
Abstract
Study Design
A Retrospective Study
Objective
To determine the prevalence and characteristics of DISH using whole spine CT scans and to evaluate the association of DISH with co-morbidities and other ossified lesions.
Method
A retrospective study of whole-spine CT scans of polytrauma patients from 2018-2021 above the age of 20 years. The screening was done using modified Resnick criteria. Overall and age-specific prevalence, characteristics, and associations with obesity, diabetes mellitus (DM), ischemic heart disease (IHD), aortic calcification (AC), ossified posterior longitudinal ligament (OPLL), and ossified ligamentum flavum (OLF) were evaluated.
Results
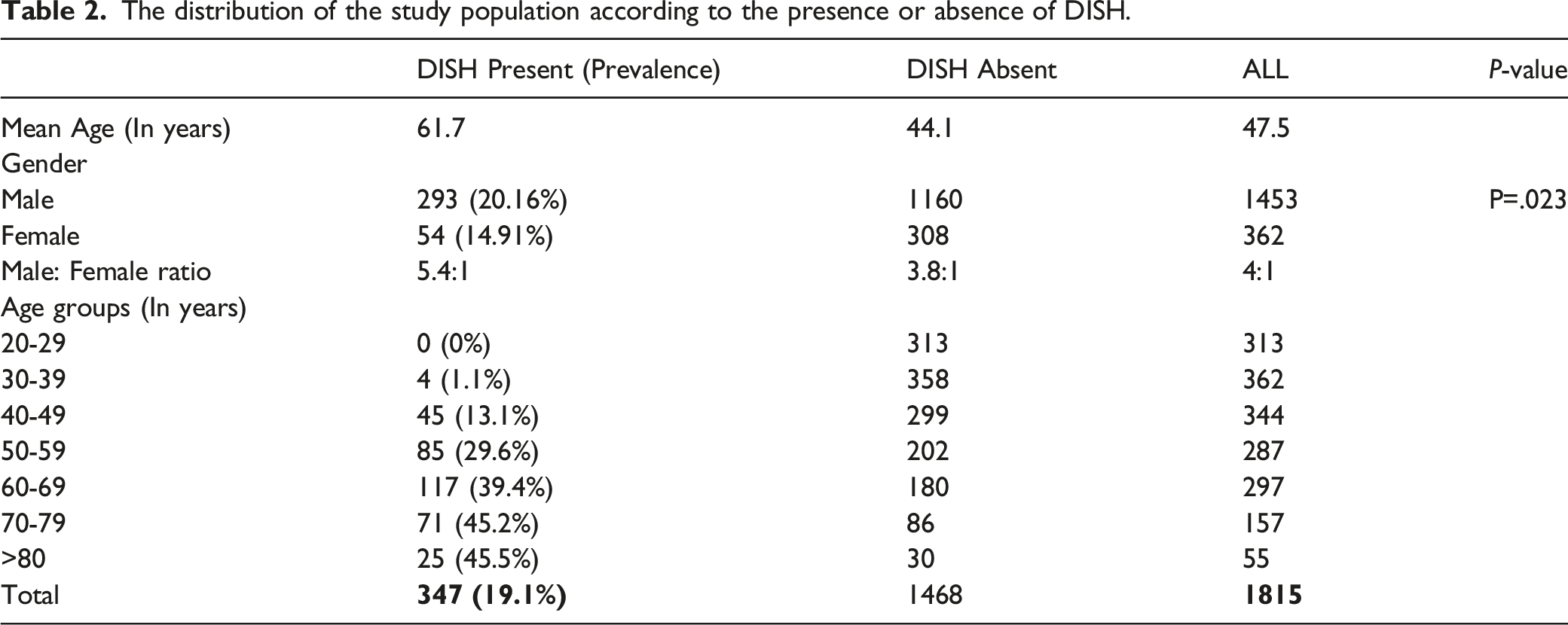
Out of 1815 patients, 347 had DISH, with a prevalence rate of 19.1% and a mean age of 61.7 years. The highest prevalence of DISH was seen in individuals over 80 years of age (45.5%). The prevalence among males (20.2%) was higher than for females (14.9%). The most commonly involved level was T8-T9 (95.4%), followed by T9-T10 (91.9%), and the most common vertebra involved was T9 (96%). All the cases involving T9 had ossification on the right anterior aspect of the vertebral body. The presence of DM, high BMI, and IHD was found to be significantly higher in patients with DISH (P value < .001). The incidence of aortic calcification was 22.5%, OPLL was 13.3%, and OLF was 4.9% in patients with DISH.
