
Abstract
Study Design
Multicenter prospective cohort study
Objective
To analyse therapeutical strategies applied to osteoporotic thoracolumbar OF 4 injuries, to assess related complications and clinical outcome.
Methods
A multicenter prospective cohort study (EOFTT) including 518 consecutive patients who were treated for an Osteoporotic vertebral compression fracture (OVCF). For the present study, only patients with OF 4 fractures were analysed. Outcome parameters were complications, Visual Analogue Scale, Oswestry Disability Questionnaire, Timed Up & Go test, EQ-5D 5L, and Barthel Index after a minimum follow-up of 6 weeks.
Results
A total of 152 (29%) patients presented with OF 4 fractures with a mean age of 76 years (range 41-97). The most common treatment was short-segment posterior stabilization (51%; hybrid stabilization in 36%). Mean follow up was 208 days (±131 days), mean ODI was 30 ± 21. Dorsoventral stabilized patients were younger compared to the other groups (P < .001) and had significant better TuG compared to hybrid stabilization (P = .049). The other clinical outcomes did not differ in the therapy strategies (VAS pain: P = 1.000, ODI: P > .602, Barthel: P > .252, EQ-5D 5L index value: P > .610, VAS-EQ-5D 5L: P = 1.000). The inpatient complication rate was 8% after conservative and 16% after surgical treatment. During follow-up period 14% of conservatively treated patients and 3% of surgical treated patients experienced neurological deficits.
Conclusions
Conservative therapy of OF 4 injuries seems to be viable option in patients with only moderate symptoms. Hybrid stabilization was the dominant treatment strategy leading to promising clinical short-term results. Stand-alone cement augmentation seems to be a valid alternative in selected cases.
Introduction
Osteoporotic vertebral compression fractures (OVCF) of the thoracolumbar spine are frequent with an increasing prevalence.
Recently, a new classification system together with a score for therapeutic decision making have been developed by the working group “Osteoporotic Fractures” of the Spine Section of the German Society of Orthopaedics and Trauma.1,2 With regard to treatment, one of the most controversially discussed fracture type are OF 4 injuries with deformation of both endplates and with or without posterior wall involvement.3-5 Generally, the evidence for operative and non-operative treatment of OF 4 type fractures is very limited.6,7,8 The huge majority of studies did not specifically include OF 4 type fractures.5,6,8 Palmowski et al 4 looked at the reduction potential of kyphoplasty and reported of reliable restoration of the vertebral bodies even in type OF 4 fractures. A recent cochrane database systematic review looked at the effect of exercise as component of non-operative treatment for improving outcomes after osteoporotic vertebral fracture. 8 None of the included trials classified the fractures in detail. Thus, no associations can be made between fracture morphology and the outcome. However, from a biomechancal point, it can be expected that the fracture morphology has impact on the fracture stability which has an impact on the outcome depending on the treatment that has been applied.
To investigate the treatment of OVCF, a prospective German multicentric study (Evaluation of the Osteoporotic Fracture classification, Treatment score and Therapy recommendations - EOFTT) was concluded.
One aim of this study was to analyse the treatment choices, the incidence of new fractures, outcomes of patients suffering from OF 4 injuries and to assess related complications.
Materials and Methods
A multicenter prospective cohort study (EOFTT) was conducted at 17 spine centers in Germany and Switzerland. The study was approved by the local or regional institutional ethics committees of each participating center. Inclusion criteria were OVCF, either spontaneous or because of low energy trauma, in patients older than 18 years and proven osteoporosis following national and international recommendations. 9 Patients received conventional AP and lateral radiographs, a CT scan and an MRI scan. Fractures were classified according to the OF classification. 2
The OF score was applied including clinical information (pain, mobilization, neurology, health status) in addition to radiographic parameters. If the OF score is above 6 points surgical therapy is recommended. However, final treatment decision was at physician’s discretion. 1
For clinical evaluation the type of treatment - conservative or surgical in general and detailed surgical intervention - and the following variables were obtained at time of treatment decision (TD) and at follow-up (FU): Pain with visual analogue scale (VAS-P, 0-10), bone quality using either bone mineral density (DXA; t-score) or CT (Hounsfield units; HU), 10 Oswestry Disability Index (ODI), Barthel index, Timed up and go test (TuG), EQ5D-5L index value and visual analogue scale of subjective health status from EQ5D (VAS-EQ5D). The TuG measures mobility impairment by measuring the patient’s time needed for stand up on a chair with armrests, walk a distance of 3 meters, turn around and sitting down again. The EQ5D-5L index value was calculated using the data set for German index values. The higher the value, the better the health status up to a maximum of 1. The reported subjective health status in the EQ5D (VAS-EQ5D) was chosen with a VAS with the limits of 0 (zero) and 100, where 100 reflects the best and 0 the worst health status. The Barthel index is an assessment tool to define the autonomy of patients on tasks for daily living. Zero (0) represents complete independency whereas 100 reflects full autonomy.
