
Abstract
Study Design
Survey.
Introduction
AO Spine Research Objectives and Common Data Elements for Degenerative Cervical Myelopathy (AO Spine RECODE-DCM) is an international initiative that aims to accelerate knowledge discovery and improve outcomes by developing a consensus framework for research. This includes defining the top research priorities, an index term and a minimum data set (core outcome set and core data elements set – core outcome set (COS)/core data elements (CDE)).
Objective
To describe how perspectives were gathered and report the detailed sampling characteristics.
Methods
A two-stage, electronic survey was used to gather and seek initial consensus. Perspectives were sought from spinal surgeons, other healthcare professionals and people with degenerative cervical myelopathy (DCM). Participants were allocated to one of two parallel streams: (1) priority setting or (2) minimum dataset. An email campaign was developed to advertise the survey to relevant global stakeholder individuals and organisations. People with DCM were recruited using the international DCM charity Myelopathy.org and its social media channels. A network of global partners was recruited to act as project ambassadors. Data from Google Analytics, MailChimp and Calibrum helped optimise survey dissemination.
Results
Survey engagement was high amongst the three stakeholder groups: 208 people with DCM, 389 spinal surgeons and 157 other healthcare professionals. Individuals from 76 different countries participated; the United States, United Kingdom and Canada were the most common countries of participants.
Conclusion
AO Spine RECODE-DCM recruited a diverse and sufficient number of participants for an international PSP and COS/CDE process. Whilst PSP and COS/CDE have been undertaken in other fields, to our knowledge, this is the first time they have been combined in one process.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is a syndrome of chronic symptomatic spinal cord compression secondary to a range of degenerative pathology in the cervical spine. 1 It is the most common cause of adult spinal cord impairment worldwide,1-3 has a large number of debilitating symptoms4,5 and amongst the worst quality of life of any chronic disease.6,7 Unfortunately, past translational research efforts have been hindered by lack of public awareness and lack of recognition by governmental and non-governmental funders of research. This has been compounded by the lack of standardisation of clinical assessment tools, a lack of preclinical research using translationally relevant models of DCM, a lack of high quality prospective clinical research studies with an excess reliance on small single-centre case series and inadequate synergy between researchers due to the lack of collaborative investigative initiatives.8-11
AO Spine Research Objectives and Common Data Elements for Degenerative Cervical Myelopathy (RECODE-DCM) is an international initiative designed to improve the efficiency of DCM research. 12 A number of objectives are encompassed within the project: the definition of the top DCM research priorities; establishment of a minimum dataset; and agreement of a single index term for the condition. Research priority definition follows James Lind Alliance Priority Setting Partnership (PSP) methodology. The minimum dataset incorporates two separate components, a core outcome set (COS) to include critical outcomes of the disease and a core data element (CDE) set, to include the additional data that should be reported to interpret outcomes. The initiative also aims to encourage international collaboration between all DCM stakeholders: clinicians, researchers, people living with DCM 13 and people supporting those living with DCM.
Degenerative cervical myelopathy stakeholders comprise a diverse group, most obviously people living with DCM, their supporters and spinal surgeons, who are the final common pathway in the management of DCM. 2 However, appropriate clinical suspicion by non-specialists and prompt referral on to specialists is fundamental to effective DCM care. 14 General practitioners, emergency department clinicians, neurologists, physiotherapists, osteopaths and a range of other healthcare professionals are therefore key DCM stakeholders. These latter perspectives have been underrepresented in DCM research to date, and whilst AO Spine and Myelopathy.org represent a large and international community of surgeons and people with DCM respectively, no such community of interested ‘other healthcare professionals’ exists. Achieving a broad and diverse perspective is fundamental to meeting the objectives of AO Spine RECODE-DCM.
The objective of this article is to describe the methods used to achieve a global perspective and the resultant sampling characteristics underpinning the recommendations of AO Spine RECODE-DCM.
Methods
Leadership Team
An international group of DCM stakeholders including spinal surgeons, other healthcare professionals, people with DCM and supporters of people with DCM comprise the AO Spine RECODE-DCM steering committee (SC), with responsibility for the project. A small group comprising an AO Spine Research Manager, a representative from the James Lind Alliance and three clinician-researchers comprise the study management group (MG), which is responsible for day-to-day operations. Global partners were recruited as an extended study group, forming an expert panel of advisors and collaborators. The global partners formed a network of local ambassadors throughout the world for study advertisement and dissemination.
Survey Development
Surveys were developed and piloted by the management group before steering committee piloting and discussion at a series of online meetings, to reach a final consensus.
