
Abstract
Study Design
Case report.
Objectives
With only two previously reported cases, localized amyloidosis of the sacrum is extremely rare. Here we report a 64-year-old woman with a large osteolytic lesion accompanied by weakness and paresthesia of the right leg and difficulties in bladder control.
Methods
Fine needle biopsy and standard staging procedures revealed a primary solitary amyloidoma that was treated with intralesional resection, lumbopelvic stabilization, and consolidation radiotherapy.
Results
Clinical follow-up revealed the diagnosis of multiple myeloma 9 months after initial treatment. At 12 months, no local recurrence has occurred, the neurologic symptoms have resolved, and the systemic disease is in remission.
Conclusions
Intralesional resection with adjuvant radiotherapy of the amyloidoma achieved good local tumor control with limited morbidity.
Introduction
Localized amyloidosis, also referred to as amyloidoma, is a rare type of amyloidosis in which the amyloid deposition is focal. In soft tissues, various localizations including the breasts, the respiratory and gastrointestinal tract, and the central nervous system have been reported. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 In contrast, solitary amyloidoma of the bone is rare. In the axial skeleton, the thoracic spine is most commonly involved, followed by the cervical spine. 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 However, the involvement of the sacrum is extremely rare; only two cases have been reported previously. 25 , 26
Amyloidoma of the bone is a benign tumorlike lesion characterized by bone destruction and extension into the adjacent soft tissue. At the level of the axial skeleton, the destruction of the bone may result in vertebral instability and compression of the spinal cord. 12 , 15 , 18 , 19
The clinical and radiologic diagnosis of amyloidoma may be difficult due to its variable clinical manifestations and unspecific radiologic findings on plain films, computed tomography (CT) scans, and magnetic resonance imaging (MRI). 18 , 27 , 28 , 29 Definitive diagnosis is based on histopathology including immunohistochemistry for IgG lambda and kappa light chains and the demonstration of amyloid protein A (AA) and anti-transthyretin in tissue obtained by an open biopsy or fine needle aspiration. 7 , 8 , 11 , 27 , 29
Due to the frequent development of neurologic deficits, amyloidomas of the axial skeleton are usually treated surgically. The clinical course of the local lesions is usually favorable. However, the overall prognosis depends on the presence or development of a systemic disease. Those cases are usually associated with a poor prognosis. 30 Here we report the rare case of a localized amyloidoma of the sacrum, its diagnosis, and its surgical and oncological treatment as well as the later clinical course.
Case Report
A 64-year-old woman with a history of several years of lower back pain presented to our clinics with increasing pain and neurologic deficits including weakness and paresthesia of the right leg and difficulties in bladder control. Conventional radiographs and a CT scan revealed a large osteolytic tumor (75 × 60 × 55 mm) with destruction of the posterolateral aspect of the sacrum extending the right sacroiliac joint. MRI of the sacrum showed an extradural mass with low signal intensity on T1-weighted and enhanced intensity on T2-weighted images with complete obliteration of the spinal canal below S1 (Fig. 1). Single-photon emission CT and intravenous contrast CT of the thorax and the abdomen did not show any further skeletal lesions or signs for a primary tumor or metastases.
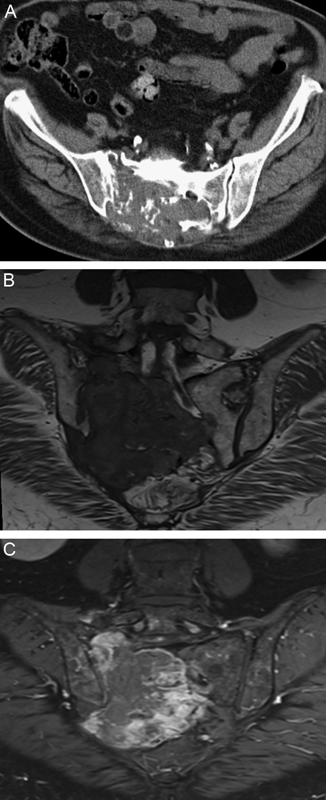
Preoperative computed tomography (transversal plane) at the level of SI joint and magnetic resonance imaging (coronal plane) scan show the osteolytic tumor and extradural mass (75 × 60 × 55 mm) with low signal in T1-weighted and inhomogeneous enhancing intensity in T2-weighted images with complete obliteration of the spinal canal below S1.
