
Abstract
Study Design
Systematic review.
Objectives
Vertebral haemangioma has been classified into typical and aggressive vertebral haemangioma (AVH). Management options for AVH are many and the clinician has decision dilemma in choosing the right one. Metastases mimic AVH in clinical and radiological presentation. Differentiating pointers between them has not been clearly delineated in literature. Aim of our review is to identify treatment options; to formulate a management algorithm for AVH based on clinical presentation and to identify radiological differentiating pointers between them.
Methods
Systematic review was conducted according to PRISMA guidelines. We systematically reviewed all available literature from the year 2001 to 2020. Relevant articles were identified as per laid down criteria from the medical databases. After inclusion, first and second authors went through full text of each included article.
Results
Of 139 studies reviewed, eight met our criteria for review of management and three separate studies for radiological differentiating pointers. 99 patients with 88 AVH had undergone treatment. Back pain with myelopathy is the presenting symptom in majority of patients. Patients with backpain - myelopathic symptoms had improved following surgery; patients with back pain alone had improved with either percutaneous vertebroplasty or CT guided alcohol ablation. Dynamic contrast MRI, Diffusion weighted MRI and ratio of signal intensity between T1w and fat suppression T1w MR help the clinician in differentiating them.
Conclusion
Management of AVH can be based on the patient’s clinical presentation. Patients presenting with AVH and back pain can be managed with either Percutaneous vertebroplasty or CT guided alcohol ablation. Patients presenting with AVH and neurological symptoms could be managed with surgery. Dynamic contrast enhanced MR, Diffusion weighted MR, ratio of signal intensity between T1w and Fat suppression T1w MR imaging could help the clinician in differentiating the two before contemplating biopsy.
Grade Practice Recommendation
C
Keywords
Introduction
Vertebral haemangiomas are the most common primary benign tumors of the spine. Its incidence in literature is quoted to be 10-12% with thoracic spine being the commonest location.1,2 The International Society for the Study of Vascular Anomalies quote them as ‘venous malformation’ as they are histologically composed of fully developed adult blood vessels, with slow flowing dilated venous channels surrounded by fat infiltrating the vertebral body medullary cavity. 3
The literature has divided vertebral haemangioma into Typical and Atypical based on its characteristics. The presence of corduroy appearance in CT without any osseous expansion or extra-osseous extension beyond the vertebral body; hyper-intensity in T1w, T2 w MRI (Magnetic resonance imaging) images - is considered as Typical. 4 The presence of Osseous expansion or extra-osseous extension; low signal on T1w and high signal on T2w MRI images is considered as Atypical or the Aggressive variant. Aggressive vertebral haemangiomas(AVH) can mimic metastases as they present with similar clinical and radiological features and are most notorious to present with severe symptoms of backpain, radiculopathy or spinal cord compression.5,6 Literature documents various management options for AVH including medical management, CT guided alcohol ablation, External beam radiation, Percutaneous vertebroplasty and Surgery with or without preop embolization.3,16,19,20 Due to the wide array of treatment options, clinicians has decision dilemma in choosing the optimal line of management to maximise patient outcome. Nigro et al 7 in his editorial in Journal of Spine Surgery in the year 2017 has stated that AVH are common lesions with many unknown aspects and with no universal consent in its line of management.
Our hypothesis is that management of AVH can be based on the clinical presentation of the patient and a suitable algorithm can be devised based on its clinical presentation. We conducted a systematic review of the existing English literature on AVH to summarise the clinical presentation pattern, its management options based on the clinical presentation and to devise a management algorithm suitable to spine specialists in day-today clinical practice. We also attempt to summarise the various magnetic resonance imaging features that will aid in differentiating AVH from metastases.
Materials and Methods
Search Strategy and Selection Criteria
We systematically reviewed the available English literature regarding AVH and the differentiating radiological pointers between AVH and metastases. The systematic review was conducted as per PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Randomized controlled studies, prospective and retrospective studies were searched via PubMed, Science Direct, and Ovid Medline databases during the time period June -September 2021. The keywords “Vertebral” AND haemangioma, “Aggressive” AND haemangioma, “Atypical” AND haemangioma, “Spinal” AND haemangioma and their combination of MeSH terms were searched for analysis. The search was limited to articles published in the last two decades (2001 to 2020) and full text articles written in English were selected. Studies conducted before the year 2000, studies quoting the number of patients less than 5, systematic reviews, meta-analysis, case reports, grand rounds, expert comments, studies with follow-up less than one-year, non-spine studies and duplicates were excluded. Abstracts of all the articles obtained through electronic database search were reviewed. To include and exclude studies according to the defined criteria, the first and second authors went through the manuscript of all the identified articles obtained from medical databases. Discrimination in the inclusion of studies was eliminated with mutual agreement between authors (MHS and VM). As the study was conducted according to ethical guidelines, an institutional review board approval waiver was obtained. The systematic review was registered with ‘PROSPERO’ vide reference number: CRD42021266613. [Figure 1] Flowchart of literature research according to the PRISMA guidelines.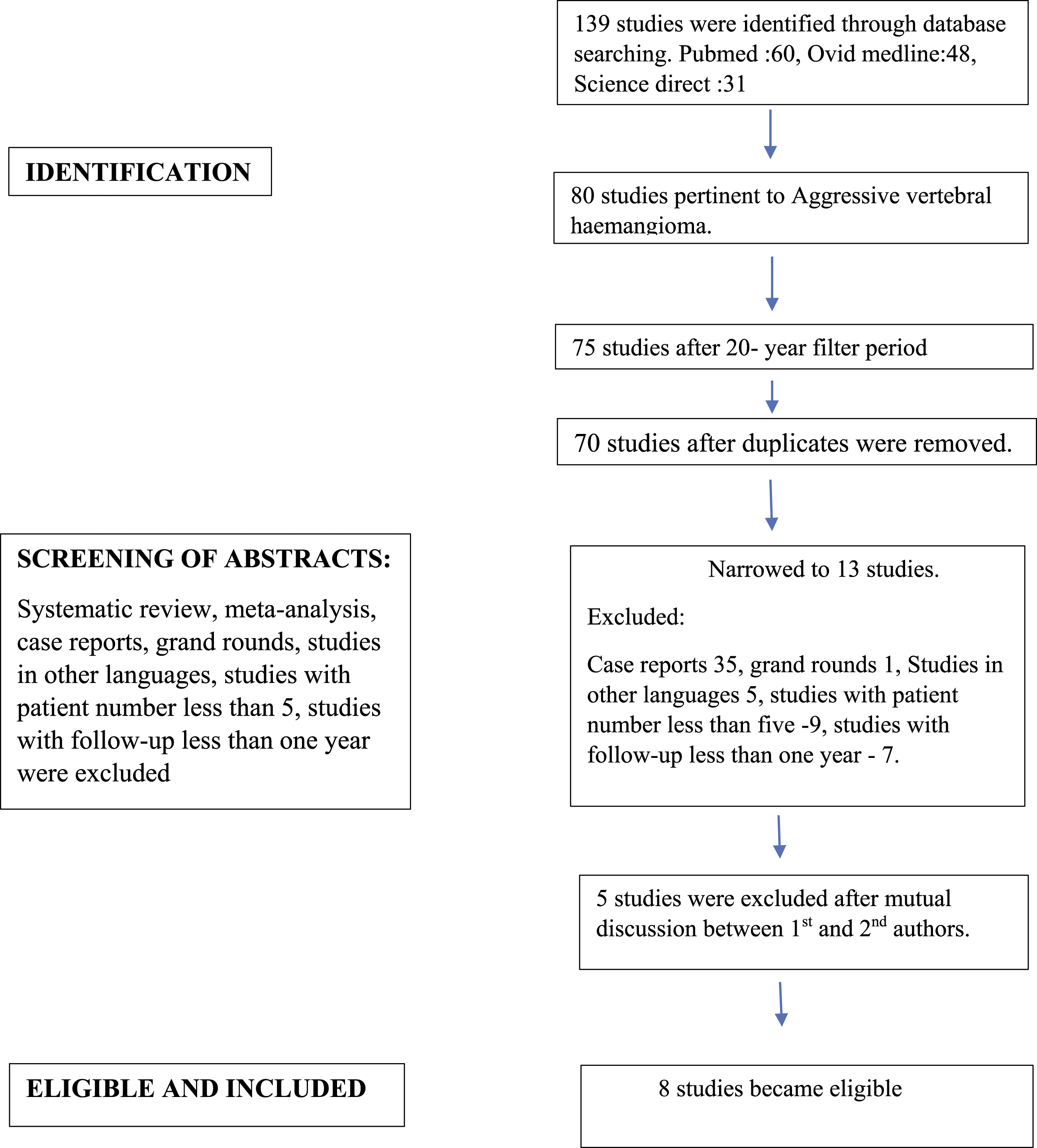
Data Extraction
All the articles which were included in the review were evaluated for the following details individually: The first author, year of study, the type of study, country - where the study was conducted, mean age of the patients, number of patients treated, mean number of AVH treated, spinal location of haemangiomas, clinical presentation of the patients in the study cohort, the type of treatment undergone by the study cohort, intra-operative parameters(mean blood loss, duration of surgery), mean follow-up duration, recurrences following treatment and any complications due to the treatment. The data was extracted into a Microsoft Excel sheet (Microsoft Corporation, USA).
