
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Symptoms caused by spinal metastases are often difficult to distinguish from symptoms caused by non-malignant spinal disease, complicating timely diagnosis, referral and treatment. The ensuing delays may promote the risk of neurological deficits or severe mechanical instability and consequent emergency surgery, leading to poorer prognosis. Presumably, treatment delay may subsequently lead to more health-care consumption and therefore increased average costs of treatment.
Methods:
All patients surgically treated for spinal metastases were included in the current study. Based on the presence of alarming symptoms and urgency of the required intervention, patients were categorized as having received timely or delayed treatment. Pre-surgical, in-hospital, aftercare and total costs were analyzed and compared between the 2 groups.
Results:
In total, 299 patients were included, of which 205 underwent timely and 94 delayed treatment. There was no significant difference in pre-surigcal costs (€3.229,13 in the timely treated group vs. €2.528,70 in the delayed treatment group, p = 0.849). The in-hospital costs (€16.738,49 vs. €13.108,81, p < 0.001) and the aftercare costs (€13.950,37 vs. 3.981,93, p < 0.001) were significantly higher for delayed treatment vs. timely treatment, respectively. The total costs were €33.741,71 for delayed treatment and €20.318,52 for timely treatment (p < 0.001).
Conclusions:
The total costs for timely treated patients with spinal metastases are significantly lower compared with patients receiving delayed treatment. Investing in the optimization of referral patterns may therefore reduce the overall pretreatment delay and subsequently increase patient outcome, leading to better clinical outcomes at lower costs.
Keywords
Introduction
Spinal metastases occur in approximately 20% of all oncological patients.1,2 Due to an increase in overall cancer survival rates, this number is expected to rise considerably over the next few decades.3,4 Because symptoms caused by spinal metastases are commonly non-specific, patients with spinal metastases are at-risk for delayed diagnosis, referral and treatment.5-7 Problematically, untreated spinal metastases can eventually cause mechanical instability of the spine and/or neurological deficits due to compression of neural structures, requiring emergency surgery.6,8-12 It is well studied that emergency surgery leads to considerably worse patient outcome compared with timely interventions.13,14
The optimization of referral patterns for patients with spinal metastases may reduce overall delay, preventing the negative effects associated with delayed treatment. A subsequent potential cost increase of more extensive diagnostics and referrals may, however, discourage health-care providers and insurance companies in pursuing this practice. Nonetheless, a potential decrease in clinical and aftercare costs is rarely considered and may outweigh the increase in upfront costs. Until now, no study has investigated the difference in costs between patients undergoing timely and delayed treatment for symptomatic spinal metastases.
The purpose of this study was to assess the difference in costs between timely and delayed surgical treatment for symptomatic spinal metastases. It was hypothesized that delayed treatment is associated with higher costs than timely treatment.
Methods
Study Design
The ethics review board (METC Utrecht, protocol no. 18-841-C) approved a waiver of informed consent for this observational, retrospective cohort study. Patient and treatment data has been prospectively collected for all patients referred to a single tertiary spine center for surgical treatment of radiographic or histologically proven symptomatic spinal metastases between March 2009 and January 2019. Age, sex, primary tumor type, EQ-5D-5 L scores, Karnofsky Performance Scores (KPS), Visual Analog Scale (VAS) scores for pain, neurological status and date of death were extracted from medical records.
Patients were categorized into “timely” or “delayed” treatment. Delayed treatment was defined as requiring surgical treatment within 3 days, either due to (progressive) neurological deficts and/or gross mechanical instability. It indicates limited time during work-up, potential surgery during after-hours and preclusion of elective intervention. Timely treatment was defined as the ability to undergo elective surgery more than 3 days after initial presentation. It suggests sufficient time left for work-up until planned treatment. The 3-day cutoff was chosen in accordance with the protocol used by the Global Spine Tumor Study Group. 15
All treating spine surgeons adhered to generally accepted principles for surgical treatment of patients with spinal metastases, combining common scoring systems (currently NOMS: ASIA/Frankel classification for neurological status combined with Bilsky score for degree of epidural compression; Bollen classification for prognosis; SINS for spinal stability and KPS for general patient condition).16-18 Furthermore, a uniform treatment strategy was achieved by a weekly plenary multidisciplinary “spine meeting.”
