
Abstract
Study design
Systematic review and meta-analysis.
Objective
Minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) is a classic surgical procedure for the treatment of lumbar degenerative diseases (LDD). With the development of endoscopic technology, endoscopic transforaminal lumbar interbody fusion (Endo-TLIF) can also achieve adequate decompression and interbody fusion. However, whether Endo-TLIF is superior to MIS-TLIF has not been adequately studied. In this systematic review and meta-analysis, we aimed to evaluate the treatment difference between Endo-TLIF vs MIS-TLIF.
Methods
We conducted a systematic review and meta-analysis of the studies to compare the clinical outcomes and complications associated with Endo-TLIF vs. MIS-TLIF for the treatment of LDD. A literature search was conducted using the PubMed, Embase, Cochrane Library and Scopus databases for studies published up to April 1, 2022. Both retrospective and prospective studies that compared between Endo-TLIF and MIS-TLIF were included.
Results
A total of 8 studies involving 581 patients were finally included in this meta-analysis. Endo-TLIF significantly prolonged the operation time, but reduced the blood loss amount and length of hospital stay. Moreover, Endo-TLIF was superior to MIS-TLIF on relief of back pain and functional recovery in the early postoperative period. However, there were no significantly differences in long-term clinical outcomes, fusion rate and incidence of complications between Endo-TLIF and MIS-TLIF.
Conclusions
Endo-TLIF was similar to MIS-TLIF in the long-term clinical outcomes, fusion and complication rates. Endo-TLIF prolongs the operation time, but shortens the length of hospital stay, and has the advantages of less surgical trauma, less blood loss, faster recovery, and early postoperative back pain relief.
Introduction
In 1982, Harms and Rolinger first described transforaminal lumbar interbody fusion (TLIF). 1 The use of minimally invasive surgery of TLIF represents the most recent modification of methods to reduce the occurrence of intraoperative soft-tissue injury. Compared with traditional open surgery, the minimally invasive approach is a safe and effective method with advantages of less blood loss, fewer postoperative pain, shorter hospital stays, fewer infections, and fast recovery after surgery. 2 MIS-TLIF has been the classical procedure of minimally invasive lumbar fusion for the treatment of partial lumbar degenerative diseases requiring fusion, such as degenerative lumbar disc herniation (LDH), lumbar spinal stenosis (LSS), lumbar spondylolisthesis or instability, etc. 3
Percutaneous endoscopic lumbar discectomy (PELD) techniques have undergone great development in the past few decades since professor Kambin experimentally introduced arthroscopy to treat LDH.4-6 Nowadays, indications of PELD and related techniques have been extended from LDH to LSS.7,8 With the advance of endoscopic decompression technology, TLIF procedure with the assistance of percutaneous endoscopy has been developed for the treatment of LDD.9,10 The Endo-TLIF technique was developed on the basis of the Kambin’s triangle method, it allows direct reaching the disc for decompression and fusion without resection of the lamina, superior and inferior articular processes, and ligamentum flavum.11,12 Theoretically, Endo-TLIF technique, compared with traditional MIS-TLIF, was more minimally invasive with less soft-tissue injury and less perioperative blood loss. However, the steep learning curve in this technique led to a huge challenge for spinal surgeons. It is not clear Whether the Endo-TLIF technique is superior to MIS-TLIF for LDD. Therefore, the purpose of this systematic review and meta-analysis was to compare clinical outcomes and complications between the two techniques in treating LDD.
Methods
A systematic review of the literature was conducted using the PubMed, Cochrane Library, Embase and Scopus databases. Articles published till April 1, 2022 were analyzed. This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and AMSTAR (Assessing the methodological quality of systematic reviews) guidelines.13,14 The systematic review was registered in the PROSPERO (International Prospective Register of Systematic Reviews - NHS; Registration Number: CRD42021286318).
Search Strategy
A literature search was performed using PubMed, Embase, Cochrane Library and Scopus databases on April 1, 2022. The following keywords were used in the search: “endoscopic,” “endoscopy,” “interbody fusion,” “lumbar fusion,” “minimally invasive,” “MI,” “transforaminal lumbar interbody fusion,” and “TLIF.” All the relevant literatures were screened by two reviewers independently based on title and/or abstract, following this step, the full text of the manuscripts was further investigated based on the inclusion and exclusion criteria. Disagreements were resolved through consensus with the involvement of a third reviewer.
Inclusion Criteria for Studies
Studies were considered to be eligible according to the following inclusion criteria: (1) patients diagnosed with single-level or two-level lumbar degenerative diseases including degenerative lumbar disc herniation, lumbar spinal stenosis, lumbar spondylolisthesis or instability; (2) compared between Endo-TLIF and MIS-TLIF in the treatment of lumbar degenerative diseases; (3) provided data on one or more of the following measures to describe the outcomes: operation time, blood loss amount, length of hospital stay, VAS of LBP and/or leg pain, ODI, fusion rate and complications. (4) published in English.
Exclusion Criteria
Studies were excluded from this systematic review according to the following exclusion criteria: (1) literature reviews, case reports, conference abstracts and editorials; (2) Biomechanical, animal, cadaver research; (3) unable to access the full text or extract data.
Data Extraction
The data extraction from the included studies was performed using a predesigned extraction form. The extracted data included productive country, year of publication, study design, patient demographics, operation characteristics, clinical outcomes, length of hospital stay, follow-up time, fusion rate and incidence of complications. Data extraction was first performed by one reviewer according to a pre-designed form, then another reviewer repeated this step and checked the previously extracted form, and if inconsistencies were found, the two would re-extract and proofread, to control the accuracy.
Quality Assessment for Studies
The quality of all included articles was assessed independently by two reviewers. The Newcastle–Ottawa scale (NOS) was used to assess quality for the cohort and case-controlled studies. 15 Studies assessed via the NOS can be assigned a total of 9 stars, with a score of 7 to 9 considered high quality, 4 to 6 considered moderate quality, and 3 or below considered low quality. The Cochrane risk of bias tool (RoB 2 tool) was used to assess bias for the randomized controlled trials (RCTs). 16 Discrepancies in the assessment were resolved through discussion until a consensus was reached.