Quality Assessment
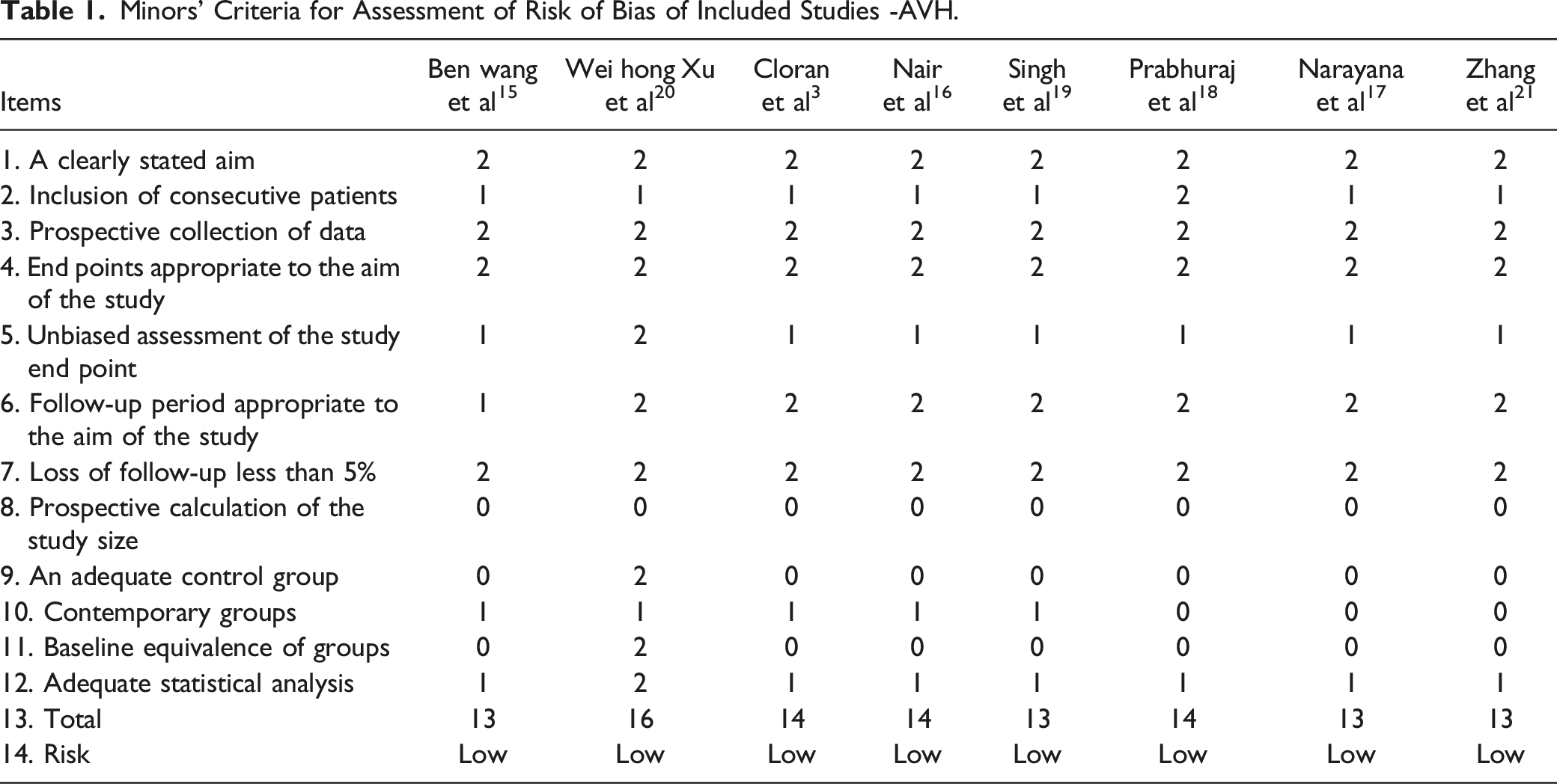
Minors’ Criteria for Assessment of Risk of Bias of Included Studies -AVH.
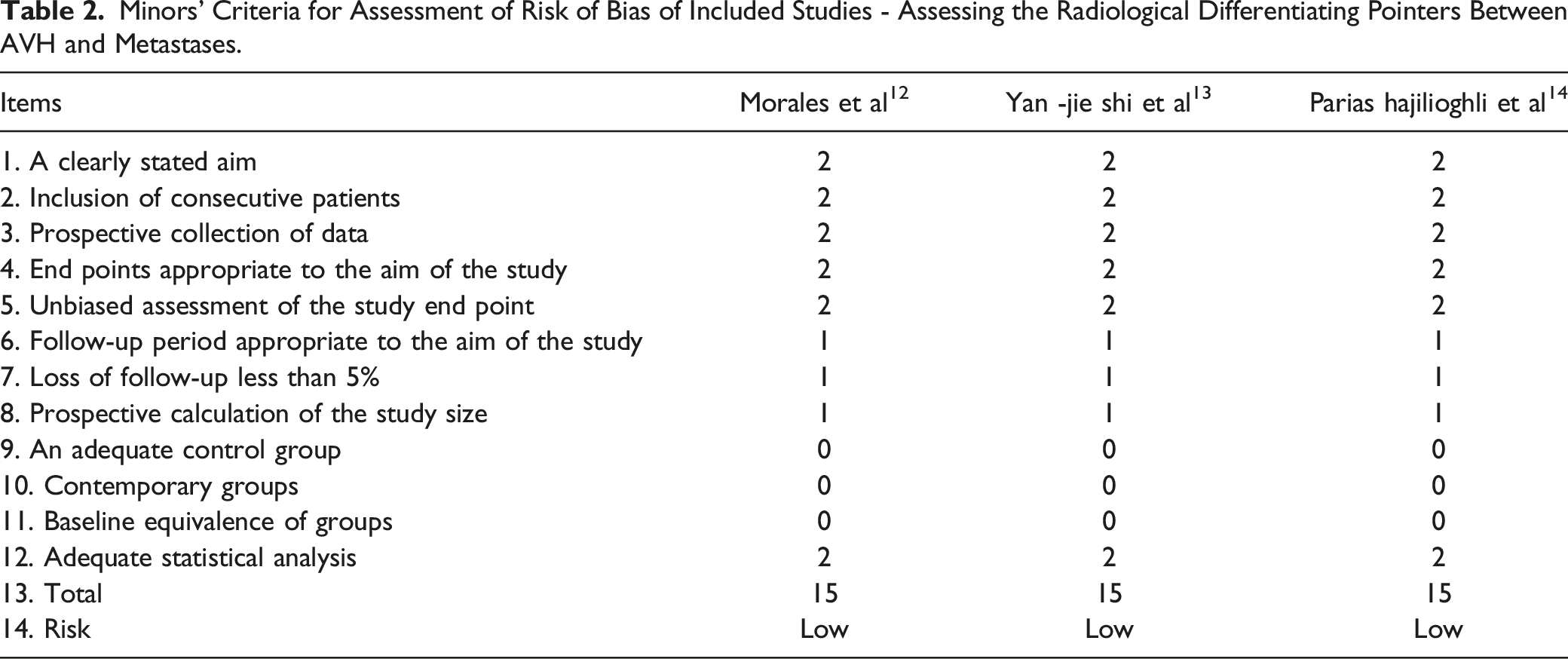
Minors’ Criteria for Assessment of Risk of Bias of Included Studies - Assessing the Radiological Differentiating Pointers Between AVH and Metastases.
Results
Of 139 studies reviewed, eight met our criteria for review of AVH management and three separate studies for radiological differentiating pointers between AVH and metastasis.