The referral chain for each individual patient was analyzed using medical records and all relevant correspondence with other health-care providers. In the Netherlands, all health-care providers send a summary of consultation to the patient’s general practitioner. Therefore, the medical record possessed by the general practitioner can be used for, near complete, reconstruction of the timeline of referral, diagnosis and treatment.
Health-care costs were calculated in Euros. Costs were analyzed separately for 3 different stages: Pre-surgical costs (from the first medical consultation for spinal metastases related symptoms until admission to our spine unit), in-hospital costs (from admission to our spine unit until discharge) and initial aftercare costs (from discharge until 3 months postoperatively).
Pre-Surgical Costs
The pre-surgical costs consisted of outpatient care, general practitioner visits, diagnostics and previous admission days (related to metastatic spinal disease) at a different ward or hospital. Because only the involvement of a health-care provider (outpatient clinic or general practitioner) was available, and not the number of visits, 1 visit per health-care provider involved was assumed. The national average prices for outpatient visits, diagnostics and admission days were used. 19 For SPECT-scans and conventional spinal radiographs, no nationwide average reference costs were available. Therefore internal prices of our institution were used (Table 1). Costs for one admission day were multiplied by the LOS (in days) for each individual patient.
Prices Used for Cost-Analysis.
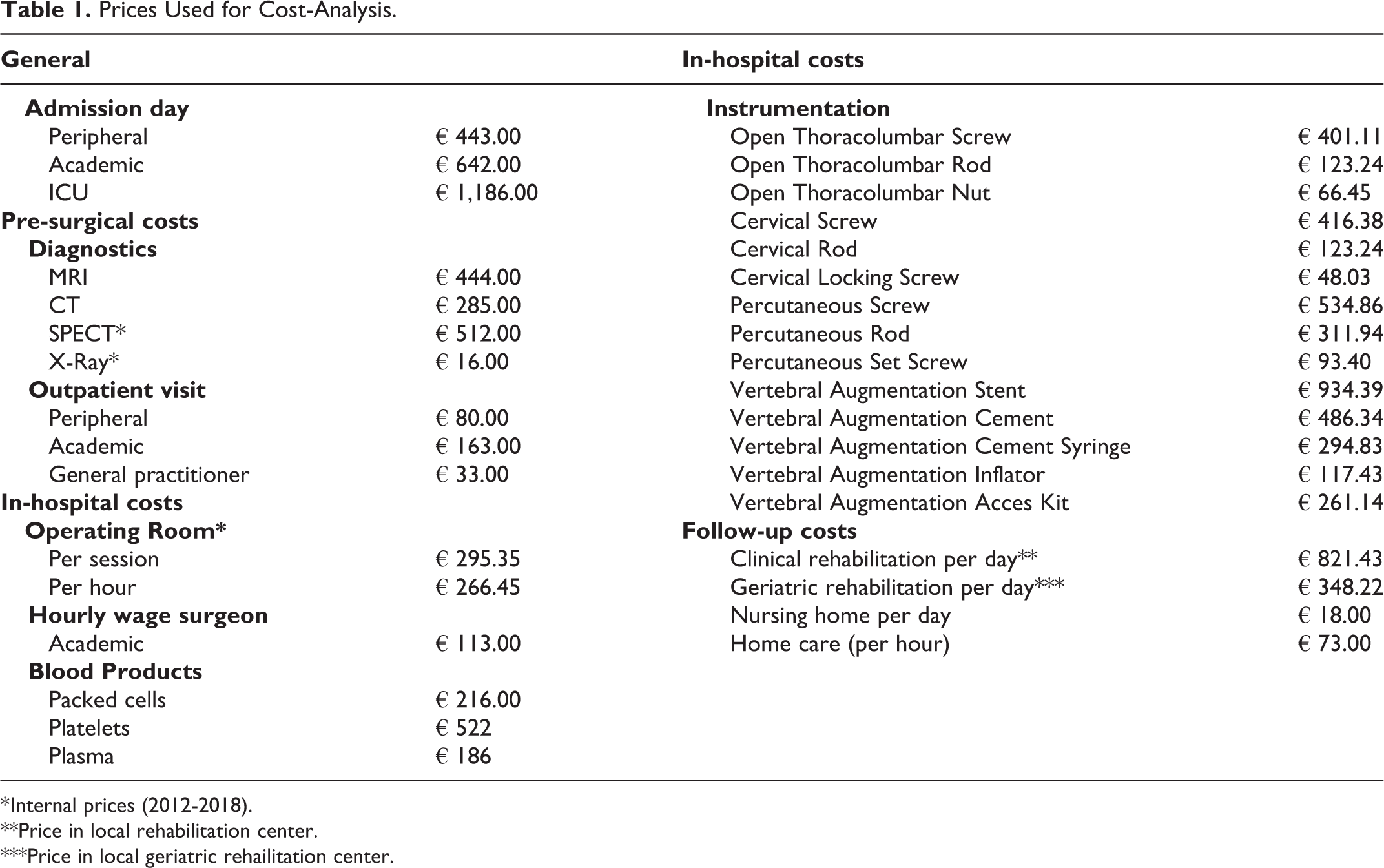
* Internal prices (2012-2018).
**Price in local rehabilitation center.
***Price in local geriatric rehailitation center.
In-Hospital Costs
The in-hospital costs consisted of surgical and hospital admission costs. To calculate the surgical costs, the following data were extracted from the patients’ medical records; the implants used, time in operating room (OR) and surgeon operating time. Nationwide average prices were available for the surgeon’s salary. For the costs associated with the surgical implants and the OR utilization (including associated costs such as OR staff salary, logistics, cleaning ect.), internal prices were used. To calculate the hospital admission costs, the number of admission days and use of blood products were extracted from medical records and nationwide average prices were used (Table 1). 19