Statistical Analysis
The continuous outcomes were presented as mean differences (MD) or standardized mean differences (SMD), and odds ratios (OR) were presented for binary variables. The confidence intervals (CI) were reported at the 95% level. Statistical significance was set at P-value of <.05. The random-effects model was used for all outcomes. The heterogeneity among the studies was qualitatively and quantitatively evaluated by Cochran’s Q test and I2 statistics. The heterogeneity was considered as significant When I2 value of >50%. Microsoft Excel 2021 (Microsoft, Redmond, WA) was used to summarize the data. Statistical analyses and forest plots were performed by Cochrane Review Manager (version 5.3; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration). The clinical outcomes were defined as short-term (within 3 months), and long-term (more than 12 months), and data were analyzed according to the closest time interval.
Results
The PRISMA flow diagram of this study is given in Figure 1. A total of 158 articles were screened, and 28 full-text articles were selected for a detailed investigation, of which 8 studies were finally included in the meta-analysis. One study was a randomized controlled trial,
17
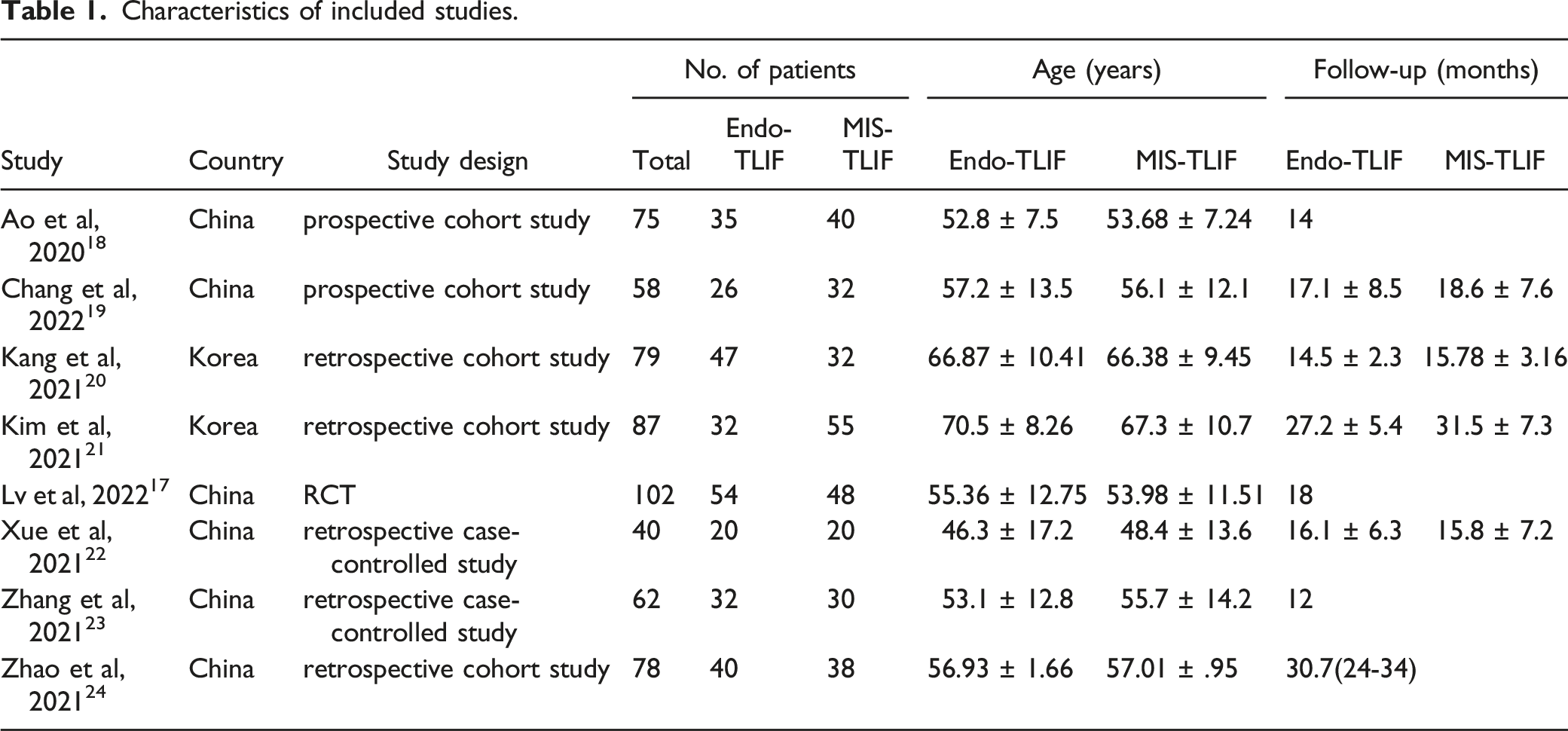
two studies were prospective studies,18,19 and 5 studies were retrospective studies.20-24 The characteristics of these included studies are presented in Table 1. The meta-analysis included a total of 581 patients, 286 of which were treated with Endo-TLIF and 295 with MIS-TLIF. The mean age in the Endo-TLIF group was 58.13 years compared with 58.18 years in the MIS-TLIF group. The length of follow up in the all included studies was more than one year with a range of 12 months
23
to 34 months.
24
Seven of all included studies evaluated single-level fusion,17-19,21-24 one study reported fusion of one or two levels.