Aggressive Vertebral Haemangioma
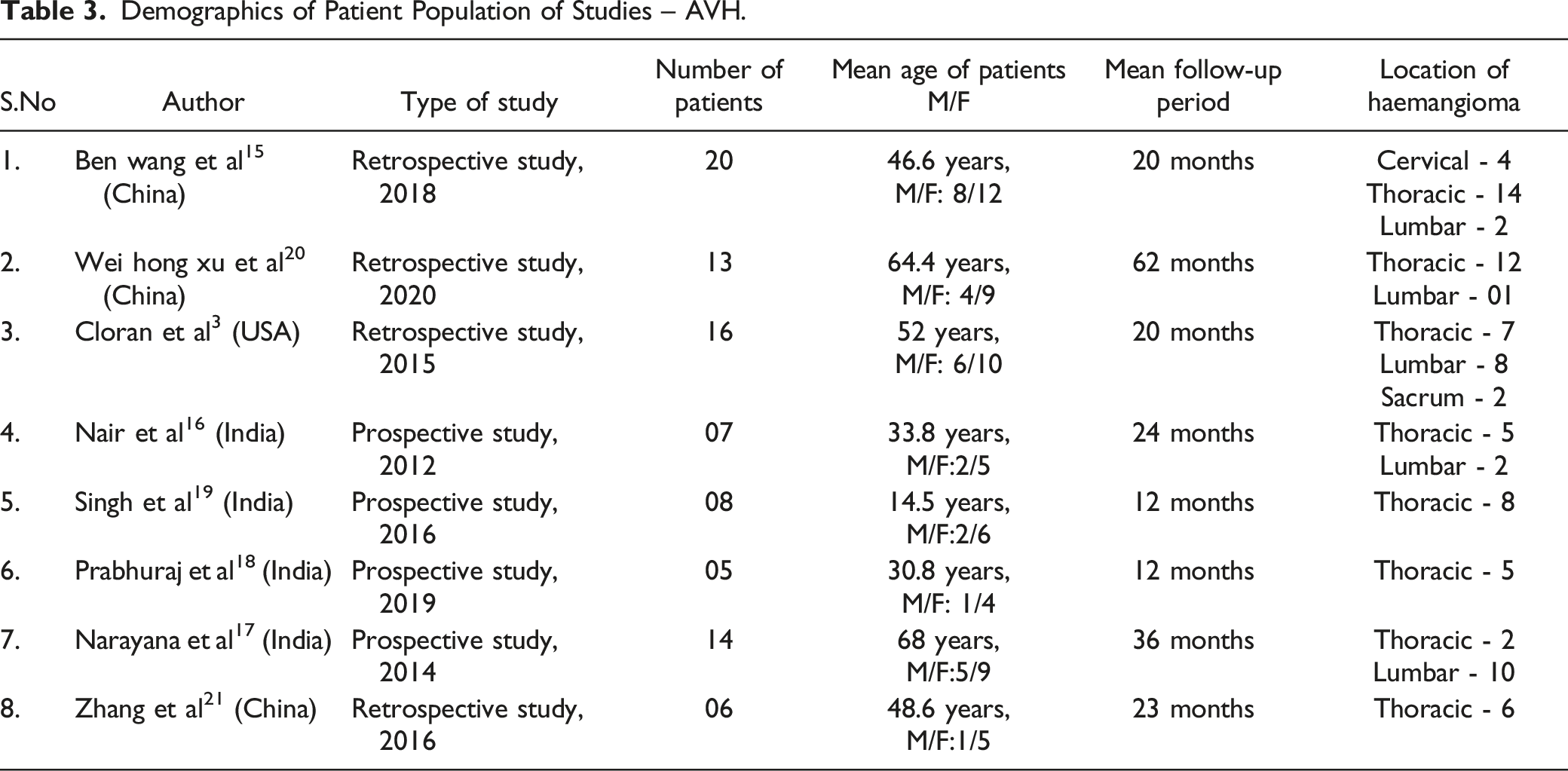
Demographics of Patient Population of Studies – AVH.
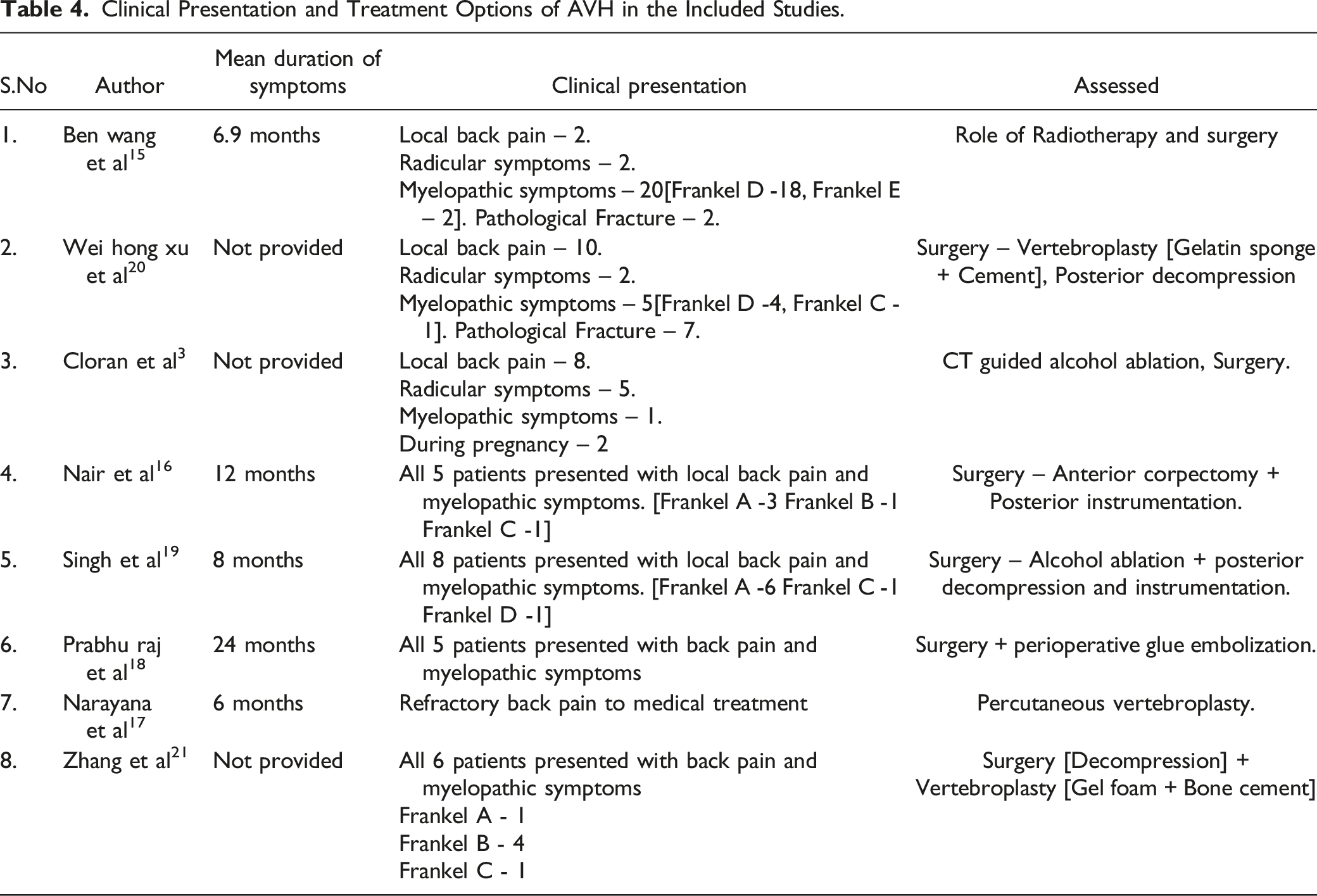
Clinical Presentation and Treatment Options of AVH in the Included Studies.
Percutaneous Vertebroplasty
14 patients had undergone the less invasive intervention procedure in the study. The Visual analog scale (VAS) for pain following percutaneous vertebroplasty had improved from mean 8.5 to mean 1.7 with a significant 57.1 percent of patients becoming pain free at 6 months of follow-up
17
[Figure 2]. A mean quantity of 3.5 ml of bone cement was injected into the vertebral body by transpedicular approach. No major complications were encountered during the procedure except in a single patient, who had extra vertebral cement leakage following the procedure that remained asymptomatic. As a routine, all the patients had undergone postoperative CT screening of the spine to identify any extra vertebral cement leakage in the study cohort. The recurrence rate following percutaneous vertebroplasty was found to be nil in the study cohort. Improvement in VAS score [back pain] following percutaneous vertebroplasty.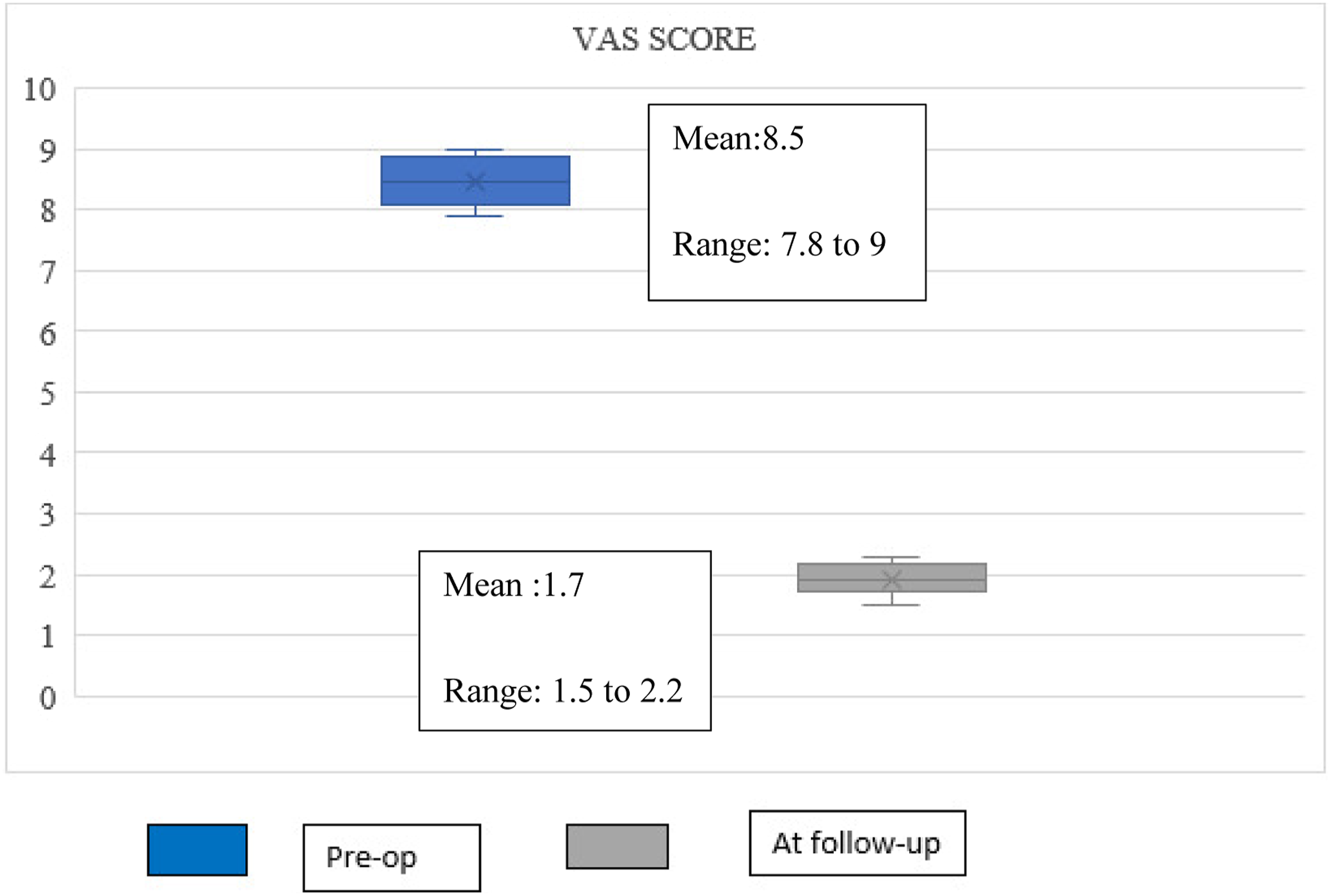
CT Guided Alcohol Ablation
Six patients had undergone CT guided alcohol ablation in the study cohort. 3 Three patients had back pain alone, two had back pain with radicular pain and one had radicular pain alone as the presenting symptoms. The patients had been followed up for mean 36.8 months. Out of the three patients who had symptomatic back pain alone as the issue, two patients (66.6%) had persistent back pain at mean follow-up. In patients with symptomatic back pain and radicular pain, 50% had residual back pain at mean follow-up. The patient with radicular pain alone had undergone alcohol ablation twice as the radicular pain had not completely resolved following the initial procedure. 33.3% of patients had relief of pain at the end of follow-up. The recurrence rate following CT guided alcohol ablation was 66.6% in the study cohort.