Conclusion
This study reports a prevalence rate of 19.1% for DISH, with the highest prevalence among individuals above 80 years of age (45.5%). DISH has a higher propensity to affect the right anterior aspect of the vertebral body in the thoracic spine and is strongly associated with obesity, DM, IHD, and AC.
Keywords
Introduction
Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a systemic non-inflammatory musculoskeletal disorder characterized by progressive ossification of the anterior longitudinal ligament and peripheral enthesis 1,2. DISH has been documented in the fossil remains of dinosaurs of the Mesozoic era and the mummies of Egyptian pharaohs 3,4. Although the term DISH was coined by Resnick in 1975, it was first described by Forestier et al in 1950 1,2. Ossifications in DISH have been classically described as flowing ossification along the ventrolateral aspect of at least three contiguous vertebral levels or four contiguous vertebrae 5 . DISH most commonly involves the thoracic spine, followed by the cervical and lumbar regions 2,6–8.
The exact etiopathogenesis of DISH is not fully understood, but several factors like metabolic, genetic, environmental, and mechanical have been implicated 9,10. It is a disease of the elderly population and is usually associated with various metabolic disorders like diabetes mellitus (DM), obesity, hyperinsulinemia, and atherosclerosis2,11–13. DISH can be asymptomatic, an incidental finding on radiographs, or may present with radiculopathy, myelopathy, restricted spine movements, dyspnoea, or dysphagia 6,14–17. The ankylosis of the adjoining spinal segments alters the biomechanics of the spine and makes an affected individual susceptible to spine fractures 17 .
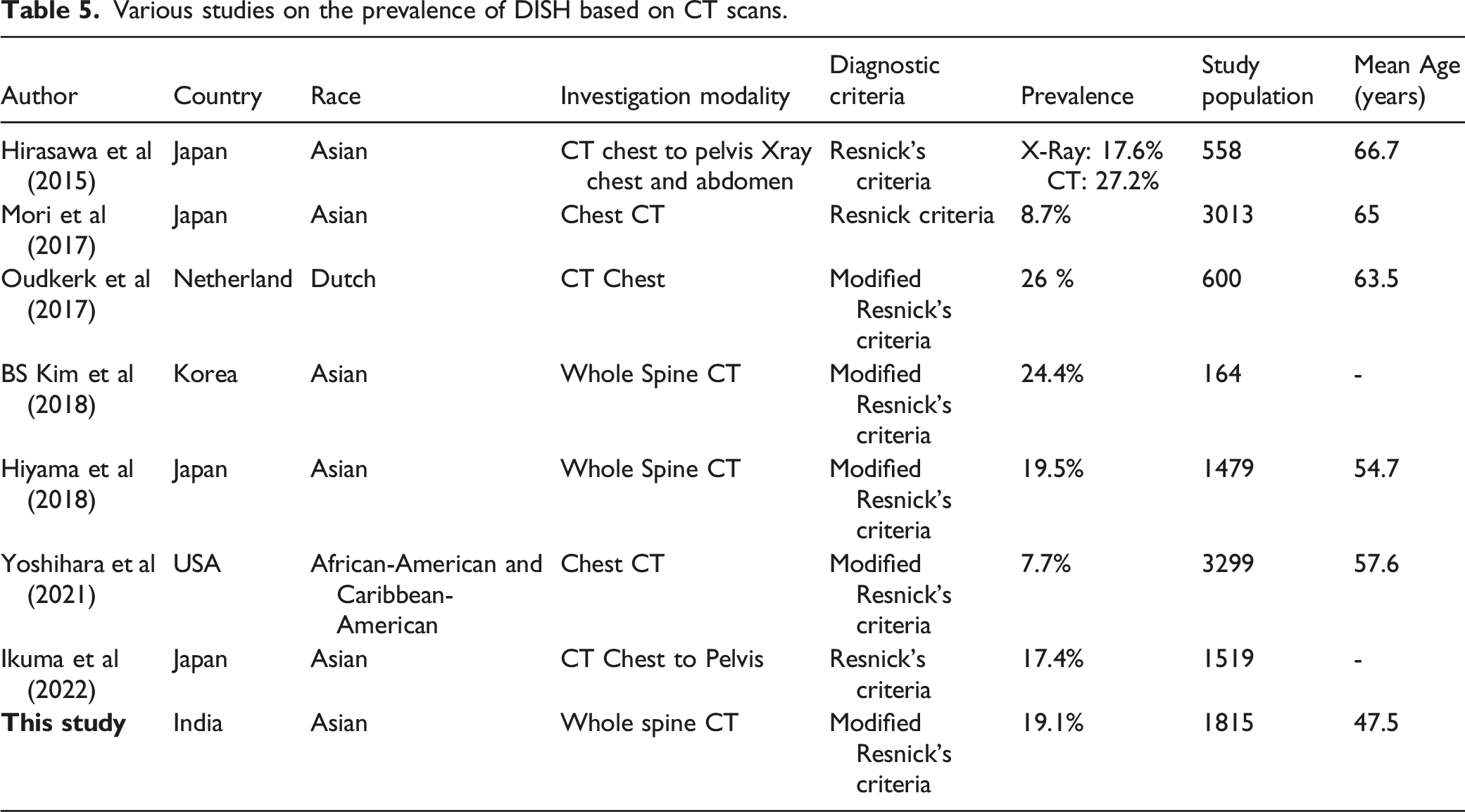