20
Two case-controlled studies and five cohort studies were considered to be of high methodological quality with a NOS score of ≥7 (Supplemental Table 1 and Table 2). One RCT was assessed as a low risk of bias (Supplemental Figure 1). Flow diagram of literature search and selection of included studies for meta-analysis. Characteristics of included studies. Complications reported in the included studies.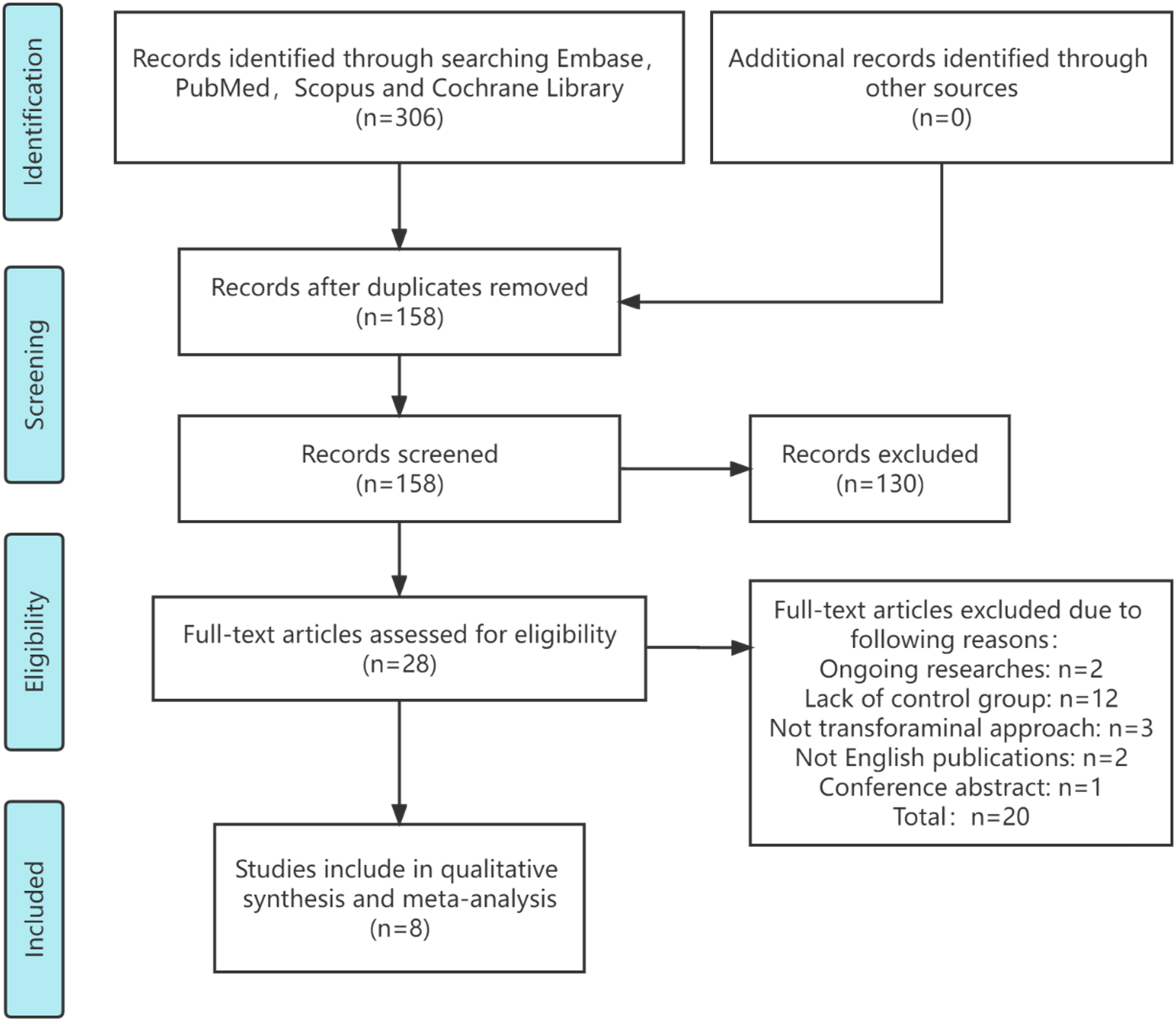
VAS Score of Low Back Pain
All 8 studies reported the VAS score of low back pain (LBP).17-24 Two studies were excluded from the analysis due to incomplete data.20,24 Five studies reported the VAS score of LBP within 3 months postoperative,17,18,21-23 and six studies reported at least 12 months after surgical procedures.17-19,21-23 The VAS score of Endo-TLIF group in the short-term follow-up was significantly lower compared to the MIS-TLIF group (P = .002; SMD = -.81 [95% CI = -1.33−-.30]) (Figure 2A). However, there were no significant differences between the two techniques at the long-term follow-up (P = .14; SMD = -.49 [95% CI = -1.13−.16]) (Figure 2B). Comparison of VAS score of LBP at the short-term (A) and long-term follow-up (B) between the Endo-TLIF group and MIS-TLIF group. The short-term was defined as within 3 months, and long-term was defined as more than 12 months.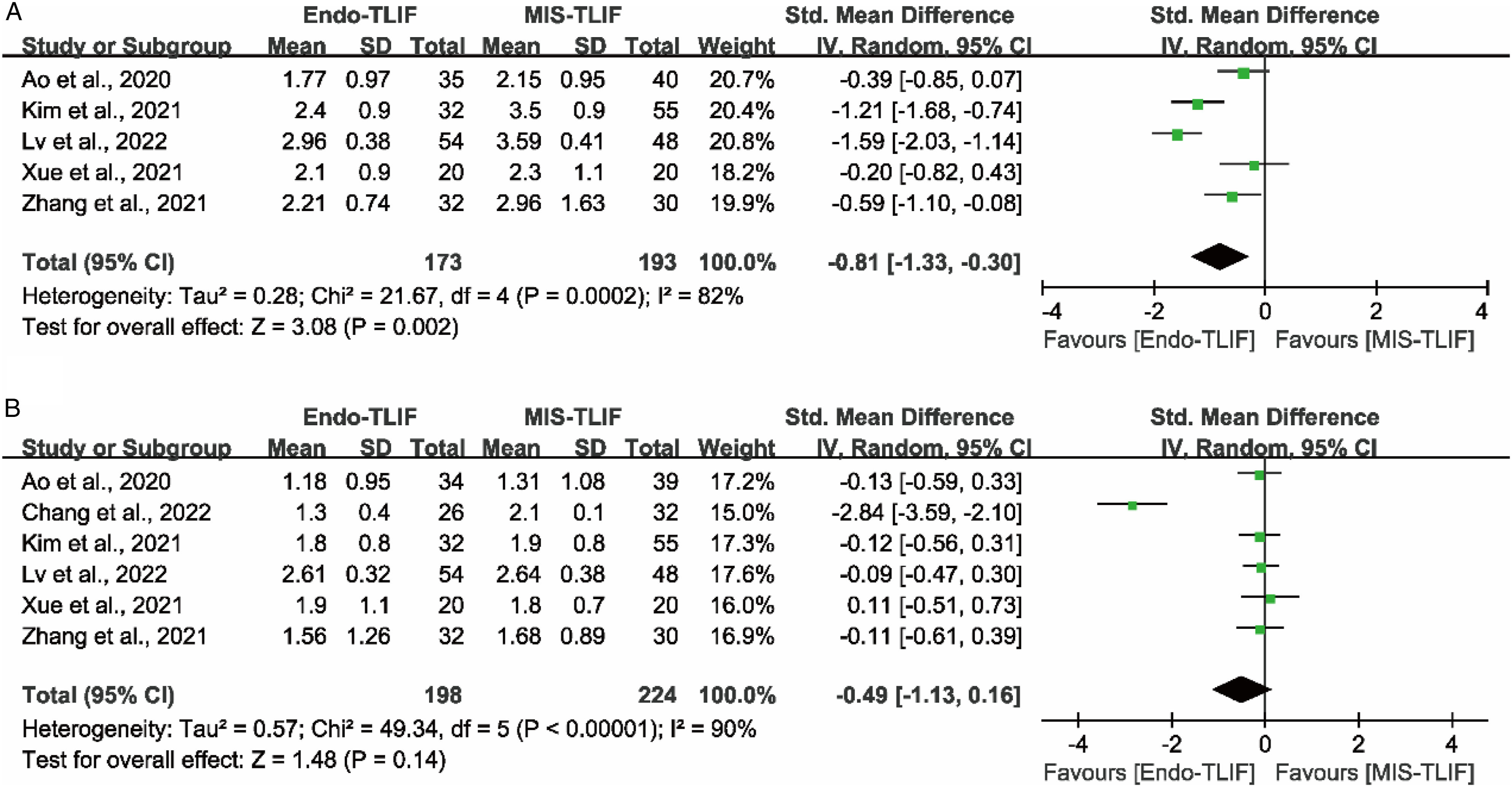
VAS Score of Leg Pain
Seven studies reported the VAS score of leg pain,17-23 one of which was excluded from the analysis because of incomplete data.
24
Five studies reported the VAS score of leg pain at the short-term follow-up,17,18,21-23 and 6 studies reported at the long-term follow-up.17-19,21-23 There were no significant differences in the VAS score of leg pain between the Endo-TLIF group and MIS-TLIF group either at the short-term (P = .81; SMD = .04 [95% CI = -.25−.33]) (Figure 3A) or long-term follow-up (P = .87; SMD = .03 [95% CI = -.32−.39]) (Figure 3B). Comparison of VAS score of leg pain at the short-term (A) and long-term follow-up (B) between the Endo-TLIF group and MIS-TLIF group. The short-term was defined as within 3 months, and long-term was defined as more than 12 months.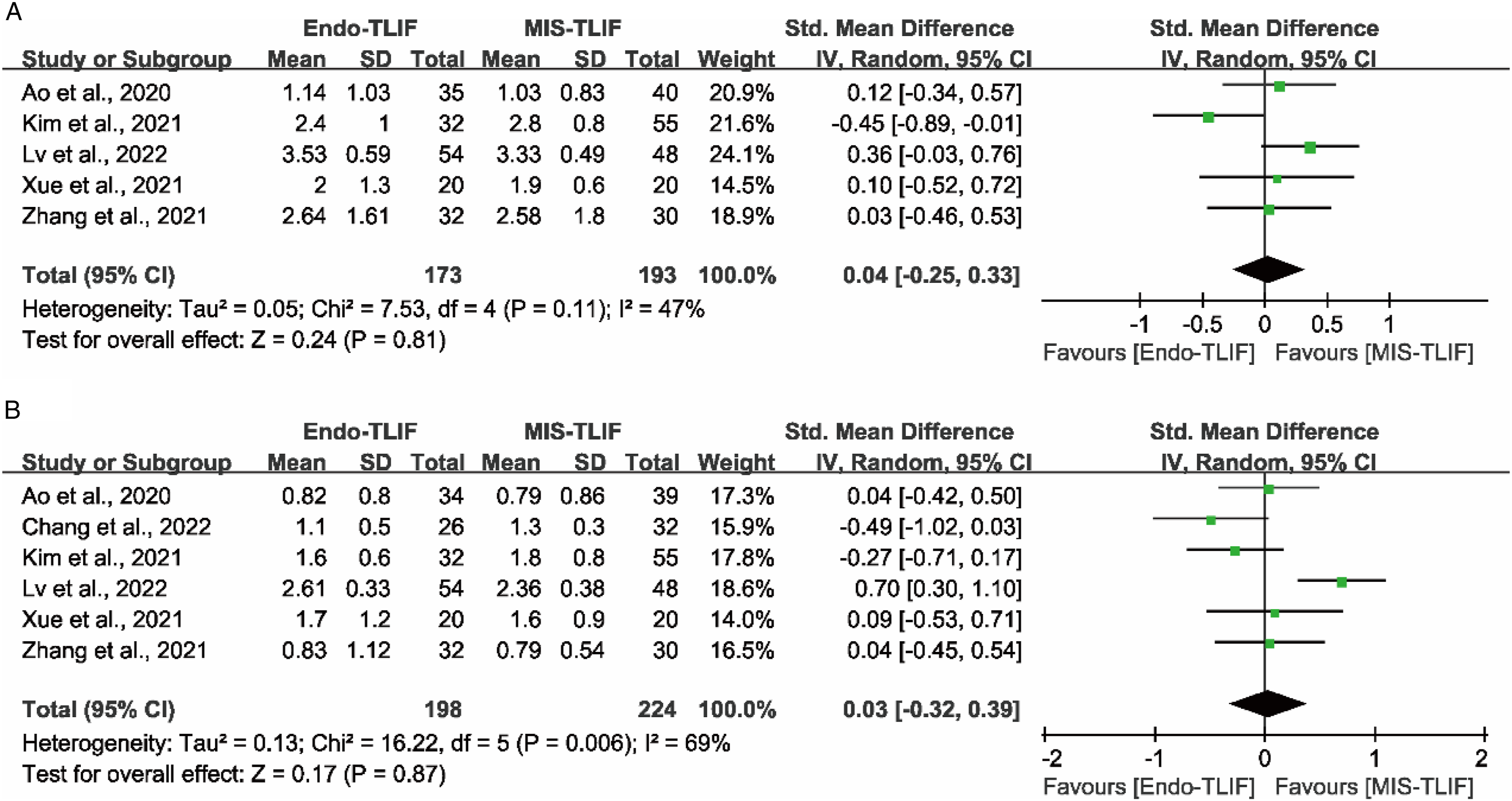
ODI
The ODI is tool used to evaluate patients’ functional disabilities with a total score of 50 points.