Aftercare Costs
After discharge, patients went to either a (geriatric) rehabilitation clinic; a nursing home; a different hospital; a different ward in the same hospital; or their own home with or without homecare assistance. Nationwide average prices for stay in a nursing home (per day), homecare (per hour) and a hospital admission day were used (Table 1). In the Netherlands, a stay in a nursing home generally means limited perspective on returning home. Therefore, the daily price was multiplied by the days left until the 3 months follow-up.
For a rehabilitation clinic, the average daily price was calculated by using the average reimbursement price for a stay of 6 weeks with 99-223 treatment hours, divided by 42. For geriatric rehabilitation, the average daily price was calculated using the reimbursement price of a standard stay of 29 to 56 days with more than 59 treatment hours, divided by 42. In case the duration of (geriatric) rehabilitation could not be extracted from the medical record, the standard rehabilitation period for patients with metastatic spinal disease of 6 weeks was assumed.
After (geriatric) rehabilitation, data about homecare assistance was extracted from medical records up to 3 months postoperatively. Data on re-admissions, including reoperations, were extracted from patients’ medical records up to 3 months postoperatively.
Statistical Analysis
For continuous data, means and standard deviations (SD) were used in case of normally distributed data. Medians and interquartile range (IQR) were calculated in case of non-normally distributed data. For categorical data frequencies were used. In case of normally distributed data, unpaired T-tests were used to compare continuous parameters and Chi-squared tests to compare categorical parameters. Normality was assessed visually using Q-Q plots and in the case of non-normal distribution, the data was log-transformed for statistical analysis. All analyses were performed using IBM SPSS Statistics for Macintosh, Version 24.0 (Armonk, NY: IBM Corp).
