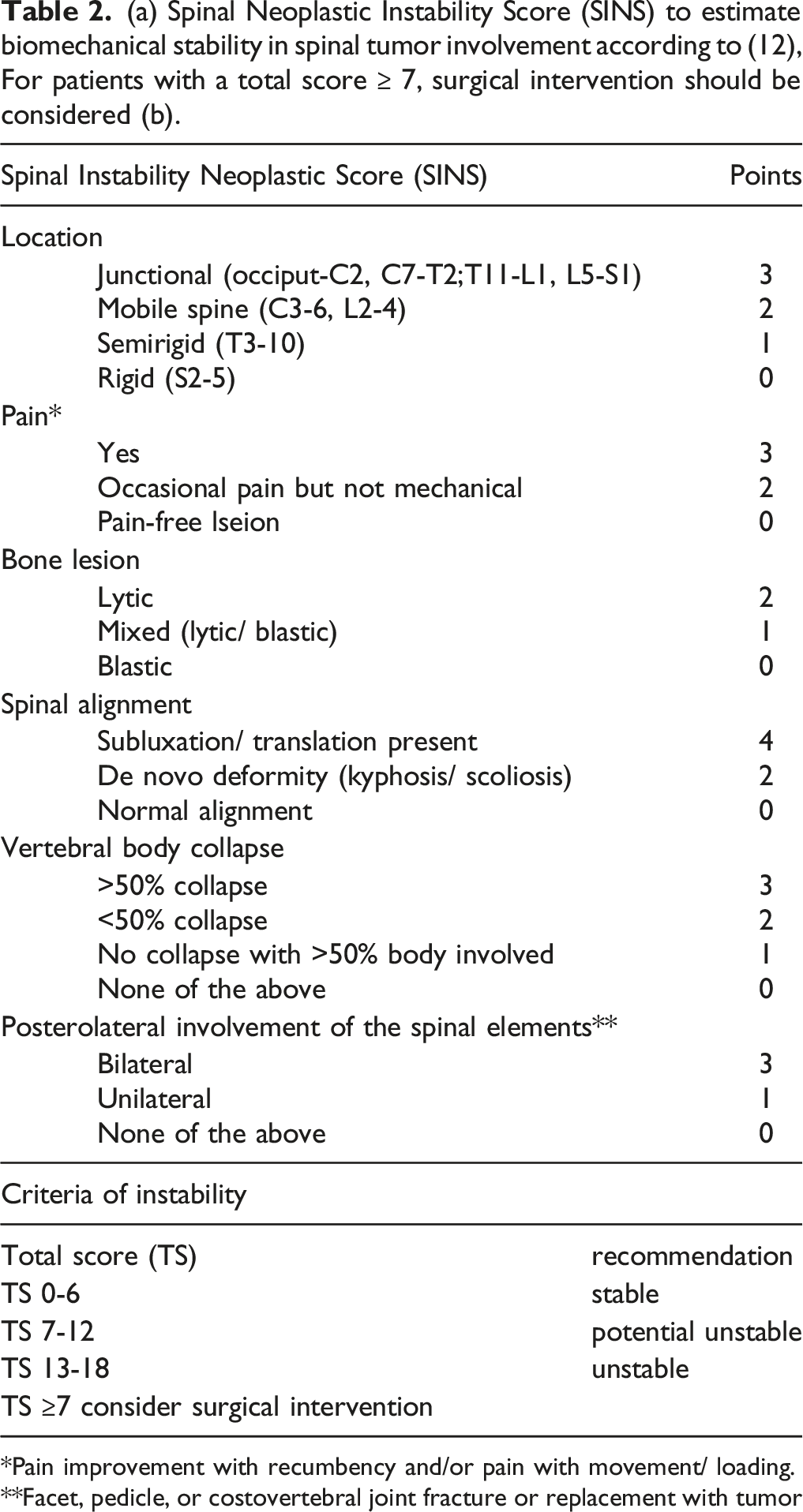
*Pain improvement with recumbency and/or pain with movement/ loading.