25
The lower the score, the better the patient’s functional condition. Seven studies compared the effect between Endo-TLIF and MIS-TLIF on the ODI,17-23 one of which was excluded from the analysis owing to incomplete data.
20
Five studies reported the ODI score at the short-term follow-up,17,18,21-23 and 6 studies reported at the long-term follow-up.17-19,21-23 The meta-analysis showed that the improvement of patients’ functional status in the Endo-TLIF group was significantly better than those in the MIS-TLIF group at a short-term follow-up (P = .008; SMD = -.41 [95% CI = -.71−-.11]) (Figure 4A). However, there were no significant differences between the two techniques at the long-term follow-up (P = .28; SMD = -.11 [95% CI = -.30−.09]) (Figure 4B). Comparison of ODI score at the short-term (A) and long-term follow-up (B) between the Endo-TLIF group and MIS-TLIF group. The short-term was defined as within 3 months, and long-term was defined as more than 12 months.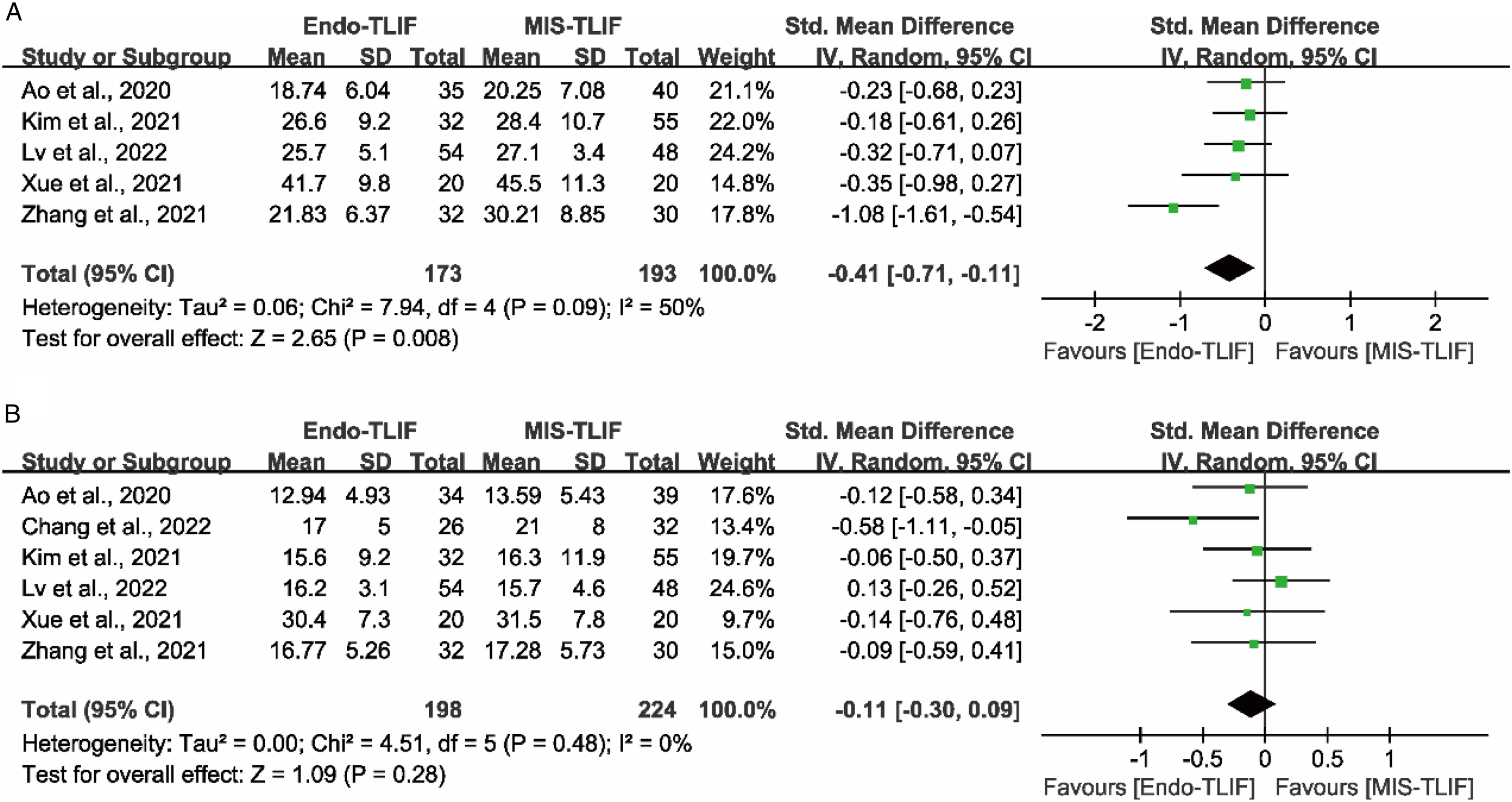
