
Abstract
Study Design
Systematic Review and Meta-Analyses.
Objective
To assess the 30- and 90-day readmission rates after a traumatic spinal cord injury (SCI).
Methods
A systematic search of MEDLINE and Embase was performed. The period was from inception to June 2022, with no language restrictions. All studies investigating the 30- and/or 90-day readmission rate following traumatic SCI were included. A random-effects model to combine effect sizes in our meta-analysis was applied.
Results
Seven out of 2959 reports met eligibility. The mean age of the patients was 50.2 ± 19.9, with a male-to-female ratio of 2.4:1. The most common traumatic SCI was cervical injury (55.3%). The meta-analysis model revealed a 30-day readmission rate of 14.2% after traumatic SCI, with heterogeneity in the studies. The 90-day readmission rate was 35.7%, with homogeneity in the studies. The meta-regression analysis found significant positive associations between cervical and thoracolumbar injuries and patient age and the 30-day readmission rate, while male sex demonstrated a negative association with the 30-day readmission rate. The 30-day readmission rate following index admission was 13.1% and the 30-day readmission rate after rehabilitation facilities was 15.8%. The study found that the 30-day readmission rate in the USA was 14.0%.
Conclusions
There is no doubt that readmission is an adverse health outcome. The outcome is also complex and multifaceted, which makes it difficult to predict. Injury level is 1 of the predictors that affect readmission, making it essential to consider factors during discharge planning for high-risk people to reduce 30-day readmission rates.
Introduction
Spinal cord injury (SCI), particularly cervical spine trauma, can lead to serious adverse effects on physical and social functions, greatly impairing quality of life measures. 1 Studies have shown that 2 to 6 percent of blunt trauma victims sustain spinal column and/or spinal cord injuries. 2 Apart from mortality, the relative morbidity associated with acute traumatic SCI is also high. Many survivors require repeated admissions due to adverse events or morbidities from their initial injury. Many patients require further rehabilitation to maximize neurologic recovery and functionality after the first admission. These readmissions and rehabilitations are associated with a considerable financial burden for the person and the healthcare system. 3
Early readmission after spinal surgery is increasingly used as a quality-of-care measure to evaluate performance. Generally, spinal literature reports 30-day readmission rates between 2.5% for anterior cervical discectomy and fusion and 14% for metastatic and primary spine tumors. 4 Various factors have been attributed to readmission rates, including age, gender, and comorbidities—hypertension, diabetes mellitus, and coronary artery disease. 5
In this study, our main objective is to determine the 30-day and 90-day readmission rates following traumatic SCI based on the collected studies and the 30-day readmission rate based on country, rehabilitation facilities, and index admission.
Material and Methods
An electronic search of published articles was conducted in MEDLINE/PubMed and EMBASE for published articles and updated from inception until June 2022 using appropriate MeSH term and Emtree such as “readmission”, “spinal cord injuries”, “paraplegia”, “tetraplegia” without language restrictions. All the search strategy are presented in Table A1. The reference lists of each article were also individually searched to find further relevant articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines were utilized. 6
Inclusion and Exclusion Criteria
The main objective of our study was to determine the 30- and 90-day readmission rates following traumatic SCI, and secondary outcomes were subgroup analyses based on the country and 2 distinctive categories: 1. Index admission: acute care from the time of hospitalization and discharge to any location other than transfer to acute care in another hospital; 2. Inpatient rehabilitation: people who were discharged from rehabilitation facilities. So, we included all studies that reported the 30- and/or 90-day readmission rate following traumatic SCI without any language or geographical restriction.
Exclusion Criteria
• Studies report readmission rates following scoliosis, fractures, deformities, chronic illness, and traumatic brain injury without concomitant traumatic SCI. • Studies exclusively involve pediatrics—younger than 16 years old.
Selection Method and Data Extraction
After an initial search and the removal of duplicates, 4 reviewers (MH, MRJ, AS, and SDA) were separated into 2 groups. For data extraction, 2 reviewers (MH and SDA) independently screened the full texts of selected papers. Any discrepancy regarding the eligibility of studies was solved by the decision of the third author (HM). The data was placed into predefined extraction sheets. The specific fields included: title, first author’s name, year of publication, sample size, location and setting, design, and participants’ characteristics, including the injury levels and the 30- and 90-day readmission rates.
Risk of Bias Assessment
We assessed the methodological quality of each study using the National Institutes of Health’s (NIH) quality assessment tool. 7 According to the score, bias likelihood, and completeness of reporting, the studies were graded as good (A), fair (B), or poor (C). Each outcome was graded separately within each study. We extracted data from eligible papers, grouped them by comparator type, and conducted the analysis. In addition to measuring the quality of the methodology, we considered the consistency of results across studies, the directness of the evidence, as well as other factors such as the degree of imprecision and sparsity. The tables for each article are available in Table A2.
Statistical Analysis
The meta-analyses were conducted by Comprehensive Meta-Analysis Software V.2 (Biostat Inc., New Jersey, USA). The meta-analysis was reported as an event rate with a 95% confidence interval (CI). Due to study heterogeneity, the meta-analysis used a random-effects model. This model accounted for both within-study and between-study variance, making it better for varied patient populations and treatment settings. This method predicted 30- and 90-day readmission rates across hospital settings and patient demographics. Heterogeneity was evaluated using the I2 statistic and Q-value test. The I2 statistic measures the percentage of variation in study results owing to heterogeneity, rather than chance, indicating inconsistency. In each analysis, if I2 was more than 50% or its P-value was less than 0.1, our group considered the data heterogeneous.