**Facet, pedicle, or costovertebral joint fracture or replacement with tumor
A PET-CT can be a valuable option to assess the tumor burden, metabolic activity, the response to therapy and the detection of extramedullary lesions. 13 Due to their low sensitivity and specificity, conventional radiographs play a minor role in detecting fractures, but might be useful for pre-operative planning and as a baseline for follow-ups. A dual energy x-ray absorptiometry (DEXA-) scan can be recommended in order to analyse the need of osteoprotective medication.
Treatment
Conservative and Adjuvant Treatment
Non-Operative Functional Treatment
Several studies demonstrated the positive effects of physical activity and rehabilitation programs on patients with multiple myeloma. But all studies excluded patients with acute fractures. 14 In stable fractures (SINS <7), functional treatment can be performed following back care principles, and exercises supervised by physical therapists. 15 Orthotic treatment is also an option for conservative treatment of stable lesions, fractures with impending instability (SINS score 7-12), or in patients with poor overall status. Malhotra et al. retrospectively compared 183 patients treated with either thoracolumbar-sacral orthosis (TLSO) (51.37 %) or balloon kyphoplasty plus postoperative TLSO. 16 All patients suffered from pathologic vertebral fractures (SINS score 1-12) due to multiple myeloma and the mean follow-up was 205 days (92-418). Patient reported outcome measures improved in both groups significantly. However, delay in treatment showed a negative impact in clinical outcome, particularly if managed with TLSO only. From the authors’ point of view and if applicable, functional orthoses should only be used in patients with SINS score of 7 or above, especially if several fractures or lesions do exist. 17
Chemotherapy
Treatment of MM has significantly evolved over the last two decades. The introduction of several highly effective drug classes and combination therapies, including monoclonal antibodies, immune-modulatory drugs, proteasome-inhibitors and lately emerging immunotherapeutic treatment approaches have improved the outcome of myeloma patients significantly.18-22 With the currently available treatment options, long-term control of the disease is possible in the majority of patients, although the ultimate goal of cure is still not achieved.
Patients suffering from symptomatic MM skeletal involvement regularly present with substantial bone pain, pathologic fractures or even spinal cord compression. In these patients, a multi-disciplinary evaluation is of high importance and is required to define the initial treatment strategy and timing of chemotherapy, especially when neurological symptoms are present. Although the timely initiation of a systemic anti-myeloma therapy is warranted in symptomatic myeloma, specific situations require additional radiotherapy or surgery. Surgical intervention should always be evaluated in patients with vertebral column instability or spinal cord compression related to vertebral fractures. 23 The use of bisphosphonates or denosumab has been shown to significantly prevent skeletal events.24,25 Therefore, their use is recommended for all patients with active myeloma. 26
Radiotherapy
The use of local radiotherapy is mainly directed to the improvement of bone pain, prevention of fractures, and for avoidance or treatment of neurological deficits.26,27 Sole radiotherapy of myeloma-associated pain showed a significant reduction in 69% to 85% of cases and several radiotherapy regimens are available.28-30 For a myeloma induced spinal cord compression Rades et al. showed, that in 238 patients treated with radiation an overall response rate of 97%, a 1-year local control of 93%, and a 2-year local control of 82% was reached. Regaining the ability to walk was shown in 64% of patients.
30
Radiotherapy also triggers the process of recalcification.
29
Dose restrictions for sensitive organs at risk must be considered. Combination with systemic treatment should be done very cautiously. Possible deterioration of hematopoiesis, as well as renal, hepatic, and/or intestinal function should also be considered.
31
Stereotactic body radiotherapy (SBRT) offers an interesting treatment option for patients with multiple myeloma. Previous radiation, manifestation of spinal cord compression, or lack of systemic therapeutic options are no contraindications. Single doses of 16Gy can achieve 91% local control and 85% durable pain reduction.
