
Abstract
Study Design
Multicenter prospective study.
Objective
The influence of central sensitization (CS) on neurological symptoms and surgical outcomes in patients with degenerative cervical myelopathy (DCM) remains unknown. This study aimed to investigate the effects of preoperative CS on surgical outcomes of patients with DCM following posterior decompression surgery.
Methods
77 consecutive patients with DCM (mean age 67.1) who received posterior decompression surgery were included in this study. The participants completed CS inventory (CSI) scores and the following patient-reported outcome measures (PROMs) preoperatively and 12 months postoperatively: the Japanese Orthopaedic Association (JOA) score for cervical myelopathy and JOA cervical myelopathy evaluation questionnaire (JOACMEQ) for cervical spinal diseases. The association of preoperative CSI scores with preoperative and postoperative PROMs was analyzed, and their changes were statistically evaluated.
Results
The preoperative CSI score was significantly decreased at 12 months postoperatively, and it was significantly associated with the JOA score and JOACMEQ preoperatively and at 12 months postoperatively. However, no significant association was observed between preoperative CSI and the postoperative change of any PROMs at 12 months. The posterior decompression surgery significantly improved the JOA scores and ‘lower extremity function’ and ‘quality of life (QOL)’ domains of the JOACMEQ, independent of the severity of preoperative CSI score. Multiple regression analysis demonstrated that preoperative CSI was significantly associated with the ‘QOL’ domain of JOACMEQ and original JOA score at 12 months postoperatively.
Conclusion
The CSI score can be an auxiliary indicator of surgical outcomes of patients with DCM following posterior decompression surgery.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is a common neurological disorder in adults worldwide.1,2 DCM encompasses various spondylotic and non-spondylotic pathologies related to degeneration of cervical spine structures, including ligaments (hypertrophy, calcification, and ossification), intervertebral discs, and osseous tissues.1-3 The static and/or dynamic compression of spinal cord due to these degenerative changes of cervical spine induces ischemia, inflammation, and apoptosis within the spinal cord, that results in cervical myelopathy 4 with various symptoms ranging from paresthesia in the upper extremities, clumsiness of hands, motor weakness, gait abnormality to quadriparesis.
Posterior decompression surgery, particularly cervical laminoplasty, is an effective treatment for this condition because of its excellent surgical outcome 5 ; however, surgical outcome does not always reach satisfactory results for the patients because of residual neurological symptoms such as hand numbness and gait disturbance. 6
The development of chronic pain in the musculoskeletal system is associated with the changes in pain processing in the central nervous system. 7 CS is a physiological manifestation of the excessive plasticity of the somatosensory nervous system in response to inflammatory stimuli and/or neural injury. 7 Central sensitization (CS) is defined as an amplification of neural signaling within the central nervous system that elicits pain hypersensitivity. 7 There is growing evidence that CS is responsive for the underlying mechanism of musculoskeletal disorders including low back pain, 8 osteoarthritis, 9 rheumatoid arthritis, 10 and neck and/or shoulder pain. 11 Recently, the CS inventory (CSI), a patient reported screening tool, has been widely used to assess the severity of CS-related symptoms in musculoskeletal disorders.12-15 It has been previously reported that CS evaluated by the CSI had a significant association with preoperative neurological symptoms and health-related QOL for patients who received cervical spine surgeries. 16 However, the influence of CS on postoperative clinical outcomes following cervical spine surgeries remains unknown. We hypothesized that the CS has effects on the neurological symptoms of patients with DCM and is also associated with outcomes of posterior decompression surgery.
This study aimed to investigate whether preoperative CS has an effect on the surgical outcome of patients with DCM following posterior decompression surgery in a multicenter prospective study.
Material and Methods
Study Design and Setting
This is a prospective multicenter cohort study. This study was approved by the Clinical Research Ethics Review Committee of Mie University Hospital (Approval number: H2020-027). Written informed consent was obtained from all the patients included in this study.
Participants