The first part of the survey was designed to provide background to AO Spine RECODE-DCM, including an educational video and hyperlinks to the project website. The first question divided participants into three stakeholder groups: people with DCM and their supporters, spinal surgeons and other healthcare professionals. The first page of the survey was a registration form capturing basic participant data: age, sex, country of residence, full name, email address and informed consent. For healthcare professionals, the registration form also included questions capturing profession, speciality, job title, hospital/university affiliation, number of people with DCM treated each year, years working with people with DCM and desire to be involved in future DCM research initiatives.
The survey captured a number of additional data points from people with DCM: year of diagnosis, history of surgery, history of physiotherapy, additional DCM treatments, self-reported modified Japanese Orthopaedic Association (mJOA) score, self-rated pain score, previous involvement in DCM research and employment status. For supporters, the same data about the person with DCM were captured, in addition to supporter employment status and involvement of the supporter in previous DCM research.
Following completion of the registration page, participants were randomised to either the PSP or COS/CDE stream, before being presented with further information pertaining to the specific stream. These two processes were split to reduce the length of the survey for each participant but enable a single recruitment process.
For the PSP steam, participants were invited to enter as free text what they thought were the most important DCM research questions within each of the 4 categories of diagnosis, treatment, long-term care and follow-up and other. For a random subset of participants, an identical page followed in which a word-cloud appeared for each category. Word clouds were developed by piloting the PSP questions on approximately 60 individuals from all stakeholder groups. Participant entries from the first page were carried forward, allowing addition of further ideas stimulated by the word clouds.
Proposed outcomes presented to participants in the round 1 COS/CDE survey.
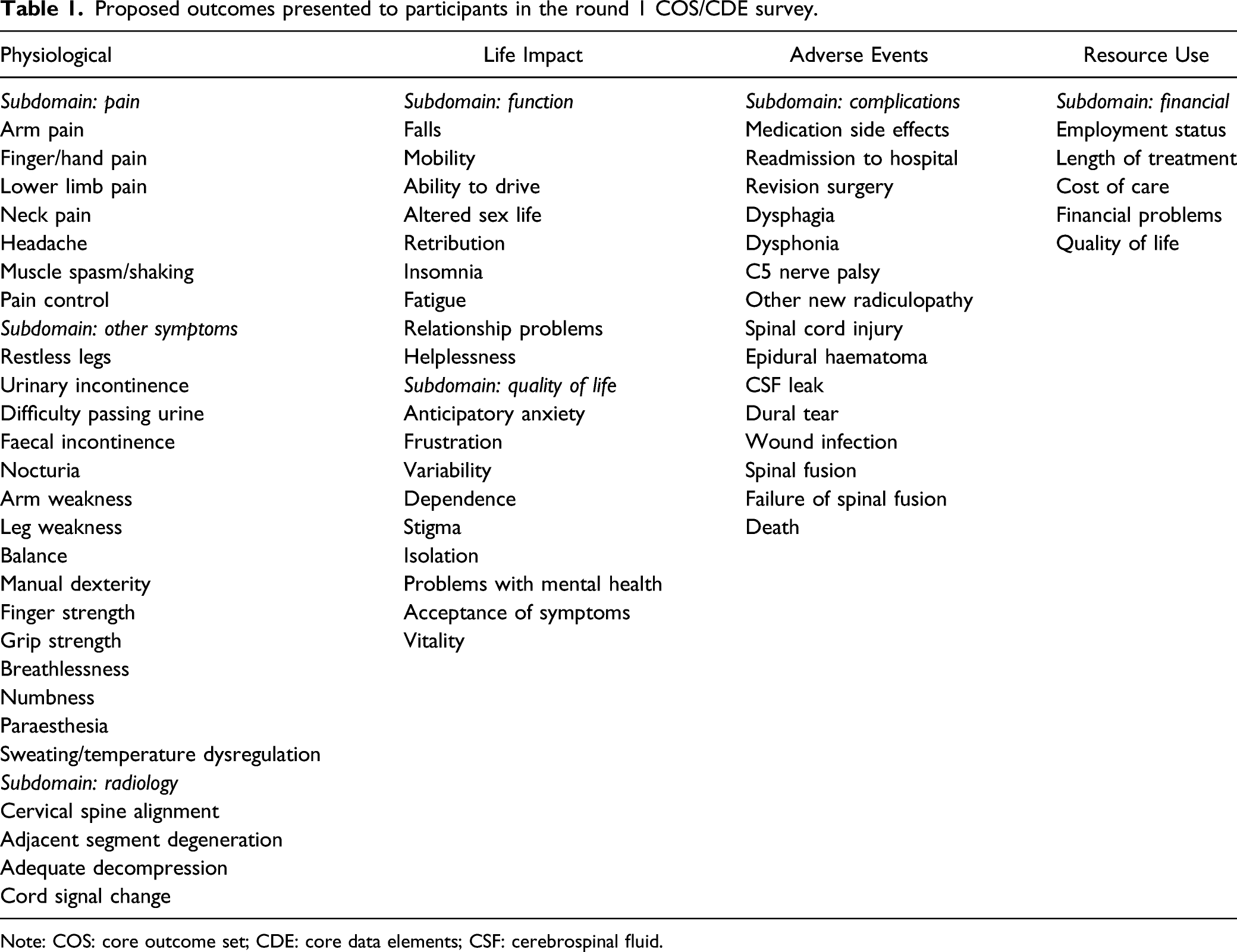
Note: COS: core outcome set; CDE: core data elements; CSF: cerebrospinal fluid.
