
Abstract
Study Design
Subgroup analysis of a multicenter prospective cohort study
Objective
To analyse surgical strategies applied to osteoporotic thoracolumbar osteoporotic fracture (OF) 5 injuries with anterior or posterior tension band failure and to assess related complications and clinical outcome.
Methods
A multicenter prospective cohort study (EOFTT) was conducted at 17 spine centers including 518 consecutive patients who were treated for an osteoporotic vertebral fracture (OVF). For the present study, only patients with OF 5 fractures were analysed. Outcome parameters were complications, Visual Analogue Scale (VAS), Oswestry Disability Questionnaire (ODI), Timed Up & Go test (TUG), EQ-5D 5L, and Barthel Index.
Results
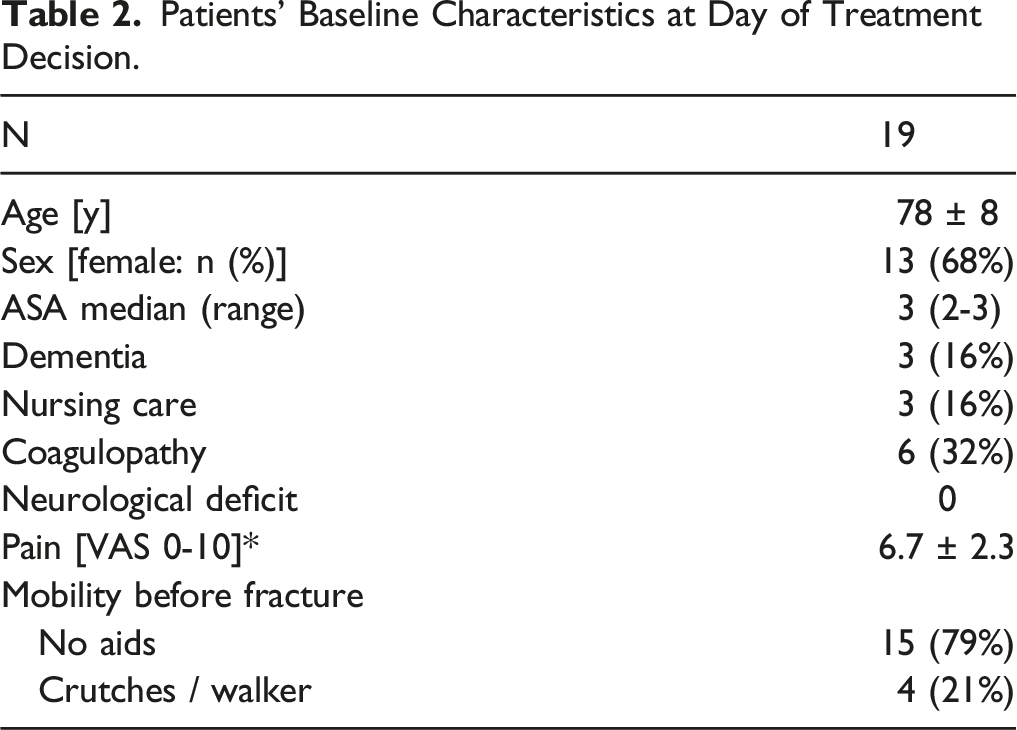
In total, 19 patients (78 ± 7 years, 13 female) were analysed. Operative treatment consisted of long-segment posterior instrumentation in 9 cases and short-segment posterior instrumentation in 10 cases. Pedicle screws were augmented in 68 %, augmentation of the fractured vertebra was performed in 42%, and additional anterior reconstruction was done in 21 %. Two patients (11 %) received short-segment posterior instrumentation without either anterior reconstruction or cement-augmentation of the fractured vertebra. No surgical or major complications occurred, but general postoperative complications were observed in 45%. At a follow-up of mean 20 ± 10 weeks (range, 12 to 48 weeks), patients showed significant improvements in all functional outcome parameters.