For the present analysis, only patients with a fracture type OF 4 and a planned follow-up of at least 6 weeks were included. Generally, the last follow-up that was available was considered.
In addition to the clinical scores a further secondary outcome parameter was the occurrence of complications. Complications were divided in those related to the surgical intervention (implant failure, adjacent level fracture, neurological deficit and surgical site infections) and general complications (thromboembolic event, urinary tract infection, pneumonia, delirium). Surgical site infections were defined as any wound-related complication that required surgical revision.
Statistical Methods
All data was finally recorded in an Excel database (Microsoft Corp., Washington, DC, USA) and exported to SPSS 27.0 (SPSS Inc., Chicago, IL, USA) for statistical analysis. Data was summarized as mean with standard deviation (SD).
Differences in primary outcome parameters (depending variables) between conservative vs surgically treated in general and in addition differentiated between all therapy strategies (fixed factor) were analysed with separate multivariate, general linear models (GLM), respectively. Post hoc Bonferroni Test was performed for pairwise comparisons. The level of significance was defined as P < .05.
Results
Baseline Characteristics.
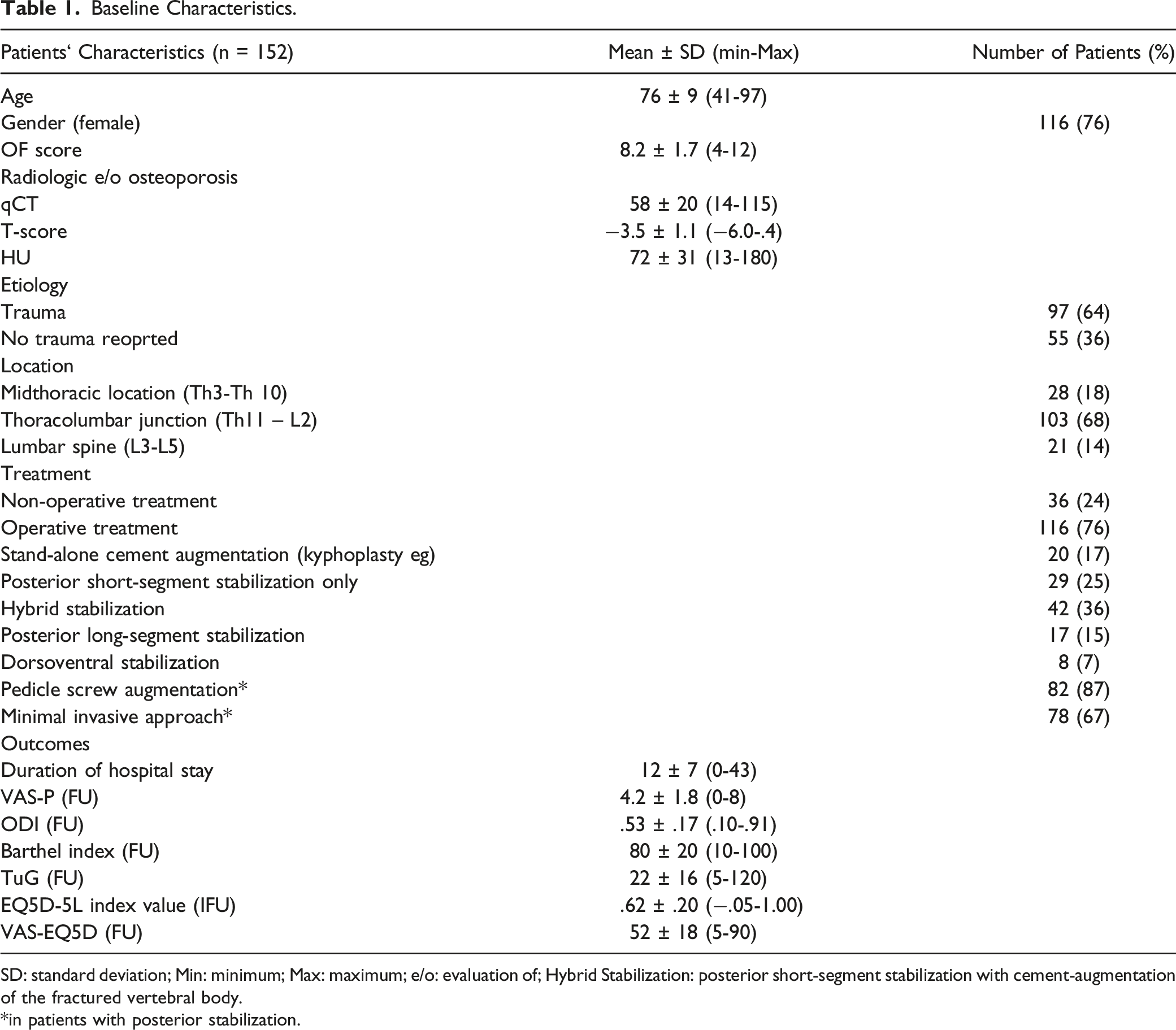