An identical process was undertaken for the CDE survey. The potential core data elements presented to participants in the round 1 survey were mental health, obesity, diabetes, smoking status, other neurological diseases, other diseases, performance status, age, biological sex, ethnicity, medication, illness coping/resilience, welfare support, family history of DCM, length of symptoms, rate of progression, presence of myelopathy, number of previous surgeries, definition of DCM, levels of spinal cord compression, pathology causing spinal cord compression, presence of spinal cord signal change, amount of spinal cord compression, structured non-operative management, nerve root injection, operation type, operated levels, instrumentation, operative approach, intraoperative neurophysiology, post-operative collar and post-operative rehabilitation/physiotherapy.
Surveylet (Calibrum International, Virginia, US) was used for the round 1 survey. Both PSP and COS/CDE streams were built into the same software, with individuals randomised to one stream of the survey only. The SC agreed on a pre-defined sampling aim of 25% spinal surgeons, 25% other healthcare professionals and 50% people with DCM.
Survey Piloting
All members of the SC and MG completed the survey in a pilot-run. Technical issues such as typographical errors, problems with hyperlinks, video playback and navigation buttons within the survey were identified and corrected before a further round of piloting. Piloting was repeated until all SC and MG members approved the final survey.
Global Contact Directory
An international contact directory was compiled of DCM stakeholder individuals and organisations. A team of medical student researchers was recruited and trained to assist with directory development. All 53 countries with DCM research output over the past 20 years 8 were the initial focus of the directory. Students were each assigned several countries. Within each country, students compiled a list of names and contact email addresses for stakeholder individuals such as neurosurgeons, orthopaedic surgeons, neurologists, general practitioners and physiotherapists. Students also included contact details for stakeholder organisations such as medical charities, universities, medical colleges, hospitals and medical journals. The directory was compiled manually; no commercial datasets were acquired. In total, 1010 organisations and 3889 individuals were included. An estimated 90% of individuals in the directory were spinal or neurological surgeons. A small number of organisations agreed to disseminate the survey to their members.
Email Campaign
An email campaign targeted at stakeholders in the contact directory was executed using MailChimp (Georgia, US). Emails provided a concise introduction to AO Spine RECODE-DCM and explained that we had identified the individual as someone who may be interested in participating. Email style was alternated between emails with colourful infographics and an embedded introductory video and emails consisting of simple plain text. Real-time analytic data were utilised to optimise email advertisements. Unique emails were sent to individuals and organisations. Recipients were offered the opportunity to opt-out via a link in every email. All emails included a contact email address. Stakeholders who did not wish to participate contacted our research manager requesting to be removed from subsequent emails.
Interim analysis of respondent demographics identified underrepresentation of the other healthcare professional group. An additional global contact directory consisting of 1511 other healthcare professional stakeholders was therefore developed.
Dissemination and Recruitment
A total of 5 emails were sent to the global contact directory, each separated by approximately 1 week; 3 emails were sent to the directory of organisations, each separated by approximately 2 weeks; 2 emails were sent to the directory of other healthcare professionals, separated by approximately 2 months. These mailing intervals were selected based on email performance data. The aim was to maximise response rate whilst avoiding overwhelming respondents.
Myelopathy.org is an international DCM charity with an online community of thousands of people with DCM. The charity website and its social media channels were utilised to target people with DCM and their supporters. Social media posts were utilised to solicit stakeholder views in survey design, including word cloud development, and to recruit people with DCM to complete the survey. AO Spine is the largest international community of spinal healthcare professionals. The organisation was utilised to advertise the study via its website and social media outlets. AO Spine RECODE-DCM also has a designated page on the AO Spine website (https://aospine.aofoundation.org/research/recode-dcm). Advertisements were also published in newsletters and online by organisations, including the World Federation of Neurosurgical Societies and the European Association of Neurosurgical Societies.