A CT-guided needle biopsy was performed. Upon histologic analysis, the tumor consisted of amyloid deposits as revealed by typical apple-green birefringence following Congo red staining. Amyloid deposits were partially engulfed by multinucleated giant cells, and an accompanying lymphocytic infiltration was found. Immunohistologic specification of the amyloid deposits revealed lambda light chain amyloidosis (AL; Fig. 2).
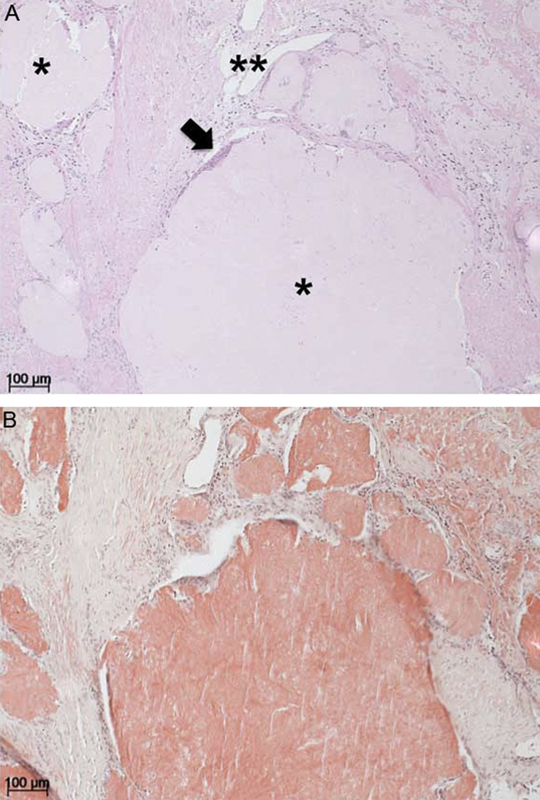
Hematoxylin and eosin (A) and Congo red (B) staining of the biopsy material in 100× magnification. The biopsy largely consists of rather homogeneous, pale pink, nonfibrillary, amorphous extracellular mass (amyloid, A, asterisk), which typically stains brick red in a Congo stain (B) and reveals a classical apple-green birefringence under polarized light. Giant cells of the foreign body type were found as a reaction to the amyloid deposits (A, arrow).
Multiple myeloma was excluded by bone marrow biopsy and immunoelectrophoresis of the serum and the urine. Systemic amyloidosis was ruled out by MRI of the heart and biopsies of the colon and the kidney. The results of the preoperative blood examination are shown in Table 1.
Preoperative blood examination
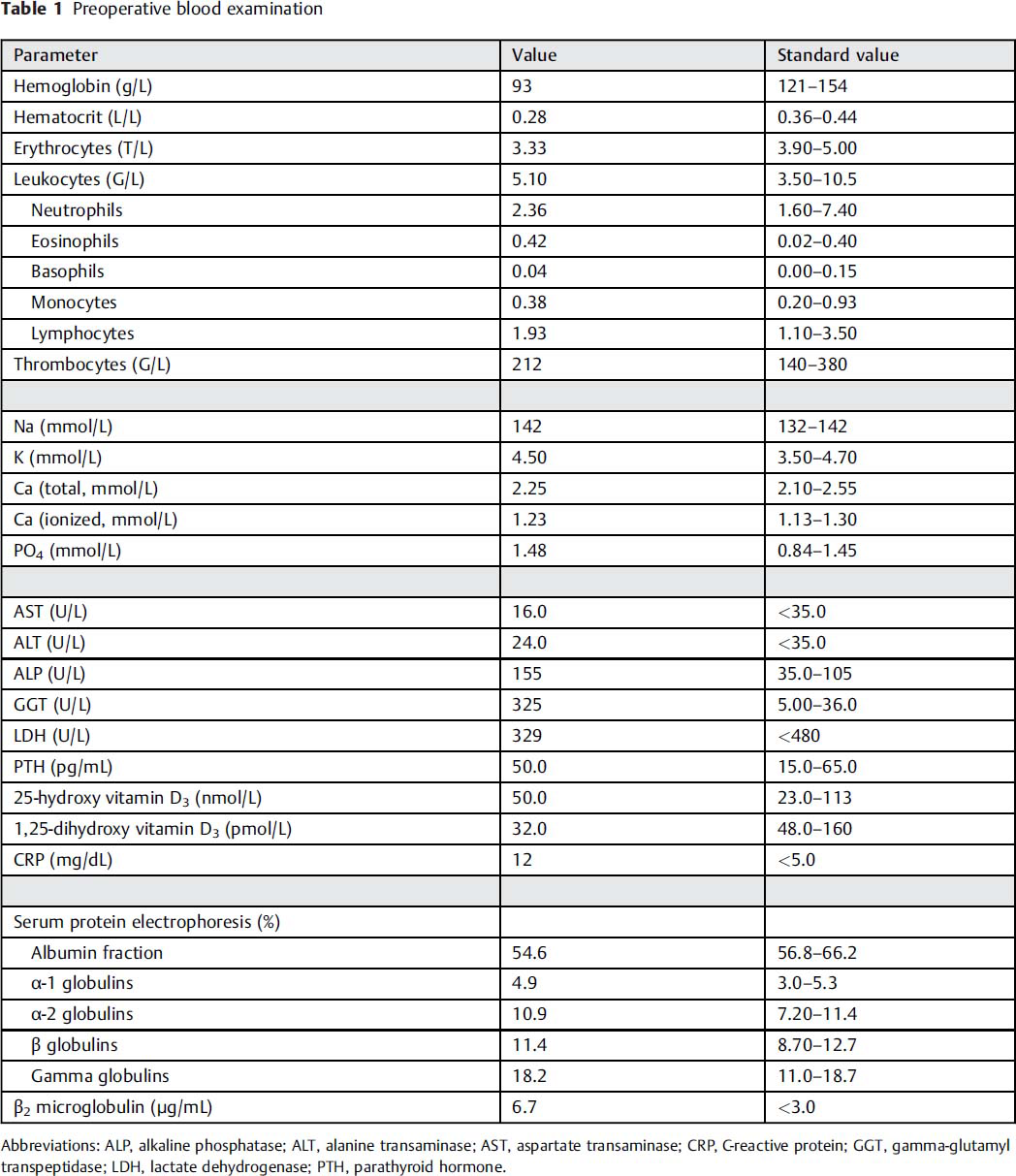
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; CRP, C-reactive protein; GGT, gamma-glutamyl transpeptidase; LDH, lactate dehydrogenase; PTH, parathyroid hormone.
En bloc tumor resection was not possible without sacrificing the L5 to S3 nerve roots. Therefore, an intralesional resection was performed by a posterior approach. The tumor tissue was very brittle and the resection was performed in a piecemeal fashion with curettage and suction. The L5 to S3 nerve roots were decompressed. Lumbopelvic stabilization from L4 to the ileum was performed with a modified Galveston technique using the USS Ileosacral system (DePuy Synthes, Oberdorf, Switzerland) because the sacrum could not be used for screw placement due to its lytic destruction. 31 , 32 Solid screw purchase could only be achieved in the supra-acetabular region of the right ilium. All nerve roots as well as the presacral iliac vessels could be separated from the tumor mass and preserved. Sufficient soft tissue coverage after tumor resection and lumbopelvic stabilization was achieved. Primary wound closure was performed without the need for soft tissue reconstruction. The surgical intervention took 3 hours 45 minutes, and the intraoperative blood loss was 1,700 mL. No intraoperative or postoperative complications occurred (Fig. 3).