External Beam Radiation
Twenty patients had undergone External beam radiation treatment in the study cohort.
15
All patients had back pain with slowly progressive neurological symptoms. External beam radiation was divided into 2-25 cycles with a 50 Gy individual dose being given during each cycle. Patients had been followed up for a period of mean twenty months. 65% of patients had prompt relief of pain and improvement in neurology following external beam radiation. However, the remaining patients showed deterioration in neurology from Frankel D to Frankel B or C. Those patients with failed radiation treatment had undergone surgery in the form of posterior decompression and intra-lesional vertebroplasty. The mean duration between radiation treatment and surgery among the cohort was 1.4 months. The recurrence rate following external beam radiation treatment was 35% in the study cohort [Figure 3]. Recurrence following CT guided alcohol ablation and External beam radiation treatment.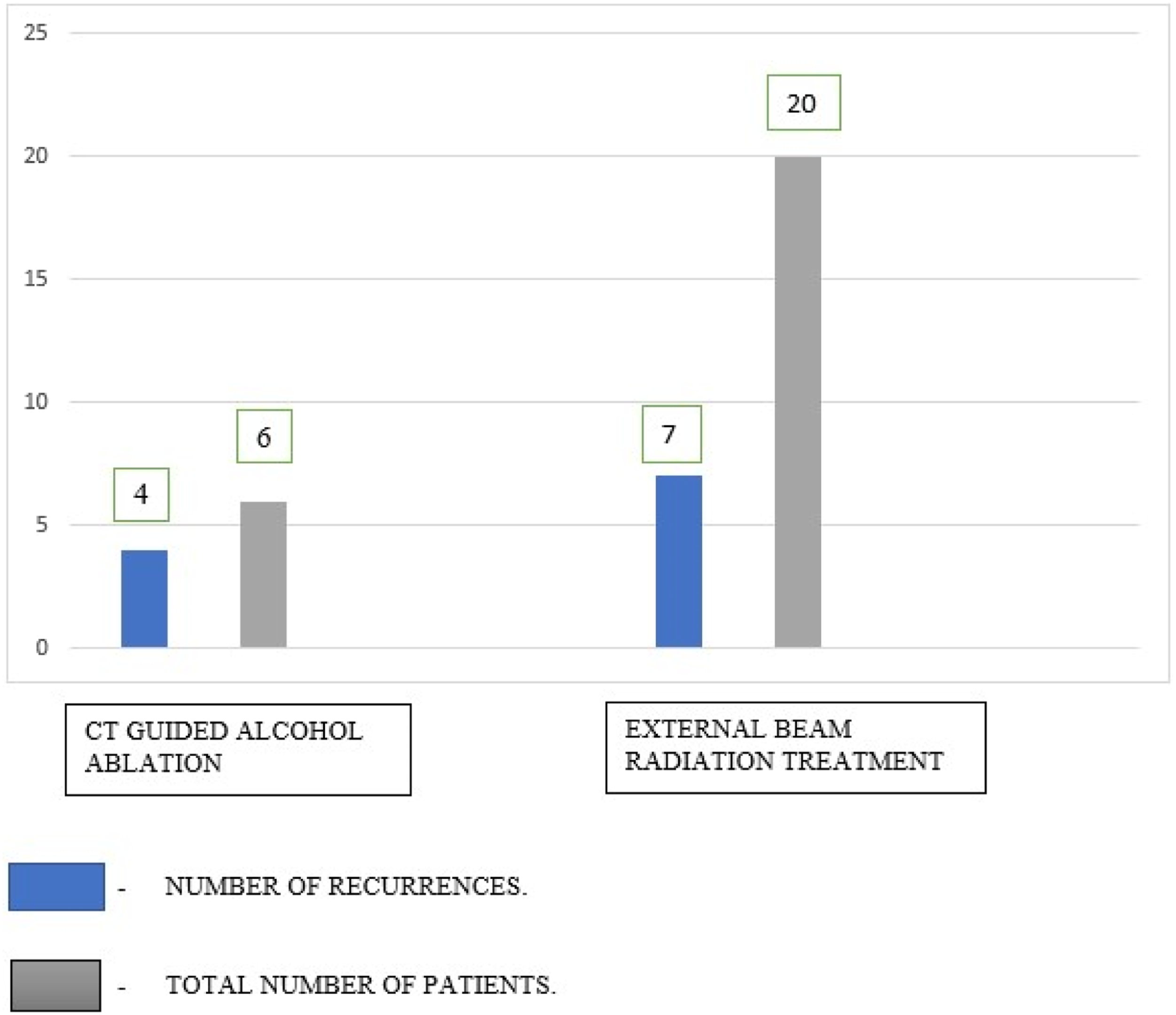
Surgery
45 patients had undergone surgery in the study cohort.15,16,18-21 27 patients had undergone percutaneous vertebroplasty using bone cement with or without gel foam and posterior decompression.15,16,18,20,21 Eight patients had undergone alcohol ablation with posterior decompression
9
and five patients had undergone anterior corpectomy, reconstruction with prior feeding vessel embolization.
16
The remaining five patients had undergone surgery following failed external beam radiation treatment.