A study website was established (https://recode-dcm.com/). The website hosts background information about DCM and the AO Spine RECODE-DCM project, regular progress updates, study protocols, participant information sheets, privacy, consent and GDPR statements. It also formed a key method of dissemination and recruitment.
Analytics
Urchin Tracking Module (UTM) survey links were sent to each organisation. This enabled each organisation to receive a unique hyperlink, which was tracked in AO Spine RECODE-DCM Google Analytics account. UTMs were also utilised for each dissemination strategy targeted at individuals. UTMs, therefore, enabled evaluation of the study recruitment strategies.
Results
Engagement
In total, 208 people or supporters of people with DCM, 389 spinal surgeons and 157 other healthcare professionals participated.
Definition of Survey Endpoints
For the PSP, the survey endpoint was defined when saturation of uncertainties was achieved. This was identified by analysis of submitted uncertainties until no new uncertainties had been suggested in the preceding month. The survey was terminated at saturation, despite not meeting pre-defined sampling criteria. The PSP survey was live for 12 weeks, with PSP/COS randomisation paused for the final 6 weeks to direct all participants into the PSP stream.
The COS/CDE survey responses involved ranking a list of possible outcomes; hence, the concept of saturation did not apply. The survey was open for 9 months in total, with all participants initially randomised to the PSP or COS/CDE streams for 6 weeks, all directed to the PSP for 6 weeks period, before all being directed to the COS/CDE stream after the PSP closed in August 2019. The SC agreed to close the COS/CDE survey on February 20, 2020 as responses had fallen to negligible levels.
Sampling Characteristics
Survey Participant Demographics.
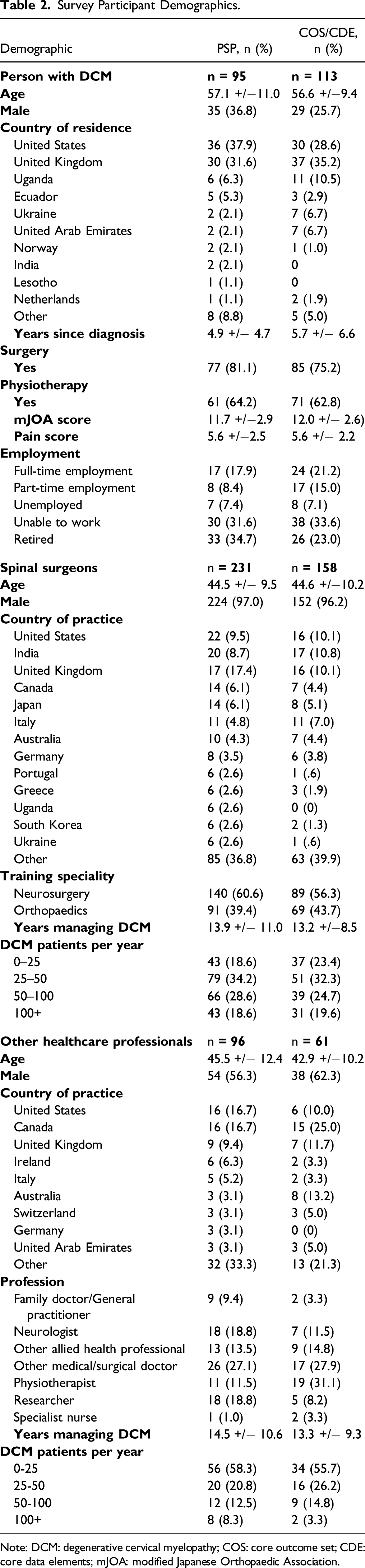
Note: DCM: degenerative cervical myelopathy; COS: core outcome set; CDE: core data elements; mJOA: modified Japanese Orthopaedic Association.