Using chest radiographs, DISH's prevalence has been reported to be 2.9% in Asians, 3.9% in Africans, and 17% in Caucasians 7,18,19. The visualization of DISH on plain radiographs is limited by the overlap of the shoulder and ribs, hence computed tomography (CT) scans are preferred. Studies using CT scans have reported a prevalence of 19.5% in Japanese, 24.4% in Koreans, and 7.7% in the African American population 8–10.
The prevalence of DISH in the Indian population has not been studied so far. The current study is a cross-sectional survey in the local geographic sample of the Indian population to determine the prevalence of DISH based on the whole spine CT scan using Modified Resnick criteria 20 . The study also aims to look for characteristics of DISH, its association with ossified posterior longitudinal ligament (OPLL), ossified ligamentum flavum (OLF), aortic calcification (AC), and systemic disorders like diabetes mellitus (DM), obesity, and ischemic heart disease (IHD).
Material and Methods
A cross-sectional single institute study was conducted after obtaining institutional review board approval (Ganga Medical Centre & Hospital Pvt Ltd Institutional Review; IRB Application No: 2021/07/12). Skeletally mature polytrauma patients (>20 years) who underwent whole spine CT scans from 2018-2021 were enrolled in the study. Because our analysis was a retrospective study based on CT, we were exempt from obtaining informed consent.
Sample Size
We calculated the required sample size based on the assumption of a prevalence rate of 19%. Considering the level of confidence to be 97% and the allowable error of 2%, which resulted in a requirement of at least 1815 participants. A sample size (N) was calculated using the formula
21
Radiographic Assessment
A Siemens Emotion 6 slice CT system was used and a whole spine CT scan was performed. The scan acquisition went from the head to the whole pelvis. PACS (Picture Archiving and Communication System) software was used to analyze the sagittal, axial, and coronal plane images. All images were evaluated by an orthopedic resident and spine fellow and reviewed by a senior spine surgeon. An intra-observer agreement was determined.