Funnel plots and Begg’s and Egger’s tests were used to assess publication bias. Funnel plots show possible bias, and statistical tests determine if the plot has asymmetry, which may imply publishing bias. These procedures ensure meta-analysis results are trustworthy and not affected by selective publication of research. A meta-regression analysis examined patient factors like age, sex, and injury type and 30-day readmission rates. Meta-regression explores how specific factors affect outcomes and helps explain subgroup readmission rates. Finally, subgroup studies compared readmission rates for index admissions and rehabilitation facility discharges. These analyses sought to identify differences in readmission reasons between the 2 groups due to care settings and patient requirements. This distinction is crucial to understanding how healthcare settings affect readmission rates and outcomes. Due to the small number of studies in the 90-day readmission rate, subgroup analysis and meta-regression were performed only for the 30-day readmission rate.
Results
Through the initial database searches and subsequent additional references, 2959 publications were retrieved. After removing duplicate titles and abstracts, 2660 articles went through titles and abstracts with detailed evaluation. This resulted in the exclusion of an additional 2635 articles. After reviewing the entire manuscript of the remaining articles in detail, all met our inclusion criteria. Thus, 7 papers8-14 met all of the eligibility criteria and were included in the meta-analysis (Figure 1). Of these, 6 were retrospective cohort studies,9-14 and 1 was a retrospective cross-sectional
8
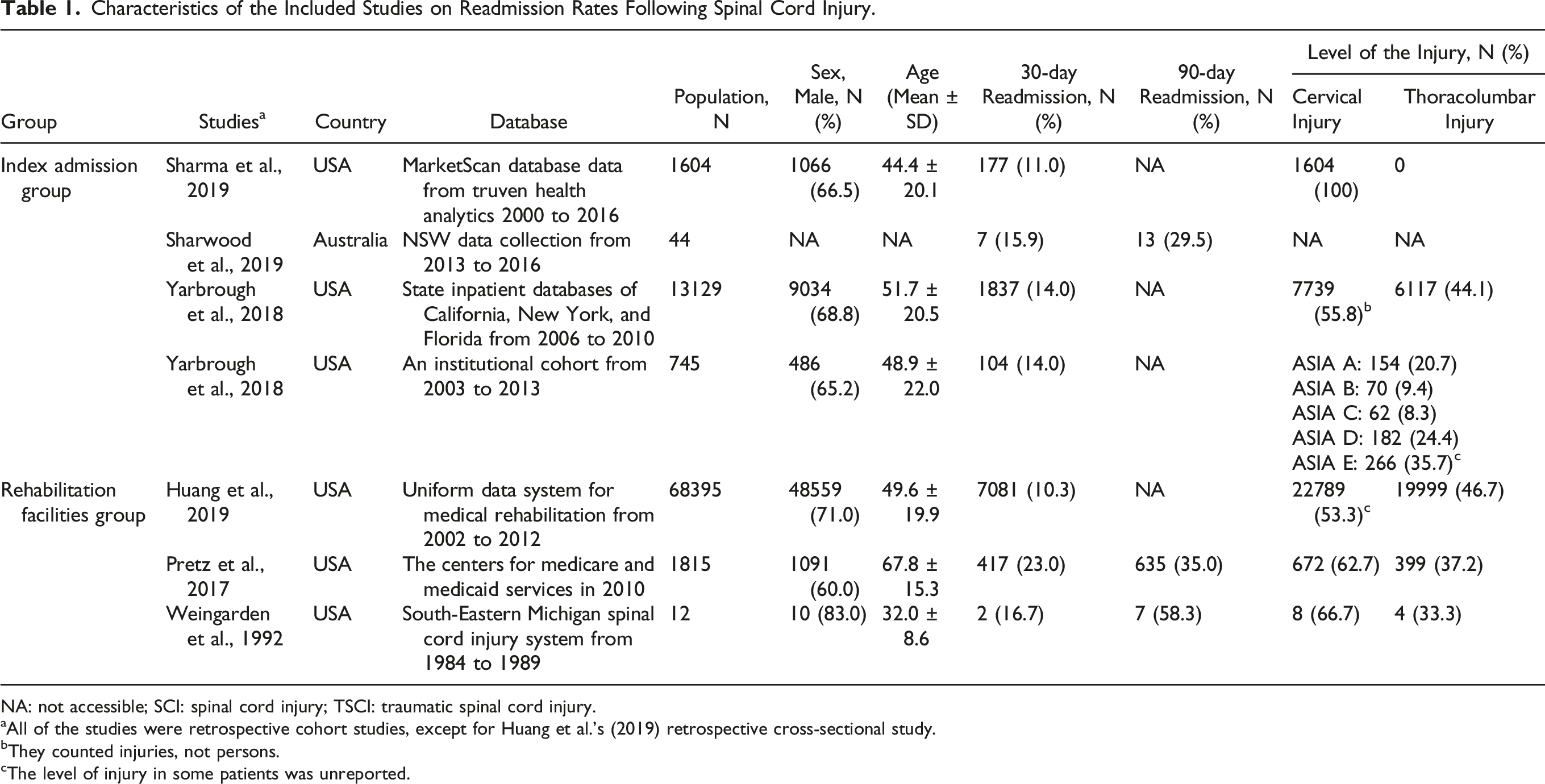
study. The sample sizes of the studies ranged from 12 to 68,395 patients, with a male-to-female ratio of 2.4:1 and an age mean ± standard deviation based on 6 studies of 50.2 ± 19.9.8-10,12-14 The most common traumatic SCI was cervical injury (55.3%), based on 4 studies that reported the level of SCI.8-10,12,13 The main characteristic of all included studies is summarized in Table 1. Flow diagram illustrating the PRISMA 2020 guidelines for systematic review and meta-analysis of the readmission rate of traumatic spinal cord injuries. Characteristics of the Included Studies on Readmission Rates Following Spinal Cord