Global Reach
Individuals from 76 countries from 6 continents participated in the round 1 surveys, with the United Kingdom and United States the largest contributors (Figure 1). AO Spine RECODE-DCM participants. The darker the colour, the greater the number of participants from that country. Countries shaded in white had zero participants.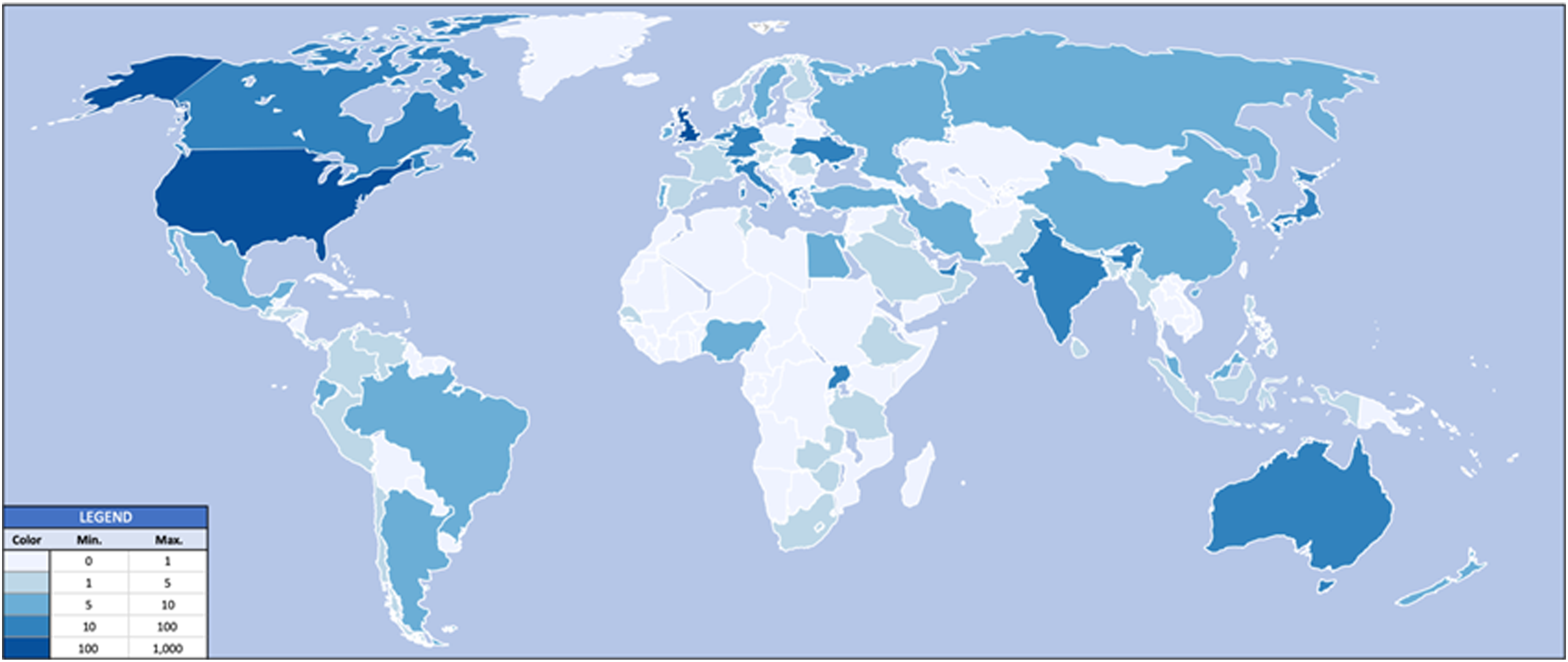
Dissemination Strategies
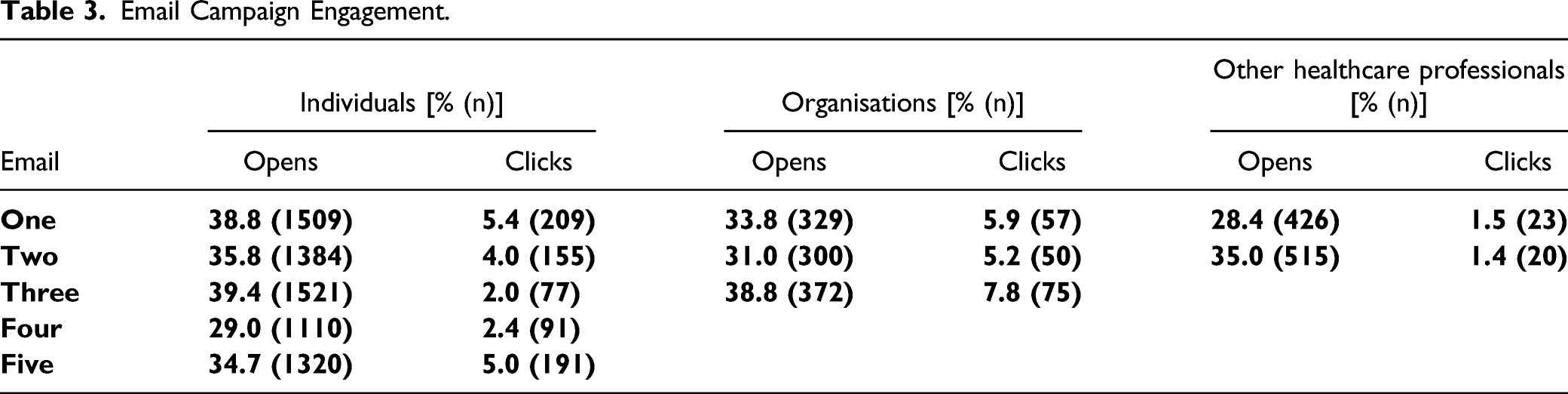
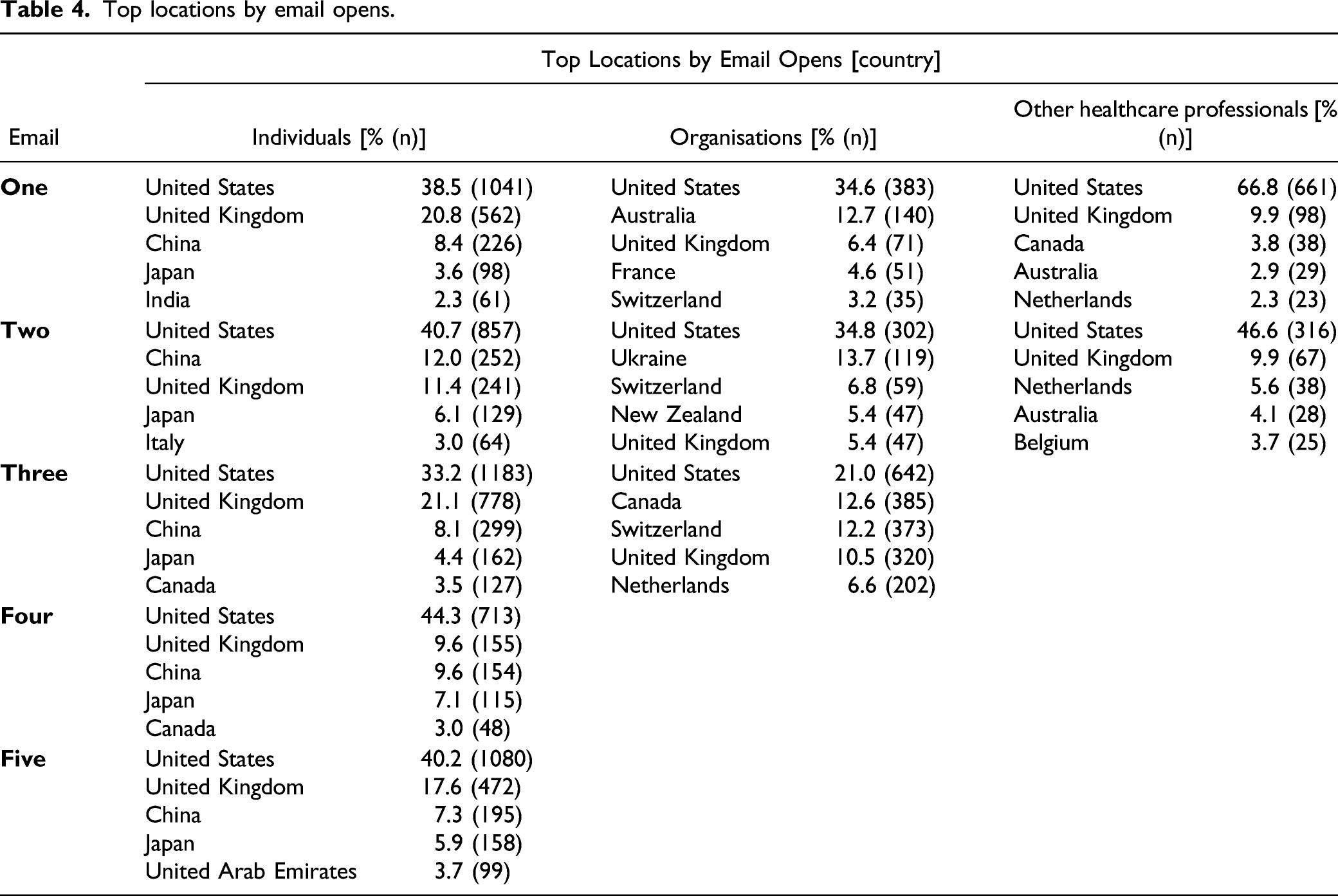
Email Campaign Engagement.
Top locations by email opens.