Results
In total, 299 patients were included of which 205 underwent timely treatment and 94 delayed treatment. No significant differences were found in terms of patient age, sex, tumor histology, VAS-pain scores and median survival in months. As expected, timely patients had higher baseline EQ-5D-5 L and KPS scores and a lower percentage of neurological deficits, compared with delayed patients (Table 2).
Patient Characteristics for Patients in Both Surgery Groups.
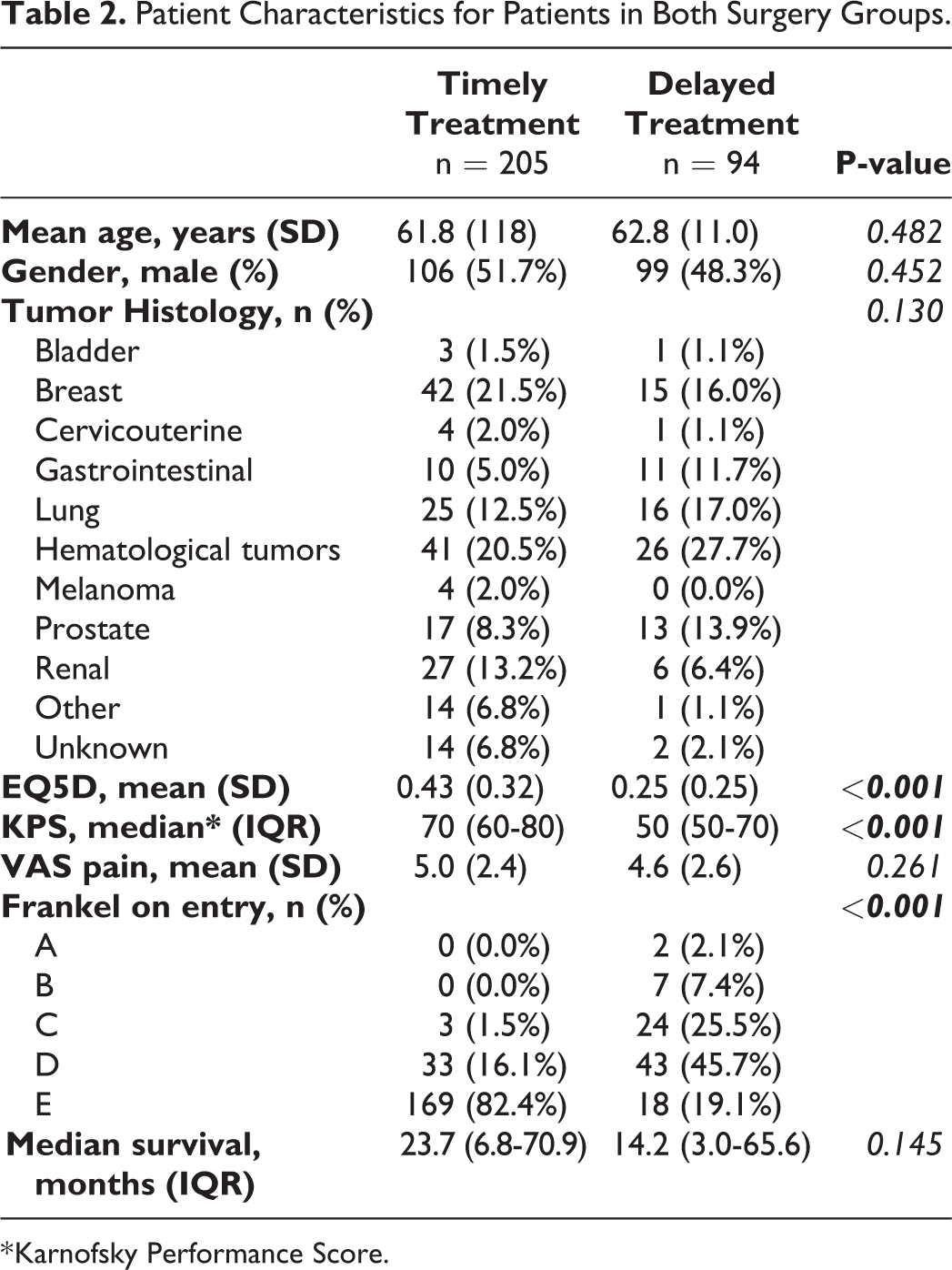
* Karnofsky Performance Score.