Conclusions
In this analysis of patients with type OF 5 fractures, surgical stabilization was the treatment of choice and lead to significant short-term improvement in terms of functional outcome and quality of life despite a high general complication rate.
Introduction
For the majority of osteoporotic vertebral fractures (OVF) non-operative treatment is possible, especially in case of no or little deformity. In fractures with a higher degree of deformity or intrinsic instability, however, non-operative treatment is prone to failure. 1 Recently, a new classification system for OVF, the osteoporotic fracture (OF) classification, has been developed and validated in order to better predict the natural course of these fractures. 2 Based on this classification, operative treatment with long-segment instrumentation or combined posterior short segment fixation and anterior reconstruction has been suggested for OF 5 injuries. 3 Osteoporotic fracture 5 injuries are defined as injuries with anterior or posterior tension band failure implying distraction or rotation components and, hence, are considered highly unstable. However, the indication for surgery of OVF remains controversial. Complication rates reported for multi-level instrumentation in osteoporotic bone and elderly patients are high.4,5
Focusing only on the risks of operative treatment may lead to a neglect of the chances of surgical therapy. It is the authors’ hypothesis that in selected patients surgical management according to existing recommendations of the German Society of Orthopaedics and Trauma can result in improved patient outcome. 3
Recently, a German multicenter study (Evaluation of the Osteoporotic Fracture classification, Treatment score and Therapy recommendations - EOFTT) was concluded.
In a first step, this evaluation focussed on the prospective cohort of OF 5 injuries. The aim was to analyse the surgical strategies applied to OF 5 injuries to thoracolumbar spine and to assess related complications and clinical outcome.
Materials and Methods
Osteoporotic Fracture (OF) score (Blattert et al 2018).
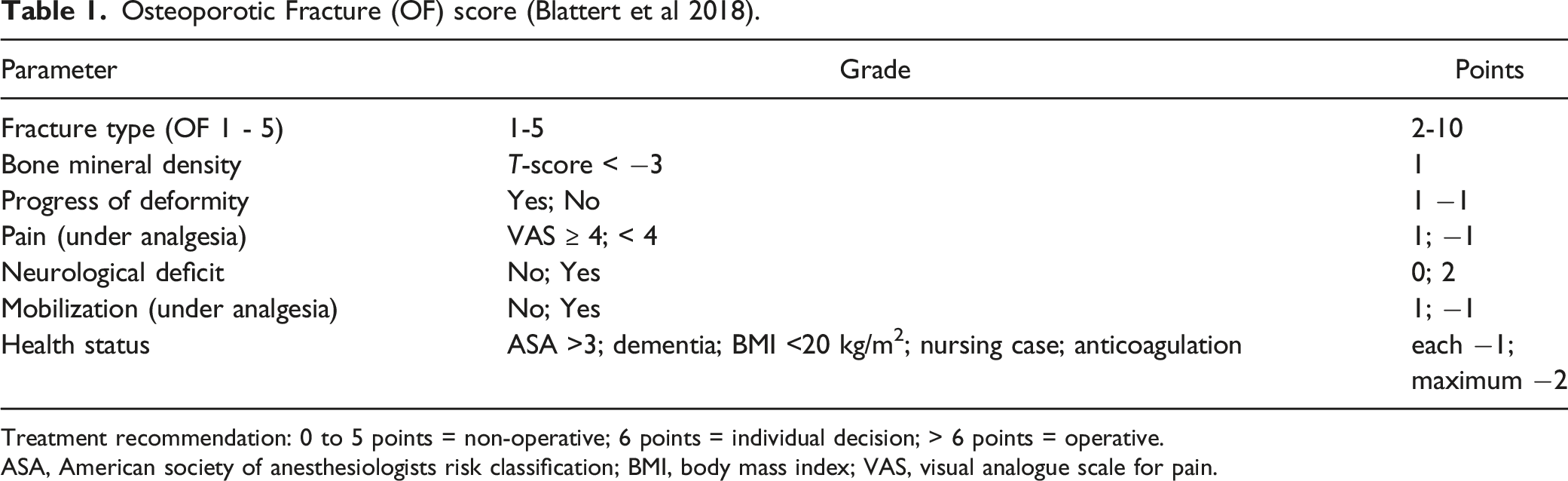
Treatment recommendation: 0 to 5 points = non-operative; 6 points = individual decision; > 6 points = operative.