The diagnosis of DISH was made based on the modified Resnick’s Criteria proposed by Oudkerk et al
20
, which includes 4 items: (1) Anterior bridging ossification (Flowing ossification) with involvement of a minimum of 4 contiguous vertebrae or 3 contiguous disc levels, (2) CT scan images with fixed bone settings to prevent errors (false positive and false negative cases), (3) More than 900 angles formed by osteophytes in relation to the vertebral body, (4) Absence of severe degenerative disc changes. (Figure 1) A case of DISH involving thoracic and lumbar segments of the spine. (A) Sagittal Images showing flowing ossification extending from T3 level to L2 and also ossification over lower lumbar vertebral bodies which are not bridging. (B) Coronal images showing ossification over right side of the thoracic spine.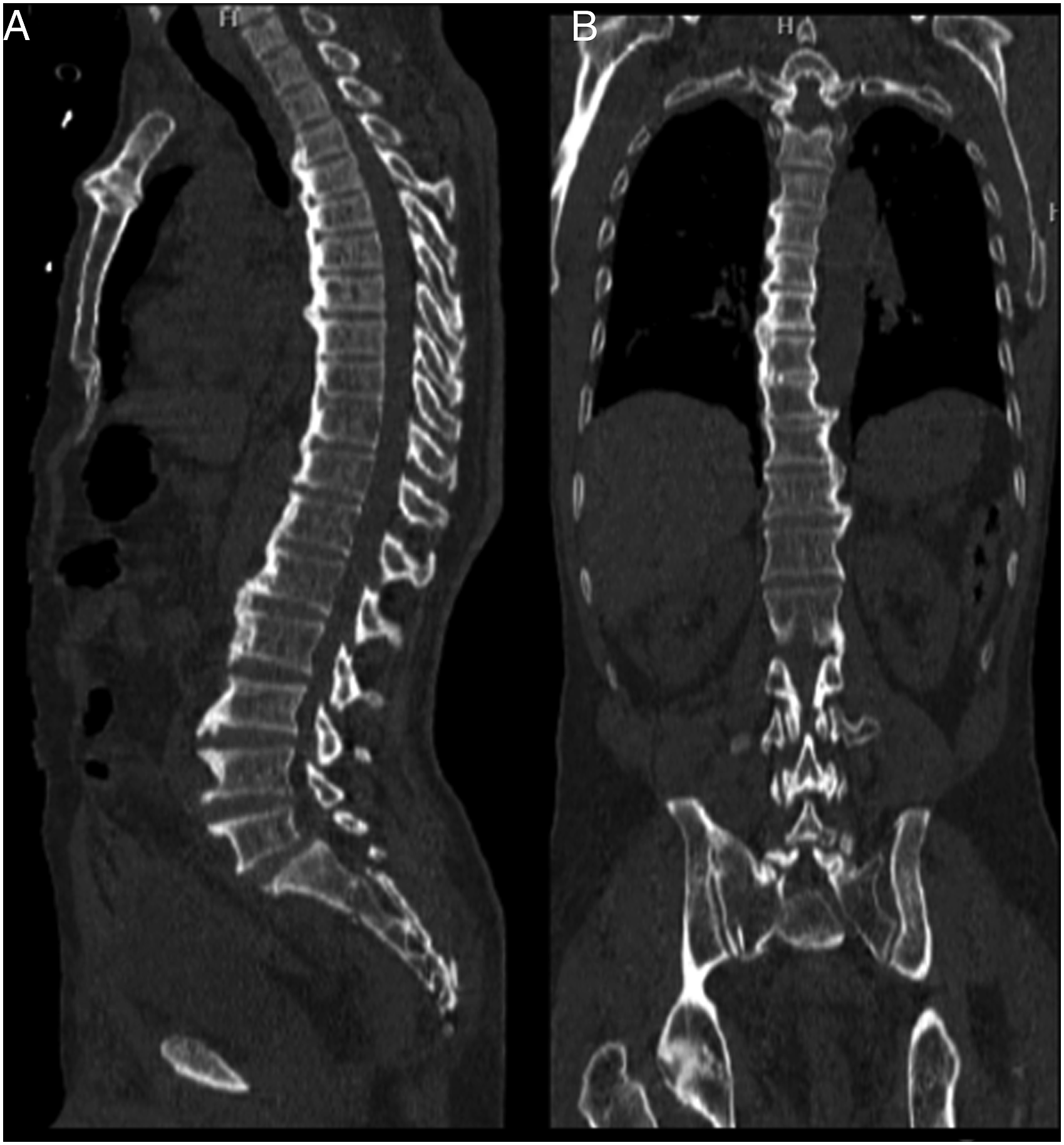
Patients who fulfilled these criteria were considered DISH positive. These patients were further evaluated for characteristics of DISH, the incidence of the ossified posterior longitudinal ligament (OPLL), ossified ligamentum flavum (OLF), aortic