In total, 152 consecutive patients who received cervical spine surgery at 8 different institutions from May 2019 to May 2020 were included in this study. Of the patients, 9 who received spine surgeries because of acute spinal injury, spinal hematoma, infection, and spinal metastasis were excluded from this study. Initially, 143 patients were included; however, 21 patients with cervical spondylotic radiculopathy, cervical spondylotic amyotrophy, cervical deformity, or cervical tumor and 13 patients who underwent anterior cervical discectomy and fusion were excluded. Among the 109 remaining patients, 32 patients (29.4%) dropped out from the study at 12 months of follow-up. Finally, data of 77 patients were analyzed for this study (Figure 1). The patients with DCM were subtyped into cervical spondylotic myelopathy (CSM) and ossification of posterior longitudinal ligament (OPLL) patients according to the main pathology of cervical myelopathy. Flowchart of patient selection. Degenerative cervical myelopathy (DCM), cervical spondylotic myelopathy (CSM), and ossification of posterior longitudinal ligament (OPLL).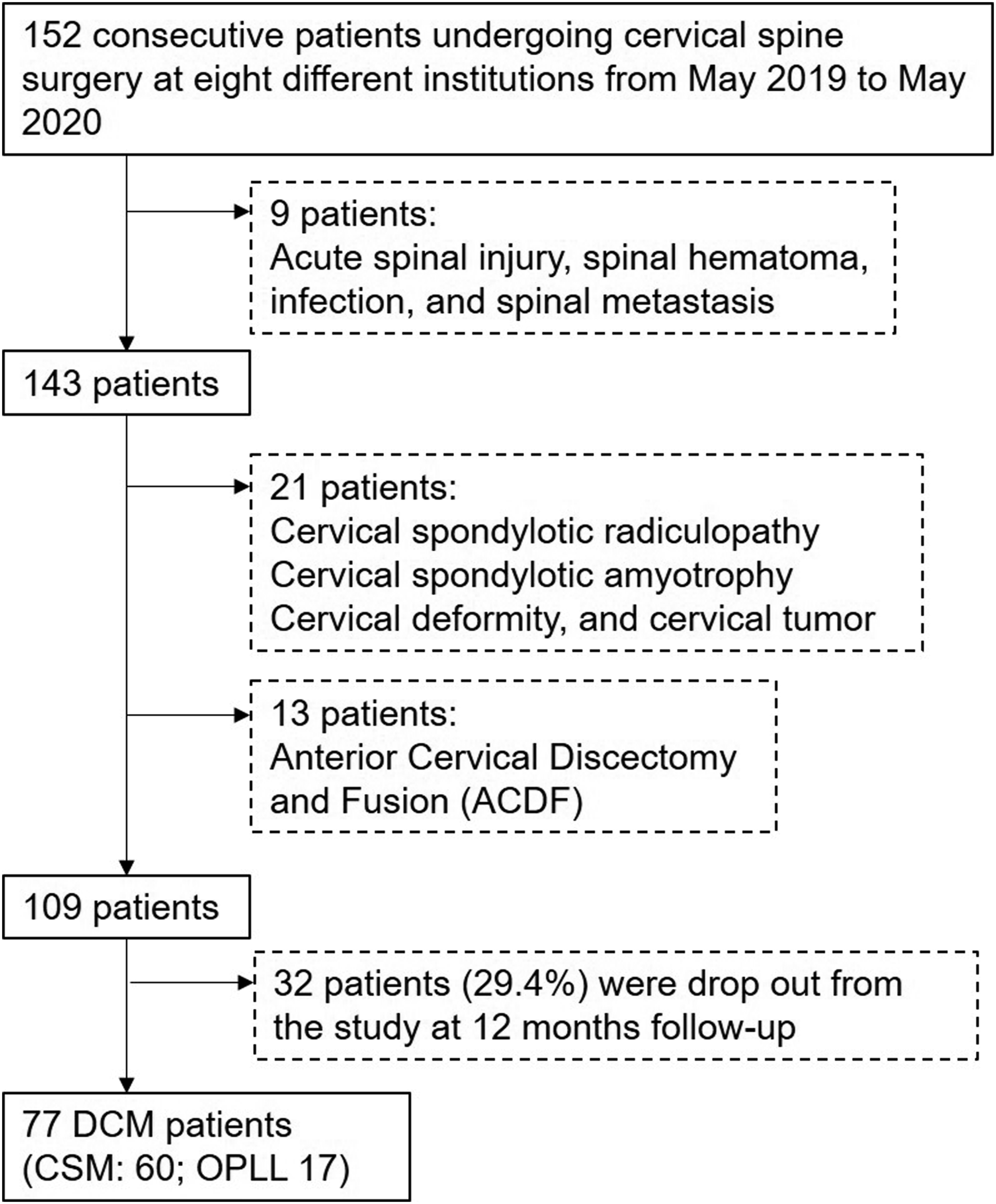
Measurement Properties
Demographic information, including age, sex, and spinal disease diagnosis, were collected. The participants completed the following patient-reported outcome measures (PROMs) preoperatively (Pre) and 12 months postoperatively (Post 12M).
Central Sensitization Inventory
The CSI is a self‐reported measure for quantifying the extent of individual somatic and emotional complaints associated with CS. 12 The Japanese version of the CSI, with high reliability and validity of which has been reported, 15 was used in this study. The Japanese CSI is a 25‐item questionnaire for assessing health‐related symptoms common in CS conditions, where each item can be scored on a 5‐point Likert scale ranging from 0 = “never” to 4 = “always.” The total score ranges from 0 to 100 points. CSI severity was classified into 5 categories according to the total score points as follows: subclinical (0 to 29 points); mild (30 to 39 points); moderate (40 to 49 points); severe (50 to 59 points); and extreme (60 to 100 points). 13 For evaluating the association between CSI severity and PROMs, CSI severity was classified into 3 groups: subclinical (0 to 29 points); mild (30 to 39 points); and moderate to extreme (≥40) in this study.
Japanese Orthopaedic Association Score for Cervical Myelopathy
The JOA score 17 consists of 6 domain scoring systems including the following: motor dysfunction in the upper extremities; motor dysfunction in the lower extremities; sensory function in the upper extremities; sensory function in the trunk; sensory function in the lower extremities; and bladder function, with a minimum total score of −2 to 17. Higher scores indicate better condition.
Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire
The JOACMEQ is a self-administered questionnaire for evaluating specific outcome measures, including patient disability, handicaps, and general health of cervical myelopathy.18-23 The JOACMEQ comprises 24 questions in 5 domains: cervical spine function, upper extremity function, lower extremity function, bladder function, and QOL; and the range of the score for each domain is from 0 to 100, with higher scores indicating better condition. The degree of pain or stiffness in the neck or shoulder (neck or shoulder), tightness in the chest (chest), pain and numbness in the arms or hands (arms or hands), and pain or numbness from chest to toe (chest to toe) was evaluated using a visual analog scale (VAS) of 0 to 100 (mm), with 0 as “no pain or numbness at all” and 100 as “the most intense pain or numbness imaginable.”
Statistical Analysis
Differences in CSI, VAS (mm), and the 5 domains of JOACMEQ between the Pre and Post 12M periods were analyzed using a paired T-test or Mann–Whitney U test. Correlations between CSI and age and PROMs were evaluated using the Pearson’s correlation coefficient test or Spearman rank-order correlation test. Differences in each domain of the JOA score and JOACMEQ among the CSI severity groups were analyzed using the Kruskal–Wallis test both Pre and Post 12M. Differences in VAS scores among the CSI severity groups were assessed using a one- or two-way repeated measured analysis of variance (ANOVA), followed by the Bonferroni post hoc test both Pre and Post 12M. A multiple regression analysis was performed to identify factors contributing to the scoring of CSI as a dependent variable with patient-related parameters. Significance was set at P < .05. All the statistical analyses were performed using IBM SPSS Statistics (Software version: 28.0, IBM Japan, Tokyo).
Results
Patient Characteristics
Patient Characteristics.
