
Abstract
Introduction:
Multiple myeloma is caused by abnormal proliferation of plasma cells that affects more commonly African Americans. It classically presents with hypercalcemia, renal failure, anemia, and lytic bone lesions. The aim of this article is to present an unusual case of a 63-year-old African-American female with multiple myeloma who presented with worsening right-sided eye swelling for the past 3 weeks and to briefly review ophthalmologic manifestations of multiple myeloma.
Case description:
Our patient’s presentation was associated with a throbbing frontal headache, nasal congestion, malaise, and weight loss. Differential diagnosis on admission included giant cell arteritis, conjunctivitis, preseptal cellulitis, glaucoma, acute sinusitis, or cavernous sinus thrombosis. Extensive ophthalmologic evaluation did not show any intraocular abnormality. However, a magnetic resonance imaging of the brain showed hyperintense foci in the right frontal calvarium leading to the eye swelling. Further evaluation revealed pancytopenia, elevated protein levels, and inverse albumin–globulin ratio suggestive of a plasma cell dyscrasia. A skeletal survey revealed multiple osteolytic lesions. Serum and urine protein electrophoresis revealed elevated immunoglobulin G Kappa monoclonal gammopathy. Bone marrow biopsy demonstrated a hypercellular marrow comprised at least 70% mature appearing plasma cells staining positive for CD138. Chemotherapy with cyclophosphamide, bortezomib, and dexamethasone was initiated. After 2 months of chemotherapy, orbital swelling has resolved with decrease in M-spike, immunoglobulin G, and serum kappa light chains.
Conclusion:
This case illustrates an unusual presentation of multiple myeloma which was eye swelling caused by bony infiltration in the calvarium. Although hematologic malignancies tend to have more specific signs and symptoms, they should be included in the differentials of unilateral orbital edema.
Introduction
Multiple myeloma (MM) is the most common hematologic malignancy of African Americans and accounts for less than 1% of all cancers. 1 It is caused by abnormal proliferation of plasma cells that overproduce immunoglobulins generally confined to the bone marrow. It classically presents with hypercalcemia, renal failure, anemia, and lytic bone lesions due to invasion of the plasma cells in the bone and renal insufficiency from light chain deposition. Patients are diagnosed with a median age of 66 years old. 2 The aim of this article is to present an unusual case of a 63-year-old African-American female with International Staging System Stage III MM with elevated Lactate Dehydrogenase (LDH) who presented with worsening right-sided eye swelling for the past 3 weeks and to briefly review ophthalmologic manifestations of MM.
Case description
A 63-year-old African-American female with past medical history of discoid lupus and hypertension presented with worsening right-sided eye swelling for the past 3 weeks. This was associated with a throbbing frontal headache, blurring of vision, nasal congestion, malaise, and weight loss. Patient has allergy to sulfamethoxazole. The medication list included hydrochlorothiazide. No previous surgeries. Social history was significant for smoking. Family history was pertinent for breast cancer of the daughter. Physical examination included diffuse right eyelid edema and right frontal tenderness (Figure 1(a)). The rest of the examination was unremarkable. Differential diagnosis on admission included giant cell arteritis, conjunctivitis, preseptal cellulitis, glaucoma, acute sinusitis, or cavernous sinus thrombosis. Extensive ophthalmologic evaluation did not show any intraocular abnormality. However, a magnetic resonance imaging (MRI) of the brain showed hyperintense foci in the right frontal calvarium leading to the eye swelling (Figure 1(b)).