calcification (AC), and association of co-morbidities like DM, obesity (high BMI), and IHD were analyzed. Demographic details and data on comorbidities were collected from hospital information software and patient records.
According to the location in which ossification was observed, DISH was classified into six types
9
: 1.Cervical – Ossification only in the C1-C7 segment 2.Cervicothoracic – Ossification in the C1-T12 region 3.Thoracic – Ossification in the T1-T12 segment 4.Thoracolumbar – Ossification in the T1-L5 region 5.Lumbar – Ossification only in the L1-L5 segment 6.Whole spine – Ossification involving C1-L5
Statistical Analysis
SPSS version 26 was used for statistical analysis. The level of significance was set at 5%, so P-values of less than .05 was considered statistically significant. Descriptive statistical analyses were done, and categorical measurements were presented as percentages.
Results
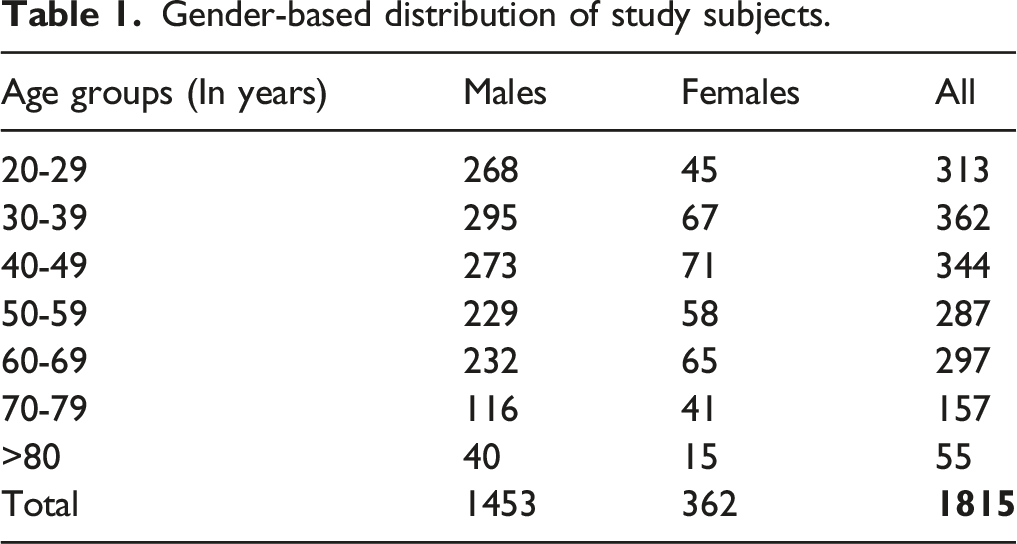
Gender-based distribution of study subjects.
DISH Prevalence and Morphology
The distribution of the study population according to the presence or absence of DISH.