ASA, American society of anesthesiologists risk classification; BMI, body mass index; VAS, visual analogue scale for pain.
Patients
In the EOFTT study, 518 consecutive patients who were treated operatively or non-operatively in one of the participating centers for one or more osteoporotic thoracolumbar vertebral fracture between Sep 2017 and Jul 2020 were included. Osteoporotic vertebral fracture were defined as any vertebral fracture in the presence of osteoporosis. Osteoporosis was defined to be present if: (a) the patient had a dual energy X-ray absorptiometry (DXA) with a T-score ≤ 2.5, or (b) a qCT with a bone mineral density of less than 80 mg/cm3, or (c) a CT scan of the spine with a bone density of ≤ 110 Hounsfield units,6,7 or (d) an indication for osteoporosis therapy according to the criteria of the guidelines on osteoporosis by the German Osteology Society (Dachverband Osteologie DVO).8,9 Patients with spondylitis or spondylodiscitis, patients with metastatic disease, and patients with concomitant injuries were excluded.
All patients received conventional AP and lateral radiographs, a CT scan and an MRI scan of the whole thoracolumbar spine. Fractures were classified according to the OF classification. 2
Follow-up visits were scheduled at 6 and 12 weeks and at 6 and 12 months and included a thorough history and physical examination, a conventional AP and lateral radiographs of the affected spine segment, and a number of objective and patient-reported outcome measurement tools: Visual Analogue Scale (VAS), the Oswestry Disability Questionnaire (ODI), 10 the Timed Up & Go test (TUG), 11 the EQ-5D 5L, 12 and the Barthel Index. 13
For this subgroup analysis, only patients with a fracture type OF 5 (ie injuries with anterior or posterior tension band failure) and a follow-up of at least 12 weeks were included. The OF score (Table 1) 3 was applied and recorded but treatment was made as decided by the spine surgeon on call. In general, all participating centers feel committed to the recommendations established by the Spine Section of the German Society of Orthopaedics and Trauma 3 but it was up to the surgeons to deviate from them in individual cases. For the analysis, posterior stabilizations with a long-construct (vs. short constructs).were defined as constructs spanning more than 2 segments. Percutaneous posterior instrumentation (vs. open) was defined as any surgery were the pedicle screws and rods were placed through stab incisions. Cement augmentation of pedicle screws was performed either by applying bone cement through fenestrated screws or by injecting cement into the predrilled bone and then placing the screw. Cement augmentation of the fracture level was defined as any technique that injected bone cement into the fractured vertebral body including vertebroplasty or any type of kyphoplasty. Decompression was defined as any surgical intervention that decompressed the osseous spinal canal including laminectomy and hemilaminectomy.
For OF type 5 fractures, the OF score usually recommends operative treatment as long as the patient is not asymptomatic and has a reduced health status (see Table 1). If the treatment decision deviated from the OF score’s recommendation, reasons were documented.