SD: standard deviation; Min: minimum; Max: maximum; e/o: evaluation of; Hybrid Stabilization: posterior short-segment stabilization with cement-augmentation of the fractured vertebral body.
*in patients with posterior stabilization.
The majority of fractures occurred at the thoracolumbar junction between T11 and L2 (68%).
34% of the patients suffered from insufficiency fractures and could not recall any trauma history.
In total 36 patients were treated conservatively (24%) and 116 of the patients (76%) received surgical therapy. The duration between the patients’ admission and the treatment decision was 4 ± 4 days (range: 0-26, median 2 days) and did not differ depending on surgical or conservative therapy choice (P = .376). At the day of treatment decision the mean OF-score was 8.2 ± 1.7 (range 4-12) and differed between conservative (7.6 ± 1.8) and surgical treated patients (8.4 ± 1.7, P = .029). Thereby a total of 15 patients were treated conservatively despite an OF score of more than 6 and 7 patients were treated surgically despite an OF score of less than 6. Additionally, the VAS-P differed significantly between the treatment choices (conservative: 4.3 ± 2.0, surgical: 6.6 ± 2.2, P = .012). No differences could be found for age (P = .624), ODI (P = .587), bone density (qCT P = .537, DXA P = .323, HU P = .715), Barthel Index (P = .215), TuG (P = .383), EQ5D-5L index value (P = .685) and VAS-EQ5D (P = .736) at the day of treatment decision. The most common surgical therapy strategy was short-segment stabilization with cement augmentation of the fractured vertebral body (Hybrid stabilization, Figure 1). Conservative treated patients showed shorter hospital stay (mean difference: 5d, P = .002). Legends: 74 years old woman with acute severe back pain after fall on buttock in garden. Xray and CT- scan demonstrate OF 4 type fracture of T12 and osteoporotic bone quality with HU 67 (a,b,c). OF score was 11 points and percutaneous stabilization with internal hybrid fixator was performed. X-ray in standing position after 3 days (d,e) and a CT (f) during the hospital stay showed correct implant positioning and an anatomic fracture reduction. Similarly, X-rays in standing position after 3 months (g,h) showed an unchanged situation. Pain without medication was moderate (3).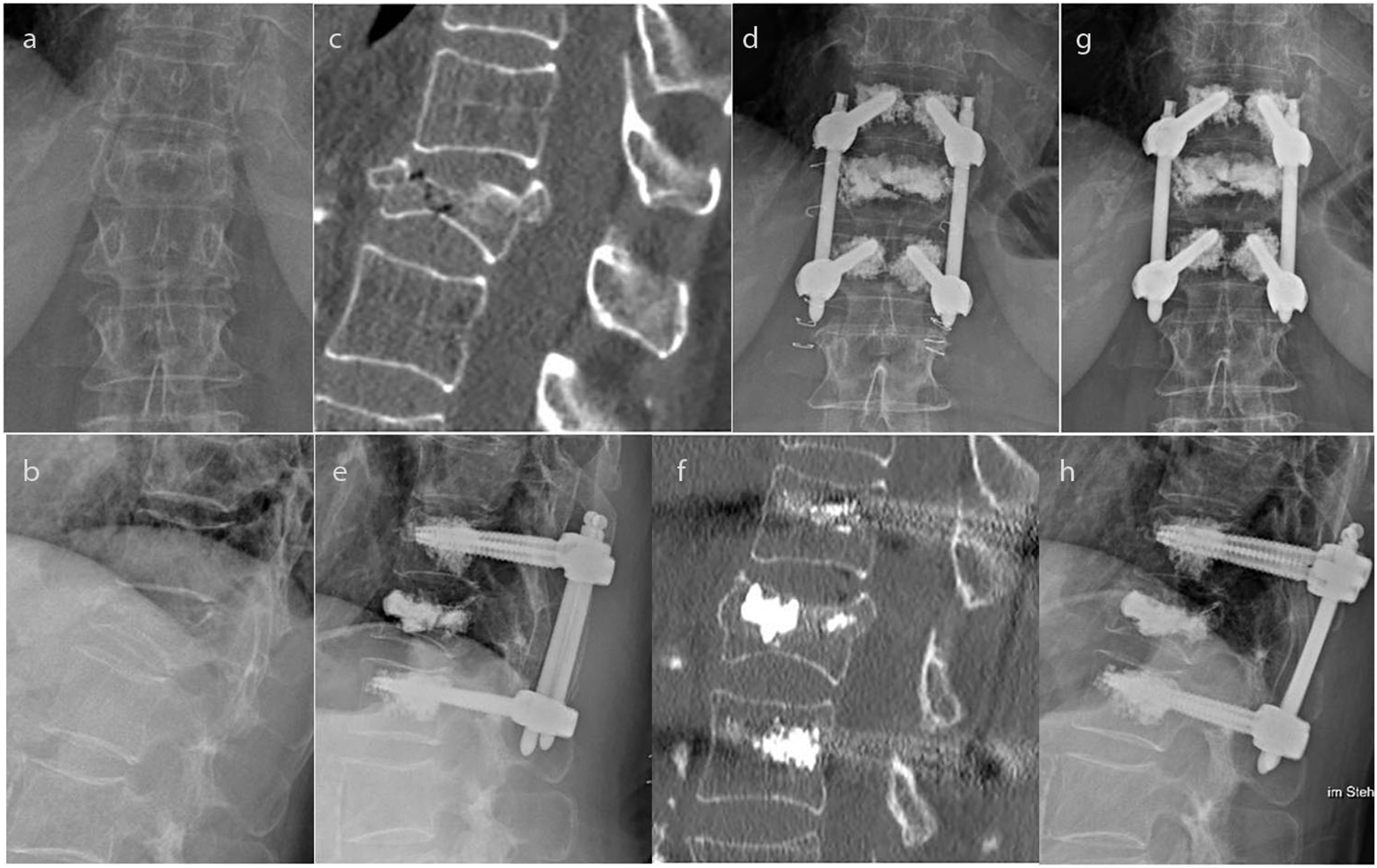
At the follow up (208 ± 131 days, range 42-563 days), a complete data set of clinical outcome parameters was available for 101 patients (66%), consisting 21 patients treated conservatively with a mean follow up of (220 ± 124 days, range 42-453 days) and 80 patients treated operatively with a mean follow up of (165 ± 151 days, range 42-563 days, P = .137).
Outcomes.