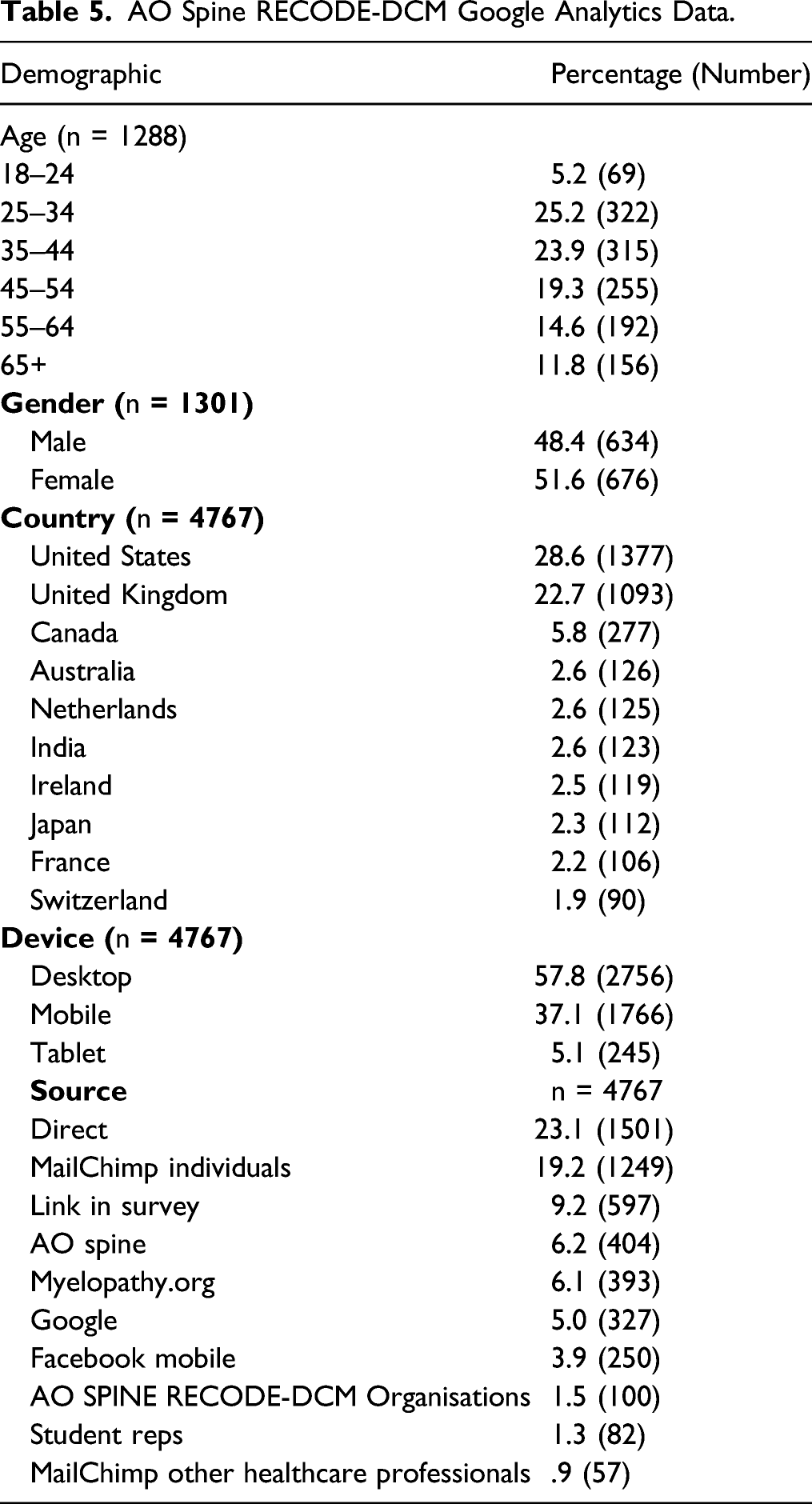
Google Analytics
AO Spine RECODE-DCM Google Analytics Data.
Discussion
Although challenging to implement, the AO Spine RECODE-DCM survey methodology has successfully engaged a global multi-disciplinary cohort of DCM stakeholders, with representation of surgeons, non-surgical healthcare professionals and people with or supporting those with DCM.
Key Demographics
The mean age of people with DCM who participated was in the mid-late 50s, similar to international trial cohorts,19,20 providing reassurance of a representative sample. However, the gender composition was around 70% female, in contrast to male-dominance in trial data, but consistent with previous online DCM surveys, where it has been postulated that this may be due to greater engagement of females with online health initiatives.7,21 The mean age of around 45 for spinal surgeons suggests a large number of experienced consultant/attending surgeons were included; the gender composition of 96% male for the spinal surgeon group roughly matches the gender composition of the speciality.22-25 As expected, although spinal surgeons and other healthcare professionals report similar years of managing people with DCM, the modal number of patients managed per year was much higher for spinal surgeons than other healthcare professionals, perhaps reflecting the predominance of surgeons in the management of DCM 2 and heterogeneity in non-surgical service provision for people with DCM. 26
Large Representation of Surgeons
The SC had agreed a target representation of 25% surgeons, 25% other healthcare professionals and 50% people with DCM and their supporters. In reality, a much greater representation of surgeons of 51.6% was achieved. Targeted efforts directed at non-surgical stakeholder groups were unable to fully redress this. This is not surprising given that DCM is a condition typically managed by surgeons19,20,27 and surgery has dominated the DCM research literature over the past 20 years. 8 Nonetheless, other healthcare professionals and people with DCM and their supporters were represented, making up 27.6% and 20.8% of participants, respectively. Given the desired representation of stakeholders amongst the MG and SC and evidence of information saturation within the survey, this was considered sufficient.