Outcome
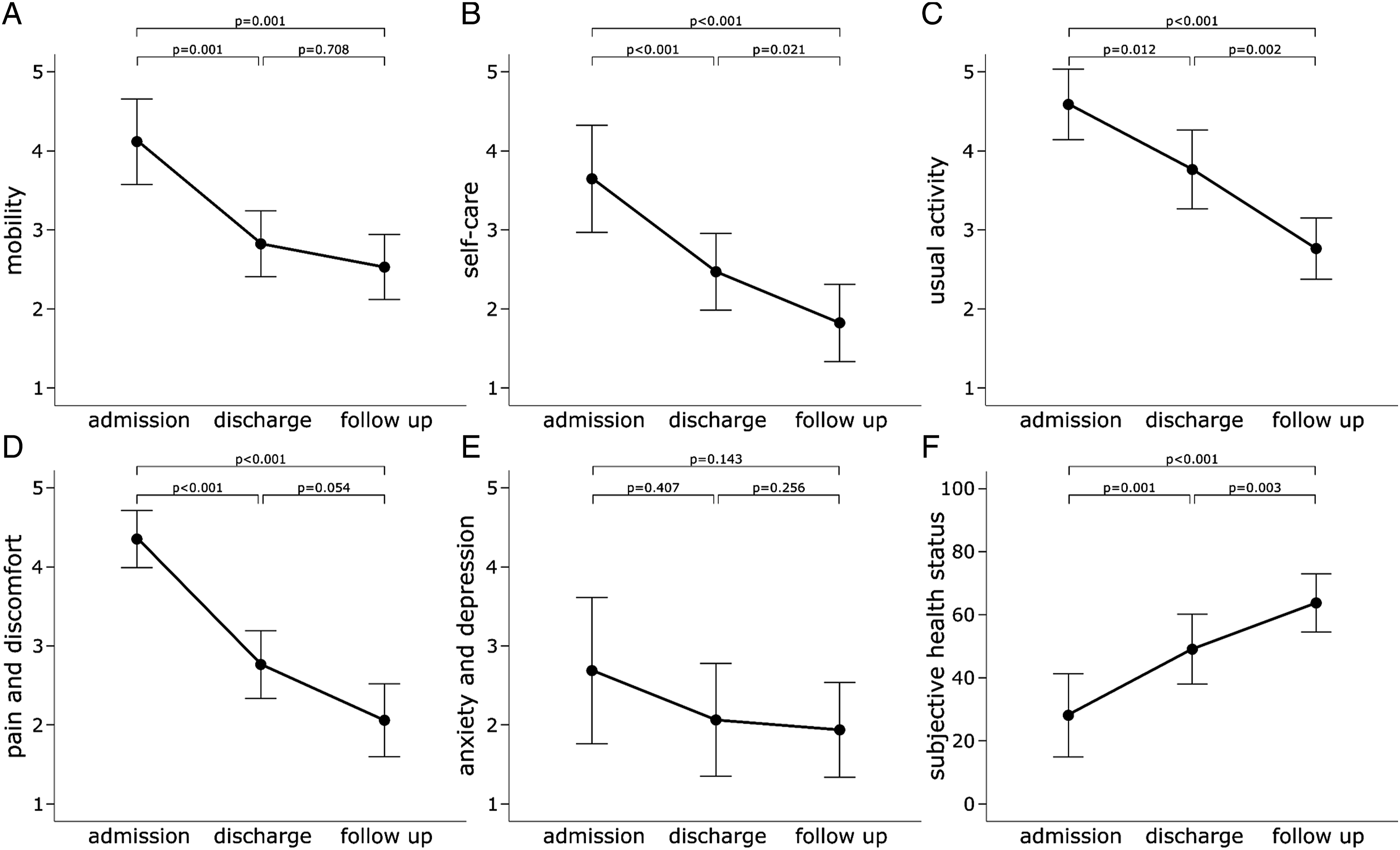
Primary outcome was functional outcome measured by the ODI. Secondary outcome parameters were pain, functional outcome, quality of life, and the availability to perform activities of daily living (ADL) as measured by VAS, TUG, Barthel Index and EQ-5D 5L (mobility, self-care, usual activities, pain/discomfort, anxiety/depression, and subjective health status) at a minimum of 3 months after the treatment decision.
A further secondary outcome parameter was the occurrence of complications. Complications were divided in those related to the surgical intervention (implant failure, adjacent level fracture, neurological deficit, and surgical site infections) and general complications (thromboembolic event, urinary tract infection (UTI), pneumonia, delirium, in-hospital death). Surgical site infections were defined as any wound-related complication that required surgical revision.