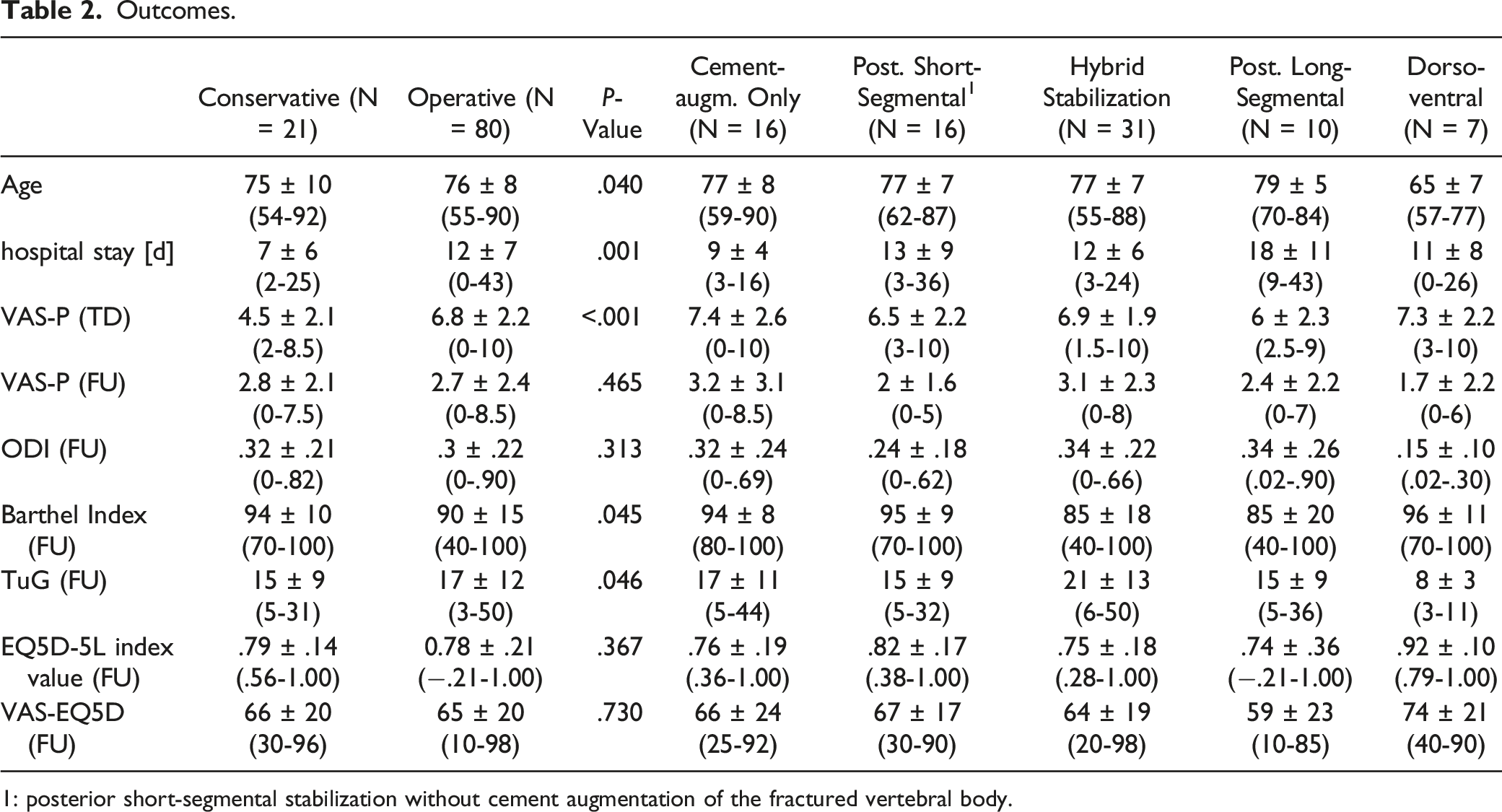
1: posterior short-segmental stabilization without cement augmentation of the fractured vertebral body.
Complications.
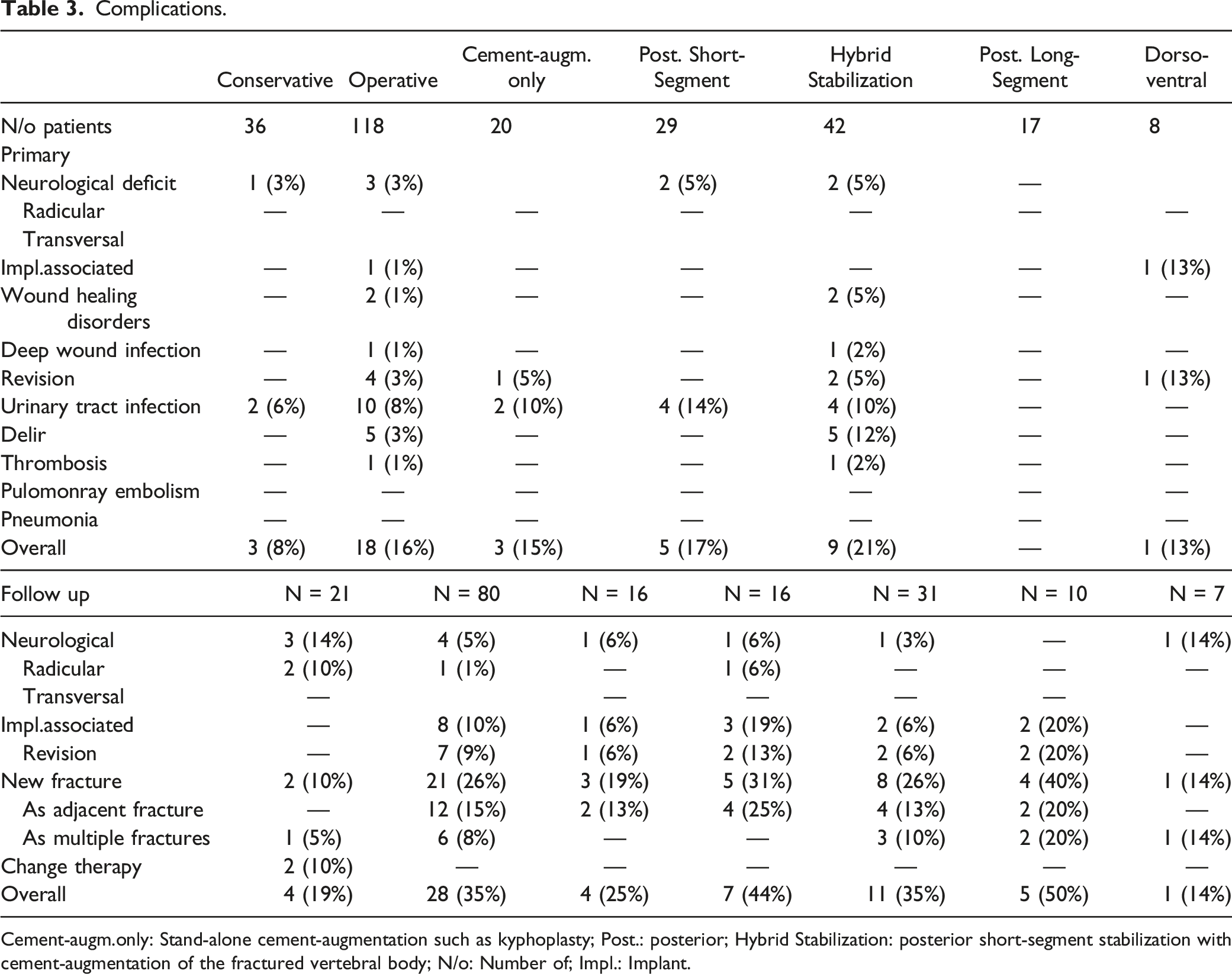
Cement-augm.only: Stand-alone cement-augmentation such as kyphoplasty; Post.: posterior; Hybrid Stabilization: posterior short-segment stabilization with cement-augmentation of the fractured vertebral body; N/o: Number of; Impl.: Implant.
Discussion
Osteoporotic vertebral compression fracture show different morphological patterns. The recently proposed OF classification includes 5 subgroups. 2 OF 4 are defined as injuries with deformation of both endplates with or without posterior wall involvement. Thus, OF 4 injuries consist of complete burst fractures, pincer-type fractures, and fish-bone deformations. Due to the variety of fracture morphologies, it is no surprising finding that the therapeutic strategies varied considerably.
This study aimed to analyse the treatment concepts and outcomes of patients suffering from OF 4 injuries.
Scheyerer at al reported, that high degree of posterior wall affection is a risk factor for failure of conservative treatment. 11 Blattert et al 1 recommended, surgical treatment with long-segment instrumentation or combined posterior short-segment fixation and anterior reconstruction for OF 4 injuries. In contrast, almost one quarter of our patients (24%) were conservatively treated. Generally, the majority of patients treated conservatively, had minor symptoms, lower complication rates favoring the conservative treatment. In contrast the mean VAS pain level at the time of treatment decision was more than 2 points higher in the surgically treated group. However, despite the favorable initial course of the patients treated conservatively this was associated with a high rate of neurological deficits at follow-up of 14%.
Just over 50% of the patients were treated with posterior short-segment stabilization most commonly a hybrid stabilization (augmented pedicle screws and cement augmentation of the fractured index- level vertebra).
Stand-alone cement augmentation was performed in 17% of the patients. Finally, no significant differences in the outcome scores between the groups could be seen.