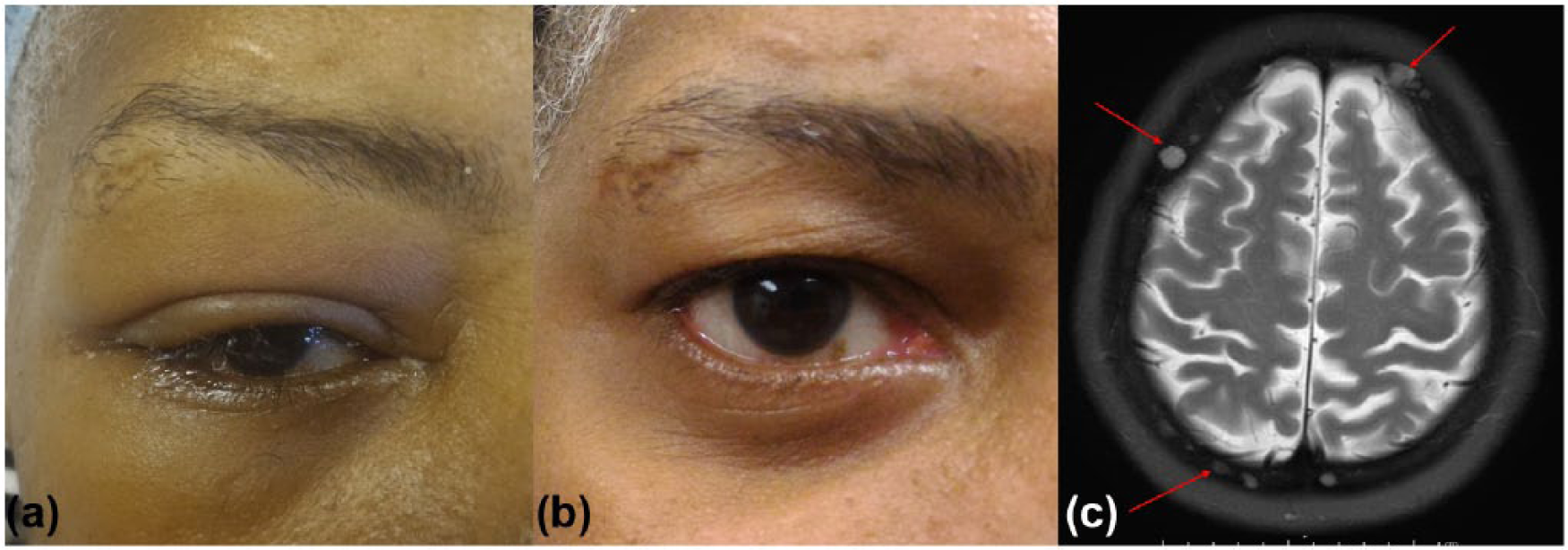
(a) Right eye swelling, (b) resolution of eye swelling after 2 months of chemotherapy, and (c) MRI of head and neck showing T2 hyperintensities in the calvarium.
Further evaluation revealed pancytopenia, elevated protein levels, inverse albumin-globulin ratio, elevated β2 microglobulin, elevated erythrocyte sedimentation rate, and a normal C-reactive protein suggestive of a plasma cell dyscrasia which differed from the patient’s lab work 2 years ago. Calcium and serum creatinine levels were within normal limits. A skeletal survey revealed multiple osteolytic lesions. Serum and urine protein electrophoresis revealed elevated immunoglobulin G (IgG) Kappa monoclonal gammopathy. Bone marrow biopsy demonstrated a hypercellular marrow comprised at least 70% mature appearing plasma cells staining positive for CD138 (Figures 2 and 3). Flow cytometry also showed a small population of kappa clonal plasma cells expressing CD38, CD138, and CD56 comprising 2% of the total cellularity, which was negative for CD19 and CD117. Further analysis of lymphocytes shows a predominant T-cell population (78% of lymphocytes) expressing pan T-cell markers and normal CD4/CD8 ratio (1.0). B cells (10% of lymphocytes) are polyclonal. Natural killer (NK) cells are within normal limits. There is no evidence of increased blasts (Figure 4). Fluorescence in situ hybridization (FISH) test was positive for IGH@ gene rearrangement involving 14q32.3, CCND1/IGH@ gene for translocation (11;14)(q13.3;q32.3), and deletion 13q (RB1) (Figure 5).