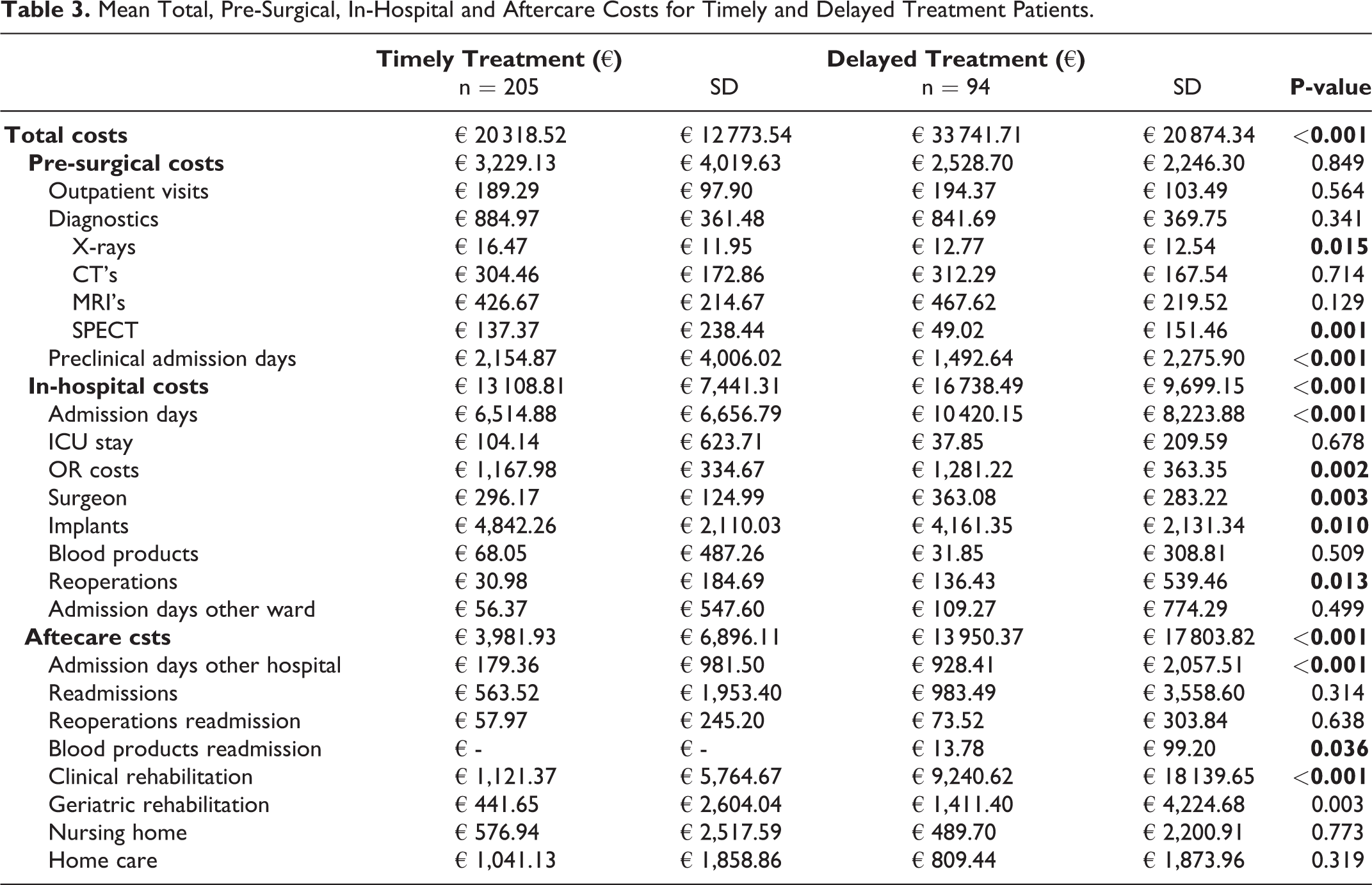
The results of the cost-analyses are listed in Table 3. The exact duration of could not be found in 19% of patients requiring clinical rehabilitation and 43% of patients requiring geratric rehabilitation. The mean total costs for timely treated patients was significantly lower compared with patients undergoing delayed treatment (€20.318,52 vs. €33.741,71, p < 0.001). Pre-surgical costs were higher in the timely treated group (€3.229,13 vs. €2.528,70, p = 0.849). The mean outpatient costs for conventional radiograph, SPECT-scans and costs associated with pre-surgical admission days in a different hospital were significantly higher in timely treatment. The in-hospital costs were significantly lower in the timely treated group (€13.108,81 vs. €16.738,49, p < 0.001). The in-hospital cost differences were mainly caused by differences in the costs of admission days. Timely treated patients averaged €6.514,88 for 10 days LOS vs. €10.420,15 for 16 days LOS in patients undergoing delayed treatment (p < 0.001). In contrast, the implants used in timely treated patients were significantly more expensive compared with the implants used in delayed treated patients (€4.842,26 vs. €4.161,35, p = 0.010). The aftercare costs were significantly lower in timely treated patients (€3.981,93 vs. €13.950,37, p < 0.001). The largest difference was found in the clinical rehabilitation, which averaged €1.121,37 in timely treated patients and €9.240,62 in delayed treated patients (p < 0.001).
Mean Total, Pre-Surgical, In-Hospital and Aftercare Costs for Timely and Delayed Treatment Patients.
Discussion
This cost-analysis study is the first to compare costs for delayed versus timely surgical treatment of patients with symptomatic spinal metastases. The current study shows that costs associated with timely treatment are significantly lower compared with costs of delayed treatment, confirming our hypothesis of the multiple benefits of timely treatment in patients with symptomatic spinal metastases. The results from this study can serve as encouragement for investing in referral patterns, thereby increasing patient outcome without necessarily increasing the associated costs.
