
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To evaluate the risk of subsequent lumbar fusion following sacroiliac (SI) joint fusion in patients with lumbar degenerative disease (LDD) and identify associated risk factors.
Methods
Patients with undergoing SI joint fusion with concurrent diagnosis of LDD between 2010-2022 were identified in the PearlDiver Mariner Database. Those with prior lumbar fusion were excluded. A 1:10 propensity-matched control group of LDD patients without SI joint fusion was created. Logistic regression assessed the odds of subsequent lumbar fusion. Risk factors were analyzed using multivariable regression. Kaplan-Meier analysis evaluated time to lumbar fusion over 5 years.
Results
Among 22 957 patients with LDD undergoing SI joint fusion, 4.5% required subsequent lumbar fusion. SI joint fusion was associated with significantly higher odds of subsequent lumbar fusion compared to controls (OR: 2.97 [2.77-3.19], P < 0.001). Risk factors included open SI joint fusion (aOR: 2.78), bilateral fusion (aOR: 1.97), Elixhauser Comorbidity Index ≤ 4 (aOR: 1.91), preoperative opioid use (aOR: 1.53), osteoarthritis (aOR: 1.45), fibromyalgia (aOR: 1.26), and age ≥ 70 (aOR: 1.15). Minimally invasive and unilateral SI joint fusion were associated with reduced risk. Kaplan-Meier analysis showed increased lumbar fusion risk beyond 1250 days post-SI joint fusion.
Conclusions
SI joint fusion significantly increases the risk of subsequent lumbar fusion in patients with LDD, particularly following open or bilateral procedures. These findings emphasize the need for thorough preoperative risk assessment and patient counseling regarding potential long-term lumbar effects. Future research should investigate clinical outcomes and biomechanical mechanisms underlying stress redistribution after SI joint fusion.
Keywords
Introduction
The sacroiliac (SI) joint is the largest axial joint in the body, acting as a damper to transfer loads between spine and the lower extremities. 1 The SI joint is a commonly overlooked source of low back pain (LBP), with estimates that it is responsible for 10%-45% of LBP. 2 Common causes of SI joint pain include capsular and ligamentous tension, hypo or hypermobility, soft tissue injury, inflammation, and extraneous compression or shearing forces. 3 Diagnosis of SI joint pain includes provocative maneuvers such as the distraction, thigh thrust, compression, Gaenslen, and FABER tests, and is confirmed with a diagnostic anesthetic block that results in >70% reduction in pain. 4 When conservative treatments such as physical therapy, steroid injections, and radiofrequency nerve ablation fail, patients may be indicated for SI joint fusion, which has been shown to lead to significant improvements in patient pain and functionality.4,5 This has led to a dramatic increase in utilization of SI joint fusion in the United States, rising annually by an average of 33% between 2010 and 2021. 6
Many studies have highlighted that lumbar fusion can increase motion and stress across the SI joint, contributing to adjacent segment disease. 7 In contrast, the impact of SI joint fusion on the lumbar spine has received much less attention. In a finite element analysis, Lindsay et al found that SI joint fusion increases adjacent segment motion in the lumbar region by <5%. 8 However, there is limited research investigating the long-term clinical effects of SI joint fusion on the lumbar spine.
The purpose of this study was to utilize a national database to investigate whether patients with lumbar degenerative disease (LDD) undergoing SI joint fusion are at an increased risk for future lumbar fusion compared to those without a history of SI joint fusion. Additionally, risk factors for future lumbar fusion in these patients undergoing SI joint fusion were analyzed.
Methods
Data Source and Study Population
This retrospective cohort study utilized the PearlDiver Mariner Database (PearlDiver Technologies, Colorado Springs, CO, USA), a large, nationwide insurance claims dataset containing de-identified information on approximately 157 million patients across all payer types. The database includes demographic, diagnostic, and procedural information from inpatient and outpatient encounters between 2010 and 2022. As this study used anonymized data, institutional review board approval and informed consent were not required.
Identification of Study Cohorts
Patients were identified using International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 and ICD-10), along with Current Procedural Terminology (CPT) codes. The complete list of diagnostic codes used for cohort identification is provided in Supplemental Table 1.
Two cohorts were defined for comparison. The first cohort (SI joint fusion group) included patients diagnosed with lumbar degenerative disease who subsequently SI joint fusion for SI joint dysfunction. To ensure that SI joint fusion was performed independently of lumbar fusion, patients were excluded if they had undergone lumbar fusion prior to or within 1 week following the SI joint procedure. However, patients with prior lumbar decompression were included. SI joint fusions performed for trauma, malignancy, or infection were excluded.
The second cohort (control group) comprised patients diagnosed with LDD without history of SI joint fusion. These patients served as controls and represented individuals with degenerative lumbar pathology who did not undergo SI joint fusion during the study period.