Operation Time
The differences of operation time between the Endo-TLIF and MIS-TLIF groups were reported in all 8 studies.17-24 The operation time in the Endo-TLIF group was significantly longer than those in the MIS-TLIF group (P = .002; SMD = 1.79 [95% CI = .68−2.89]) (Figure 5A). Comparison of operation time (A), blood loss mount (B) and length of hospital stay (C) between the Endo-TLIF group and MIS-TLIF group.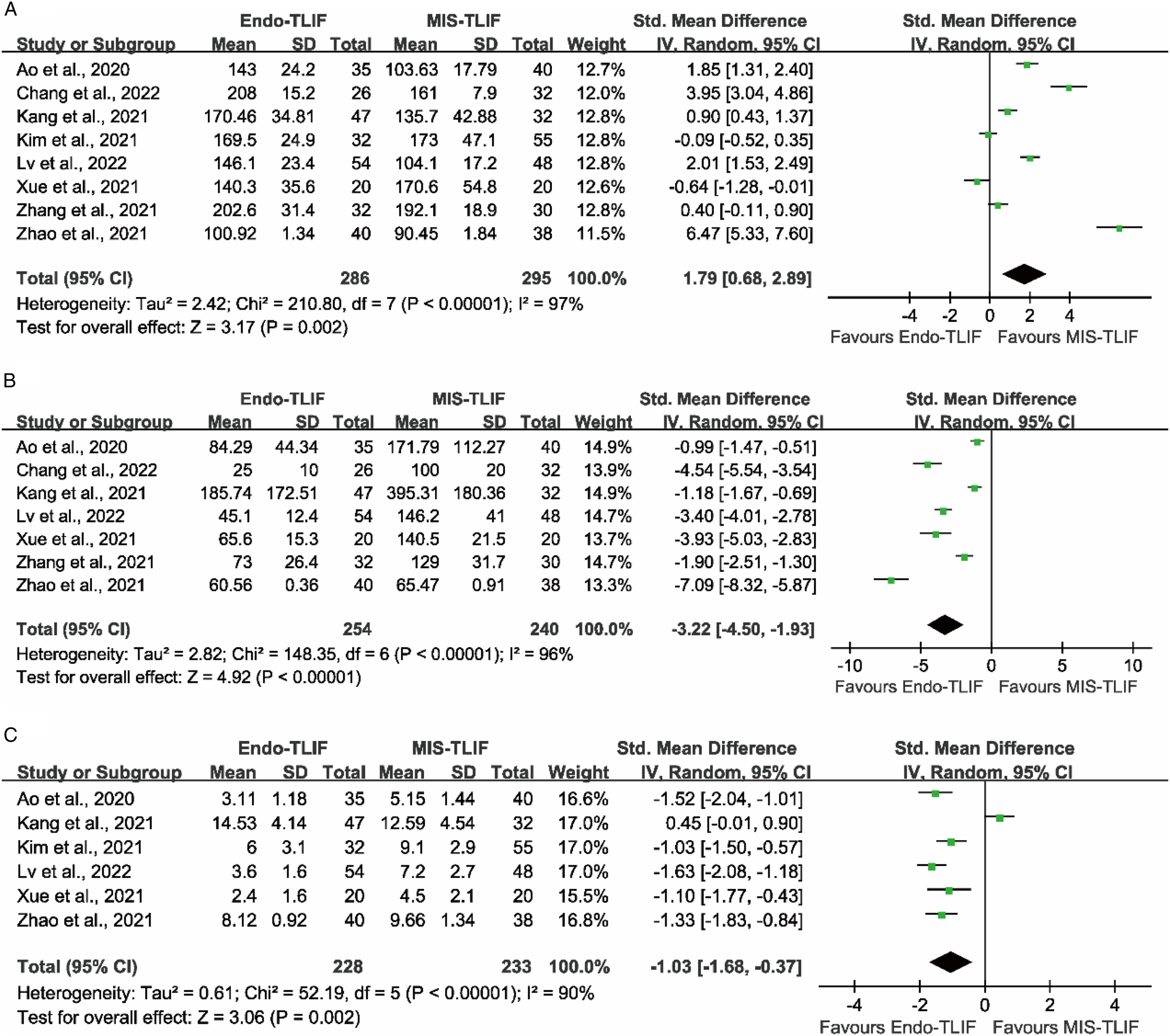
Blood Loss Amount
Seven studies reported the blood loss amount.17-20,22-24 The meta-analysis showed that the blood loss amount in the Endo-TLIF group was significantly less than the MIS-TLIF group (P < .001; SMD = -3.22 [95% CI = -4.50−-1.93]) (Figure 5B).
Length of Hospital Stay
The length of hospital stay was reported in six studies.17,18,20-22,24 The Endo-TLIF group was significantly shorter than those in the MIS-TLIF group in the length of hospital stay (P = .002; SMD = -1.03 [95% CI = -1.68−-.37]) (Figure 5C).