Costs for emergency treatment compared with elective treatment has been previously studied outside the field of spinal surgery.20,21 In a study by Haider et al., the mean costs for emergency surgery in several different procedures (i.e. abdominal aortic aneurysm repair and coronary artery bypass graft) were on average € 6.756,71 higher than costs for the same elective procedures (using US Dollars to Euro exchange rate of € 0.91 508 in June 2015). 20 Similarly, Jestin et al. showed a relative cost increase of 50% for patients undergoing emergency surgery compared with elective surgery for colonic cancer. 21 In line with our findings, the biggest contributor to the cost difference observed by Jestin et al. was increased LOS.
Several previous studies investigating costs specifically in metastatic spinal disease show that overall the in-hospital costs are the biggest contributor to total costs.22,23 Likewise, in the current study the in-hospital costs account for approximately half the total costs (54% in timely treatment, 45% in delayed treatment). A previous study by Turner et al., investigating costs associated with surgical treatment for spinal metastases, has shown that the mean in-hospital costs for treatment in patients with confirmed symptomatic spinal metastases was €23.669,39 (using UK pounds to Euro exchange rate of € 1.3866 in June 2015). 23 In our study, the mean in-hospital costs for all patients were considerably lower at €14.249,91. The biggest difference between the current study and the study by Turner et al. can be found in OR-costs (€1.203,58 vs. €5.804,85). Furthermore, Turner et al. investigated several factors not included in the current study, such as imaging during admission, pathology and pharmacy costs. However, the authors of this study assumed that such factors would not be unequally distributed between timely and delayed treatment and therefore would not have changed the conclusions of the current study.