Both cohorts were limited to adults aged 18 years or older and required a minimum of 90 days of continuous enrollment both before and after the index procedure or diagnosis. Patients were excluded from both groups if they underwent lumbar fusion for trauma, malignancy, or infection during the study period.
Study Endpoints
The primary aim of this study was to evaluate whether patients with LDD who underwent SI joint fusion for SI joint dysfunction were at increased risk of subsequent lumbar fusion compared to patients with LDD who did not undergo SI joint fusion over the study period. Subsequent lumbar fusion was used as a proxy for progression of LDD. The time interval between SI joint fusion and lumbar fusion was also assessed. Secondary objectives included identifying risk factors associated with undergoing lumbar fusion following SI joint fusion. These included patient age, sex, comorbidity burden as measured by the Elixhauser Comorbidity Index (ECI), preoperative opioid use within 6 months of surgery, surgical characteristics of the SI joint fusion procedure (such as open vs minimally invasive (MIS) technique and unilateral vs bilateral approach), previous lumbar decompression, and lumbar diagnoses prior to the SI joint fusion procedure (spondylolisthesis, lumbar disc herniation, spinal stenosis, scoliosis, radiculopathy). The distinction between open and MIS procedures was incorporated beginning in 2015, when CPT code 27279 was introduced to denote MIS techniques. Indications for lumbar fusion following the SI joint fusion procedure were analyzed by investigating which LDD diagnostic codes were billed on the day of the lumbar fusion.
Statistical Analysis
Statistical analyses were performed using RStudio (version 4.4.2) within the PearlDiver Mariner platform. Continuous variables were compared using Student’s t-test, and categorical variables were analyzed using Pearson’s chi-squared test. To control for confounding variables, the control cohort of patients with LDD but no SI joint fusion was exact propensity-matched to the SI joint fusion cohort at a 1:10 ratio based on age, sex, and ECI.
To evaluate the association between SI joint fusion and the likelihood of subsequent lumbar fusion, a univariate logistic regression model was used. Kaplan-Meier survival analysis was performed to assess the time from initial diagnosis of LDD to lumbar fusion surgery over a 5-year period. Among patients in the SI joint fusion cohort, univariate and multivariable logistic regression models were used to evaluate predictors of subsequent lumbar fusion, adjusting for age, sex, and ECI. A P-value < 0.05 was considered statistically significant for all analyses.
Results
Cohort Identification and Matching
Baseline Demographic Characteristics of Propensity-Matched Patients with Lumbar Degenerative Disease With vs Without Sacroiliac Joint Fusion
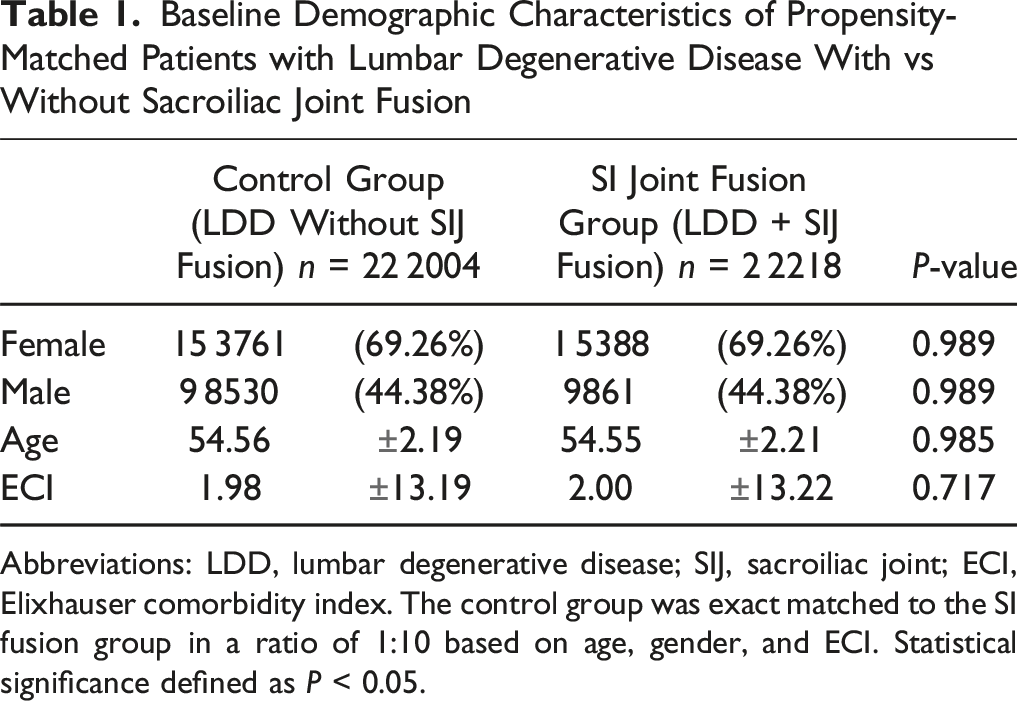
Abbreviations: LDD, lumbar degenerative disease; SIJ, sacroiliac joint; ECI, Elixhauser comorbidity index. The control group was exact matched to the SI fusion group in a ratio of 1:10 based on age, gender, and ECI. Statistical significance defined as P < 0.05.