Fusion Rate
All 8 studies reported the differences in the fusion rate between the Endo-TLIF and MIS-TLIF group.17-24 Two studies were excluded from the analysis due to incomplete data.19,20 The fusion rate was 92.0% (195/212) in the Endo-TLIF group and 93.9% (216/230) in the MIS-TLIF group. The meta-analysis showed no significant differences between the two surgical procedures (P = .47; SMD = .75 [95% CI = .35−1.63]) (Figure 6A). Comparison of fusion rate (A) and incidence of complications (B) between the Endo-TLIF group and MIS-TLIF group.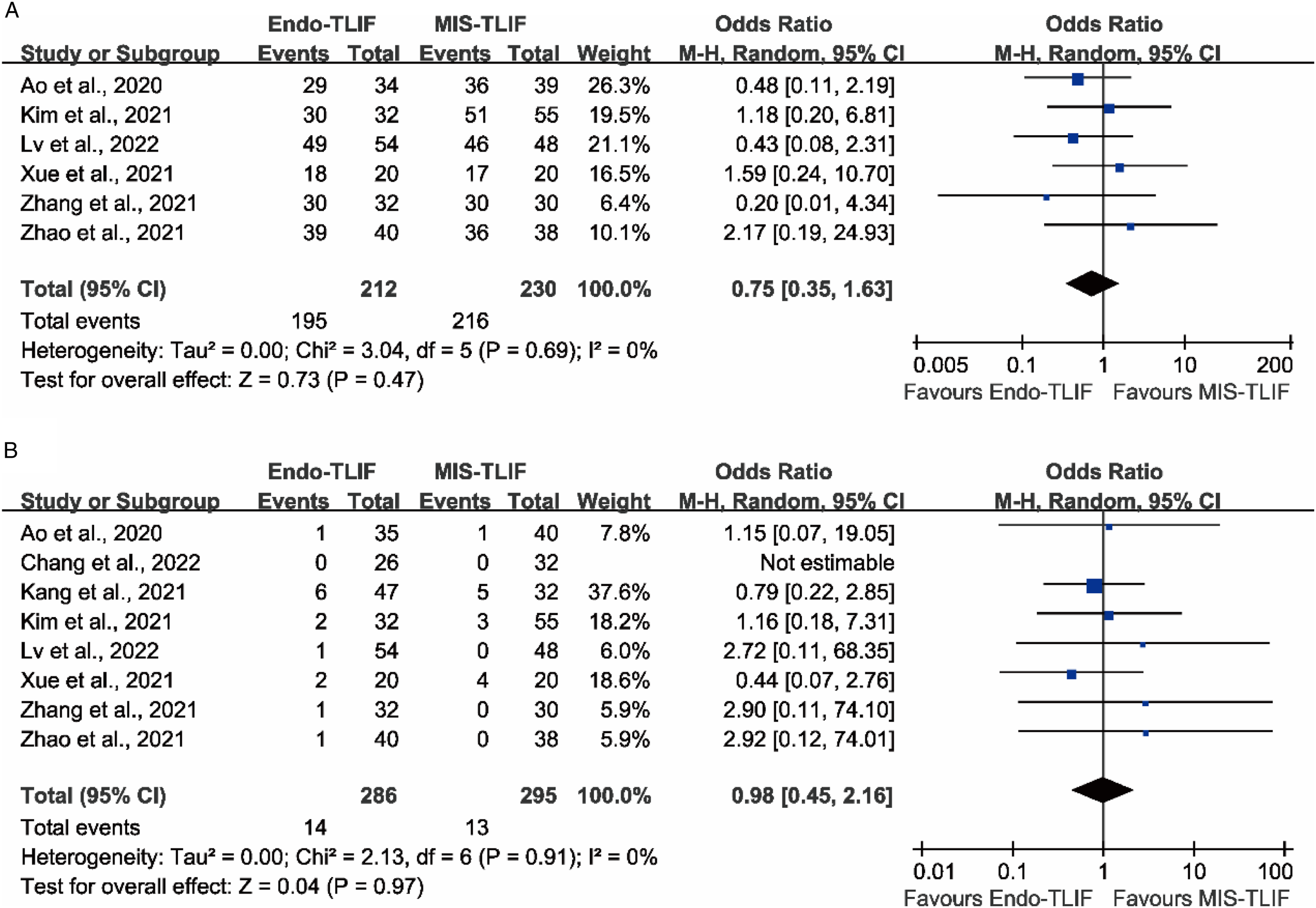
Complications
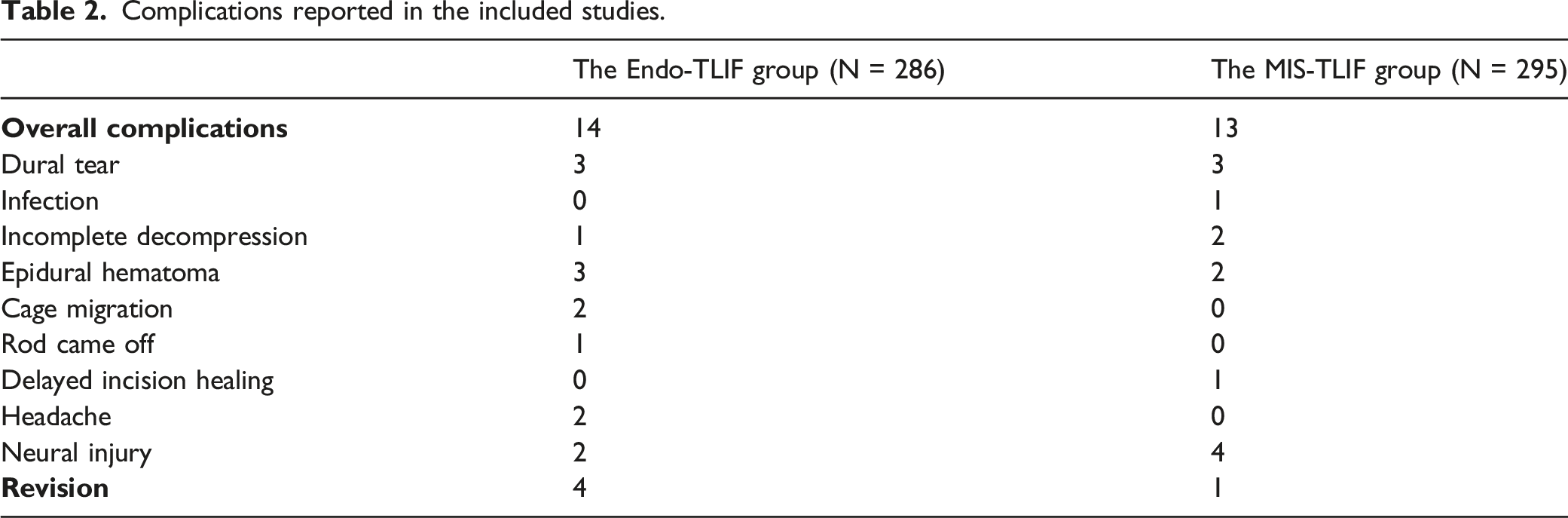
Complications related to the techniques were reported in all eight studies.17-24 The overall incidence of complications was 4.9% for Endo-TLIF group vs. 4.4% for MIS-TLIF group. The specific complications related to the two techniques reported in the included studies were summarized in Table 2. The meta-analysis showed that there were no significant differences between the groups (P = .97; OR = .98 [95% CI = .45−2.16]) (Figure 6B).