Injury. NA: not accessible; SCI: spinal cord injury; TSCI: traumatic spinal cord injury. aAll of the studies were retrospective cohort studies, except for Huang et al.'s (2019) retrospective cross-sectional study. bThey counted injuries, not persons. cThe level of injury in some patients was unreported.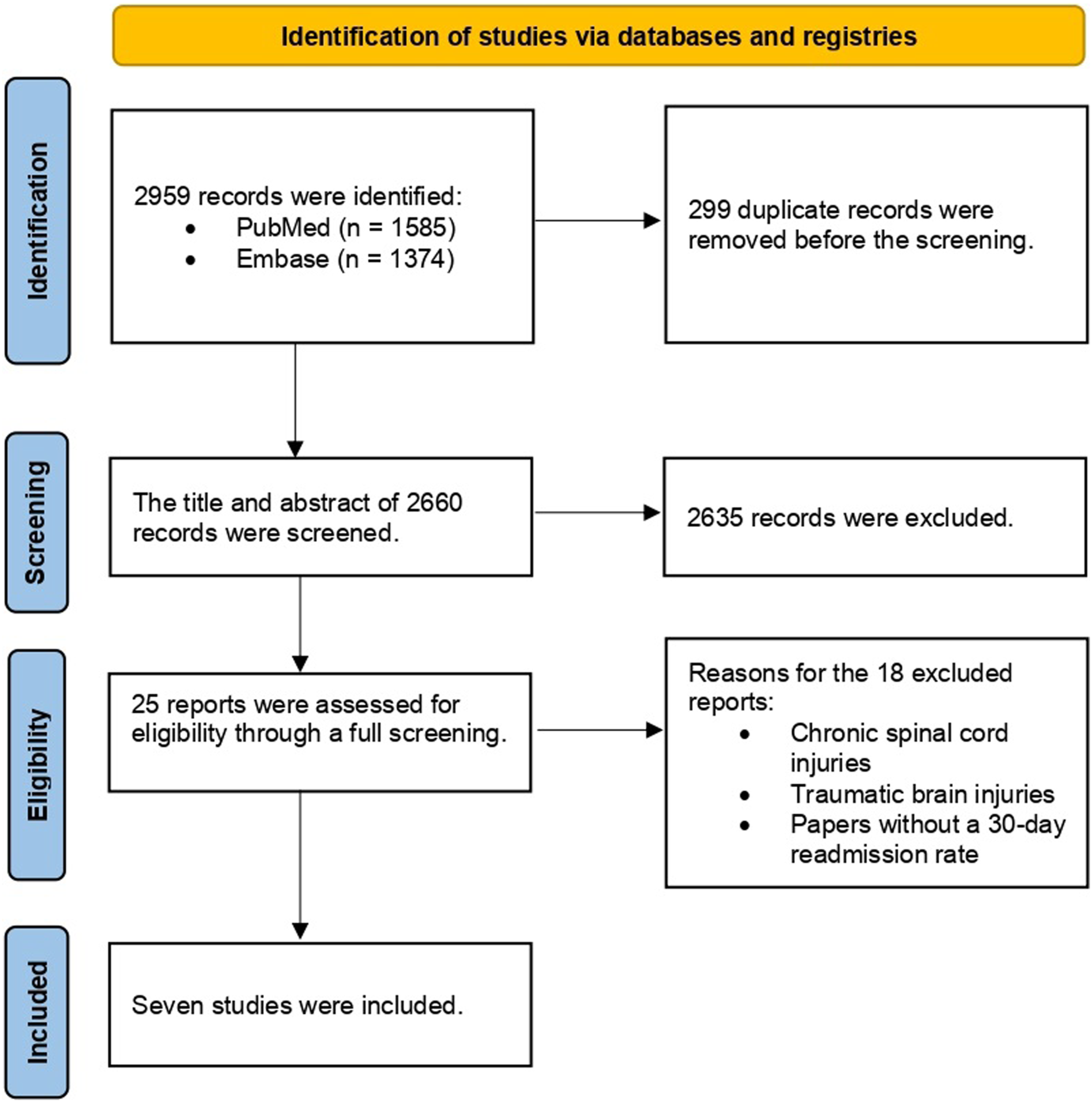
Meta-Analysis, Sensitivity Analysis, and Meta-Regression
The random-effect meta-analysis model revealed the 30-day readmission rate after traumatic SCI was 14.2% (95% CI, 11.1-18.0; P < 0.001), and the studies showed heterogeneity (I2 = 98.5%) (Figure 2). In the sensitivity analysis after excluding Pretz et al., 2017 study,
9
the 30-day readmission rate got lower as 12.5% (95% CI, 10.2-15.1; P < 0.001), and after excluding Huang et al., 2019 study,
8
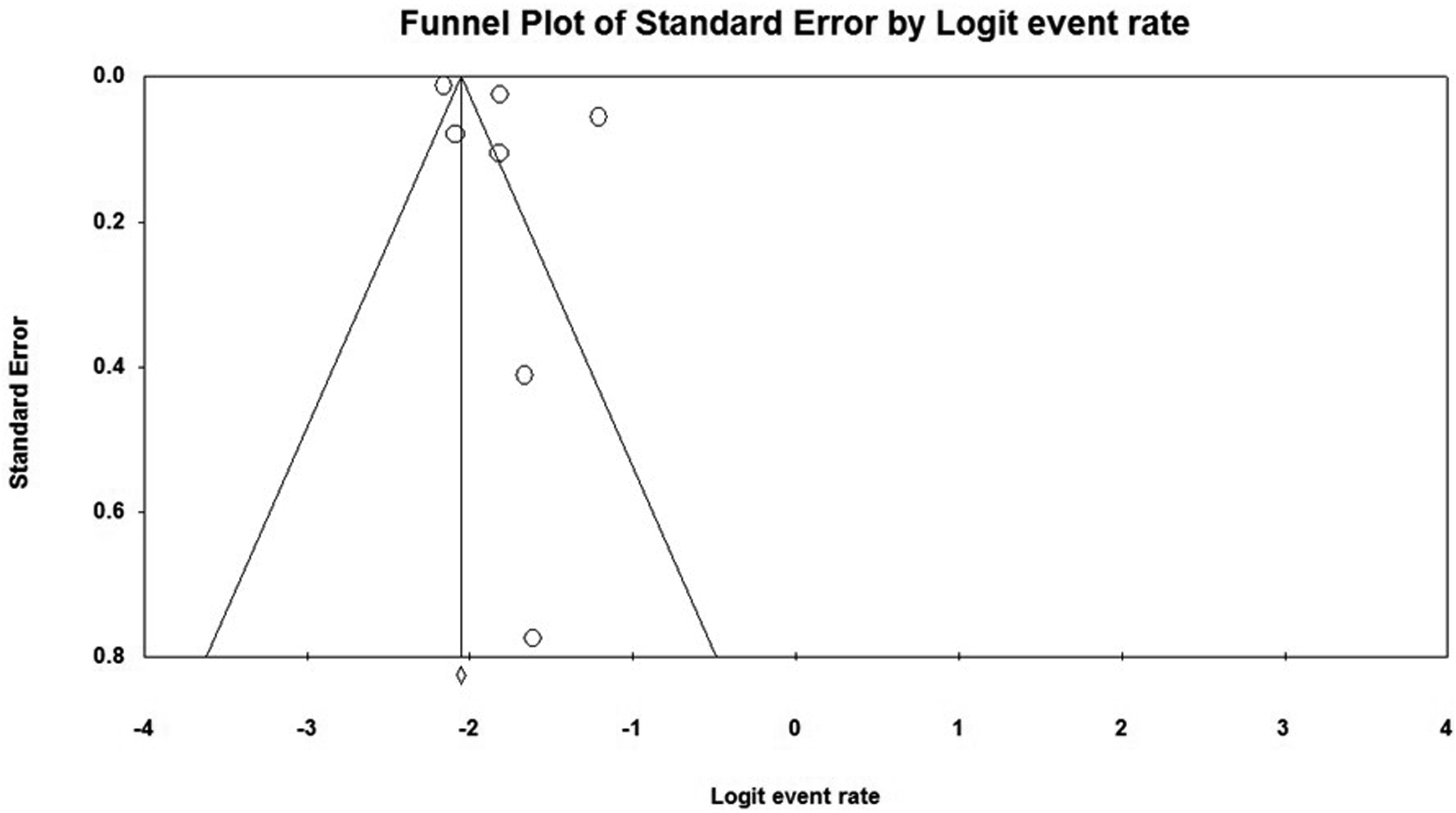
the 30-day readmission rate turned to a higher rate as 15.2% (95% CI, 11.5-19.9; P < 0.001). In the publication bias assessment, it was revealed that the studies did not have any publication bias (P = 0.26). Figure 3 presents the funnel plot of the 30-day readmission rate model. The meta-analysis of 30-day readmission rates across studies on traumatic spinal cord injury. The funnel plot depicting the distribution of the 30-day readmission rate across studies on traumatic spinal cord injury.