Comparison of SI Joint Fusion vs Control Cohort
Odds of Subsequent Lumbar Fusion in Patients With Lumbar Degenerative Disease Undergoing Sacroiliac Joint Fusion

Abbreviations: LDD, lumbar degenerative disease; SIJ, sacroiliac joint. The control group was exact matched to the SI fusion group in a ratio of 1:10 based on age, gender, and ECI. Univariate logistic regression was utilized. Statistical significance defined as P < 0.05; significant values bolded.
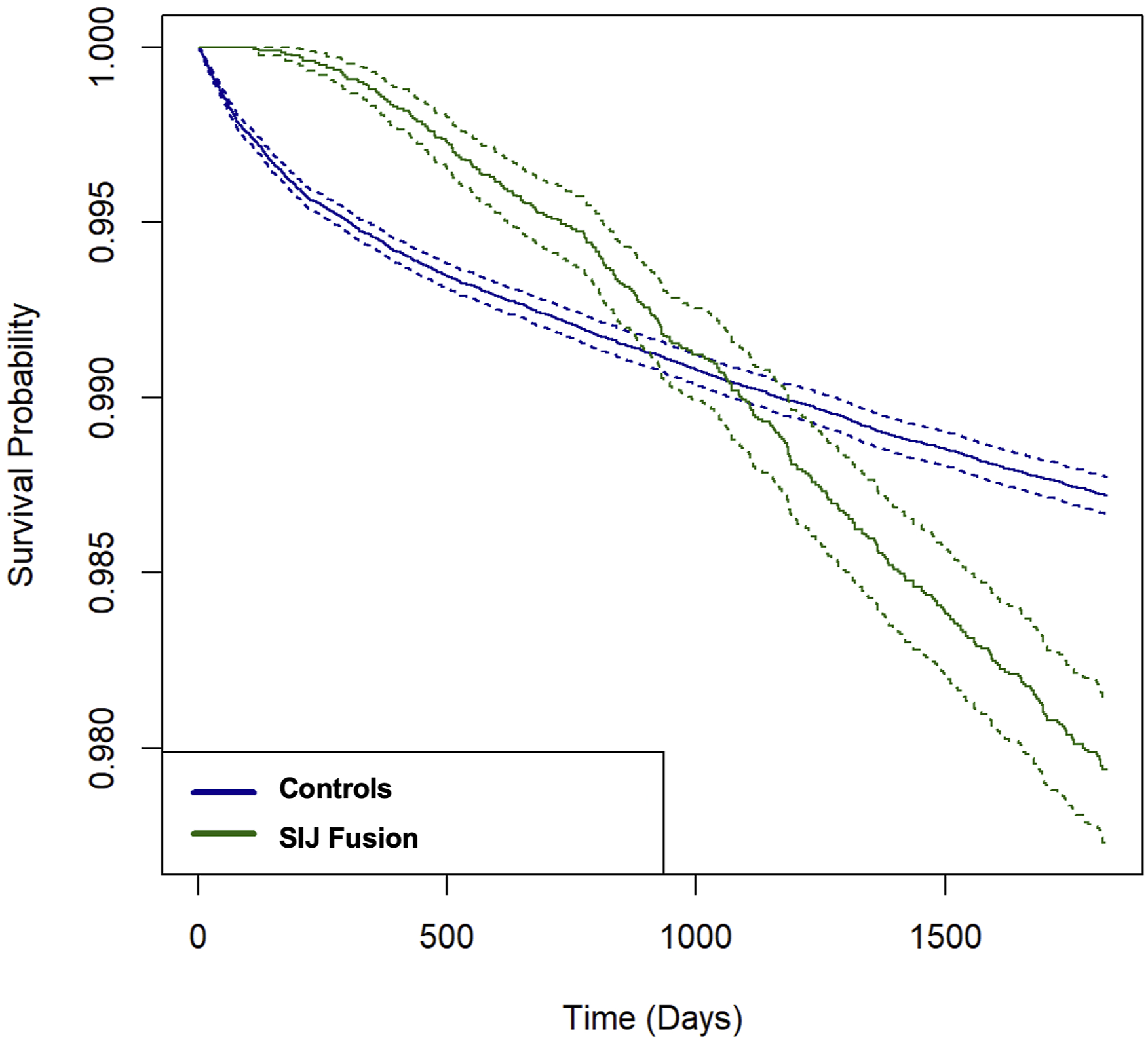