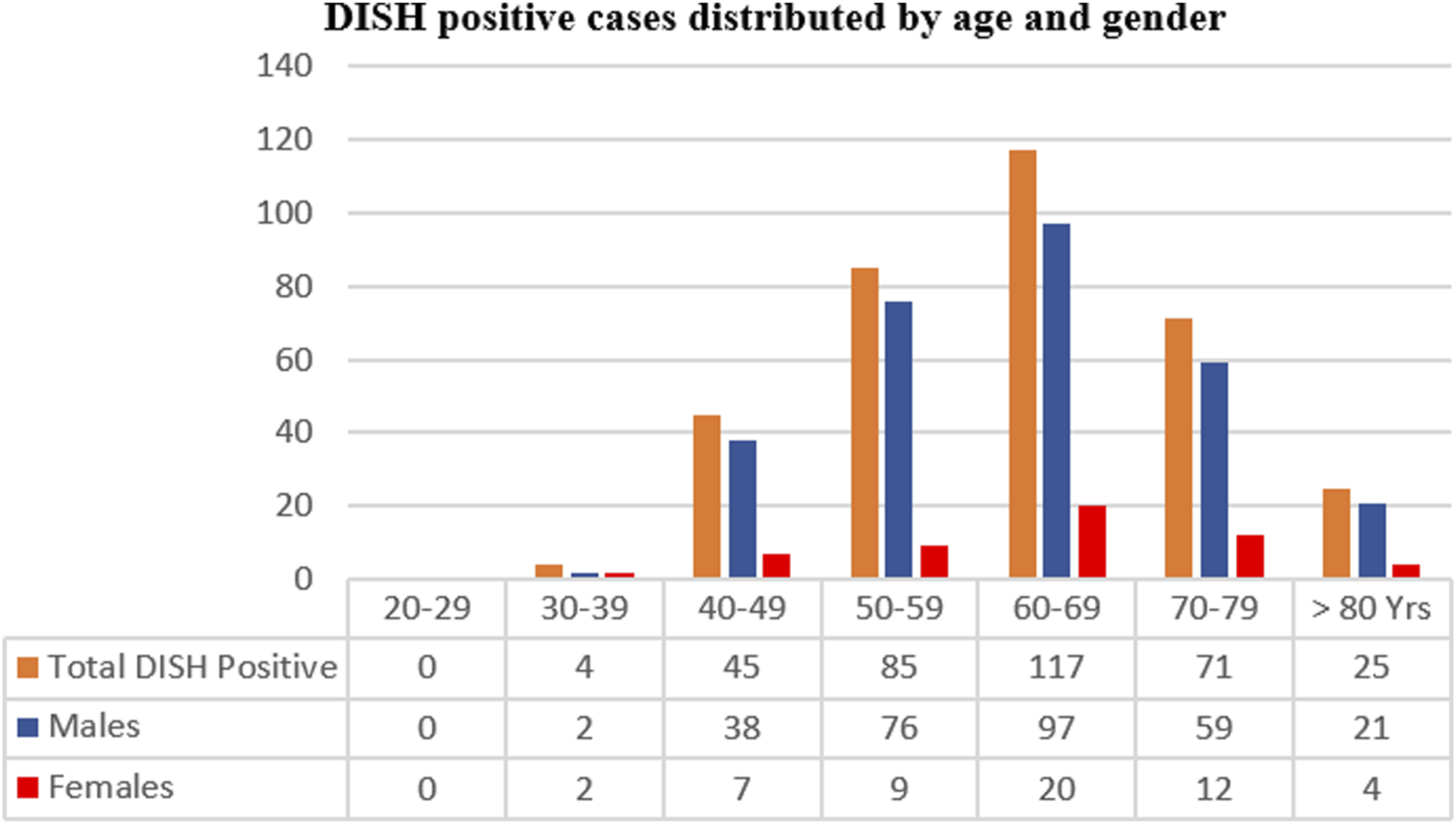
DISH age and gender distribution.