32
See also Figure 2. 70-year-old patient with multiple myeloma, IgG type kappa and acute renal failure (stage III according to KDIGO) related to cast nephropathy. Pathologic T11 fracture and posterior stabilization T10-12 and kyphoplasty T11. Concomitant therapy with denosumab 120 mg (4 weekly). 3D planned radiotherapy in isocentric 3-field technique with 6/10 MV photons of T11 including the stabilizing material (T10-12). Single dose 3Gy, total dose of target volume 24Gy. The clinical target volume (CTV = pink) was determined from magnetic resonance imaging (MRI) and computer tomography images (CT), with a 1cm expansion for the planning target volume (PTV = red). CTV: describes the volume to be treated with potential microscopic tumor cell spread. PTV: takes into account spatial positional shifts of the patient, e.g. due to respiration and motion. Cranial pre-existing posterior stabilization C7 to T4, at initial diagnosis of MM 03/2019.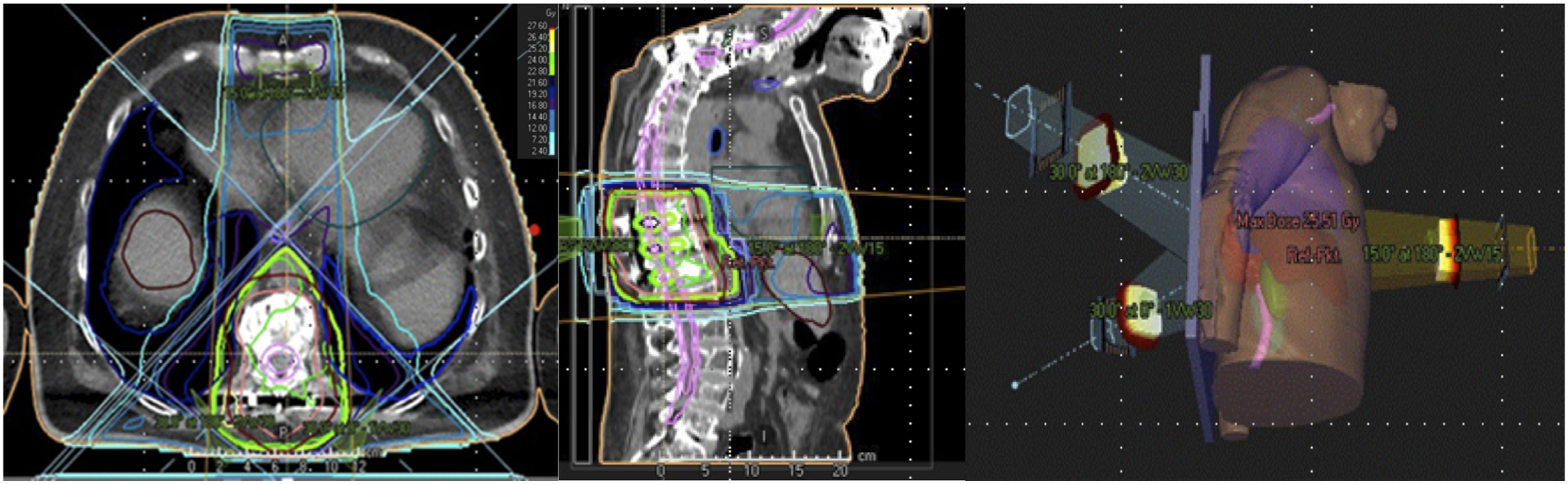
Radiation-related acute toxicities are predominantly limited to skin reactions such as erythema and hyperpigmentation. 33 In the upper cervical region, odynophagia, nausea/vomitus, and in the lower cervical spinal region, intestinal reactions may occur. Nevertheless, radiogenic edema with pain increase may occur, especially after one-time irradiation, necessitating the use of anti-edematous drugs such as dexamethasone. As a prophylactic administration of 8 mg prior to one-time irradiation, the occurrence of edema can be reduced to 3%. 34 Although there is only a low risk for post-radiation vertebral fractures after conventional radiotherapy, crude risk estimates for vertebral fractures after spinal SBRT range from 11% to 39%. 35
Surgical Treatment
Kyphoplasty/Vertebroplasty
Minimal invasive cement augmentation techniques in multiple myeloma have been recommended by the International Myeloma Working Group for MM patients with significant pain at fracture “within 4-8 weeks unless there are medical contraindications”. 23 If diagnosis is not verified biopsy should be done during surgery. Especially, potentially unstable lesions with persisting pain are indications for cement augmentation.