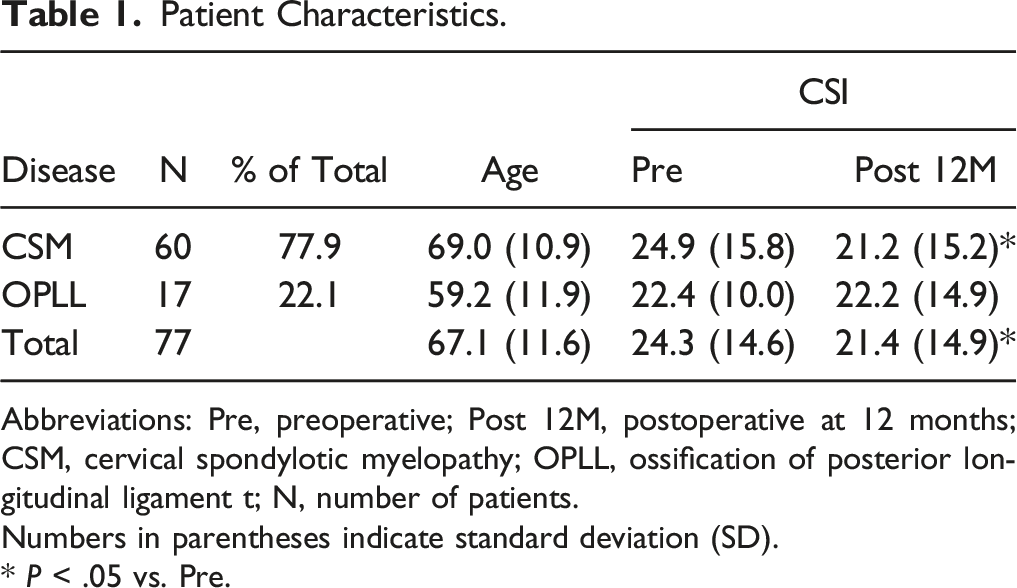
Abbreviations: Pre, preoperative; Post 12M, postoperative at 12 months; CSM, cervical spondylotic myelopathy; OPLL, ossification of posterior longitudinal ligament t; N, number of patients.
Numbers in parentheses indicate standard deviation (SD).
* P < .05 vs. Pre.
Changes in Central Sensitization Inventory
The mean preoperative CSI score of the total population was 24.3 ± 14.6 (Figure 1A). According to CSI severity group, the cases were classified as subclinical 64.9% (n = 50); mild 22.1% (n = 17); and moderate to extreme 13.0% (n = 10) (Figure 1B). The mean preoperative CSI score was significantly decreased at Post 12M (21.4 ± 14.9, P < .05) (Figure 2A), and the cases were classified as subclinical 77.1% (n = 54); mild 11.4% (n = 8); and moderate to extreme 11.4% (n = 8) (Figure 2B). Change in central sensitization inventory (CSI) score preoperatively and 12 months postoperatively. (A) Mean score at preoperative (Pre) and postoperative 12 months (Post 12M) periods. (B) Change in percentage of CSI severity groups at Pre and Post 12M. Subclinical (0 to 29 points); mild (30 to 39 points); and moderate to extreme (≥40). The italic numbers above the square brackets indicate P-value against group comparison. *P < .05, **P < .01.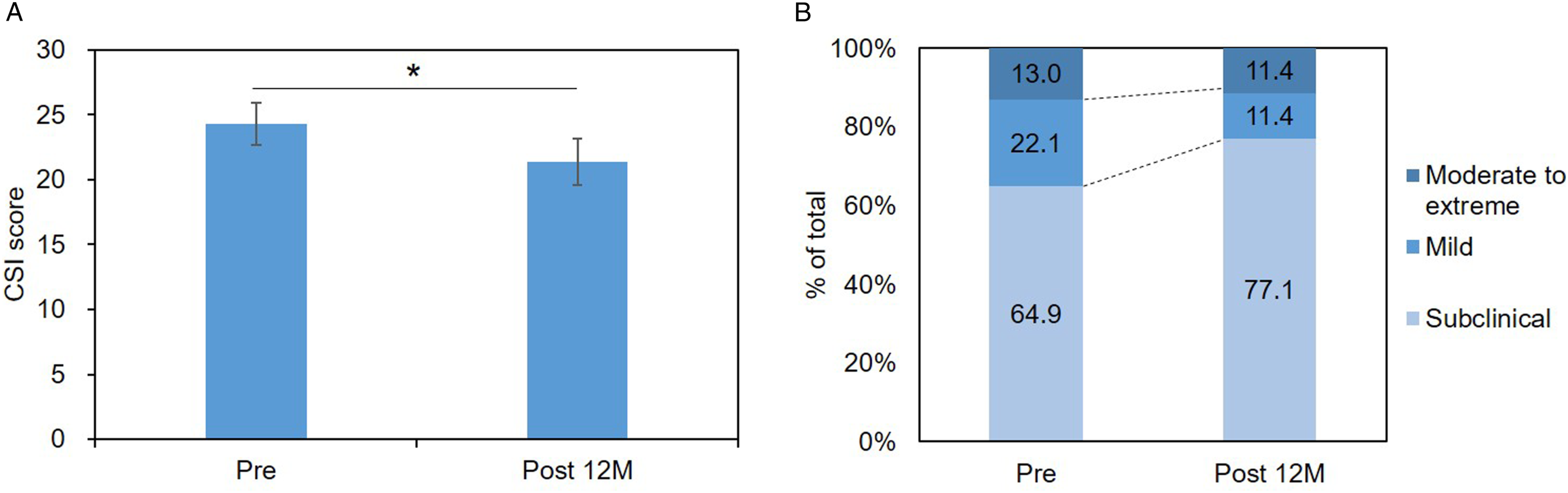
The mean preoperative CSI score of women (28.6 ± 15.2) was significantly higher than that of men (22.2 ± 14.1, P < .05); however, no significant differences were observed at Post 12M (P = .85). A significant but weak correlation between age and CSI score was observed preoperatively (r= .24, P < .05), while no significant correlation was identified at Post 12M. When the CSI score was evaluated by subtype, the mean preoperative CSI score of the patients with CSM was significantly lower than that at Post 12M (P < .05, Table 1). However, no significant differences were observed in patients with OPLL (Table 1).