Statistical Analysis
All data was finally recorded in an Excel database (Microsoft Corp., Washington, DC, USA) and exported to SPSS 27.0 (SPSS Inc., Chicago, IL, USA) for statistical analysis. Unless otherwise denoted, data was summarized as mean with standard deviation (SD). For visual comparison mean and 95% confidence intervals are used.
Differences between admission, discharge and the follow up in the primary outcome parameters were analysed separately with general linear model for repeated measures (rmGLM). Additional, effect size (ES) is given as partial eta square. The ES interpreted with .01 as small, .06 as medium and .14 as large effects. 14 For post hoc pairwise comparison between time points Bonferroni test was used.
The level of significance was defined as P < .05.
Results
Baseline Data
Patients’ Baseline Characteristics at Day of Treatment Decision.
Detailed Patient Characteristics and Complications.
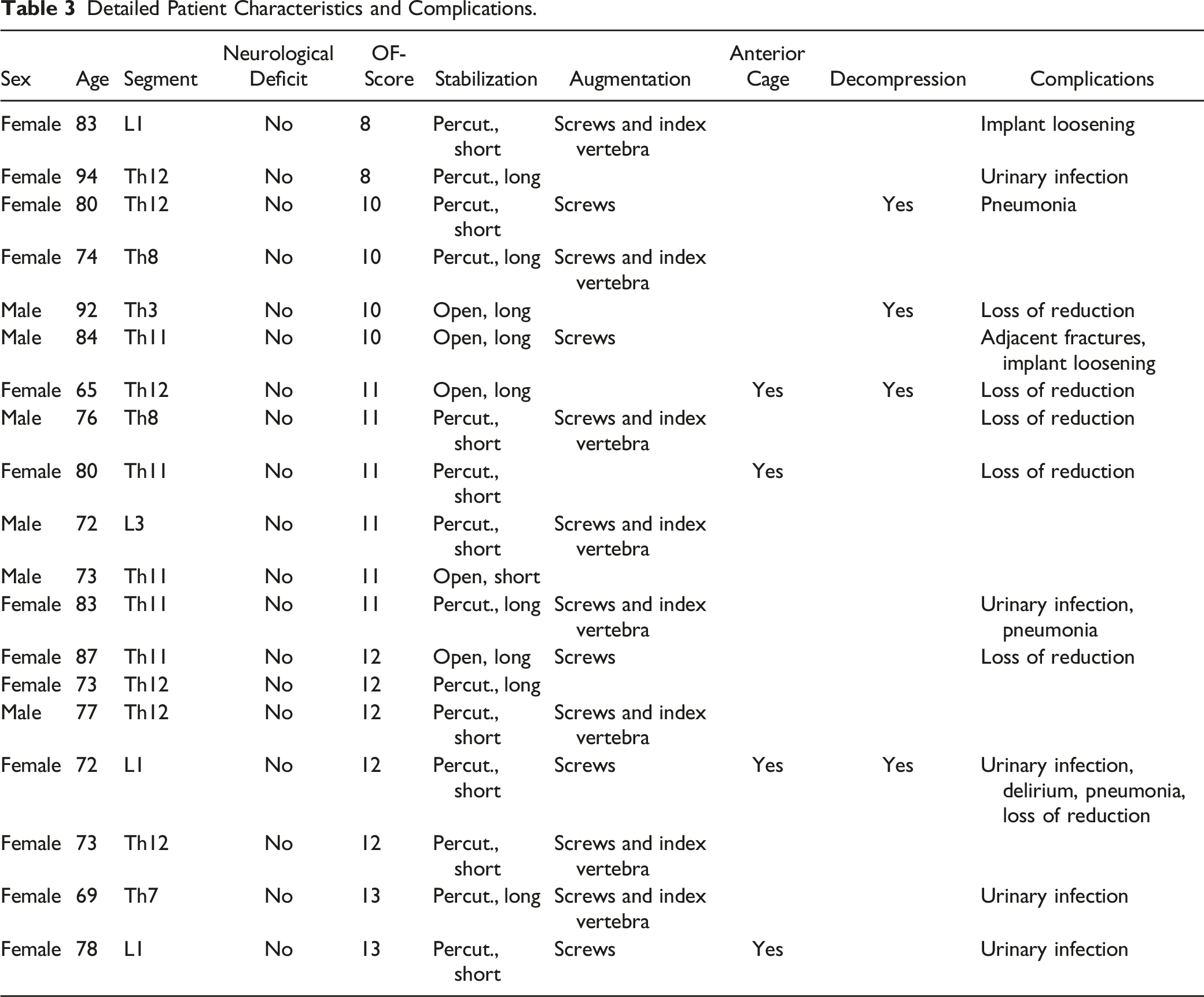
All patients with an OF 5 fracture underwent surgical stabilization. Operative treatment consisted of long-segment (> 4 levels) posterior instrumentation in 9 cases (47 %, 4 open, 5 percutaneously). Short-segment bisegmental posterior instrumentation was performed in 10 cases (53 %). In 13 cases (68%), pedicle screws were augmented with polymethylmetacrylat cement (PMMA).
In 8 cases (42%) the fractured vertebra was augmented with PMMA. Additional anterior reconstruction with cages was done in 4 patients, in 3 of those where only short-segment posterior instrumentation was performed.