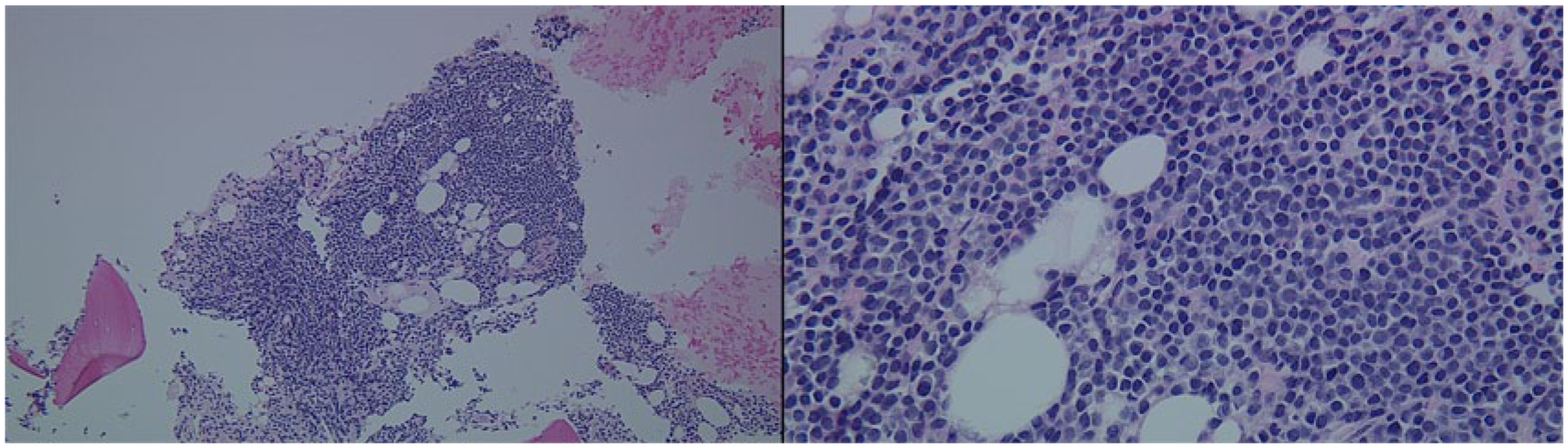
Bone marrow biopsy stained with hematoxylin and eosin showing a solid proliferation of mature appearing plasma cells. Left: objective 200×; right: objective 400×.

Bone marrow biopsy immunohistochemical stain CD138 used to highlight plasma cells. Objective 400×.
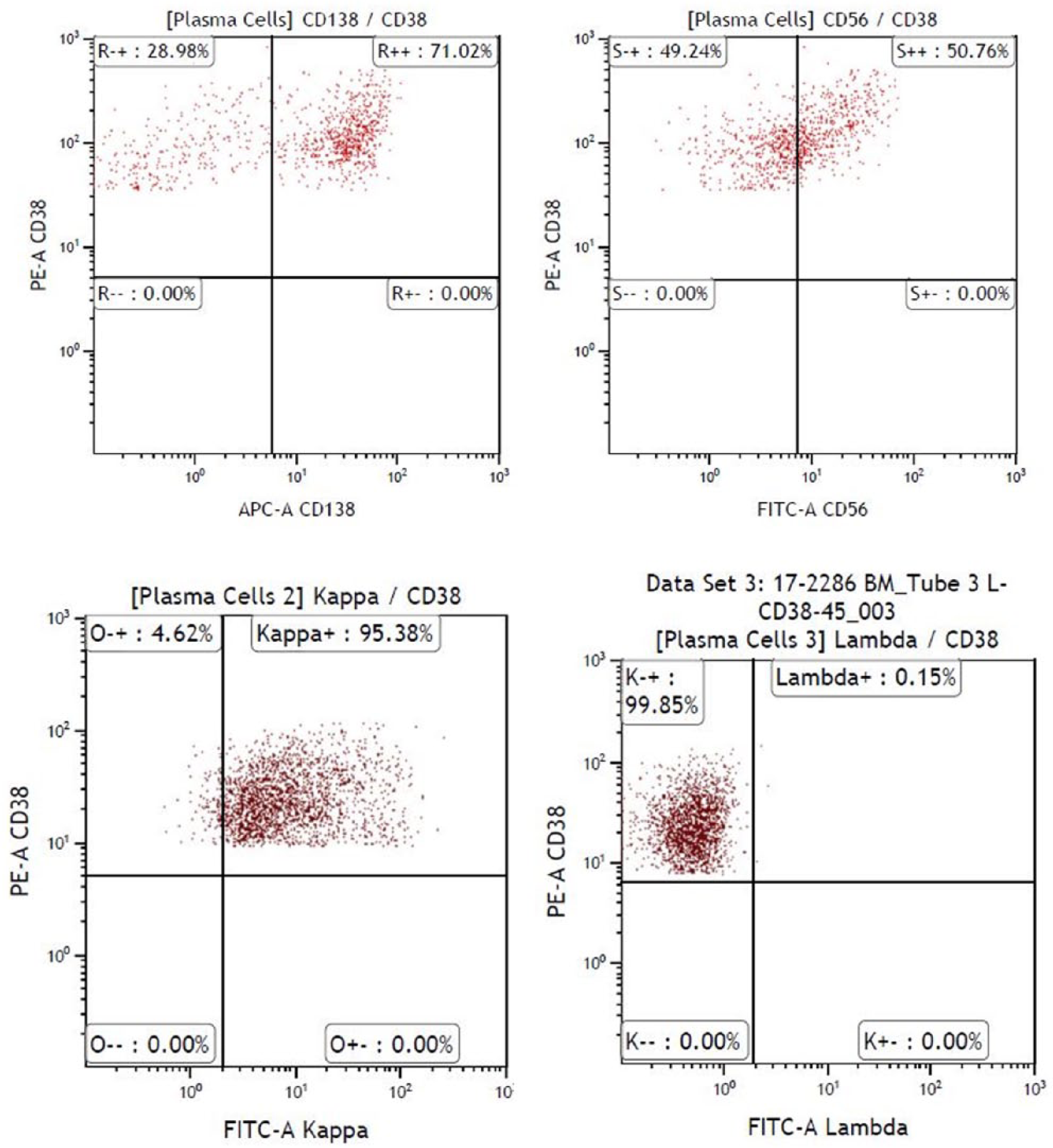
Flow cytometry showing plasma cells isolated with CD38 and CD138 antigens. They are kappa clonal and express CD56. Both markers indicate a malignancy.

Fluorescence in situ hybridization (FISH) test was performed using dual color, dual fusion probes to detect the translocation between the CCND1 gene located at 11q (orange probe) and the IGH@ gene located at 14q (green probe). Signal that has joined orange and green color confirms presence of translocation (11;14)(q13.3;q32.3).
Four consecutive day CyBorD (cyclophosphamide, bortezomib, and dexamethasone) chemotherapy with 500-mg cyclophosphamide (Cytoxan) by mouth, 1.5-mg/m2 bortezomib (Velcade) subcutaneous, and 40-mg dexamethasone by mouth were initiated. Varicella zoster virus prophylaxis with valacyclovir and tumor lysis syndrome prophylaxis with allopurinol was started. Treatment was then changed on a weekly basis. Because of neutropenia, doses of Velcade and Cytoxan were reduced to 1.3 mg/m2 and 300 mg, respectively, during the second cycle of chemotherapy. Because of nausea, valacyclovir was then shifted to acyclovir. She reports pain from the osteolytic lesions, which is relieved with MS Contin and Oxycodone. She declined any orthopedic interventions; thus, she was scheduled to begin palliative radiation therapy for the right humerus, femur, and tibia. After 2 months of chemotherapy, M-spike significantly decreased from 7.2 to 2.5 g/dL, IgG decreased from 8350 to 3689 g/dL, Kappa light chains decreased from 1523 to 316 g/dL, and Kappa/Lambda ratio decreased from 179.1 to 34. She was referred for autologous stem cell transplantation after 14 weeks of treatment. Overall, she tolerated the chemotherapy moderately well and capable of all self-care but unable to carry out any work activities (Eastern Cooperative Oncology Group (ECOG) performance scale: 2) due to moderate fatigue and unsteady gait.