Kaplan-Meier Curve Showing 5-Year Lumbar Fusion Risk by SI Joint Fusion History in Lumbar Degenerative Disease Patients
Subgroup Analysis of the SI Joint Fusion Cohort
Demographics, Comorbidities, and Procedural Characteristics of Patients Undergoing Sacroiliac Joint Fusion, Stratified by Future Lumbar Fusion
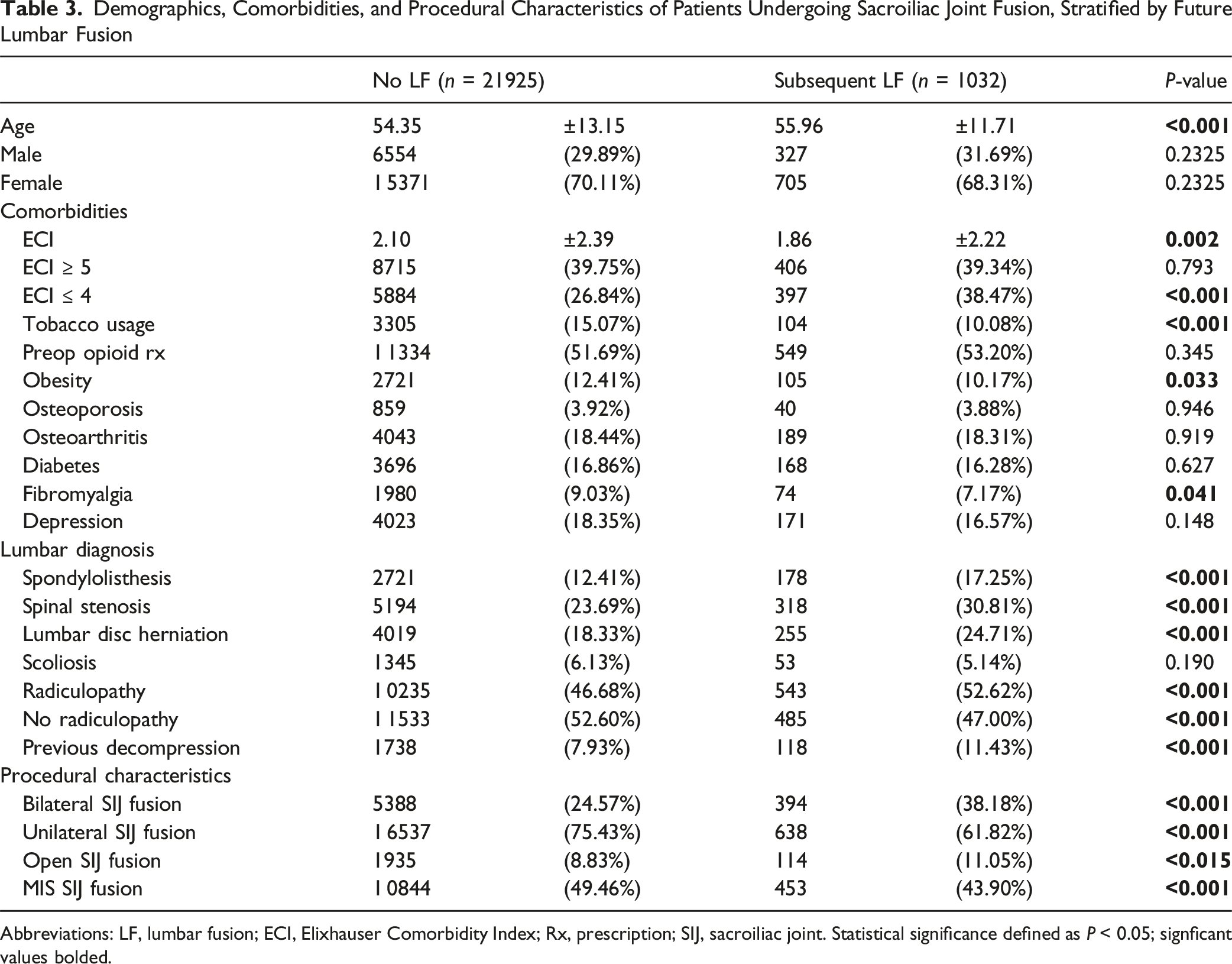
Abbreviations: LF, lumbar fusion; ECI, Elixhauser Comorbidity Index; Rx, prescription; SIJ, sacroiliac joint. Statistical significance defined as P < 0.05; signficant values bolded.