Only 2 patients (11 %) received short-segment posterior instrumentation without either anterior reconstruction or cement-augmentation of the fractured vertebra, both had injuries without significant comminution of the vertebral body. One was mobile without aids at the time of admission and the other reported very good subjective health status of 90 from 100 maximal points.
On admission, one patient was on medication with bisphosphonates and 4 had medication with vitamin D and/or calcium. When discharged after surgery, 9 patients were prescribed bisphosphonates and 15 patients vitamin D and/or calcium.
Functional Outcome, Quality of Life and ADLs
Mean follow-up was 20 ± 10 weeks (range, 12 to 48 weeks). In nearly all functional outcome parameters, patients showed significant improvements at the time of discharge and at final follow-up (P < .001) except for the anxiety/depression item of the EQ-5D 5L (P = .08, Figures 1 and 2). The ES range from .512 (mobility level) up to .812 (ODI), which are expression of very large effects, equivalent to Cohens d of 2.0 and 4.0, following.
14
The non-significant outcome parameter (EQ-5D 5L anxiety/depression) also showed a large effect with ES .155, corresponding to .8 in Cohens d. Functional outcome. (A) Pain measured by the Visual Analogue Scale (VAS). (B) Mobility with 1: no aids, 2: crutches/walker, 3: high walker 4: sitting/standing without walking 5: bedridden. (C) Oswestry