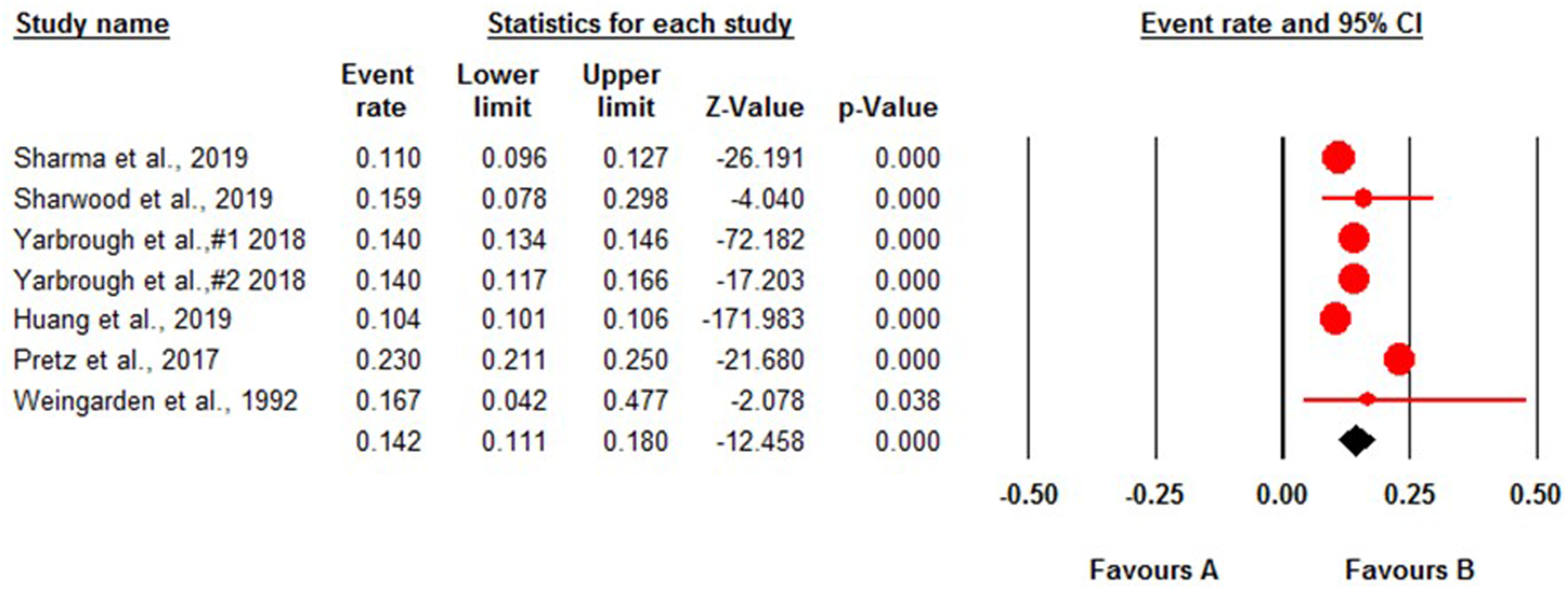
The meta-analysis showed the 90-day readmission rate after traumatic SCI was 35.7% (95% CI, 27.6-44.8; P = 0.002) and studies were homogenous (I2 = 38.2%) (Figure 4) and in the sensitivity analysis after excluding Weingarden et al., 1992,
12
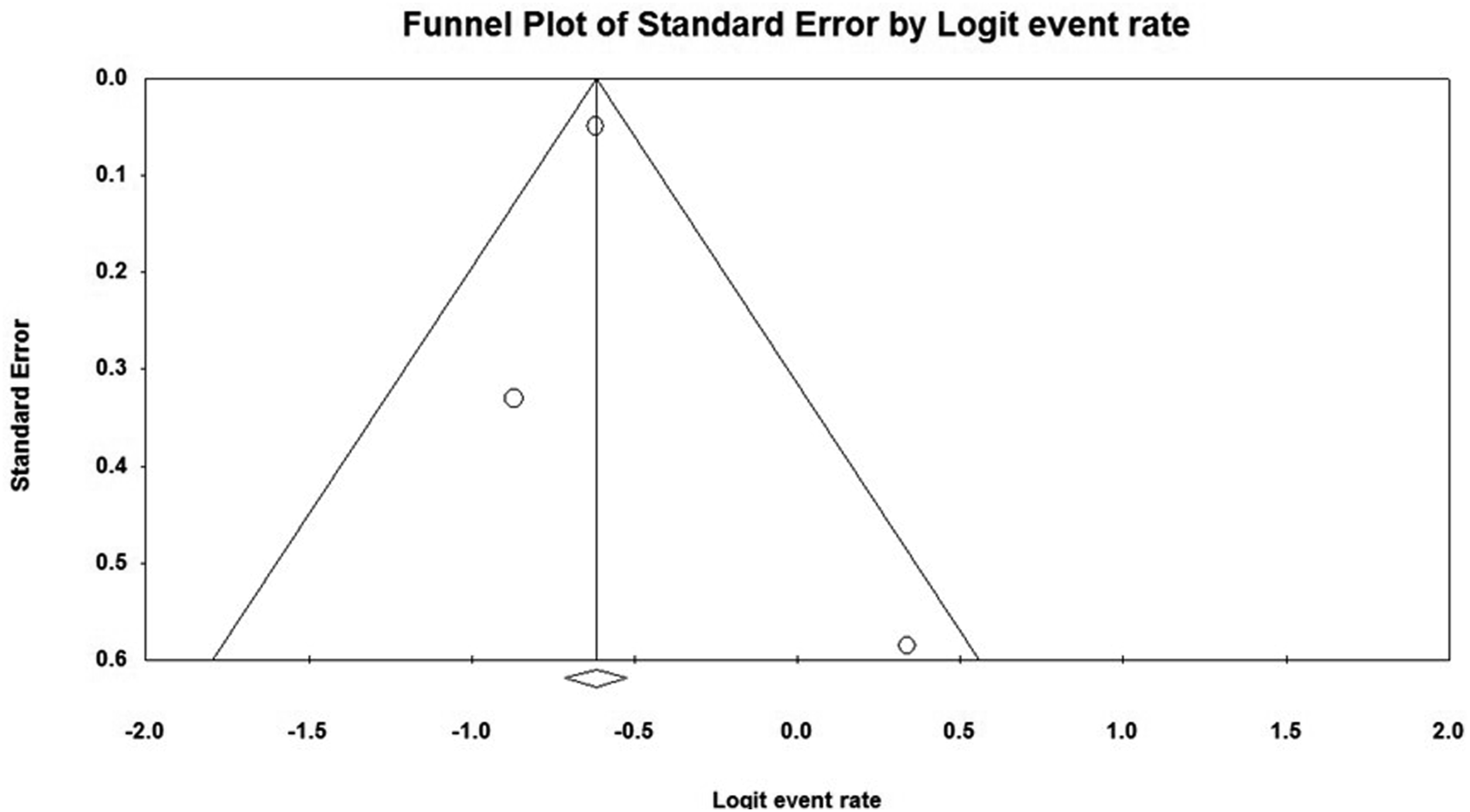
the 90-day readmission rate turned to 34.9% (95% CI, 32.7-37.1; P < 0.001); however, excluding the other 2 studies was not significant. The Egger’s test showed no publication bias (P = 0.72) and the funnel plot was symmetric (Figure 5). The meta-analysis of the 90-day readmission rate across studies on traumatic spinal cord injury. The funnel plot depicting the distribution of the 90-day readmission rate across studies on traumatic spinal cord injury.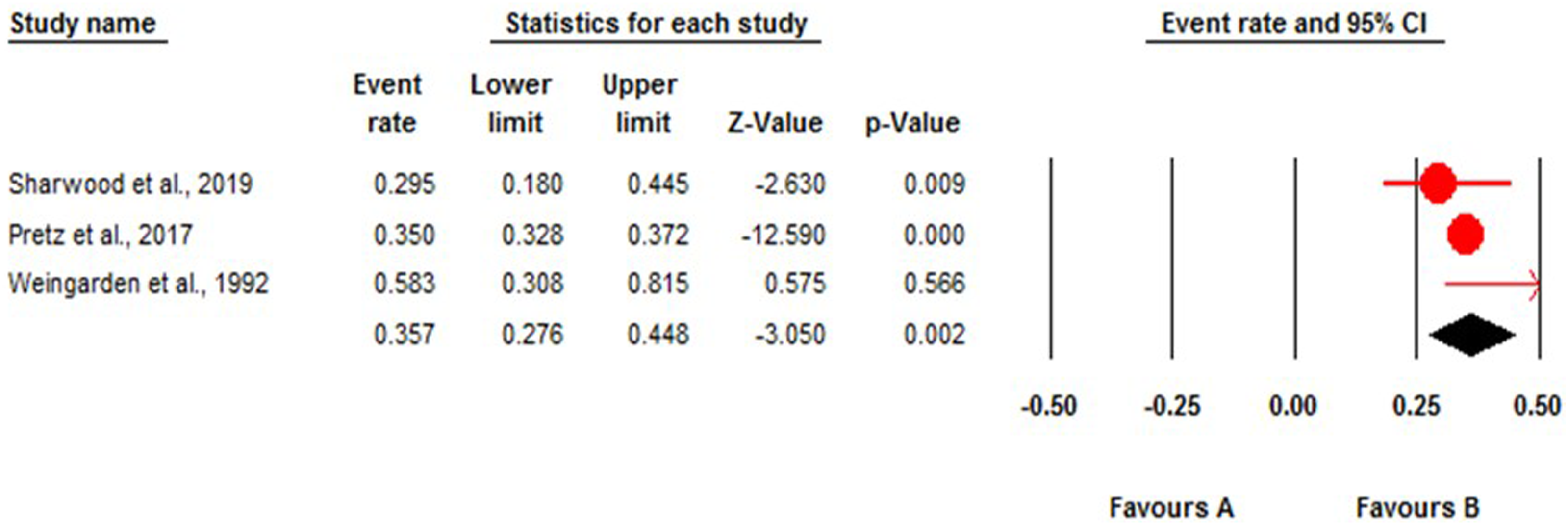
The meta-regression analysis revealed significant associations between various factors such as age, sex, and the level of injury, with the rate of 30-day readmission. Specifically, cervical