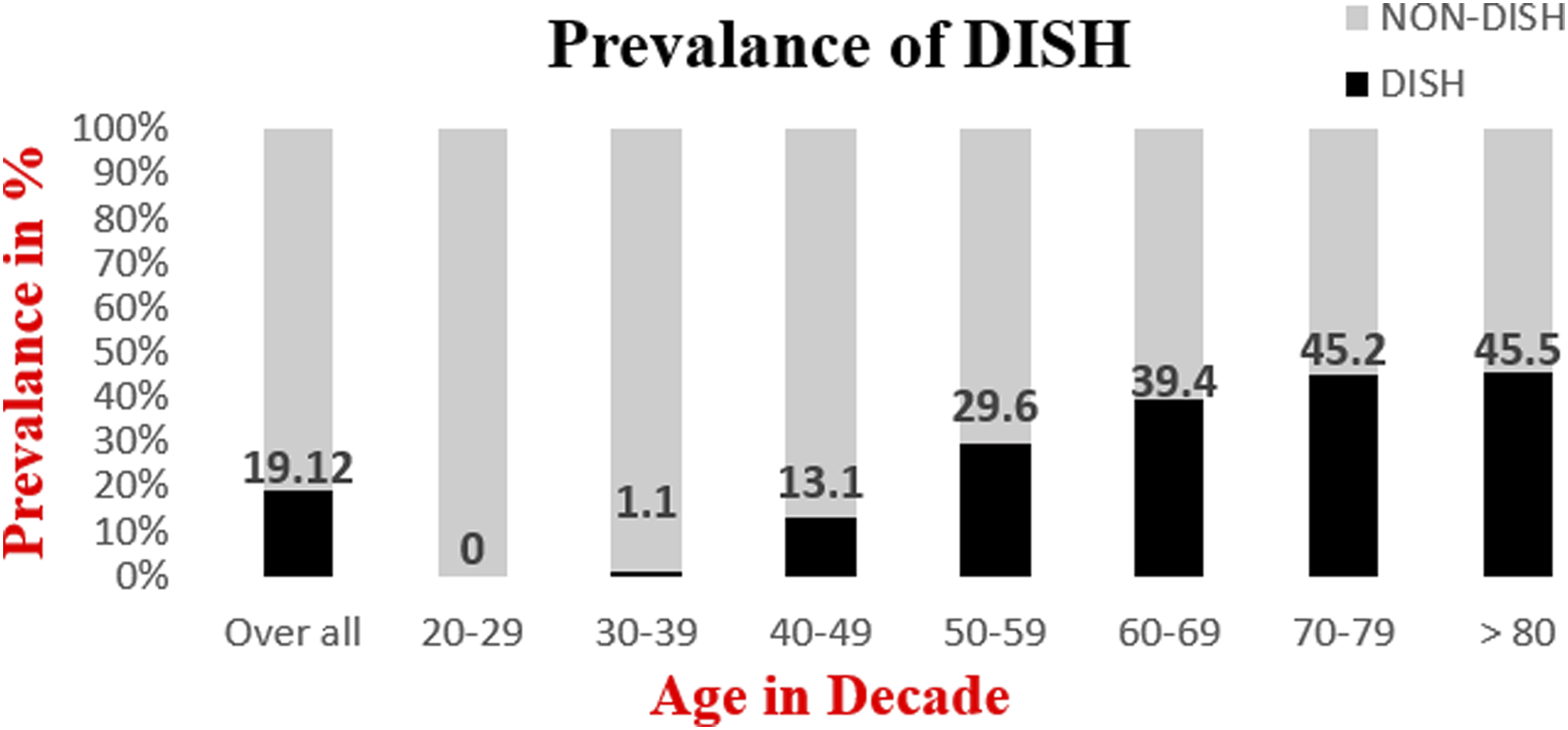
Overall and age-specific prevalence of DISH.