Changes in Patient-Reported Outcome Measures
Japanese Orthopaedic Association Score for Cervical Myelopathy
Change in Japanese Orthopaedic Association (JOA) Score for Cervical Myelopathy and Visual Analog Scale (VAS) of Neurological Symptoms
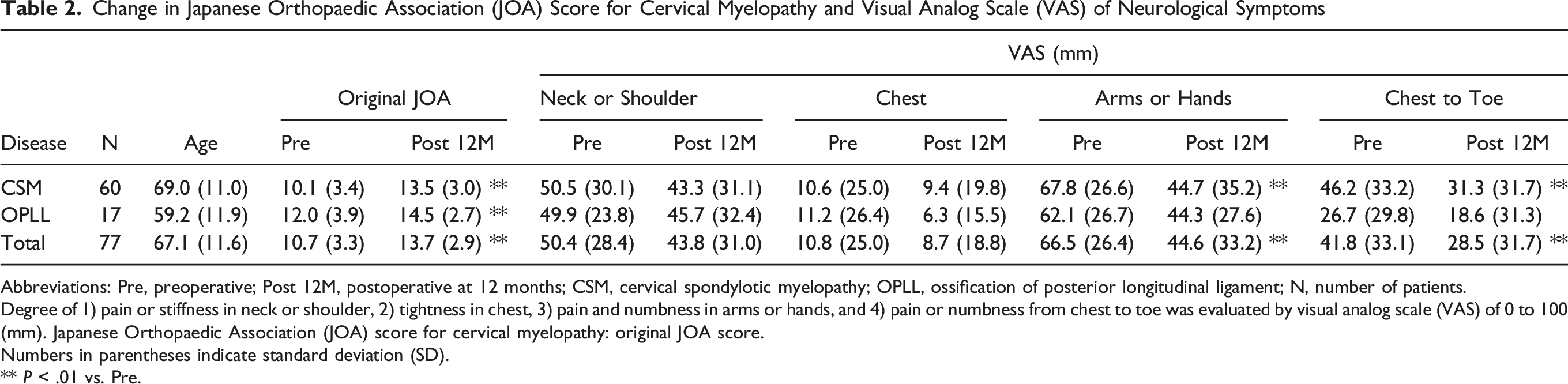
Abbreviations: Pre, preoperative; Post 12M, postoperative at 12 months; CSM, cervical spondylotic myelopathy; OPLL, ossification of posterior longitudinal ligament; N, number of patients.
Degree of 1) pain or stiffness in neck or shoulder, 2) tightness in chest, 3) pain and numbness in arms or hands, and 4) pain or numbness from chest to toe was evaluated by visual analog scale (VAS) of 0 to 100 (mm). Japanese Orthopaedic Association (JOA) score for cervical myelopathy: original JOA score.
Numbers in parentheses indicate standard deviation (SD).
** P < .01 vs. Pre.
Visual Analog Scale of Neurological Symptoms
Mean preoperative scores of VAS in ‘arms or hands’ and ‘chest to toe’ were significantly decreased at Post 12M (P < .01, respectively) (Table 2). Those of the CSM patients were significantly decreased at Post 12M (P < .01, respectively, Table 2).
Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire
Change in Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ)
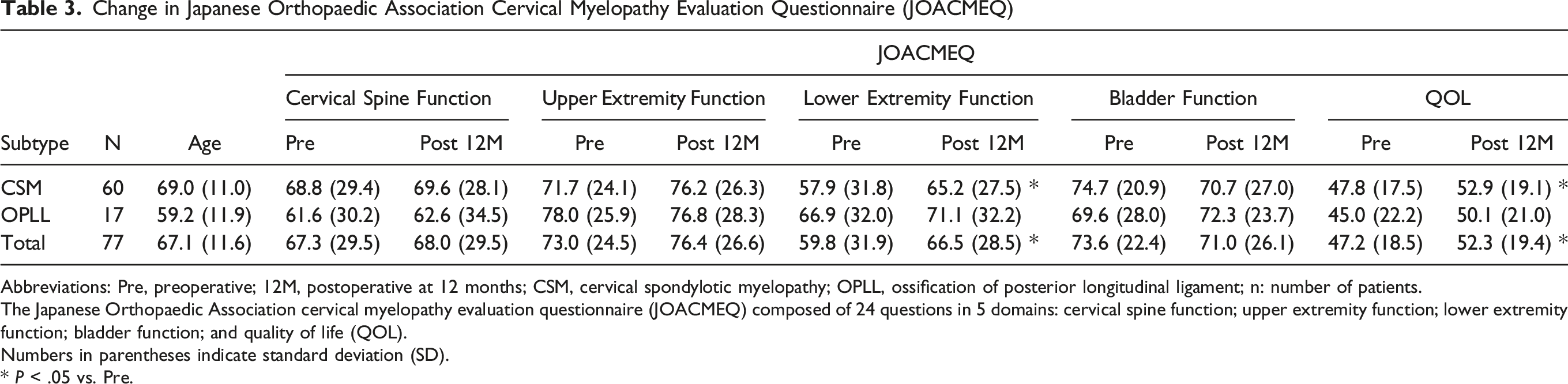
Abbreviations: Pre, preoperative; 12M, postoperative at 12 months; CSM, cervical spondylotic myelopathy; OPLL, ossification of posterior longitudinal ligament; n: number of patients.
The Japanese Orthopaedic Association cervical myelopathy evaluation questionnaire (JOACMEQ) composed of 24 questions in 5 domains: cervical spine function; upper extremity function; lower extremity function; bladder function; and quality of life (QOL).
Numbers in parentheses indicate standard deviation (SD).
* P < .05 vs. Pre.
Correlation Between Preoperative Central Sensitization Inventory and Patient-Reported Outcome Measures
Correlation Between the Preoperative Central Sensitization Inventory (CSI) and Patient-Reported Outcome Measures (PROMs).