Discussion
The presentation of orbital infiltration by lymphoproliferative and hematopoietic lesions can be grouped into four distinct clinical syndromes: (1) painless orbital masses (most common), (2) fulminant orbital infiltration, (3) secondary orbital infiltration from bone, and (4) neuro-ophthalmic manifestations. B-cell lymphomas can present as an asymptomatic progressively enlarging anterior orbital mass or infiltrate the adjacent structures of the orbit particularly diffuse large B-cell lymphoma. T-cell lymphomas can invade the orbit through the adjacent bony structures such as the paranasal sinuses. 3 Clinically aggressive hematopoietic malignancies such as acute lymphoblastic leukemia, acute myelogenous leukemia (chloromas), Hodgkin’s lymphoma, Burkitt’s lymphoma, and malignant Histiocytosis present with rapid onset orbital pain and swelling mimicking ophthalmologic infections. Late dissemination of such malignancies may also present as extraocular muscle palsies and papilledema (neuro-ophthalmic manifestations). Non-hematologic etiologies of such orbital lesions also need to be considered, such as bone granulomas, intracranial masses, and infections.4,5
Ophthalmologic manifestations of MM are uncommon and involve every part of the eye from the conjunctivae to the iris. 6 The spectrum of presentation includes all the four distinct clinical syndromes cited above. These manifestations include proptosis (most common), chemosis, hyperemia, swelling, diplopia, and vision loss and are due to infiltration of or compression from malignant cells, hyperviscosity syndrome, or light chain deposition.6,7 Retinal involvement includes the hemorrhages, microaneurysms, venous engorgement, and cotton wool spots due to paraproteinemia most commonly from immunoglobulin M (IgM). Patients with orbital involvement from MM are usually 70–80 years old with median survival of 30 months. 3
Initial diagnostic imaging usually consists of a computed tomography (CT) scan which would demonstrate myelomatous changes of the orbit and calvarium. 8 It is essential to differentiate between other tumors such as lymphoproliferative diseases, leukemias, sarcomas, and histiocytic diseases as these may present similarly on the CT scan.
In the case of our patient, only diffuse edema of the right eyelids was noted without involvement of the orbits. Majority of orbital myeloma cases originate in the superotemporal quadrant with IgG dominance. 9 Hassan et al. 10 and Waqar and Smith 11 reported similar cases who presented with unilateral swelling of the eye; however, these patients were already diagnosed with MM and were in remission unlike in our patient where it was the initial presentation. In a retrospective study by Fung et al. 12 in Australia from 1987 to 2002 of eight patients who had ophthalmic manifestations, two of the patients were not known to have MM from the beginning and three presented with orbital involvement. In a retrospective study by Yoshida-Hata et al. 13 in Japan from 2009 to 2014 of hematopoietic malignancies with neuro-ophthalmologic involvement, they reported two cases of MM with sixth nerve palsy and one case with optic nerve invasion. In our patient, there was no neurologic involvement. Treatment of MM is chemotherapy while treatment of extramedullary plasmacytoma in the orbit is mainly radiotherapy. Despite multiple records describing the poor prognosis of extramedullary involvement of MM especially in the eye, our patient tolerated 14 weeks of chemotherapy and scheduled for stem cell transplantation. Future studies include looking into prognostic scoring systems of patients with extramedullary spread of MM particularly ophthalmologic involvement and response to autologous stem cell transplantation in this group of patients.
Conclusion
This case illustrates an unusual presentation of MM which was eye swelling. This was due to bony infiltration of the disease process in the calvarium. Although hematologic malignancies tend to have more specific signs and symptoms, they should be included in the differentials of unilateral orbital edema. Awareness of these manifestations may lead to early diagnosis and treatment. Close follow-up is warranted due to the risk of recurrence of the myeloma as a solitary extramedullary plasmacytoma which portends a poor prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.