15
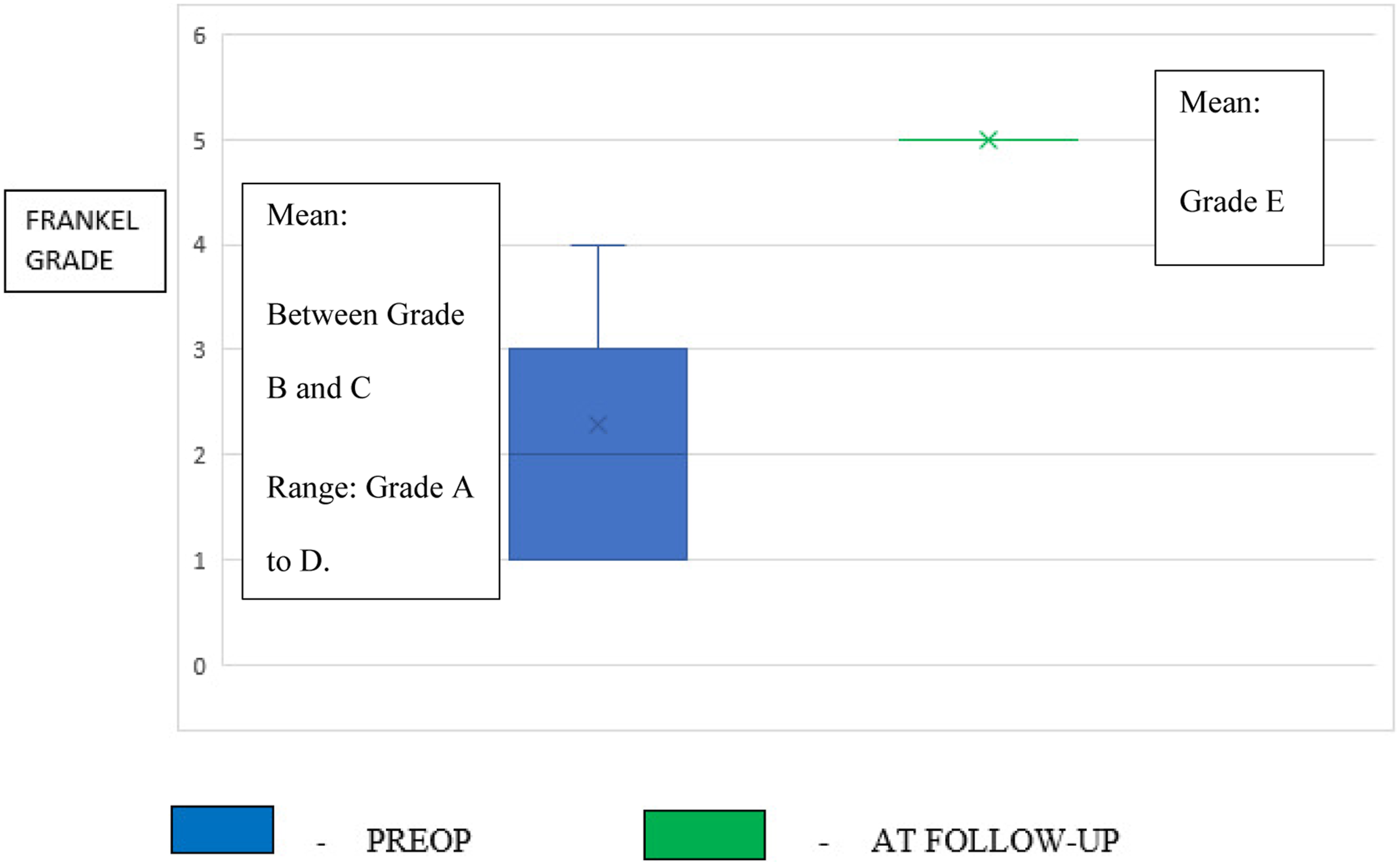
Pre-op Frankel grade was in the range A to D improved to grade E at final follow-up following posterior decompression and vertebroplasty procedure. (A single author series- Wei hong et al,
20
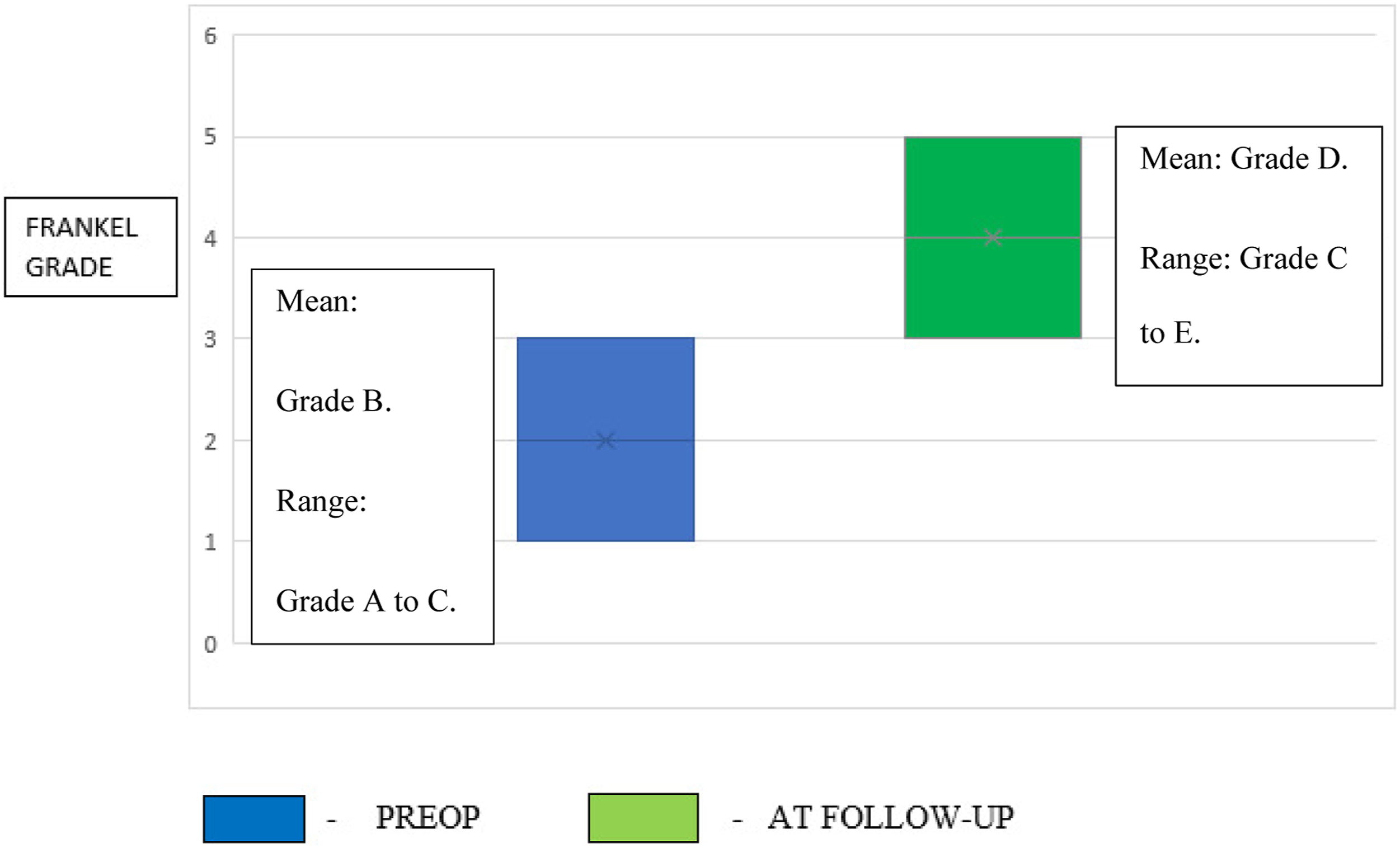
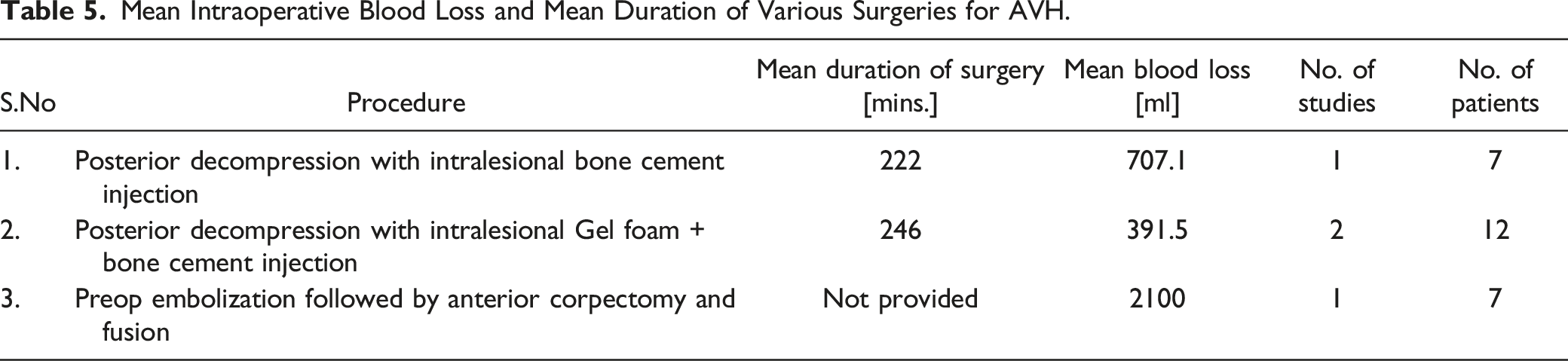
had not documented the postop improvement in neurology in his series. Hence, his series was excluded). Anterior corpectomy and reconstruction had improved the Frankel grading in the range A to C to grade C to E during final follow-up in all the five patients. Neurological improvement following surgery was gradual with 82.5% of patients showing improvement of one or two grades of Frankel grading at mean 6 months of follow-up.3,15,18-21 The mean duration of surgery and mean blood loss (even with pre-op embolization) was more with anterior corpectomy and reconstruction surgeries when compared to posterior decompression and intralesional vertebroplasty procedures
16
[Figures 4-6], [Table 5]. Mean blood loss following surgery. Neurological improvement following surgery-posterior decompression + vertebroplasty. Neurological improvement following surgery- preop embolization + Anterior corpectomy and reconstruction. Mean Intraoperative Blood Loss and Mean Duration of Various Surgeries for AVH.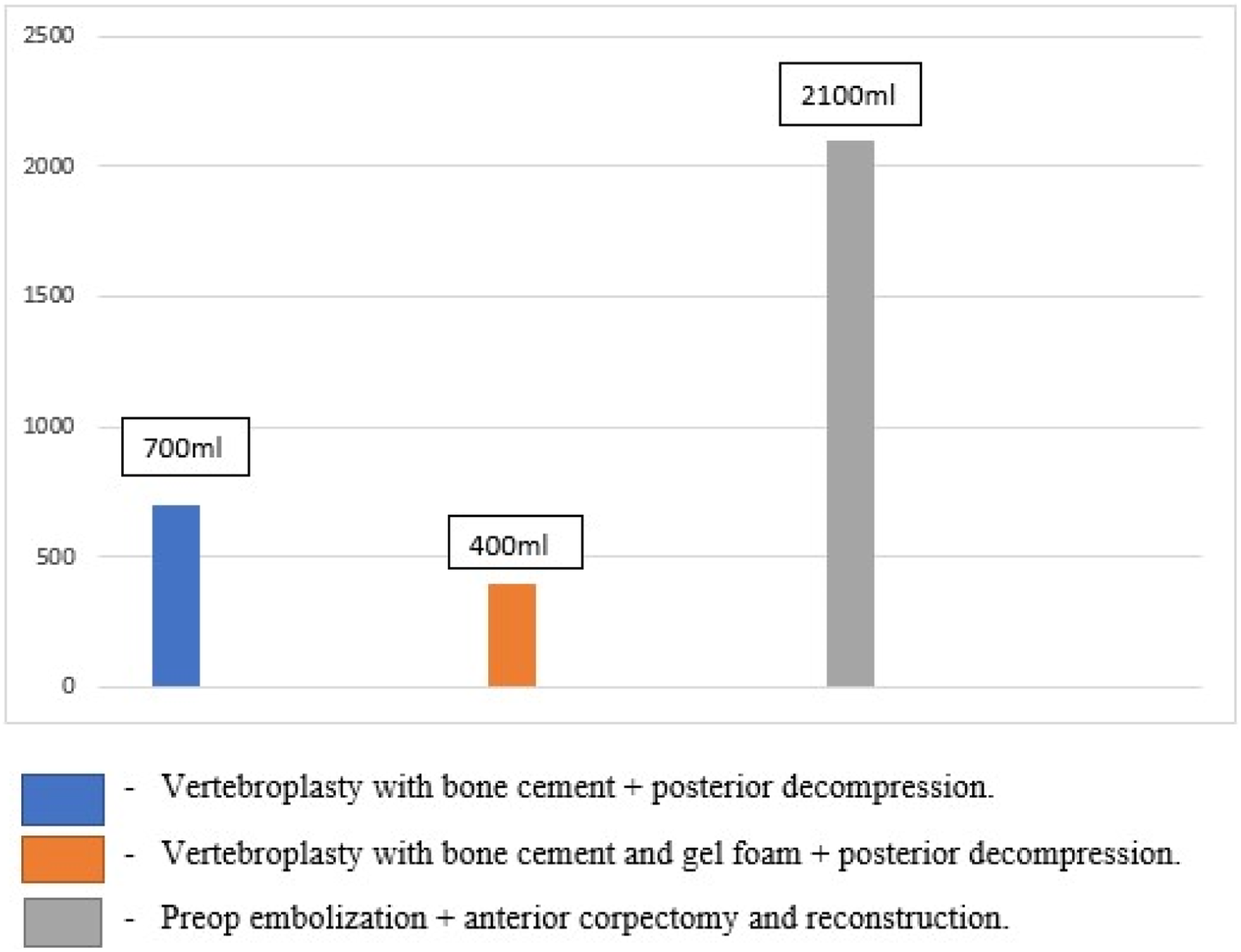
Differentiating Pointers Between AVH and Metastases
Studies Depicting Differentiating Pointers Between AVH and Metastases.