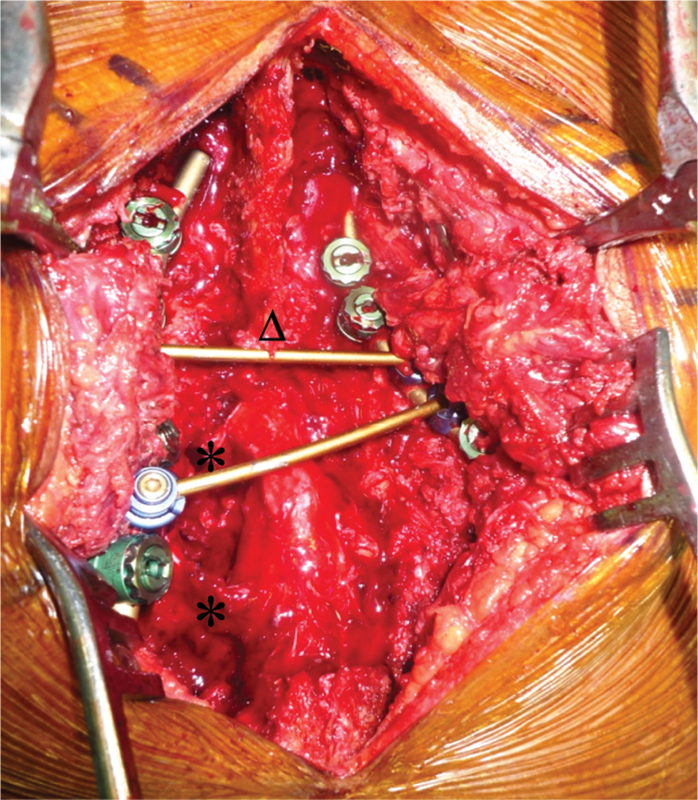
Intraoperative situ after intralesional tumor debulking and spinopelvic stabilization. On the right side, resection included the medial aspect of the ilium; therefore, two iliac screws were necessary. The dural sac was circumferentially cleared below the spinous process of L5 (triangle), and the exiting roots S1 and S2 (asterisks) were decompressed.
Histopathologic analysis of the surgical specimen revealed dense tumor-forming amyloid deposits and an accumulation of mature clonal plasma cells revealing a lambda light chain restriction and monotypic expression of IgG (Fig. 4). Bone marrow biopsy was repeated and again revealed no evidence of multiple myeloma. In the demonstrated absence of systemic disease, the diagnosis of a primary solitary amyloidoma of the sacrum was made. Surgical treatment was followed by uneventful consolidation radiation therapy (50 Gy total dose, given in 25 fractions over 5 weeks).
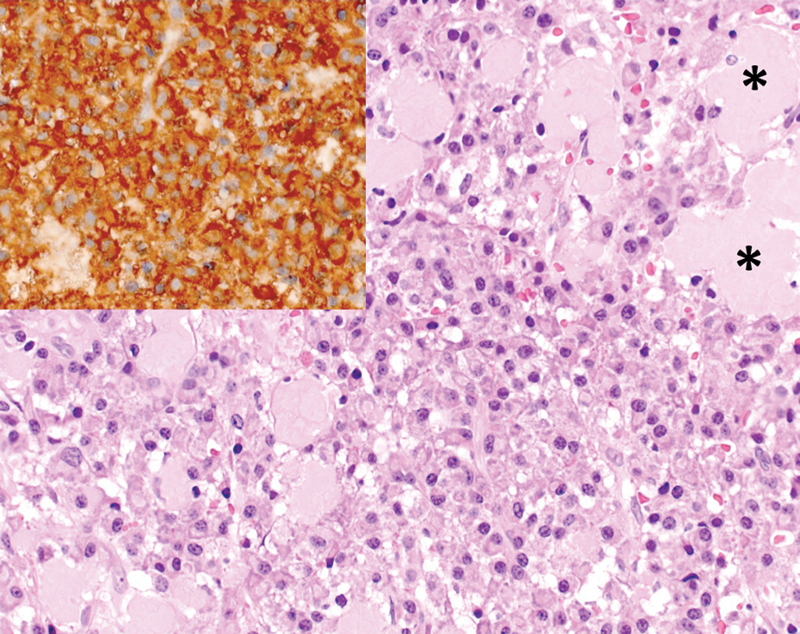
Hematoxylin and eosin staining and immunostaining for lambda light chains (inlay upper left) of the intraoperatively retrieved specimen in 400× magnification. The biopsy largely consists of sheets of mainly mature plasma cells as well as islands of homogenous, pale pink, nonfibrillary, amorphous extracellular mass (amyloid, asterisks).