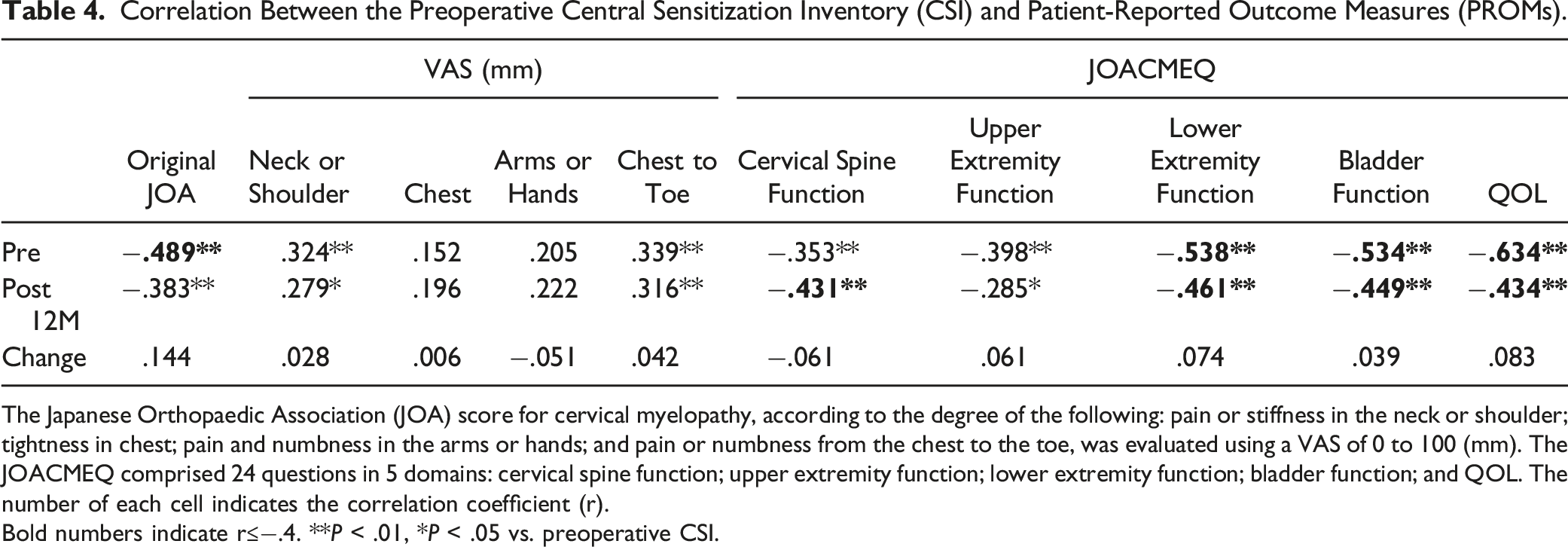
The Japanese Orthopaedic Association (JOA) score for cervical myelopathy, according to the degree of the following: pain or stiffness in the neck or shoulder; tightness in chest; pain and numbness in the arms or hands; and pain or numbness from the chest to the toe, was evaluated using a VAS of 0 to 100 (mm). The JOACMEQ comprised 24 questions in 5 domains: cervical spine function; upper extremity function; lower extremity function; bladder function; and QOL. The number of each cell indicates the correlation coefficient (r).
Bold numbers indicate r≤−.4. **P < .01, *P < .05 vs. preoperative CSI.
In the preoperative evaluation, a significant negative correlation (moderate or higher: r ≤ −.4) was observed between preoperative CSI and JOA scores and lower extremity function, bladder function, and QOL domains of the JOACMEQ (Table 4). The preoperative CSI scores were significantly correlated (moderate or higher: r ≤ −.4) with cervical spine function, lower extremity function, bladder function, and QOL of the domains of the JOACMEQ at Post 12M (Table 4). The preoperative CSI did not indicate a significant correlation with the change (Post 12M − Pre) in any PROMs (Table 4).
Association Between Preoperative Central Sensitization Inventory Severity and Patient-Reported Outcome Measures
Change in the Japanese Orthopaedic Association Score
The preoperative JOA scores were the highest in the ‘subclinical’ group followed by ‘mild’ and ‘moderate to extreme’ groups (between groups: P < .01) and those of each 3 groups increased similarly at Post 12M (P < .01, Figure 3). The changes in JOA scores (Post 12M − Pre) did not differ significantly among the 3 groups (P = .20, Figure 3). Japanese Orthopaedic Association (JOA) score for cervical myelopathy according to the severity of the central sensitization inventory (CSI). The patients were divided into 3 groups according to CSI severity (subclinical [0 to 29 points]; mild [30 to 39 points]; and moderate to extreme [>40 points]). The mean JOA score of each group at the preoperative (Pre) and postoperative 12 months (Post 12M) periods and the postoperative change (Post 12M-Pre) are presented. The italic numbers above the square brackets indicate P-value against group comparison. *P < .05, **P < .01.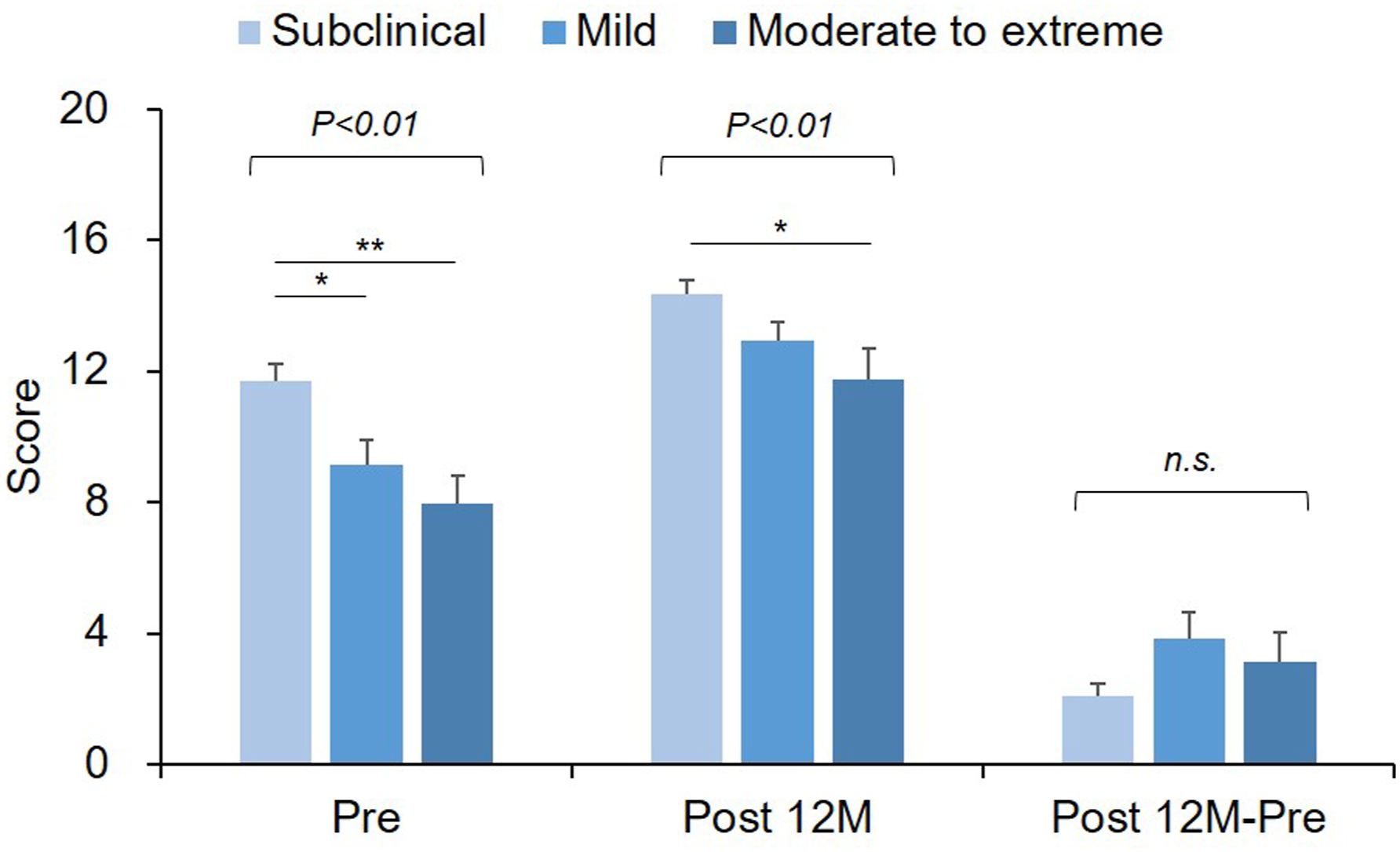