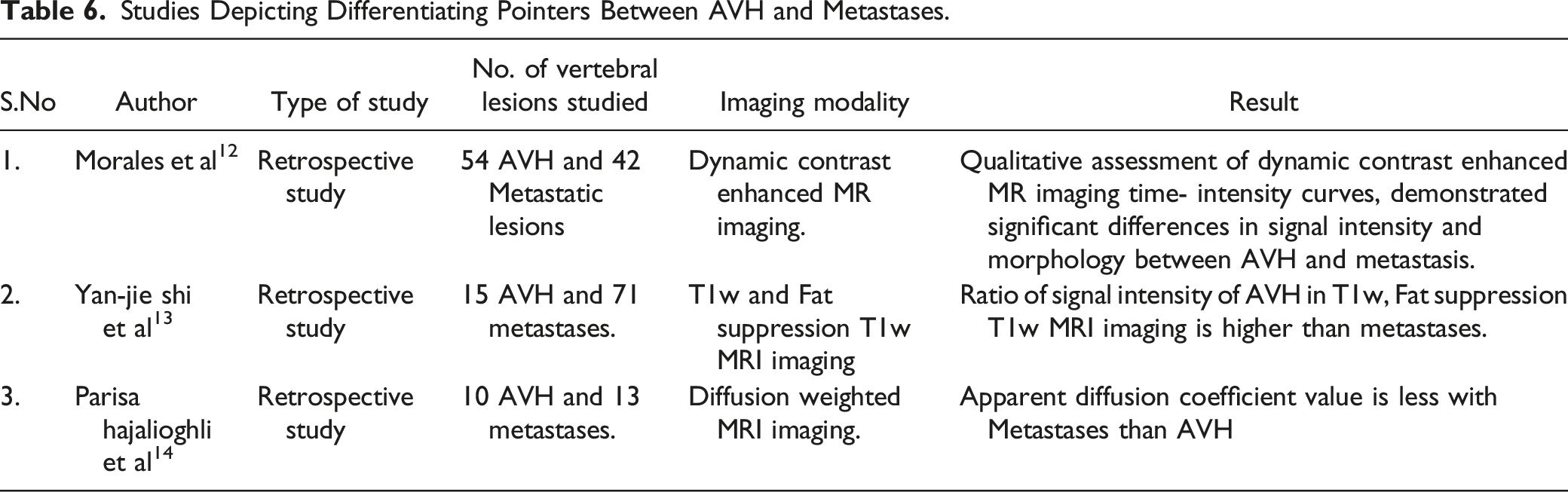
All the three studies were retrospective in nature. A total of 172 patients were studied and all of them were proven with a final confirmatory definitive biopsy. Among the 172 patients, 91 had AVH and 81 had metastasis. A sum of 79 AVH and 126 metastatic vertebral lesions had been studied in the included study cohort. These studies highlight the benefits of adding dynamic contrast imaging, 12 ratio of signal intensity in T1weighted imaging (T1w) with and without fat suppression (FS), 13 and diffusion weighted imaging 14 to conventional MRI sequences in differentiating AVH from metastases.
Qualitative inspection of dynamic contrast enhanced MR imaging time-intensity curves demonstrated differences in signal intensity and morphology between metastases and atypical haemangiomas (p < .001).
12
Signal intensity ratios (SIRs) been emphasised in distinguishing spinal haemangiomas from metastases.
13
Ratio of signal intensities (SIs) of atypical haemangiomas between T1w and FS T1w imaging was higher than those of metastases (p < .001).
13
The accuracies of ratio of SI between T1w and FS T1w imaging for differentiating typical haemangiomas and atypical haemangiomas from metastases were 96.15% and 91.86%.
13
The apparent diffusion co-efficient (ADC) determined in diffusion weighted imaging sequence differentiate between atypical haemangiomas and metastases.
14
The mean ADC value for atypical haemangiomas was 1884
Discussion
The aim of this systematic review is to devise a management algorithm for AVH based on its clinical presentation. There was definitely substantial evidence in the review regarding the utility of less invasive percutaneous vertebroplasty in patients presenting with severe refractory back pain following failed medical treatment. The role of surgery in patients presenting with backpain and neurological symptoms cannot be ignored. We have used these two essential principles in formulating our management algorithm. Our devised algorithm for the management of haemangioma is depicted in Figure 7. Authors suggested algorithm for the management of AVH.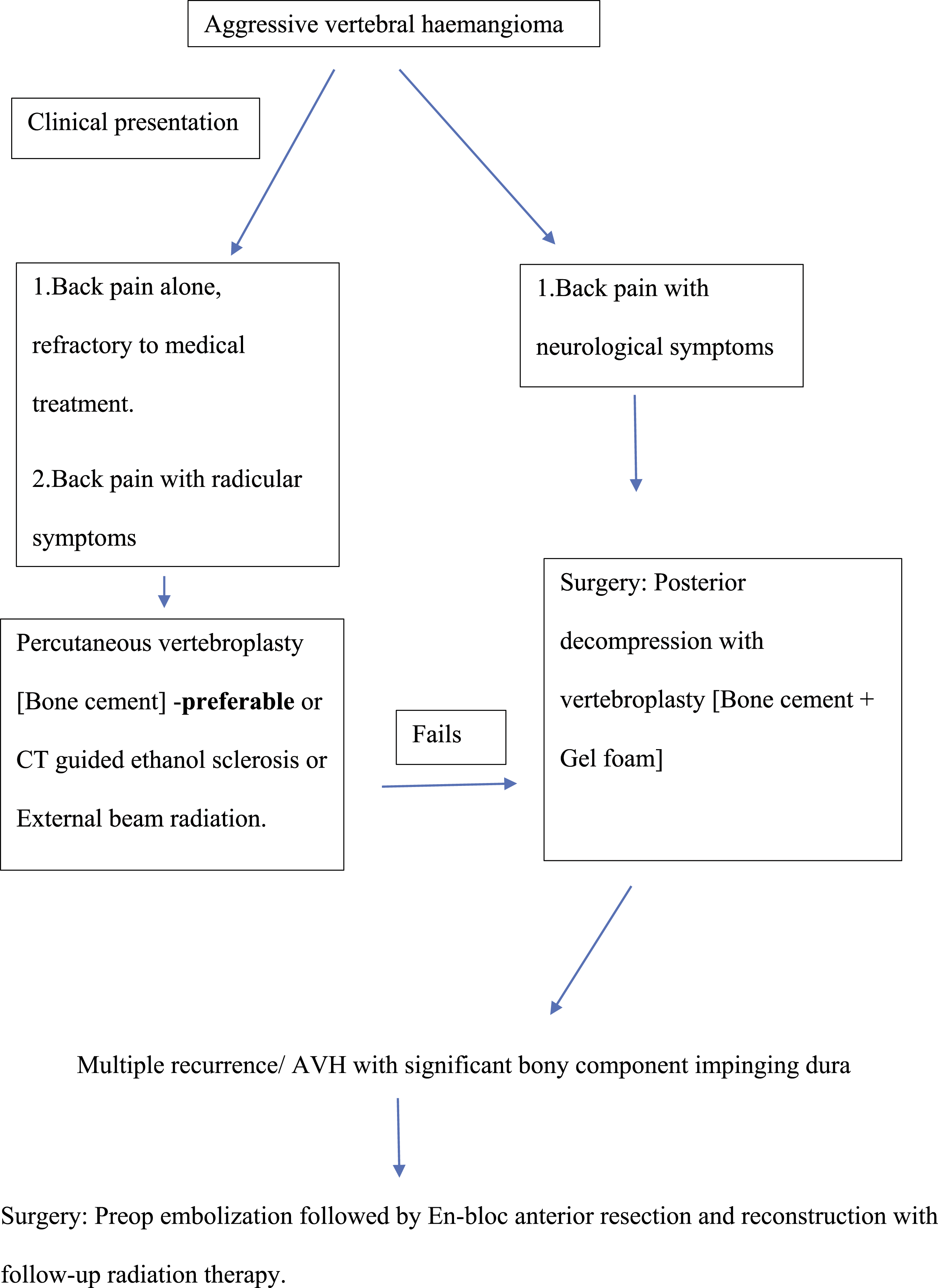
We have devised our algorithm, based on the clinical presentation of the patient after identifying it as AVH based on its radiological parameters. Patients with local back pain who are refractory to medical treatment and patients with back pain and radicular symptoms can be managed with Percutaneous vertebroplasty or CT guided alcohol ablation or External beam radiation. The preferred choice would be percutaneous vertebroplasty with bone cement. Centres not having adequately trained personnel to do percutaneous vertebroplasty can prefer CT guided alcohol ablation or External beam radiation. Patients presenting with backpain and associated neurological symptoms to be managed with surgery – percutaneous vertebroplasty (bone cement + gel foam) with posterior decompression. Patients presenting with first recurrence following CT guided alcohol ablation or external beam radiation can be offered surgery – posterior decompression with vertebroplasty. Anterior en-bloc corpectomy and reconstruction with prior embolization of the feeding vessel is to be considered if anterior bony compression exists or with multiple recurrences.