At 6 months’ follow-up, the patient showed no signs of local recurrence, had regained neurologic function of the lower extremities completely, and had normal bladder and bowel control. At 9 months, a restaging including serum immunoelectrophoresis showed elevated plasma levels of lambda light chains, which now indicated systemic disease. Along with new radiologic findings of osteolyses of the cranium and the proximal femur, multiple myeloma was diagnosed and the final diagnosis of the sacral tumor was revised to “multiple myeloma-associated amyloidoma.” Standard induction chemotherapy with bortezomib and dexamethasone was initiated. At 12 months’ follow-up (Fig. 5) the patient was free of local disease at the sacrum and the systemic disease was in remission. The osteosynthesis was stable and intact, and the patient was mobile without neurologic impairment.
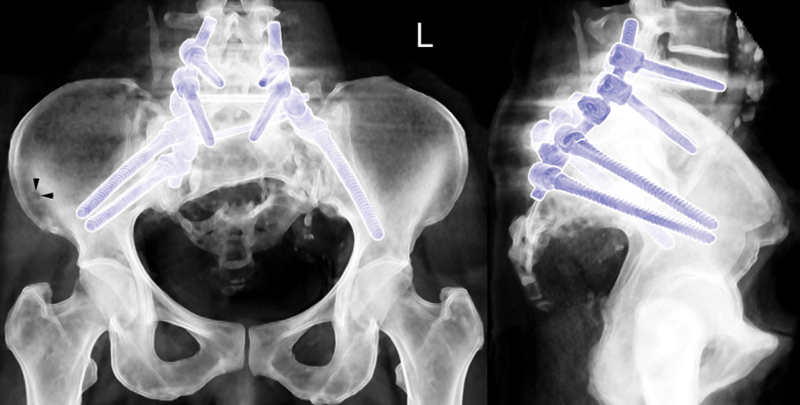
Biplanar view of a computed tomography reconstruction of the pelvis 12 months after surgery. The large defect is still visible but not progressing, and the implant material is intact without signs of loosening. There is a small lytic lesion visible in the right ileum indicative for multiple myeloma (arrowheads).
Discussion
Amyloidoses are a heterogenous group of diseases characterized by the extracellular deposition of amyloid in various locations. The disease can be localized or systemic and is defined according to the deposited protein (e.g., serum AA, light chain amyloid, β 2-microglobulin, transthyretin). 27 In systemic forms, the precursor protein is released into the circulation in its soluble form and deposited as amyloid in various locations. Localized amyloidosis, also referred to as amyloidoma, appears as a circumscribed lesion that may occur in the breast, lung, gastrointestinal tract, central nervous system, and bone. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 27 , 29 , 30 Amyloidomas present as tumorlike lesions with signs of malignant tumor growth. 15 , 18 , 28 , 29 , 33 In localized amyloidosis of the bone, the lesions are usually composed of immunoglobulin kappa or lambda light chains (AL amyloidoma). 27 , 29 , 30 The accumulation of AL amyloid in the bone may be primary or associated with systemic disease in the context of multiple myeloma. In the latter case, monoclonal immunoglobulin light chains are also present in the blood. 29 , 34
Skeletal involvement of localized AL amyloidosis is unusual. Most cases have been reported in the spine, preferentially in the thoracic and cervical part. 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 With only two reported cases so far, affection of the sacrum as in our case is extremely rare. 25 , 26 Clinical presentation of amyloidoma in the axial skeleton varies. Depending on the location, size, and involvement of neural structures patients may be asymptomatic, have localized back pain, or show varying degrees of neurologic symptoms including radiculopathy, paraparesis, and paraplegia. 14 , 15 , 16 , 26 , 33 , 35 , 36 , 37 , 38 Pathologic fractures are rare. 15 , 26 , 38 , 39
Involvement of the skeleton may lead to bony destruction mimicking other locally aggressive processes including infections or malignancies such as chondrosarcoma, lymphoma, and bone metastases. 15 , 18 , 28 , 29 , 33 On conventional radiographs, amyloidoma of bone presents as lytic lesions with varying degrees of calcification. Cortical disruption may be present due to the expansion of amyloid deposits into the surrounding soft tissue. 13 For lesions at the level of the axial skeleton, an evaluation with respect to potential instability and neurologic affection is needed. Computed tomography is well suited to evaluate bone destruction and instability with well-known limitations to assess the expansion into the soft tissue. 15 , 36 On MRI, amyloidoma usually exhibit low to intermediate signal intensity on both T1- and T2-weighted images with variable contrast enhancement on T1-weighted images. 15 , 40 However, MRI is not specific in the diagnosis of localized amyloidosis.