Change in Visual Analog Scale
Preoperative VAS scores in the ‘neck or shoulder’, ‘arms or hand’, and ‘chest to toe’ were the highest in the ‘moderate to extreme’ group followed by ‘mild’ and ‘subclinical’ groups (between groups: P < .05, P = .14, P < .05, respectively, two-way repeated measures ANOVA) and those of each group decreased at Post 12M (time: P = .09, P < .01, P < .01, respectively; interaction: P = .58, P = .46, P = .88, two-way repeated measures ANOVA) (Figure 4A, C, and D). Postoperative VAS scores in these 3 areas demonstrated a similar trend to be highest in the ‘moderate to extreme’ group followed by ‘mild’ and ‘subclinical’ groups (Figure 4A, C, and D). No significant differences in the postoperative changes (Post 12M − Pre) of the 3 areas were observed among the 3 CSI severity groups (Figure 4A, C, and D). Visual analog scale (VAS) for cervical myelopathy by severity of the central sensitization inventory (CSI). The patients were divided into 3 groups according to CSI severity (subclinical [0 to 29 points]; mild [30 to 39 points]; and moderate to extreme [>40 points]). Degree of A) pain or stiffness in the neck or shoulder, B) tightness in the chest, C) pain and numbness in the arms or hands, and D) pain or numbness from the chest to the toe was evaluated using a visual analog scale (VAS) of 0 to 100 (mm). The mean VAS score of each group at the preoperative (Pre) and postoperative 12 months (Post 12M) periods and the postoperative change (Post 12M − Pre) is presented. The italic numbers above the square brackets indicate P-value against group comparison. The numbers in the square box indicate the results of the two-way repeated measures of analysis of variance (ANOVA). *P < .05, **P < .01.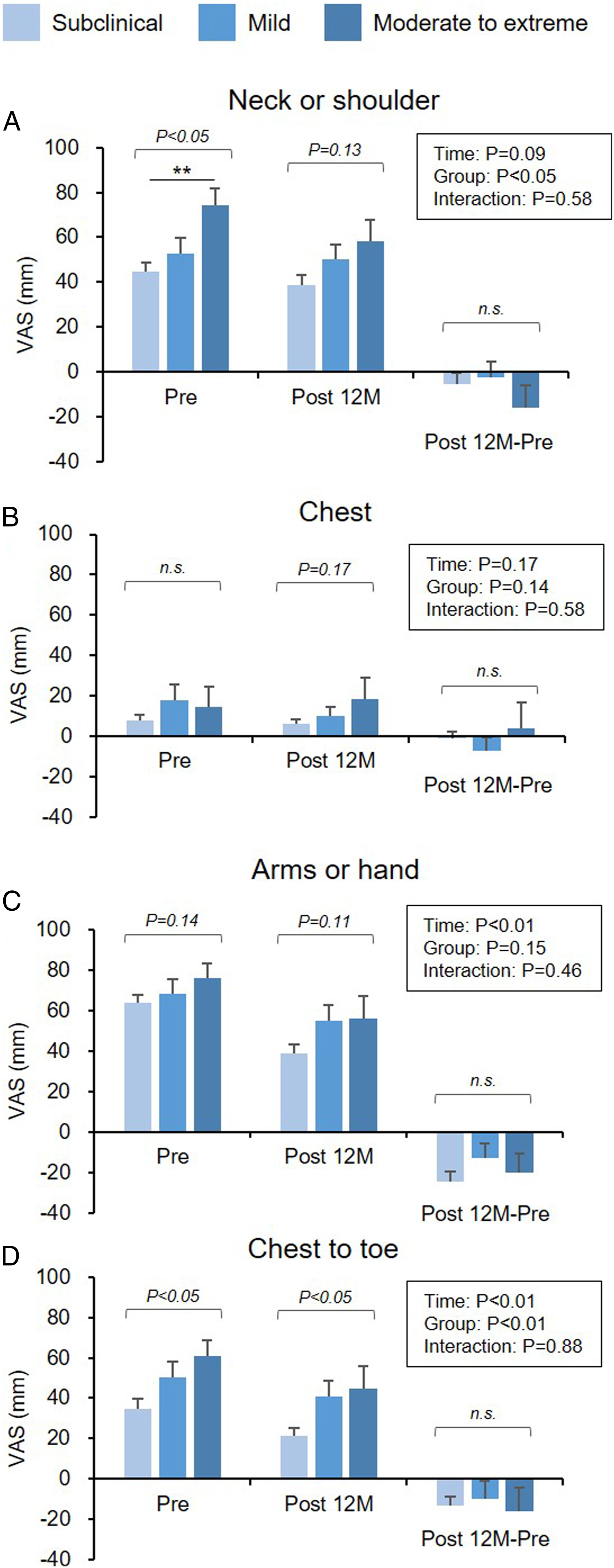
Preoperative VAS scores in the ‘chest’ of 3 groups did not significantly decrease at Post 12M (time: P = .68, interaction: P = .58, Figure 4B). The VAS scores did not differ significantly among the groups both at Pre and Post 12M (Figure 4B).