Cloran et al 3 in his paper has proposed an algorithm to treat AVH. However, the authors have not proposed which surgical approach (either anterior or posterior) to choose if the patient presents with back pain and associated severe neurological deficit. The authors prefer minimally invasive techniques (Alcohol ablation, arterial embolization of the feeding vessel) if the patient is not a surgical candidate, even in the presence of severe neurological deficits. Moreover, authors have not mentioned how to deal with recurrences following minimally invasive techniques. Lie dang et al 22 in his paper has suggested an algorithm on the basis of epidural and paravertebral extension of the tumour. He suggests vertebroplasty or radiation treatment or alcohol ablation in patients diagnosed to have haemangioma with epidural or paravertebral extension, even if the patient is symptom or pain free. He advocates surgery in patients who failed on the above lines of management even if they are neurologically intact and to consider postop radiation therapy following surgery in all patients with AVH who have developed severe or rapidly progressive neurological deficits.
The management options for AVH with back pain alone include external beam radiation therapy, CT guided alcohol ablation, percutaneous vertebroplasty and feeding vessel embolization. External beam radiation therapy 22 has been the management option of choice in the past century. It causes avascular necrosis and has a potent anti-inflammatory effect on the tumour cells. The standard regimen followed was an individual 40 Gy radiation dose in 10-20 cycles over a period of 4 weeks. Its potent adverse effects are radiation induced myelitis and secondary malignancy. Due to its severe adverse effects, it is not being considered as a primary option by many treating spine specialists. However, Heyd et al 23 in his paper claims the effects of its secondary malignancy have been overemphasized in the literature. The percent of occupancy of epidural tumour component (POET) in the spinal canal or the presence of a bony epidural tumour component has a definite say in the successful outcome following external beam radiation treatment. The patients who had a successful outcome following external beam radiation treatment had spinal canal occupancy of mean 27.5% and those who had failed radiation treatment had a mean of 61.6% spinal canal occupancy by the epidural tumour component. Patients showing absolutely no recovery following radiation treatment had significant bony compression of the cord. 15 Perhaps, POET - explains the recurrence rate of 35% with external beam radiation treatment in the study cohort.
CT guided alcohol ablation 22 is a viable alternative in the management of AVH. Alcohol injection into the vertebral body causes vascular thrombosis and destruction of its vascular endothelium, creating devascularisation of the lesion and its subsequent shrinkage resulting in cord and nerve root decompression. Doppman et al 24 suggests an alcohol volume of less than 15 ml is enough to shrink the lesion without affecting spinal stability. Its adverse effects are transient neurological deficit, pathological fractures and recurrences. Goyal et al 25 suggests – non uniform distribution of alcohol into the haemangiomatous vertebral body after injection as the primary reason behind the recurrences. This explains the high recurrence rate of 66.6% in the study cohort. Embolization of the feeding vessel has been a modality in usage in reducing the vascularity of highly vascular tumours. Kawahara et al 26 had suggested sacrifice or blockage of three consecutive segmental arteries of the spine bilaterally in canines or in humans does not cause vascular compromise to the spinal cord. However, with the advent of Vertebroplasty, direct alcohol injection usage and arterial embolization of the feeding vessel has become vague.
Percutaneous vertebroplasty 17 involves injection of polymethylmethacrylate through specialised needles into the vertebral body under image intensifier guidance. The heat produced by polymerisation of the cement destroys the highly vascular tumour cells and thereby causes shrinkage of the tumour. In ideal conditions, 4-7 ml of bone cement can be injected through a bilateral pedicular approach. Its disadvantages being cement extravasation into the epidural space and into the systemic circulation. Some authors20,21 consider mixing bone cement with gel foam while doing vertebroplasty to reduce the blood loss associated with surgery (Vertebroplasty with posterior decompression).
The management option for AVH with back pain and neurological symptoms is surgery. The goal of surgery is to excise or to ablate the tumour that compresses the neural elements and to do bony decompression.
22
The standard techniques being posterior decompressive laminectomy in addition to vertebroplasty15,18,20,21 or direct alcohol injection3,19 and anterior corpectomy, reconstruction with prior feeding vessel embolization.16,27 In patients presenting with AVH and neurological symptoms, it is the epidural soft tissue mass which causes cord compression and the neurological symptoms.
22
Hence, an appropriate posterior decompression with vertebroplasty or direct alcohol injection can produce good results. With these techniques, pre-op feeding vessel embolization is no longer recommended. Postop radiation therapy can be recommended following this procedure, if contrast enhanced CT picks up a residual lesion in the follow-up.
22
Anterior corpectomy and reconstruction is specifically indicated for ventrally located lesions causing primary bony compression over the cord or the AVH presenting following multiple recurrences.22,27 The main concern regarding the procedure is substantial blood loss and it is always recommended following feeding vessel embolization.16,22,27 [Figure 8] Ben wang et al
15
-29-year-old lady diagnosed with T3 AVH presented with back pain and weakness of her lower limbs [Frankel D], underwent surgery-posterior decompression with vertebroplasty with complete resolution of her neurological weakness [Frankel A] at two years of follow-up. A,B-CT Images, C,D-MRI Image, E, F-Intraop images, GH-At two-years follow up.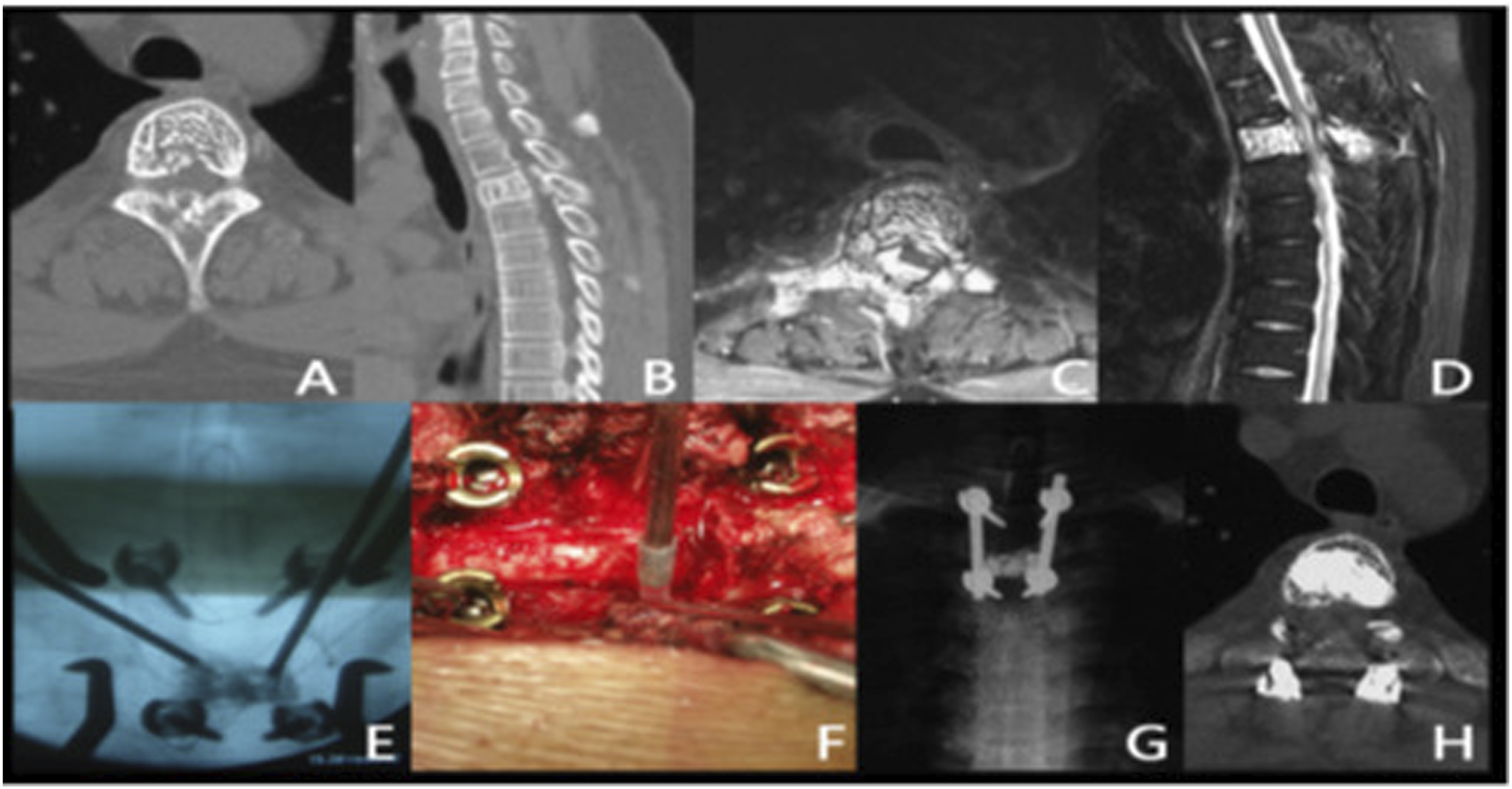
In the latest published systematic review and meta-analysis (2022), Conti et al 28 have tried to document the therapeutic role of Radiosurgery/ Stereotactic body radiation therapy in the management of AVH. The authors conclude that overall good local response (no progression of the disease) and adequate pain relief following radiosurgery in their series as 94.1 and 87.5% respectively. However, both these parameters were statistically insignificant in their analysis (p = .7, p = .2). Though radiosurgery is considered more precision oriented when compared to external beam radiation, the authors report damage to surrounding tissues following radiosurgery as 22.3% (p = .02) in their review.