The amyloidoma in our case presented as a lytic lesion with a calcified matrix on conventional radiographs and CT scan. The lesion had signs of malignant tumor growth such as the destruction of the posterolateral aspect of the sacrum with extension over the right sacroiliac joint. Our differential diagnoses were chondrosarcoma, lymphoma, and metastatic disease. Such aggressive appearance has also been described for the two reported cases of localized amyloidosis of the sacrum. 25 , 26 In agreement with the literature, MRI findings in our case showed a spinal epidural mass but were otherwise unspecific for the diagnosis of the lesion. In accordance with Bruninx et al 25 and Griffin et al, 26 definite diagnosis could not be made based upon the imaging studies. Therefore, the final diagnosis requires the histopathologic demonstration of typical apple-green birefringence of the amyloid upon staining with Congo red and an examination under polarized light. 7 , 27 , 29 , 30 , 41 Subsequently, immunohistochemical characterization of the chemical type of amyloid is required. Because localized amyloidosis of the bone are composed of AL amyloid, immunostainings for kappa and lambda immunoglobulin light chains to prove clonal restriction should be performed. 29 , 41 To exclude secondary or inflammation-associated amyloidosis, immunohistochemical characterization should also include AA, anti-transthyretin, and β 2-microglobulin. 27
In the absence of neurologic symptoms, amyloidoma can be managed conservatively by observation and serial imaging. In cases with increasing pain, instability, or cord compression, surgery is indicated. Usually, a decompressive procedure with tumor excision is performed. Subsequently, anterior and/or posterior stabilization may be required. Surgery should aim at complete excision of the mass while avoiding any neurologic deficit. In large tumors with extensive soft tissue expansion, complete excision may not be possible or associated with a high risk of complications and morbidity. Given the lack of neurologic symptoms, one of the two so far reported cases was observed without specific treatment. 26 The other patient was treated surgically with bilateral laminectomy from S1 to S3 and complete excision of the tumor mass. No adjuvant therapy was performed. 25 The lesion reported by Bruninx et al was limited to the body of S2 with expansion into the left neuroforamen of S1. 25 At 75 × 60 × 55 mm, the amyloidoma we present was very large (Fig. 1) and complete resection was not possible without removal of the L5 to S3 nerve roots. To limit the morbidity, we decided to perform an intralesional resection with postoperative radiation therapy. The role of radiation therapy in localized amyloidoma of the bone has not been established, but seemed reasonable given the similar clinicopathologic features of localized amyloidoma and plamacytoma. 27 , 28 , 30 , 42 Other amyloid deposits or an underlying multiple myeloma have to be ruled out with adequate procedures, as in our patient.
Whether primary amyloidomas represent a benign plasma cell neoplasm or a plasmocytoma with local amyloid production is controversial. The outcome of localized amyloidoma is determined by the presence or the development of multiple myeloma. A localized extraosseous plasma cell clone associated with localized amyloidosis may not necessarily imply an increased risk of progressing to systemic disease. 34 , 43 , 44 Lipper and Kahn reported three patients with amyloidomas of the bone who did not develop multiple myeloma over a follow-up period of up to 12 years. 7 In contrast, Pambuccian et al stated that amyloidomas of the bone in fact represent plasmacytomas with a frequent later progression to multiple myeloma. 30 Unfortunately, this has been the case in our patient, who developed multiple myeloma 9 months after local therapy. Therefore, the initial diagnosis of primary solitary amyloidoma of the sacrum was revised to multiple myeloma-associated localized amyloidoma. This case highlights that careful follow-up of patients with localized amyloidosis is mandatory to ensure initiation of adequate systemic therapy.
Conclusion
Solitary amyloidoma of the sacrum is extremely rare. Surgical treatment is recommended in cases with instability or neurologic symptoms. Complete resection is recommended but may be associated with significant morbidity and functional impairment. Intralesional resection with adjuvant radiotherapy can result in a favorable outcome with recovery of symptoms and local tumor control. However, the overall prognosis depends on the presence or development of underlying systemic disease that require standard staging procedures and adequate follow-up and if necessary medical treatment of multiple myeloma.
Disclosures
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript. No funding was received for the study.