Risk Factor Analysis for Subsequent Lumbar Fusion Following Sacroiliac Joint Fusion
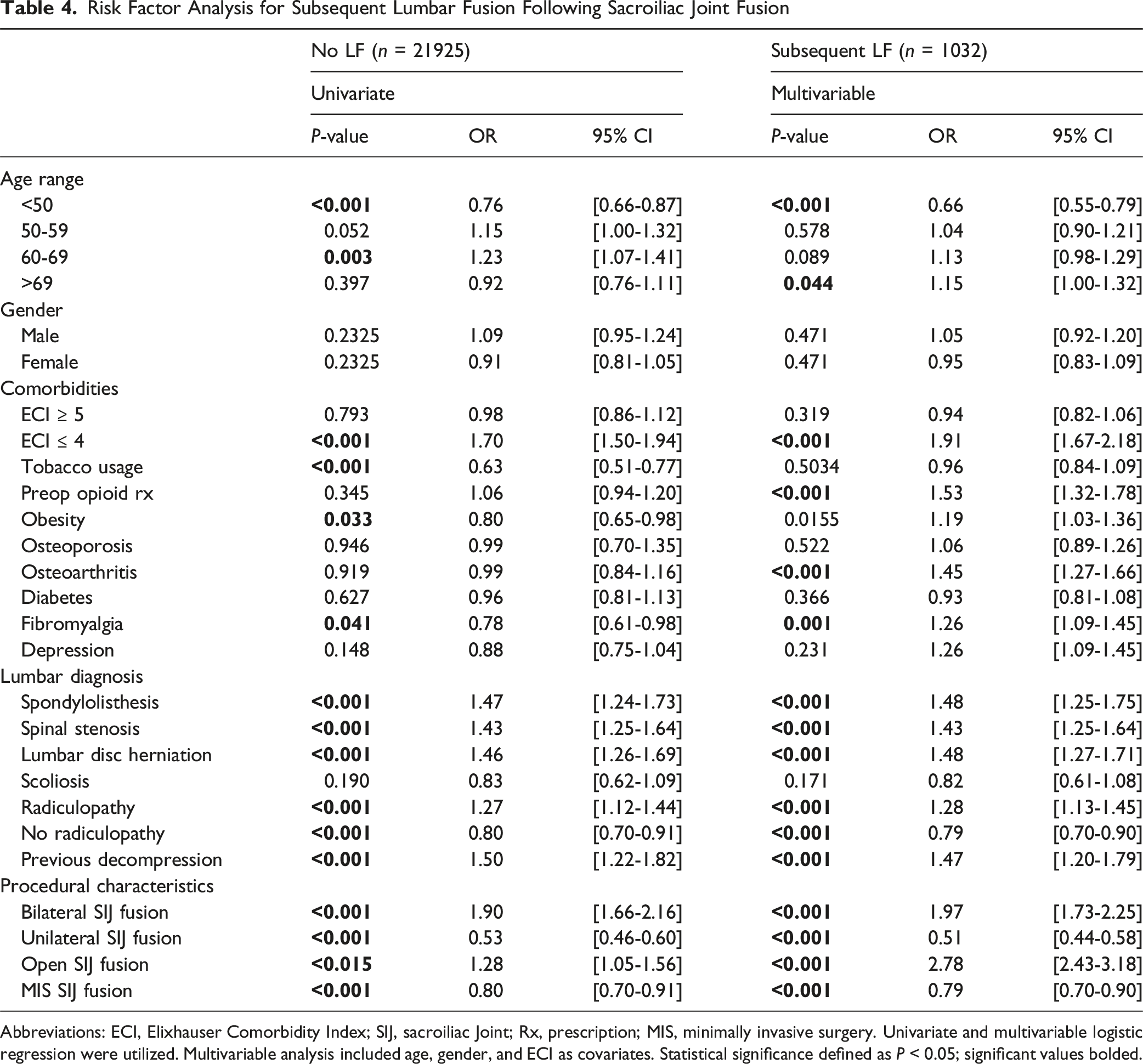
Abbreviations: ECI, Elixhauser Comorbidity Index; SIJ, sacroiliac Joint; Rx, prescription; MIS, minimally invasive surgery. Univariate and multivariable logistic regression were utilized. Multivariable analysis included age, gender, and ECI as covariates. Statistical significance defined as P < 0.05; significant values bolded.