A recent prospective randomized trial has shown advantages of balloon kyphoplasty (BKP) over non-surgical treatment of metastatic vertebral compression fractures. 36 BKP and other cement augmentation techniques offered a rapid and sustainable pain relief demonstrating vertebral body height restoration to a certain amount. 37
Posterior Stabilization
Posterior stabilization using screw-rod-systems is recommended in higher graded spinal instabilities (SINS > 12).
38
Posterior stabilization has shown to increase quality of life by reducing pain and enhancing neurological deficits even in long-term follow-up.39,38 See also Figure 3. Male patient (72y) with severe neck pain without any signs of a neurological deterioration. Blood samples evidenced MM. Local CT-scan (A + B) as well as MRI (C) demonstrated a pathological fracture C2 with C1/2 luxation. The patient underwent open posterior reduction using a C1-4 stabilisation (D1-4). Postoperative controls prior to local radiation and systemic therapy showed adequate reduction and implant placement.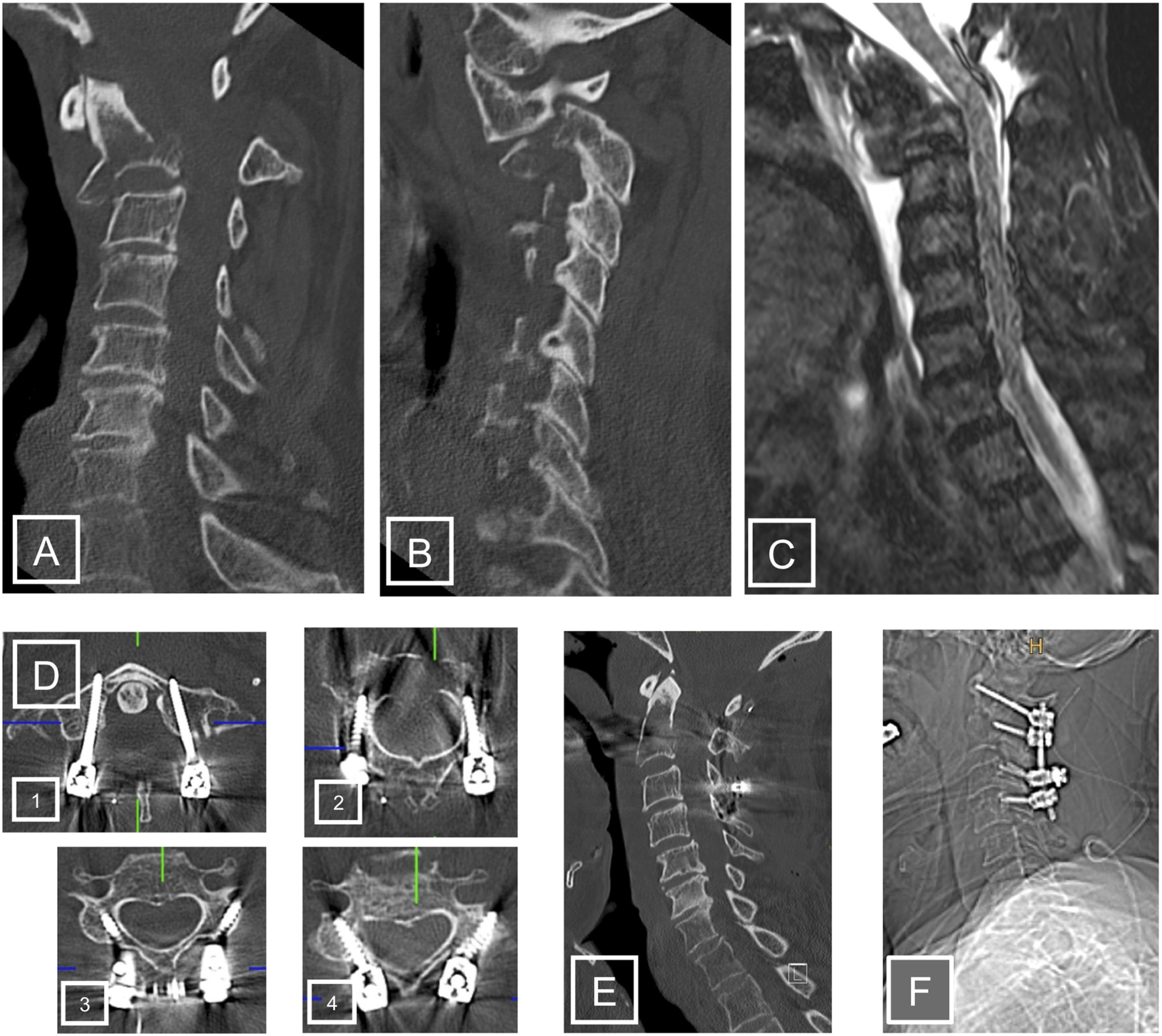
Due to an entity-related peri- and postoperative elevated complication rate, minimal-invasive screw placement is the preferred technique. Thus, soft-tissue injury, intra-operative blood-loss and length of hospital stay can be reduced while an elevated health-related quality of life (HQL) was shown compared to open procedures. 40 However, in some cases, an additive decompression might be necessary. In this case, mini-open surgical approaches are recommended to avoid open surgery.
The use of Carbon/PEEK pedicle screws should be considered in order to reduce artefacts in the post-operative MRI- and CT-imaging for radiation planning and controls. 41 Cement augmentation of pedicle screws might be necessary because of concomitant osteolysis and myeloma related osteopenic bone in adjacent vertebral bodies.