Disability Index (ODI), with lower values representing better function and less complaints. (D) Barthel Index, with higher values representing a higher ability to perform activities of daily living. Quality of life as measured by EQ-5D 5L.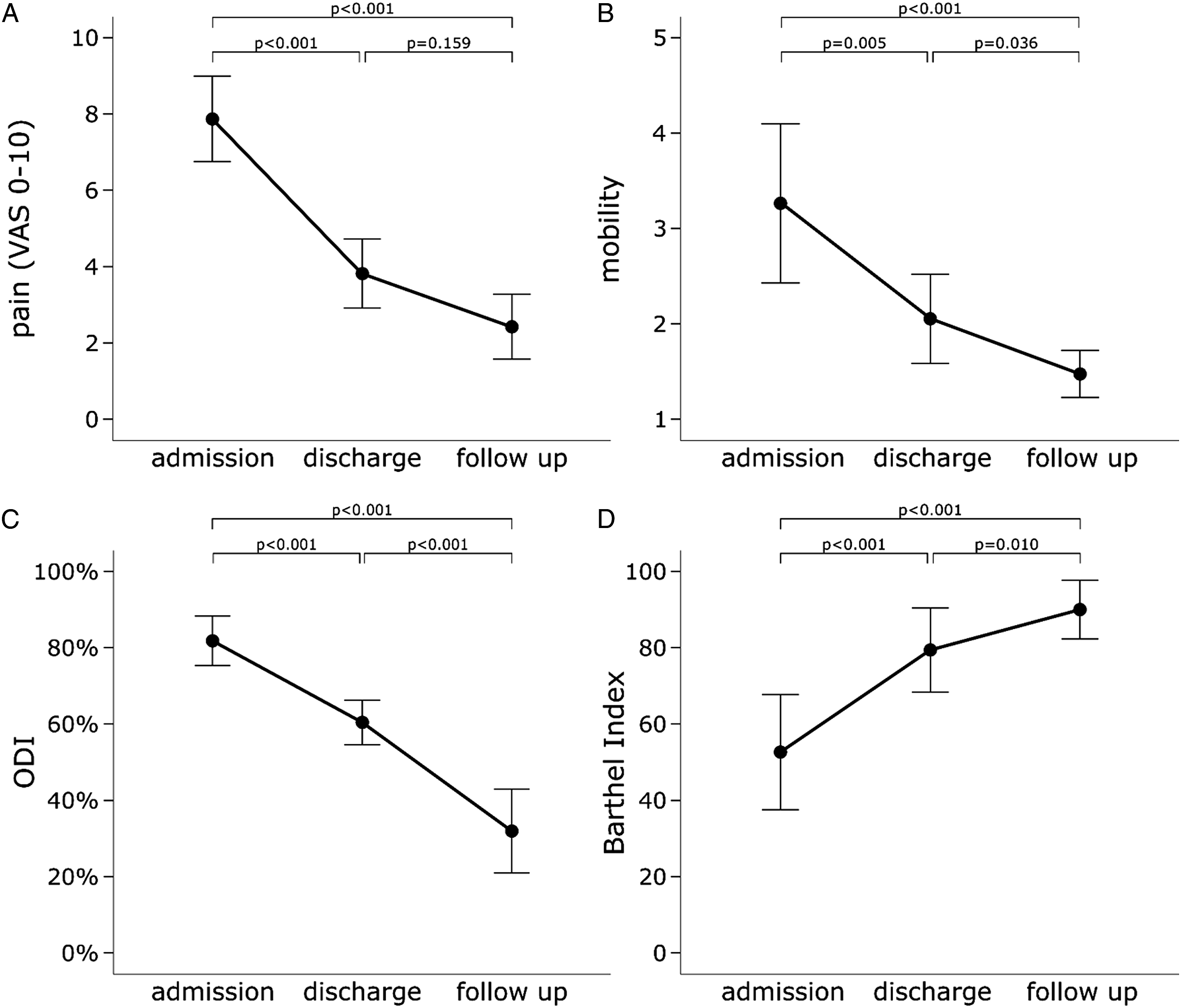
Complications
Neither neurological deficits nor thrombo-embolic events were observed postoperatively. Five patients (26 %) had UTI, 3 patients (16 %) developed pneumonia and in one patient (5 %) a delirium was observed during hospitalization. No major complication occurred and all complications resolved without sequelae.
No surgical site infection occurred during the follow-up period. Two patients showed implant loosening, in one case combined with adjacent vertebral fractures, but none of these patients required revision surgery. Four patients (21%) showed secondary fracture loss of reduction without further sequelae.
Discussion
This study aimed to analyse the surgical strategies applied to OF 5 injuries to thoracolumbar spine and to assess related complications and clinical outcome.
In this subgroup analysis of OF 5 fracture patients of a larger prospective study (EOFTT) on OVF, all patients underwent operative treatment and showed significant improvement in terms of functional outcome and quality of life. While a large part of the elderly patients had general complications like UTIs or pneumonia, no complications requiring revision surgery were observed during the observation period.