The present study is the first to compare total costs of delayed versus timely treatment in patients requiring surgical treatment for spinal metastases. The results clearly show that treatment delay of patients with spinal metastases leads to considerably higher costs. In accordance with previous studies reporting on unfavorable surgical outcomes and lower Quality of Life (QOL), functional status and survival, the need to prevent delayed surgical treatment is further emphasized.13,14,24,25 By investing in a catchment area’s referral chain, for instance by introducing a “hotline” or a multidisciplinary treatment system, the proportion of patients undergoing delayed treatment may decrease, thereby reducing the in-hospital and aftercare costs.26,27 In the current study, the pre-clinical costs were higher (albeit non-significant) for timely treated patients, strengthening the idea that a relatively limited investment at the beginning of the referral chain will lead to considerably lower in-hospital and aftercare costs. Similarly, using more advanced surgical techniques such as percutaneous pedicle screw fixation may lead to higher initial costs, as can bee seen in Table 3. Nonetheless, the subsequent favorable outcomes, such as decreased risk of complications, reduced LOS and a better overall patient convalescence, will reduce costs later on substantially. 28 Finally, delayed treatment is also associated with lower pre-operative EQ-5D and KPS scores, which persist after surgery. 14 If costs were to be viewed in light of the associated increase in QOL (i.e. costs per Quality Adjusted Life Year (QALY)), the combination of better QOL and lower costs would reasonably yield much lower costs per QALY than delayed treatment. In other words, relatively limited (financial) investments, used to optimize the referral patterns within a spine center’s catchment area, may considerably reduce the overall pretreatment delay and increase patient outcome, leading to better clinical outcomes at lower costs.
The current study has several limitations. Firstly, due to the retrospective nature, not all aspects of treatment could be considered for the current study. For example, extra costs for the treatment of complications were not included. As increased LOS is associated with a higher complication rate, the associated costs would likely have predominantly emerged from the delayed treated group. 29 Extra costs for paramedic treatments, such as physical therapy, ergotherapy or dieticians, were not considered but expected to be equally present in both treatment groups as they are included in the treatment protocol. Radiotherapeutic treatment, which is commonly provided for most patients within our spine center, was not included in the current analyses. Because delayed treated patients generally have an inferior functional status and lower life expetancy, it may be hypothesized that the type of radiotherapeutic treatment after delayed treatment is generally less complex and therefore less expensive. In some cases, assumptions were required to estimate actual costs. For instance, only the number of involved caregivers was known and a single contact-moment per caregiver was assumed. Moreover, the duration of (geratric) rehabilitation was not always available and in some cases the standard duration of 6 weeks had to be assumed. Finally, aftercare was only assessed up to 3 months postoperatively. Timely treatment, with higher chances of good outcome, may subsequently lead to a longer life-expectancy. 30 Costs and contributions of these patients for society in the long-term were not considered in the current study. Presumably, the societal costs incurred after this 3-month period are higher for delayed treatment, but the duration of survival and its impact on societal costs may be higher in timely treatment.
A strength of the current stud is that the costs were calculated manually by separately assessing all aspects of care rather than using invoiced prices. Therefore, the data in the current study is presumably more accurate than when using reimbursement tariffs. Moreover, this means the data can be applied in different countries when costs are adjusted for local tariffs.
In conclusion, costs are significantly lower in timely treatment compared to delayed treatment for patients with spinal metastases. These findings emphasize the importance of efficient referral patterns and rapid diagnosis and treatment for patients with spinal metastases. Investing in the pre-surgical trajectory, ensuring timely referral, diagnosis and treatment, may result in better outcome at lower overall costs for treatment of spinal metastases. Further research is necessary to determine how referral patterns can be improved, (e.g. investing in early imaging in patients with back pain and a history of malignancy, setting up a multidisciplinary outpatient clinic etc.). In this way, outcome for patients with metastatic spinal disease can be improved while decreasing the associated costs.
Footnotes
Acknowledgment
The authors would like to thank DePuy Synthes for providing the educational grant for the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current work was funded by an educational grant provided by DePuy Synthes (Johnson & Johnson).