Discussion
Clinical Outcomes
The present meta-analysis suggested that both Endo-TLIF and MIS-TLIF could obtain satisfactory clinical results. The Endo-TLIF group was significantly better than MIS-TLIF in terms of low back pain relief and functional improvement in the early postoperative period, especially within 3 months after surgery. This result might be related to the endoscopic spine approach which using muscle dilation rather than muscle damage.17,24 The approach can better minimize surgical trauma and preserve the lamina and superior and inferior articular processes. As a result, Endo-TLIF showed less normal soft-tissue injuries and had a more positive effect on improving early postoperative LBP and functional recovery. However, there were no significant differences in LBP and leg pain, and functional improvement between two techniques at long-term follow-up. These conclusions were similar to previous study. 26
Surgical Trauma
The present study showed that Endo-TLIF significantly reduced blood loss amount and length of hospital stay compared to MIS-TLIF. Endoscopic fusion technique can maximize the preservation of normal muscle and ligament, and posterior osseous structures, compare to traditional MIS-TLIF using a Quadrant channel 17 . Furthermore, the full visualization system which provides a clearer surgical field of vision allows surgeons to stop bleeding in advance, and avoid injuries to the blood vessels and nerves under the protection of a working tube. 24 Thus, Endo-TLIF resulted in less blood loss and faster postoperative recovery. However, the operation time in the Endo-TLIF group was significantly longer than those in the MIS-TLIF group. Undeniably, similar to the PELD technique, Endo-TLIF requires a steep learning curve, requiring the surgeon to have extensive endoscopic experience and a thorough understanding of foraminal anatomy to ensure that each step of the procedure is safe and effective. 23 In addition, adequate decompression and percutaneous pedicle screw fixation can be time-consuming.
Fusion Rate
For endoscopic spinal fusion technique, the lack of available amount of autograft or adequate manipulation space to properly delivery or placement of suitable sized cages made it difficult to achieve sufficient interbody fusion. 9 Thus, small sized or expandable cages became an alternative. Some studies suggested that the use of smaller or expandable cages might lead to nonunion, cage subsidence or migration.9,27,28 In MIS-TLIF surgeries, incomplete endplate preparation or endplate injury may also result in fusion failure or cage subsidence.29,30 However, endoscopic visualization aids in visual confirmation of the extent and adequacy in endplate preparation, which can help facilitate interbody fusion in some patients. 9 The meta-analysis showed no statistically significant difference in fusion rates between the two groups, both as high as 92%, which is slightly lower than previous study. 26 Therefore, both Endo-TLIF and MIS-TLIF could achieve satisfactory fusion rates.
Complication
The overall incidence of complications for Endo-TLIF technique reported in previous case-series studies ranged from 0% to 38.6%, which included dural tear, hematoma, infection, residual pain, postoperative dysesthesia, motor weakness, hardware failure and so on.10-12,31-35 The present meta-analysis showed that the overall complication rates of Endo-TLIF and MIS-TLIF were 4.9% and 4.4% respectively, which were significantly lower than a previous systematic review (10% vs. 12.7%) 26 . The incidence of complications may also be influenced by the surgeon's familiarity with endoscopic spinal fusion techniques. Kolcun et al reported complications included two cases of cage migration, one case of osteomyelitis, and one case of endplate fracture, three of which occurred in the first 50 cases. 10 The gradually increased familiarity and efficiency of their surgical and anesthesia teams led to an improvement in the safety of subsequent surgical cases. Furthermore, the use of conscious sedation in Endo-TLIF surgery reduces the risk associated with general anesthesia and facilitates real-time neurological feedback from the patient. 9
This study also found that the Endo-TLIF group had a higher revision rate than the MIS-TLIF group though there are no statistical differences. In Endo-TLIF group, revision surgeries were performed in four patients, one of which owing to incomplete decompression, 20 one case due to postoperative hematoma, 21 one case because of rod came off, 23 one owing to cage migration. 24 One patient accepted revision surgery because of postoperative hematoma in the MIS-TLIF group. 21 The shortage of experience and proficiency for beginners which lead to a steep learning curve may be the main reasons for the high revision rate of the Endo-TLIF technique, although its incidence of complication is similar to the MIS-TLIF technique. However, it cannot be denied that Endo-TLIF technique offers the advantages of limited invasiveness, less blood loss, short recovery time and no need for postoperative drainage. 23
Limitations
This study has some limitations. First, there is a high degree of statistical heterogeneity among the included studies. We believe that factors such as differences in follow-up periods, patient-reported outcomes, and assessment criteria used by investigators are the main reasons for the heterogeneity. Besides, although all study included in this meta-analysis were comparative studies, there was only one RCT among them. Therefore, these conclusions need to be verified by more RCT studies in the future. In addition, less than 10 studies were included, so analyses of meta-regression and publication bias were not performed. We did not perform subgroup analyses of fusion segment level, number, type of endoscopy, etc., which may have contributed to differences in final results.
Conclusions
The present study demonstrates that Endo-TLIF is an effective and safe surgical technique in the treatment of LDD. Endo-TLIF was similar to MIS-TLIF in the long-term clinical outcomes, fusion and complication rates. Endo-TLIF prolongs the operation time, but shortens the length of hospital stay, and has the advantages of less surgical trauma, less blood loss, faster recovery, and early postoperative back pain relief.
Supplemental Material
Supplemental Material - Comparison of Clinical Outcomes and Complications Between Endoscopic and Minimally Invasive Transforaminal Lumbar Interbody Fusion for Lumbar Degenerative Diseases: A Systematic Review and Meta-analysis
Supplemental Material for Comparison of Clinical Outcomes and Complications Between Endoscopic and Minimally Invasive Transforaminal Lumbar Interbody Fusion for Lumbar Degenerative Diseases: A Systematic Review and Meta-analysis by Haiwei Guo, MD, Yuke Song, MD, Rui Weng, MD, Han Tian, MD, Jiayao Yuan, MD, and Ying Li, PhD in Global Spine Journal.
Footnotes
Author Contributions
Haiwei Guo and Yuke Song led the whole research and contributed to the conception of the study. Jiayao Yuan and Han Tian were responsible to the data collection. Haiwei Guo, Yuke Song and Rui Weng performed the data analyses and wrote the manuscript. Haiwei Guo, Yuke Song and Ying Li contributed significantly to manuscript preparation and discussion.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
Registration Number: CRD42021286318
Data Availability
Data are available on reasonable requests by qualified investigators to the corresponding author.
Provenance and Peer Review
Not commissioned, externally peer-reviewed.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.