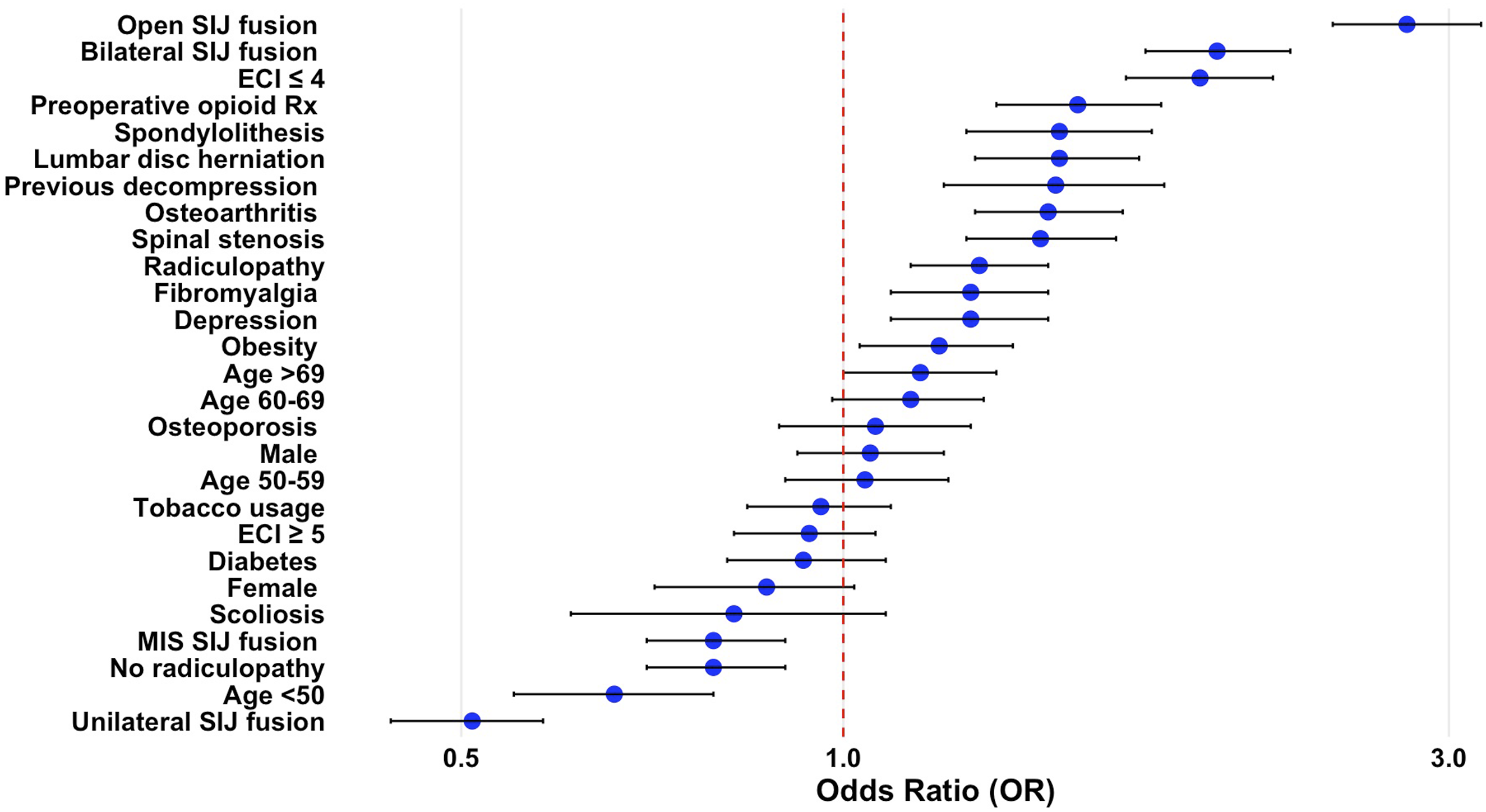
Predictors of Lumbar Fusion After SI Joint Fusion: Multivariable Odds Ratios in Forest Plot
The average time between SI joint fusion and subsequent lumbar fusion was 671 ± 635 days. No significant difference was observed in time to lumbar fusion when comparing patients who underwent unilateral vs bilateral SI joint fusion (675 ± 629 days vs 665 ± 646 days, P = 0.812). Among patients who required lumbar fusion, the most common diagnostic codes on the day of surgery included radiculopathy in 507 patients (49.1%), spinal stenosis in 485 (47.0%), spondylolisthesis in 349 (33.8%), lumbar disc herniation in 160 (15.5%), scoliosis in 68 (6.6%), and myelopathy in 24 (2.3%).
Discussion
The relationship between SI joint fusion and subsequent lumbar degeneration remains poorly understood. This study demonstrated that, among patients with lumbar degenerative disease, those who underwent SI joint fusion had significantly higher odds of requiring a subsequent lumbar fusion (OR: 2.97) compared to matched controls with LDD but without history of SI joint fusion. However, the absolute incidence was modest, with only 4.5% undergoing lumbar fusion during the study period. On average, the interval between SI joint fusion and subsequent lumbar fusion was 671 ± 635 days. Risk factors for subsequent lumbar fusion included open SI joint fusion (aOR: 2.78), bilateral SI joint fusion (aOR: 1.97), ECI ≤ 4 (aOR: 1.91), preoperative opioid prescription (aOR: 1.53), osteoarthritis (aOR: 1.45), and fibromyalgia (aOR: 1.26). Baseline lumbar diagnoses, including spondylolisthesis (aOR: 1.48), spinal stenosis (aOR: 1.43), and radiculopathy (aOR: 1.28), were also associated with increased odds of subsequent fusion. These findings are important to guide preoperative risk assessment and patient counseling while underscoring the need for further research into long-term lumbar changes and clinical outcomes following SI joint fusion.