Challenges in Engaging Non-surgical Healthcare Professionals
The difficulty in recruiting healthcare professionals other than spinal surgeons was anticipated. Firstly, this represents a diverse group of professionals, without a single representative body, but also aligns with a poor awareness of DCM linked to significant delays in diagnosis.2,28-30 DCM is currently poorly represented in medical curricula 31 and is referred to by a wide range of different terms,32,33 and the vast majority of research over the past 20 years has been conducted by surgeons. 8
Raising awareness was subsequently identified as the number one research priority for DCM by AO Spine RECODE-DCM. 34 Retaining and growing these perspectives is likely to remain an integral part of supporting progress in DCM. It is hoped therefore that AO Spine RECODE-DCM represents a foundation from which to build upon.
Value of Research Databases
The central tenet of RECODE-DCM is the need for greater standardisation and collaboration in DCM research. 35 A global contact database of all DCM stakeholders may be an effective method of communication. This is born out in our database forming the single most effective source of website traffic, after direct visitors. Our database was developed by identifying individuals and organisations whom we had reason to believe were DCM stakeholders. The success of this initiative is reflected in our email, open and click rates being significantly higher than the MailChimp industry average. Whilst a small number of individuals unsubscribed or contacted our research manager to explain they could not participate for various reasons, we experienced no major complaints from individuals who felt they were not stakeholders. In the long term, an open, online opt-in database of DCM stakeholders will help improve sensitivity and inclusiveness of stakeholder recruitment in future work and aid international collaboration.
Limitations and Reflections
Participant randomisation to PSP and COS/CDE was probably unhelpful. Due to the recruitment rates and an earlier date of the PSP consensus meeting necessitating an earlier end date of the PSP survey, the COS/CDE was temporarily closed to focus on the PSP recruitment. Further participants who had completed the COS/CDE were subsequently invited to submit research uncertainties. Whilst the decision to split these streams was taken to reduce participant attrition, it appeared that the difficulty in engaging a large and diverse community meant that this would have been better kept as one survey, or as sequential surveys.
Organisations were also harder to engage than individuals. Only 2% (100/4767) of AO Spine RECODE-DCM website traffic was directed from third parties. Willingness to assist was often significantly delayed by the necessity for approval by internal reviews and authorisation processes. Therefore, developing relationships and contacting organisations well in advance is an important lesson for future projects.
Developing a global contact directory of all possible stakeholders was an overwhelming task. Focusing our contact directory on the 53 countries with any DCM research output over the past 20 years 8 risked excluding new or under-represented stakeholder voices. Nonetheless, we are reassured by analytics data showing that individuals from 105 different countries visited the project website, with individuals from 76 countries participating. This suggests engagement from individuals not previously involved in DCM research – a key objective of the inclusive, collaborative ethos of RECODE-DCM.
Website traffic was significantly higher than total survey responses, with 4767 website users delivering 754 complete survey responses. Engagement of those stakeholders who visited the website but did not participate in the survey, especially those from countries not previously involved in DCM research, is a focus for future work in developing the AO Spine RECODE-DCM network. The concordance of analytics data from the project website with the final survey data, for example, the UK, US and Canada being the common countries in both datasets, suggests that our analytics data is a good predictor of our survey population.
Conclusions
In a short space of time, AO Spine RECODE-DCM recruited a diverse range of stakeholders, sufficient to inform the PSP and COS/CDE process. Whilst PSP and COS/CDE have been undertaken in other fields, to our knowledge this is the first time they have been combined in one process. The project has laid foundations for an ongoing global, multidisciplinary DCM research collaborative.
Footnotes
Declaration of Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research priorities were organised and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international Spinal Cord Injury experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organisation. Study support was provided directly through the AO Spine Research Department.AM is funded by a National Institute for Health Research (NIHR) Clinician Scientists Fellowship award (NIHR CS-2017-17-010) and further supported by the NIHR Biomedical Research Centre (BRC) at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol (BRC-1215-20011). MRNK is supported by the National Institute for Health Research (NIHR) Brain Injury MedTech Co-operative based at Cambridge University Hospitals NHS Foundation Trust and University of Cambridge, and BMD a NIHR Clinical Doctoral Research Fellowship. The views expressed in this publication are those of the authors and not necessarily those of the NIHR.