injury, thoracolumbar injury, and patient age showed positive associations, while male sex demonstrated a negative association. For each unit increase in the rate of cervical injury, there was an increase in the 30-day readmission rate of 0.74% (95% CI, 0.57-0.90; P < 0.001). Similarly, a unit increase in thoracolumbar injury was associated with a 0.82% (95% CI, 0.57-1.10; P < 0.001) rise in the 30-day readmission rate. Age also exhibited a significant impact, with a 5.2% (95% CI, 4.6-5.8; P < 0.001) increase in the 30-day readmission rate for every year increase in age. Conversely, male patients experienced a decrease in the 30-day readmission rate with an increase in male percentage, showing a reduction of −8.7% (95% CI, −9.7, −7.8; P < 0.001) (Figure 6). The meta-regression between cervical and thoracolumbar injuries, age, and sex (male) and the 30-day readmission rate across studies on traumatic spinal cord injury.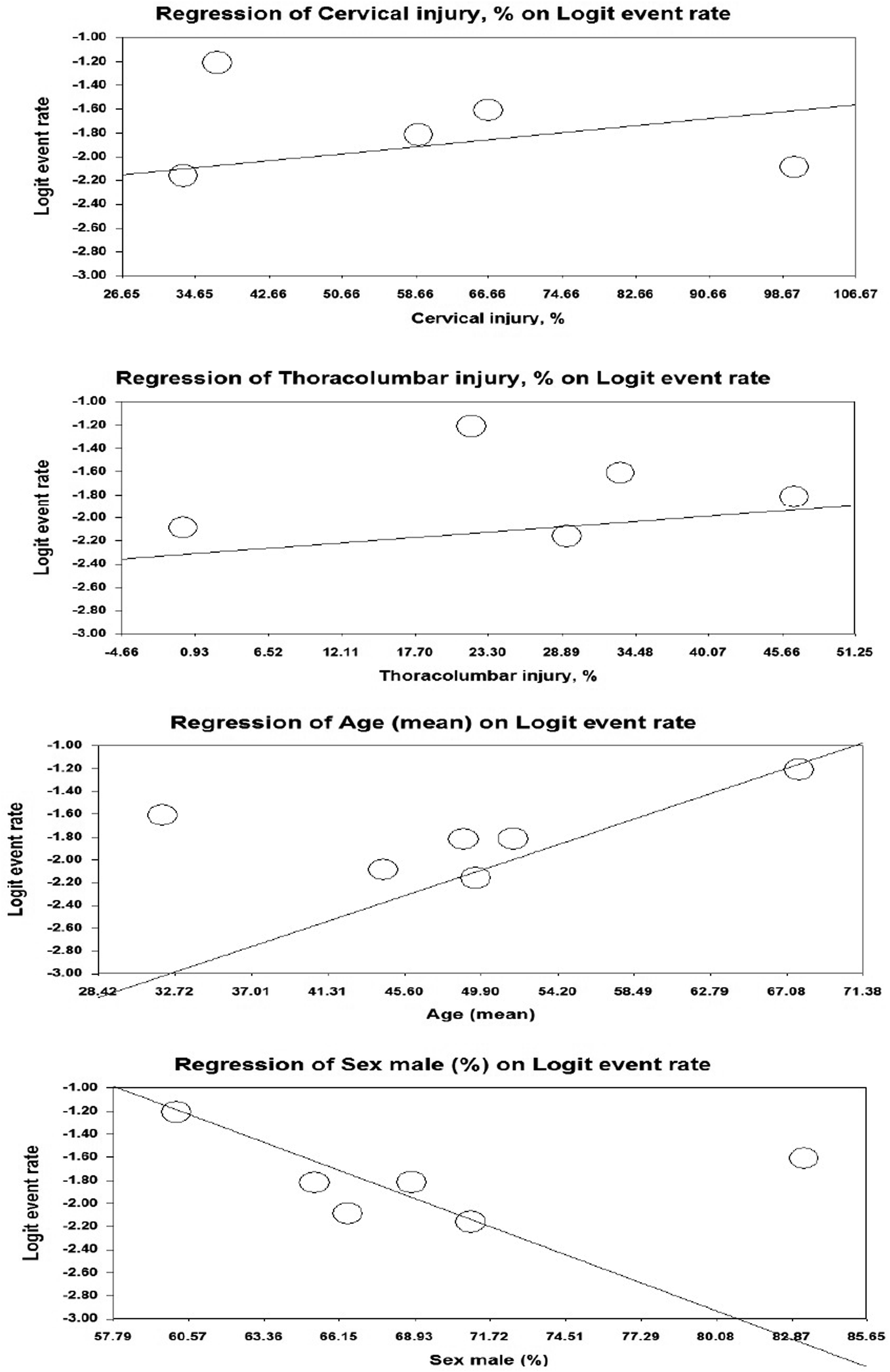
Subgroup Analysis Based on Index Admission, Rehabilitation Facilities, and Country
The Subgroup Analysis for Studies on 30-Day Readmission Rate Following Traumatic Spinal Cord Injury.