Taking the recent literature into account stand-alone cement augmentation seems to be justified. Palmowski et al4,12 reported of favorable clinical and radiological results with reduction potential and low reduction loss in the short run. Similarly, Gu et al 3 reported similar clinical results after both stand-alone kyphoplasty and hybrid stabilization. However, the authors found significant difference in the regional alignment with significant higher loss of reduction in the stand-alone cement augmentation group in the longer run, after 27 months. 13 Thus, the loss of reduction seemed to be associated with higher numbers of adjacent fractures. 13 However, more studies with longer follow-up periods are needed to analyse the status of stand-alone cement augmentation in OF 4 fractures correctly.
There were no differences in the clinical outcome of short-segment stabilization without cement augmentation compared to the hybrid stabilization. It can be hypothesized that the additional cement augmentation of the fractured vertebral body was performed mainly in severe fractures without sufficient reduction after patient positioning. Thus, a selection bias can be assumed.
Long-segment stabilization is recommended in the midthoracic spine. 14 Additionally, the authors see the indication in patients with very unstable fractures, such as high local deformity and relevant differences in the bisegmental kyphosis between standing radiographs and CT/MRI in supine position. The dorsoventral strategy was performed in a minority of 7% of the cases and only in patients < 70 years of age. Thereby patients treated dorsoventrally had significant better TUG test compared to the hybrid group. However, the differences in the TUG can be explained by the significantly younger patient age in that group. In contrast, no difference between midterm outcomes between hybrid stabilization and dorsoventral treatment was seen in the patient group between 60 and 70 years of age. 15
In general, the clinical outcomes were in accordance with the literature.16,17 Considering the clinical outcome, conservative treatment, seem to be a suitable alternative therapy concept with similar results in patients with type 4 fractures. However, in highly unstable fractures conservative treatment may lead to neurological deficits during the further course. This was seen in 14% of our patients despite the high rate of compliance with the OF score.
Limitations
The study has several limitations. Based on the multi-centric approach of the study, the treatment strategy chosen was differently among participating centers. Additionally, the follow-up period of a minimum of 6 weeks is short. Bony consolidation may not be finally completed after 6 weeks. Thus, we did not present loss of lordosis or kyphotic malalignment as a complication to avoid any bias with respect of reduction loss and correlation to a specific treatment strategy. Generally, the mean follow-up was considerably longer consisted of more than 6 months. Moreover, further adjacent fractures might lead to inferior results in the further course. Besides, no radiologic outcome parameters were included. Regional kyphotic malalignment that might cause pain in the future could not be analyzed.
A strength of this study is its prospective, multicenter design with more than 500 patients with OVCF - including 152 patients with OF 4 injuries. However, the sample size of conservatively treated patients with type OF 4 fractures was rather small. Thus, a comparison of surgically treated patients with conservatively treated patients was limited.
Conclusions
Conservative therapy seems to be viable option in cases with only mild to moderate symptoms. Posterior percutaneous short-segment stabilization with or without augmentation of the pedicle screws and - if possible - the fractured vertebral body was the most commonly applied treatment strategy. Stand-alone cement augmentation seems to be a valid alternative in selected cases. Generally, surgical treatment leads to lower rates of neurologic deficits, but higher percentages of complications overall. However, further studies with longer follow-up are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ulrich J. Spiegl: Advisory Board: European Journal of Trauma and Emergency Surgery
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).
Authors’ Contributions
Working group Osteoporotic Fractures of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU): Conception and Study design. Ulrich J. Spiegl: Vice-chair of AG-OF, patients inclusions, data collection manuscript writing, literature research, data management. Philipp Schenk: statistical analysis, editiong manuscript. Klaus John Schnake: Chair of AG-OF, patients inclusions, data collection manuscript writing and editing, literature research. Berhnard W. Ullrich: Vice-chair of AG-OF, patients inclusions, data collection revision revision, Sebastian Katscher: Patients inclusions, data collection, manuscript writing and editing, literature research. Further coauthors: data collection, responsible for patient management of the respective spine centers
Ethics Approval and Consent to Participate
This study was approved by the research ethics committee of the medical Association of Saxony-Anhalt Germany (14. June 2017, file number 31/17) and was performed in accordance with the principles laid down in the current revision of the Declaration of Helsinki. The ethics committee determined that informed consent from each patient was not necessary due to the retrospective, anonymized nature of the research.
Consent for Publication
The authors give the consent for publication of all contents of this manuscript.
Availability of Data and Material
The datasets used and analyzed with this study are available on reasonable request from the corresponding author.