Anterior Stabilization
Anterior stabilization is the preferred approach for most mono- or oligo-segmental MM lesions of the cervical spine. In these cases, the osteolytic vertebral body is resected and replaced by a cage system combined with an additional anterior plate. In selected cases, a kyphoplasty of a lytic cervical vertebra through an anterior approach can be an alternative.
Additional anterior vertebral body replacement is rarely chosen. Cement augmentation and subsequent RT are often sufficiently used to stabilize the anterior column. If radiation therapy is planned, the use of Carbon/PEEK cages and plates should be considered. 41
Solitary Plasmocytoma
A solitary plasma cell tumor is restricted to a single area of the body, without any other signs of systemic disease (absence of Slim-CRAB criteria; < 10 % plasma cell involvement of the bone marrow) can be distinguished from systemic MM by MRI or PET-CT.26,13 This distinction is of prognostic and therapeutic relevance since a solitary plasmocytoma is potentially curable by a locally applied radiation therapy, sometimes in combination with prior resection of the tumor. 42 Nevertheless, a significant proportion of patients will relapse and develop systemic MM in the later course, despite application of local treatment. Due to the fact that SBP is a highly radiosensitive disease and local response rates between 79-91% can be achieved, radiation treatment is the preferred treatment.27,2,43 Depending on the extent of spinal involvement resulting in instability, aggressive resection combined with radiotherapy are recommended in some cases.