Whenever, a spine specialist has a dilemma about differentiating the lesion between AVH and metastases due to similarities in clinical presentation and diagnostic parameters, we recommend using differentiating pointers. Morphological assessment of time-intensity curves obtained by qualitative assessment of dynamic contrast enhanced MR imaging 12 helps in differentiating between AVH and metastases.
Morales et al
12
in his paper on the role of T1w dynamic contrast enhanced MR imaging in differentiating AVH and metastases has specified the value of Time-intensity curves [Figure 9]. The time-intensity curve of metastases due to its higher vascular permeability when compared to AVH, shows a sharp slope with higher peak signal intensity followed by faster terminal washout phase. Whereas, AVH shows minimal and delayed signal intensity within a narrow range (no sharp slope and terminal slow washout phase). Time-intensity curves-AVH vs Metastases/Dynamic contrast MR imaging.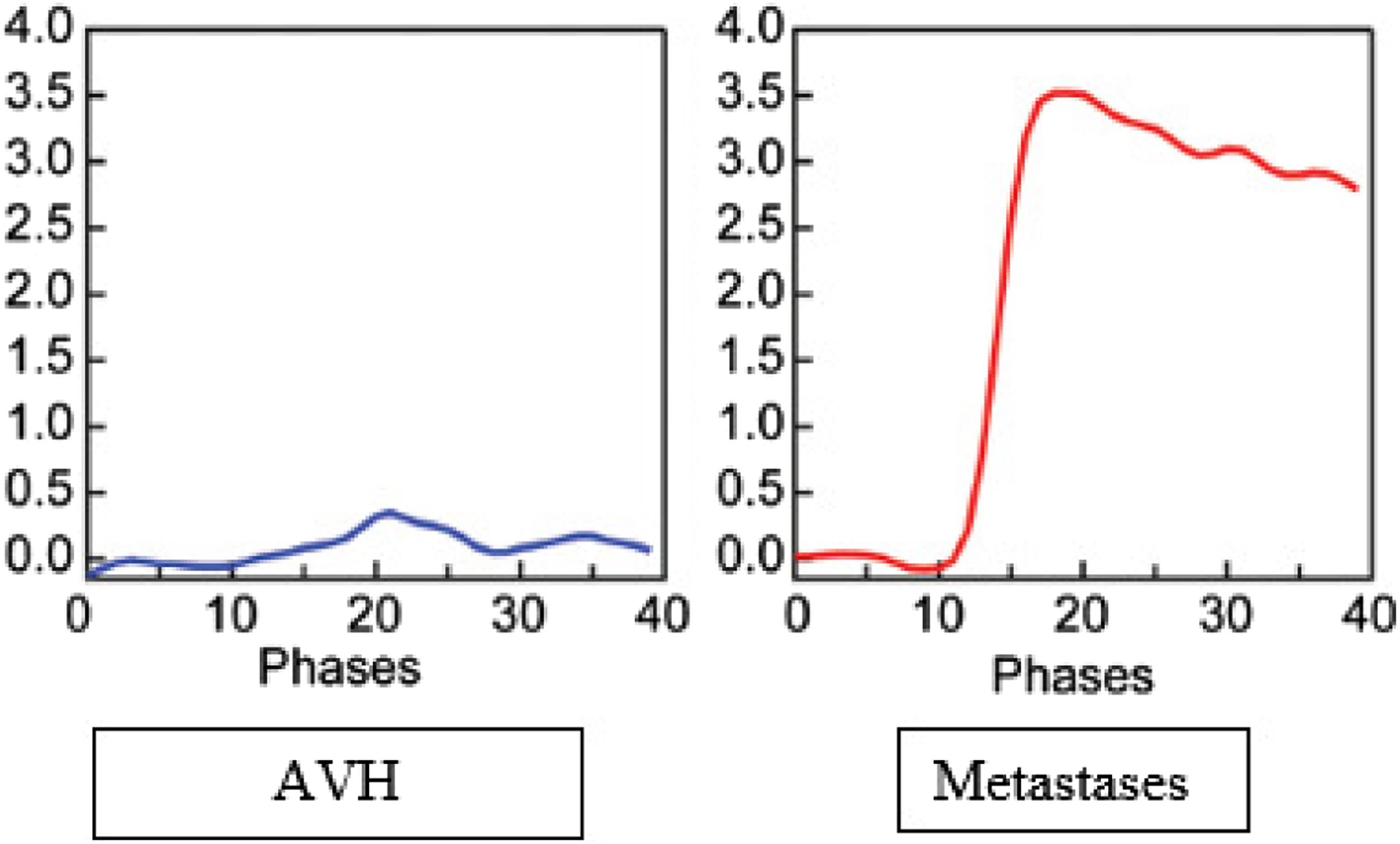
AVH has a high level of fat component when compared to metastatic destructive vertebral body lesion and it shows quite a hyperintense signal in T1w MR when compared to metastases. Yan-jie shi et al 13 suggests the ratio of signal intensity between T1w and fat suppressed T1w is more with AVH when compared to metastases and he proposes it as the highest accuracy in differentiating between AVH and metastases. Diffusion weighted MRI 14 can also be used to differentiate AVH and metastases with cut-off for an ADC value above 958 × 10-6 mm2/s for AVH and below the cut-off value as metastases.
Limitations
The limitations of this systemic review are: the risk of selection bias in the selected studies due to inclusion and exclusion criteria. As the incidence of AVH is less, studies with limited patient number (at least more than 5) have also been considered in the review which may have an effect on the results concluded. Moreover, certain studies did not clearly define the neurological improvement and the complications encountered with surgical procedures.
Grade Practice Recommendation 29 : Optional (C)
The studies were retrospective and prospective in nature and there was no randomised control study pertaining to AVH in the literature. There were consistent studies documenting the results of percutaneous vertebroplasty, external beam radiation, CT guided alcohol ablation in patients with isolated back pain, and the definite role of posterior decompression with vertebroplasty in patients presenting with backpain and associated neurological symptoms, but there were inconsistent studies regarding the role of Anterior corpectomy and reconstruction with prior embolization of the feeding vessel in the management of AVH.
Conclusion
Management of AVH can be based on the patient’s clinical presentation. Patients presenting with AVH and back pain without neurological symptoms can be managed with either Percutaneous vertebroplasty or CT guided alcohol ablation. Patients presenting with AVH and associated neurological symptoms could be managed with surgical options. Dynamic contrast enhanced MR imaging, Diffusion weighted MR imaging, ratio of signal intensity between T1w and Fat suppression T1w MR imaging could help the clinician in differentiating AVH from metastases before contemplating biopsy.
Supplemental Material
Supplemental Material - Management of Aggressive Vertebral Haemangioma and Assessment of Differentiating Pointers Between Aggressive Vertebral Haemangioma and Metastases – A Systematic Review
Supplemental Material for Management of Aggressive Vertebral Haemangioma and Assessment of Differentiating Pointers Between Aggressive Vertebral Haemangioma and Metastases – A Systematic Review by Macherla Haribabu Subramaniam, Victor Moirangthem, and Muralidharan Venkatesan in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
An IRB official waiver of ethical approval was granted from the IRB board as the study is a systematic review. Made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data; or the creation of new software used in the work: Dr.MHS and Dr.VM. Drafted the work or revised it critically for important intellectual content: Dr.MHS and Dr.MV. Approved the version to be published: Dr.MHS, Dr.VM and Dr.MV. Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: Dr.MHS, Dr.VM and Dr.MV.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.