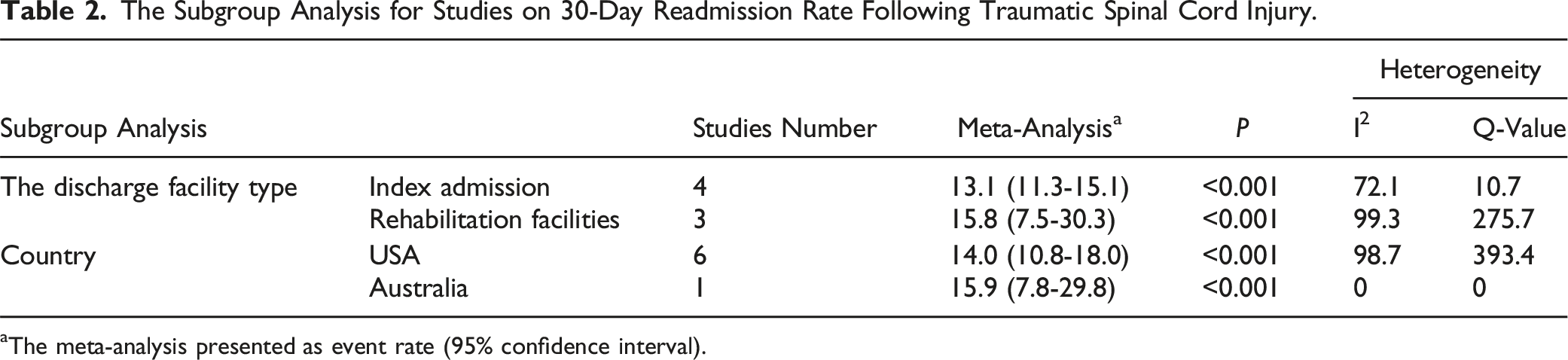
aThe meta-analysis presented as event rate (95% confidence interval).
Discussion
The early readmission rate during spine surgery is increasingly used as a metric for quality-of-care and performance evaluation. The readmission rate attempts to define quality care as a readmission that could potentially be a lost opportunity to diagnose or treat a medical illness. Additionally, by reducing readmissions, there is great potential to reduce healthcare costs. 15 The Medicare Payment Advisory Committee has reported that hospital readmissions are accountable for about $15 billion. 16
Unfortunately, the management, improvement, and prevention of chronic and secondary healthcare conditions associated with acute injuries are extremely challenging. 17 To assess outcome trajectories, a meta-analysis of hospital readmission risk over the 30 days following discharge from inpatient rehabilitation and index admission was performed. This systematic review included 8 articles. The majority were conducted in the USA. The current research has multiple variations in methodology, discrepancies in readmission rate, and predictors, but among all these differences, the 30-day readmission rate is still substantial.
The observed readmission rate among individuals after initial inpatient treatment for acute traumatic SCI was 13.1% within 30 days of index discharge. However, it was noted that these patients, even after stabilization of their most serious medical conditions, still had a lower readmission rate despite being transferred to rehabilitation facilities. SCI patients treated as inpatients for their injuries experienced a 15.8% readmission rate within the same timeframe from rehabilitation facilities. Therefore, reducing readmissions is critical to improving care coordination in the United States and reducing healthcare costs. 18 These findings highlight the significant readmission burden in this patient population and emphasize the need for effective strategies to mitigate this issue. So, our result demonstrated that the readmission rate following rehabilitation facilities is much higher than for an initial hospital stay. Various individuals’ characteristics may contribute to this disparity.19,20 Studies examining readmissions from rehabilitation units have revealed that data on functional status measurements, which healthcare practitioners can readily monitor, could enhance planning for a seamless transition of care delivery and help lower the probability of hospital readmission.21,22
In another study, 19 the 30-day readmission rate following traumatic brain injury was 6.6%, which was lower than the readmission rates after traumatic SCI. In this analysis, cervical and thoracolumbar injuries, patient age, and sex were predictor factors for the 30-day readmission rate following a traumatic spinal cord injury. In the 30-day readmission rate following traumatic brain injury, the longer length of stay, more comorbidities, severe index head injuries, and advanced age were significant determinants. 19
Other contributors to higher readmission rates include medical comorbidities, prior hospitalization, inpatient rehabilitation facilities’ length of stay, and discharge functional status were major contributors.23,24 Notably, functional status is an essential and modifiable health metric for individuals with traumatic spinal cord injuries and predicts adverse outcomes.23,25 In prior studies, the neurologic level has not been consistently associated with readmission risk.25,26
This study has illustrated that males are less likely to be readmitted to the hospital within 30 days after discharge, although they have potential to engage in fewer health-seeking activities and as expected in a trauma sampling of patients, there was a higher proportion of men compared to women. 27
The Comparison of the Top 10 Readmission Causes for Index Admission and Rehabilitation Facilities.