Change in the JOACMEQ
All the 5 domains of the JOACMEQ differed significantly among the 3 CSI severity groups both at preoperatively and 12 months postoperatively (Figure 5) and demonstrated the general trends that those scores were the highest in the ‘subclinical’ group followed by ‘mild’ and ‘moderate to extreme’ groups both at Pre and Post 12M (Figure 5). The Japanese Orthopaedic Association cervical myelopathy evaluation questionnaire (JOACMEQ) according to the severity of the central sensitization inventory (CSI) score. The patients were divided into 3 groups according to CSI severity (subclinical [0 to 29 points]; mild [30 to 39 points]; and moderate to extreme [>40 points]). The JOACMEQ comprising 24 questions in 5 domains: (A) cervical spine function; (B) upper extremity function; (C) lower extremity function; (D) bladder function; and (E) quality of life (QOL). The mean score of each group at the preoperative (Pre) and postoperative 12 months (Post 12M) periods and the postoperative change (Post 12M − Pre) is presented. The italic numbers above the square brackets indicate P-value against group comparison. *P < .05, **P < .01.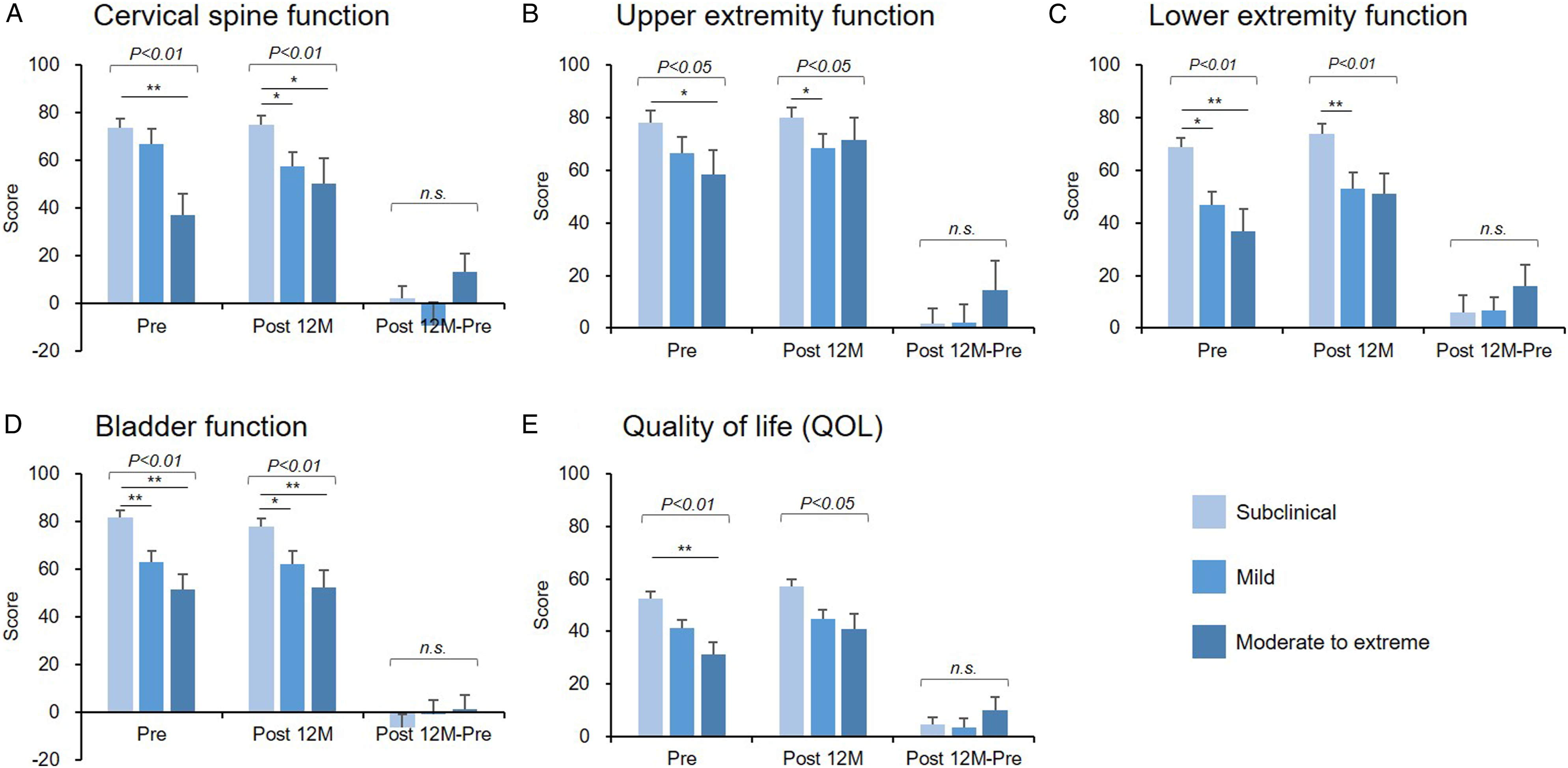
The subclinical group had significantly increased ‘lower extremity function’ (P < .05) and ‘QOL’ domain (P < .05) at Post 12M than at Pre. However, no significant differences in the postoperative changes (Post 12M − Pre) in all the 5 domains of JOACMEQ were observed among the 3 groups (Figure 5).