Many authors recommend long-segment stabilization (more than 2 segments above and below the fracture) for spinal injuries with a higher degree of instability.3,15 Even though OF 5 fractures are considered highly unstable, 10/19 patients (53 %) in the present study received short-segment bisegmental fixation. However, only 2 patients received short-segment posterior instrumentation without either anterior reconstruction or cement-augmentation of the fractured vertebra.
Biomechanical studies show a significant increase in construct stability of short-segment posterior instrumentation of OVF when anterior cement augmentation is added 16 and clinical studies show good functional outcomes and moderate complication rates for short-segment “hybrid” stabilization in OVF. 17 Korovessis et al reported good clinical and radiological outcomes after pedicle screw fixation plus kyphoplasty for thoracolumbar fractures A2, A3 and B2 in a cohort aged 59 ± 17 years. 18
Still, long-segment posterior stabilization was performed in almost half of the cases even though this was a cohort of elderly patients with impaired bone quality and a mean ASA of 3.
The fact, that no revision surgeries were necessary underlines that shorter constructs in combination with some kind of anterior support either by reconstruction or by cement-augmentation may possible in selected patients even in view of OF 5 injuries. In contrast to younger patients with spine injuries with anterior or posterior tension band failure, none of the patients in the present cohort had neurological deficits. This may indicate much a lower energy of the underlying trauma in OF5 fractures.
Limitations
The short follow-up period of mean 5 months (mean 20 ± 10 weeks, range 12 to 48 weeks) does not allow any firm conclusions on the final outcome of the patients. Unfortunately, a longer follow-up was not possible in many cases because this is a cohort of geriatric patients. In some cases, the patients had already died or were not able to be transported from their nursing homes for too many follow-up appointments. However, all patients improved after surgical treatment and were ambulatory on follow-up, and most complications after operative stabilization of OVF that require revision surgery occur within the first 3 months. 19 Hence, a follow-up of 5 months is a strong indicator for the long-term outcome. Since OF 5 injuries are highly unstable and do not heal properly with conservative treatment, the results can be considered as favourable, despite a relatively high general complication rate. A further limitation is the small sample size. Highly unstable fractures like OF 5 injuries are rather rare and account for only 2.6% of all OVF. 2 To the authors knowledge this is still the study with the biggest cohort of patients with osteoporotic thoracolumbar vertebral fractures with anterior or posterior tension band failure.
In view of the high rate of general complications, an analysis of the time from admission to surgery would have been of interest but was not possible due to the small sample size. In general, it has been shown, though, that time to surgery has no effect on mortality in geriatric patients with osteoporotic vertebral compression fractures. 20
Further limitations are that no data on sagittal or coronal spinal alignment or on pre-existing degenerative changes were evaluated as imaging of the whole spine was not a standard for patients with OVF in most contributing centers. Especially the presence of a pronounced degenerative scoliosis would be an explanation to trigger a decision towards short-segment fixation.
Even though only 4 patients received anterior column reconstruction by implantation of a cage, many of the remaining patients received cement-augmentation of the fractured vertebra. This reflects the decision-making process in OVF on a fine line between the required stability in unstable fractures and the lowest possible leverage forces to be aimed for in osteoporotic bone. This represents a dilemma that is particularly evident in OFs with anterior or posterior tension band failure (OF 5). Future studies need to address these injuries in larger cohorts or registries and longer follow-up time and may focus on the true benefit of long-segment fixation vs short-segment posterior instrumentation in combination with anterior reconstruction or cement-augmentation.
Conclusion
In this analysis of patients with type OF 5 OVF fractures, surgical stabilization was the treatment of choice and lead to significant improvement in terms of functional outcome and quality of life. While general complications like hospital-acquired infections were frequent, no revision surgery was necessary during the observation period.
Long-segment and short-segment posterior instrumentation in combination with anterior reconstruction or cement-augmentation seem to be viable options in these patients depending on the local kyphosis and vertebral body comminution.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).