To the best of our knowledge, this is the first study to demonstrate an increased risk of subsequent lumbar fusion following SI joint fusion. Prior long-term studies on SI joint fusion have primarily focused on complications localized to the SI joint itself, with limited investigation into its effects on lumbar disease progression. 5 Existing biomechanical research on the impact of SI joint fusion on the lumbar spine has largely relied on finite element models, which offer valuable insights but have notable limitations.8,9 For instance, Lindsay et al demonstrated that SI joint fusion increases the range of motion (ROM) at the L5-S1 segment by 1.1%-4.6% during unidirectional bending, changes that are modest compared to the substantial ROM increases of 20%-127% observed in adjacent segments following lumbar fusion.8,10,11 These findings have often been interpreted as evidence that SI joint fusion poses minimal risk for adjacent segment disease in the lumbar spine. 8 However, finite element models may underestimate the risk of adjacent segment disease by failing to account for stress redistribution during dynamic and compressive movements, abnormal anatomy, variation in surgical technique, as well as biological responses over time.
The SI joint has limited natural motion, with maximum rotation and translation estimated at 2-4°, mirroring the magnitude of lumbar ROM change seen in Lindsay et al’s study.12-14 Even with the slight mobility of the joint, SIJ ligaments absorb significant load during compression and dynamic movements like walking. 15 Toyohara et al argue that ossification of these ligaments after SI joint fusion may expose adjacent joints to unphysiological stress environments over time, potentially accelerating degeneration in nearby structures.15,16 This phenomenon has been demonstrated in the hip joint following SI joint fusion, where studies have reported a 5%-10% increase in contact stress and contact area, along with a 64% increase in stress when SI joint fusion is combined with L4-S1 lumbar fusion.17,18
In our study, bilateral SI joint fusion was associated with an increased risk of subsequent lumbar fusion (aOR: 1.97), supporting the hypothesis that fusing both SI joints may redistribute greater stress to adjacent structures compared to unilateral fusions, thereby accelerating lumbar degeneration. However, it is also possible that patients undergoing bilateral fusions had more severe baseline pathology or systemic conditions like osteoarthritis (aOR: 1.45) that predispose them to both sacroiliac and spinal degeneration.
Open SI joint fusion was associated with an even higher risk of subsequent lumbar fusion (aOR: 2.78), whereas MIS techniques were associated with decreased odds (aOR: 0.79). This finding aligns with prior research showing that surgical damage to adjacent soft tissues structures such as paraspinal musculature and ligaments increases the risk of adjacent segment disease by altering spinal biomechanics. 19 MIS techniques typically employ a lateral transiliac approach through the lateral buttock region, minimizing disruption to nearby soft tissues and the L5-S1 facet joints. 20 In contrast, open techniques often involve a posterior approach requiring retraction and instrumentation near the L5-S1 segment, increasing the likelihood of injury to soft tissue or facet joints. 20 Additionally, open procedures frequently involve resection of portions of the posterior iliac spine and removal of articular cartilage from the SI joint, further destabilizing adjacent soft tissue structures and potentially accelerating lumbar degeneration. 20
Other identified risk factors for subsequent lumbar fusion included a lower comorbidity index (ECI ≤ 4; aOR: 1.91), preoperative opioid prescription within 6 months of surgery (aOR: 1.53), and fibromyalgia (aOR: 1.26). Patients with lower comorbidity indices are often better surgical candidates, making them more likely to undergo future procedures such as lumbar fusions if symptoms persist or worsen over time. Similarly, patients using opioids preoperatively or previously diagnosed with fibromyalgia may have more severe underlying LDD or multifactorial pain syndromes not solely attributable to their SI joint pathology. In addition, several baseline lumbar diagnoses, including spondylolisthesis (aOR: 1.48), lumbar disc herniation (aOR: 1.48), spinal stenosis (aOR: 1.43), and radiculopathy (aOR: 1.28), were associated with an increased risk of subsequent lumbar fusion following SI joint fusion. Their association with later fusion may simply reflect a greater initial disease severity. However, it may also indicate a predisposition to accelerated degeneration after SI joint fusion. This is particularly plausible in the case of spondylolisthesis, which reflects segmental instability and may be exacerbated by the loss of stress dampening at the SI joint.