Discussion
Treatment decisions in patients with spinal myeloma manifestations are mainly driven by the aim to reduce pain, restore spinal integrity, and avoid or reverse neurological deterioration. Thus, specific HQL measurement tools are mandatory to monitor treatment success and course of treatment. 44 The key step towards proper indication is to identify the source and nature of pain, the extent of instability and the presence and the severity of neurological compromise. Manifestations of MM profoundly differ from the majority of other secondary lesions in terms of adjuvant therapy response and therefore for varying surgical indication. With a rising systemic myeloma load the pressure to subsequently start systemic treatment increases equally to achieve acceptable outcome. If a spinal manifestation is the first symptom of the disease, a surgical intervention prior to systemic therapy should be avoided whenever feasible. Only in constellations with acute onset of neurological deficits or an intractable pain situation, surgery might be indicated. However, latter patients are at a significantly higher risk for peri- and postoperative complications, mainly related to the uncontrolled malignant disease and thus have an urgent need of systemic therapy. 45 The decision of the potential surgical benefit has to be weighed against an early onset chemotherapy and possible higher survival rate.
Patients presenting with mild clinical signs of spinal cord compression related to a soft-tissue mass without radiographic signs of vertebral instability should be treated by early local radiation therapy combined with external orthoses and defined follow-up investigations. If no biopsy is needed to further establish the diagnosis, immediate initiation of systemic therapy and/or radiotherapy will mostly result in excellent resolution of the soft tissue mass and surgery is not needed in this situation. 30 Nevertheless, an MRI scan of the whole spine should be performed to exclude further manifestations.23,26 Patients with large bony defects but structurally stable vertebra can be treated conservatively in spinal orthoses for 8-12 weeks. 16 As soon as the patient can be mobilized there is usually no need for further intervention. Even in patients with impaired spinal stability (posterior wall defects, posterior involvement) spinal orthoses can be the solution until bony bridging occurs. 16 In cases of persistent immobilizing pain, vertebral cement augmentation has to be considered as the majority of patients with excessive pain return to normal level of function within a short period post-interventionally. 46 The correct timing of cement augmentation should be set in a multidisciplinary decision depending on systematic symptoms and the need of a timely chemotherapy. In cases where chemotherapy needs to start immediately, bracing can be very useful to control pain to an acceptable level and avoid vertebral collapse.
Surgical decompression should be aspired whenever higher graded neurological deficits arise. Some authors recommend to avoid the use of implants due to the immunodeficiency- and treatment-associated elevated risks for peri-implant or deep spinal infection. 23 In case of posterior tension bending involvement, posterior fixation should be performed for biomechanical reconstruction. As the risk of implant failure is higher than normal due to the weak bone structure in context of MM, cement augmentation of vertebral bodies or screws is recommended to support construct stability. 23
Mechanical pain due to instability and hyperkyphosis by vertebral collapses might be indications for a more extensive surgical treatment. Even though of limited reliability, instability assessment tools as the SINS-Score can assist in the multidisciplinary understanding and decision-making process. Malalignment can secondary lead to an impaired mobility, poor HQL and an exponential risk of subsequent fractures and additional pain due to the weakness of the spinal muscles or facet joint overload. Reduction of activities, pulmonary and gastric complications can lead to an increased overall morbidity and mortality.
The results following surgical interventions in patients with myeloma-related fractures are promising.47,36,48 Berenson et al. demonstrated evidence for the superiority of BKP versus non-surgical treatment of painful vertebral compression fractures concerning bed rest days, pain relief, reduction of analgesics, back function, QoL and activity.36,48 BKP was more effective than additional radiation or systemic therapy concerning pain relief and disability.
In some cases, pain may persist despite augmentation. In those cases, mechanical changes caused by deformity should be taken into account and surgical stabilization should be re-evaluated during the course of disease, ideally when myeloma is in stable remission. As larger controlled trials for instrumented stabilizations in MM are rare, and clinical outcome in smaller series show heterogeneous results including high rates of complications, careful patient selection and multidisciplinary individualized treatment approaches are necessary.
For all images used in this manuscript the patients gave written consent prior to therapy. According to the local ethics committee requirements no ethics approval was necessary for this narrative review.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).