Associated Factors With Preoperative Central Sensitization Inventory
Association of Preoperative Central Sensitization Inventory (CSI) with Patient-Reported Outcome Measures of Cervical Spine Diseases at 12 months Postoperatively
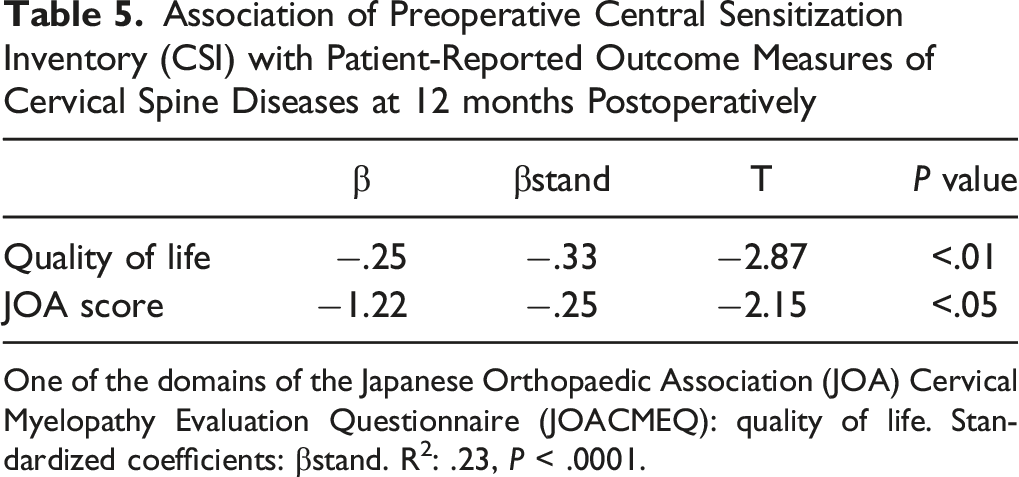
One of the domains of the Japanese Orthopaedic Association (JOA) Cervical Myelopathy Evaluation Questionnaire (JOACMEQ): quality of life. Standardized coefficients: βstand. R2: .23, P < .0001.
Discussion
Our study demonstrated, for the first time, that CS evaluated by CSI influences on the neurological symptoms, disability and QOL of the patients with CSM. The posterior decompression surgery significantly improved the JOA scores, VAS scores in the ‘arms or hand’ and ‘chest to toe’ and ‘lower extremity function’ and ‘quality of life (QOL)’ domains of the JOACMEQ, independent of the severity of preoperative CSI score. Preoperative CSI was negatively associated with ‘QOL’ of the JOACMEQ domain and original JOA score at 12 months postopertively.
The results of this study revealed that the preoperative CSI score was significantly decreased at 12 months after the posterior decompression surgery. Interestingly, Koh et al. 24 have reported no significant differences in the pre- and postoperative CSI scores after the excision of the peripheral nociceptive pain source of knee OA in patients who received total knee arthroplasty. The authors speculated that the extent of CS-related symptoms was improved by direct decompression of the damaged spinal cord, which led to the change in the microenvironment within the spinal cord following the surgical treatment. Meanwhile, in the subgroup analysis, the CSI score of patients with OPLL was not changed postoperatively. The pathomechanism of spinal cord compression in CSM patients includes disc bulging, osteophyte formation, hypertrophy, and calcification of the ligamentum flavum. 1 On the other hand, the main pathology in OPLL patients is the ectopic ossification of posterior longitudinal ligament. Although all of the patients in this study underwent posterior decompression surgery, the extent of decompression and the postoperative microenvironmental changes within the spinal cord may differ between the CSM and OPLL patients. The differences in the pathogenesis1,25 and baseline PROMs between the patients with CSM and OPLL might explain this discrepancy.
Moreover, the preoperative CSI had a weak-to-moderate correlation with the VAS in the ‘neck or shoulder’ and ‘chest to toe’, JOA score and all 5 domains of the JOACMEQ both pre- and postoperatively. This suggests that the extent of CS evaluated by CSI score was significantly associated with cervical myelopathy related neurological symptoms, disability and QOL both preoperatively and postoperatively. However, no significant correlation was observed between preoperative CSI and the postoperative changes of all the PROMs at 12 months, suggesting that the preoperative PROMs of patients with myelopathy improved by decompression surgery regardless of the preoperative CSI score.
Next, when the patients were classified according to the severity of CSI score, the VAS in the ‘neck or shoulder’, ‘arms or hands’, and ‘chest to toe’ revealed a higher score according to the CSI severity both pre- and postoperatively even though the VAS in all the 3 groups decreased postoperatively. Similarly, the JOA score and all 5 domains of JOACMEQ demonstrated the highest score in the ‘subclinical’ group followed by ‘mild’ and ‘moderate to extreme’ groups, and this trend was maintained at Post 12M regardless of the improvements of these scores by decompression surgery. These results indicate that preoperative CSI score was significantly associated with the preoperative neurological symptoms, disability, and QOL of patients with myelopathy. Importantly, this association remained unchanged until Post 12M. Hence, we have conducted a multiple regression analysis to identify the PROMs at Post 12M that were associated with preoperative CSI. Hence, preoperative CSI was independently associated with the ‘QOL’ domain of the JOACMEQ and original JOA score at Post 12M.
This study had several limitations. First, the patients who underwent posterior decompression with/without stabilization were included in this study. Second, cervical alignment, which is 1 of the important factors affecting neurological symptoms and surgical outcomes, was not evaluated. Third, the extent of CS was measured by CSI score used for evaluating CS-related symptoms12,15 but not quantitative sensory testing (QST).26,27 Therefore, evaluating CS by QST in addition to CSI might improve accuracy. Fourth, the duration of neurological symptoms from onset to the surgical interventions has not been evaluated in this study; however, it may affect the extent of CS pre- and postoperatively. Fifth, the extent of canal stenosis and spinal cord compression pre- and postoperatively evaluated by CT and/or MRI may have a significant impact on the degree of CS and surgical outcomes. The image analyses have not been conducted in this study; however, the analyses will be performed in future studies.
In conclusion, CS is associated with the neurological symptoms, disability, and QOL of patients with DCM both preoperatively and postoperatively. Posterior decompression surgery improved the extent of CS assessed by CSI. Additionally, posterior decompression surgery improved myelopathy-related symptoms and disability independent of the severity of preoperative CSI score, suggesting that it is an effective treatment for centrally sensitized patients with DCM.
Meanwhile, the postoperative surgical outcomes may be worse in centrally sensitized patients (CSI ≥40) than in the subclinical patients (CSI<30). The severity of CS evaluated by CSI score can be an auxiliary indicator for predicting surgical outcomes of patients with DCM following posterior decompression surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics were approved by the institutional review boards of Mie University Hospital (IRB reference number: H2020-027).
Informed Consent
Informed consent was obtained in the form of opt-out on the website.