Kaplan-Meier survival analysis revealed an interesting temporal pattern: during the first 1000 days after LDD diagnosis, patients undergoing SI joint fusion had lower odds of requiring lumbar fusion compared to controls; however, beyond approximately 1250 days post-diagnosis, their odds increased significantly relative to controls. One possible explanation is that patients initially delay lumbar surgery while assessing pain relief from their SI joint procedure; if pain persists or worsens over time, they may eventually pursue additional surgery for unresolved symptoms. Alternatively, this pattern could reflect a biomechanical phenomenon wherein altered stress propagation following SI joint fusion accelerates lumbar degeneration over time.
As SI joint fusion is increasingly utilized to treat SI joint pain, establishing a long-term complication profile is imperative. Extensive research has investigated how different approaches, implant types, implant number and location affect the stress and movement across the SI Joint, but most of these studies do not investigate the additional effects on the lumbar spine. 1
This study has several important limitations. First, the use of an administrative claims database precludes access to radiographic imaging and functional status measures. We were unable to assess key clinical variables such as the severity of lumbar degeneration, presence of deformity or instability, Modic changes, or disability scores like the Oswestry Disability Index. Importantly, the absence of imaging and functional data limits our ability to fully control for baseline differences between the SI joint fusion and control cohorts. Although propensity matching was used for age, sex, and comorbidity burden, unmeasured differences in underlying spinal pathology or functional impairment may have influenced both treatment decisions and outcomes. Additionally, we could not confirm how sacroiliac joint dysfunction was diagnosed, such as through diagnostic blocks or provocative maneuvers, which limits the accuracy of patient selection and may introduce heterogeneity. Finally, while the relative risk of lumbar fusion was significantly higher following SI joint fusion, the absolute incidence remained modest (4.5%), which should temper interpretation.
Despite these limitations, a key strength of this study is the use of a large nationwide insurance claims database, which enabled the inclusion of over 22 000 patients undergoing SI joint fusion. Given that SI joint fusions remain relatively uncommon and subsequent lumbar fusion is a low-frequency event, this large sample size was critical to achieving sufficient statistical power to detect clinically meaningful differences in complication rates.
Conclusion
In patients with lumbar degenerative disease, those who undergo SI joint fusion have significantly higher odds of requiring future lumbar fusion, with risk factors including open surgical techniques, bilateral fusion, and preexisting conditions such as osteoarthritis and fibromyalgia. These findings underscore the importance of thorough preoperative risk assessment and patient counseling, particularly regarding the potential long-term effects of SI joint fusion on the lumbar spine. While SI joint fusion is associated with increased odds of subsequent lumbar fusion, the absolute risk remains relatively low, emphasizing the need for individualized, risk-based decision-making. As the utilization of SI joint fusion continues to rise, future research should investigate long-term clinical outcomes related to lumbar degeneration after SI joint fusion and evaluate how different surgical techniques influence adjacent segment disease and stress redistribution across spinal segments. Dynamic biomechanical models simulating real-world activities like walking or running should also be incorporated into future studies, and stress redistribution, not just changes in adjacent motion, should be analyzed.
Key Points
• Patients with lumbar degenerative disease who underwent SI joint fusion had nearly three times the odds of requiring subsequent lumbar fusion compared to matched controls without SI joint fusion, although the absolute risk remained modest at 4.5%. • Open and bilateral SI joint fusions were associated with significantly higher risk of future lumbar fusion, whereas minimally invasive and unilateral approaches were associated with decreased risk. • Baseline lumbar pathologies such as spondylolisthesis, spinal stenosis, and radiculopathy were associated with increased risk of subsequent lumbar fusion. These diagnoses likely reflect greater baseline disease severity but may also indicate a predisposition to accelerated lumbar degeneration following SI joint fusion. • Additional risk factors such as preoperative opioid use, fibromyalgia, osteoarthritis, and lower comorbidity burden may help identify patients at increased risk for future lumbar surgery. • These findings underscore the importance of comprehensive preoperative evaluation and long-term follow-up in patients undergoing SI joint fusion with coexisting lumbar pathology.
Supplemental Material
Supplemental Material - Increased Risk of Lumbar Fusion Following Sacroiliac Joint Fusion in Patients With Lumbar Degenerative Disease: A Nationwide Cohort Analysis
Supplemental Material for Increased Risk of Lumbar Fusion Following Sacroiliac Joint Fusion in Patients With Lumbar Degenerative Disease: A Nationwide Cohort Analysis by William J. Karakash, Ali Issani, Henry Avetisian, Dil Patel, Raymond J. Hah, Ram K. Alluri, John C. Liu, and Jeffrey C. Wang in Global Spine Journal.
Footnotes
Informed Consent
Informed consent was waived due to the retrospective nature of the study and institutional review board (IRB) approval was not required as the database is de-identified.
Author contributions
William Karakash, Ali Issani, Henry Avetisian, and Dil Patel have nothing to disclose. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccential Robotics for lectures and presentations. John C. Liu has received supported from Global Spine Congress and North American Spine Society to attend meetings. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not publicly available but can be available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.