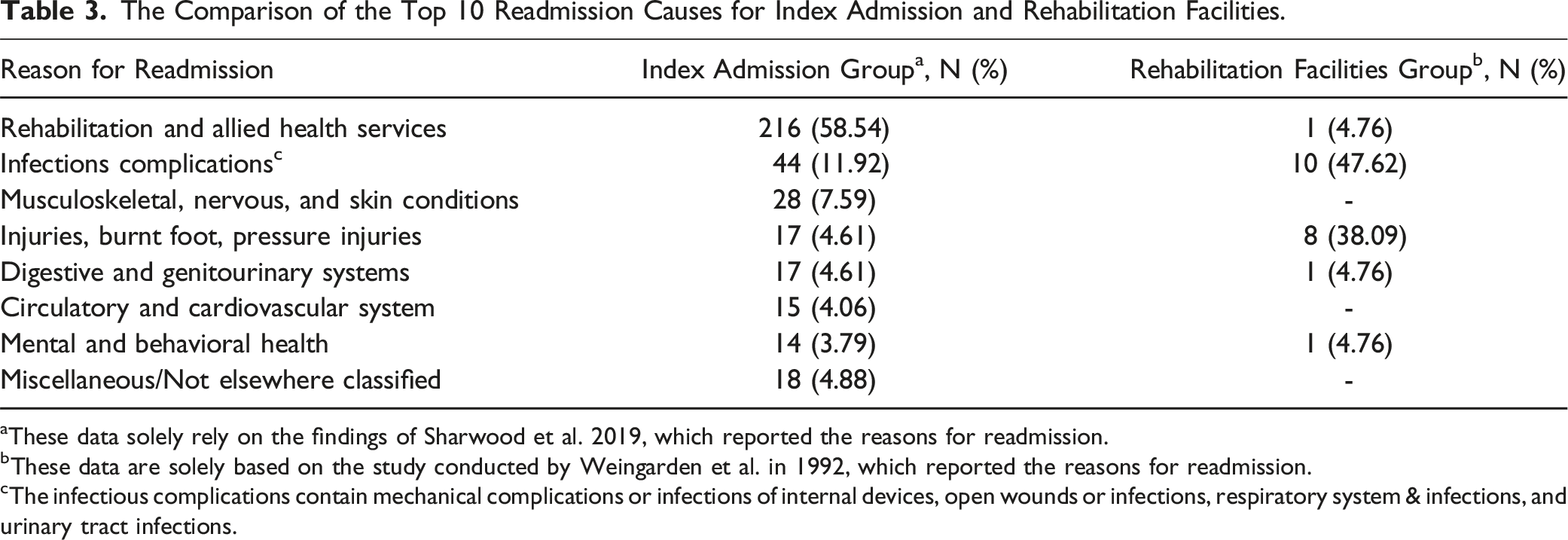
aThese data solely rely on the findings of Sharwood et al. 2019, which reported the reasons for readmission.
bThese data are solely based on the study conducted by Weingarden et al. in 1992, which reported the reasons for readmission.
cThe infectious complications contain mechanical complications or infections of internal devices, open wounds or infections, respiratory system & infections, and urinary tract infections.
This study suggests several areas of process improvement for clinical practice and healthcare systems, particularly post-discharge care for severe SCI patients. Index inpatient and rehabilitation facility patients have different readmission rates and causes, according to the study. These differences imply customized post-discharge measures to lower readmission chances. Rehabilitation facilities should improve infection control and fall prevention because patients released from these facilities had greater rates of infection and injury readmissions. In contrast, the index admission group had higher rehabilitation readmission rates, indicating a need for stronger outpatient support and follow-up to meet rehabilitation needs outside the hospital.
Hospital readmissions are a significant financial burden for healthcare providers, thus lowering these expenses could improve resources. Healthcare systems can enhance resource allocation and patient outcomes by targeting high-risk populations like cervical and thoracolumbar injury patients and rehabilitation graduates. These findings further emphasize the need for healthcare policy reforms that integrate acute and rehabilitative treatment. Traumatic SCI patients’ quality of life and readmission rates could be improved by better discharge planning, continuity of care, and post-discharge monitoring. These focused strategies should be developed and implemented in future research to reduce readmissions and enhance patient outcomes.
There were some limitations to our review. First, the majority of data was obtained from 1 healthcare system, which represents a minority of the world population. Second, the analysis of 30 days reflects a small proportion of time. Nevertheless, short-term readmissions are expensive, and reductions would not only be advantageous to patients but could also result in significant healthcare savings. Third, there are lack of evidence of readmission rate after traumatic SCI from other countries except for the USA and Australia. A significant limitation of this study is that there are many reasons for readmission rate that could raise the heterogeneity and confounding bias. Finally, this analysis includes all readmission rates following traumatic SCI and some contributors, but multiple contributors must be determining factors in readmission rates.
Readmission is an adverse health outcome that results from complex and multifaceted conditions. This makes interpreting or predicting vulnerable populations difficult. These findings underscore the importance of understanding readmission patterns following SCI and may inform healthcare strategies aimed at reducing readmissions, especially during the critical transition periods from acute care to rehabilitation. However, further research is warranted to explore factors contributing to readmissions and to develop targeted interventions to improve patient outcomes and healthcare efficiency in this population.
Supplemental Material
Supplemental Material - 30- and 90-Day Readmission Rates Following Traumatic Spinal Cord Injury: A Systematic Review and Meta-Analyses
Supplemental Material for 30- and 90-Day Readmission Rates Following Traumatic Spinal Cord Injury: A Systematic Review and Meta-Analyses by Marjan Hesari, Seyed Danial Alizadeh, Hamid Malekzadeh, Reza Tabrizi, Mohammad-Rasoul Jalalifar, Alireza Shahmohammadi, Zahra Eskandari, Zahra Ghodsi, James Harrop, and Vafa Rahimi-Movaghar in Global Spine Journal
Footnotes
Author Contributions
VR conceived the presented idea and supervised the project. MH and SDA were responsible for designing the review protocol, writing the protocol and report, conducting the search, screening potentially eligible studies, extracting and interpreting results, updating reference lists, and creating ’Summary of Findings’ tables. RT conducted the meta-regression analyses. HM was writing the report, arbitrating potentially eligible studies, extracting and analyzing data, and interpreting results. AS and MRJ contributed to data extraction and provided feedback on the report. ZE was designing the research strategy. ZG provided critical feedback and edited the draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Tehran University of Medical Sciences [grant number: 1401-1-93-55566].
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.