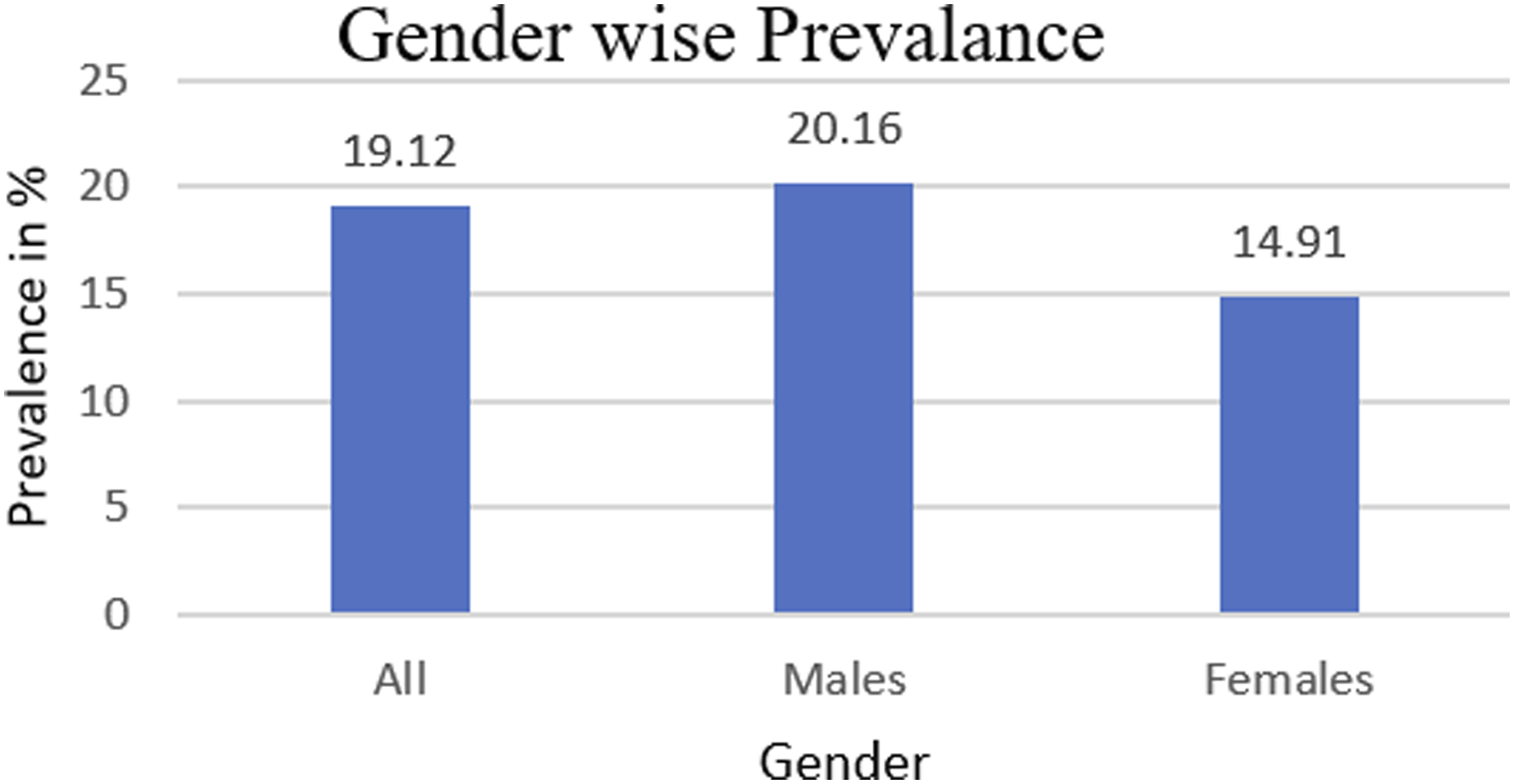
DISH prevalence in males and females.
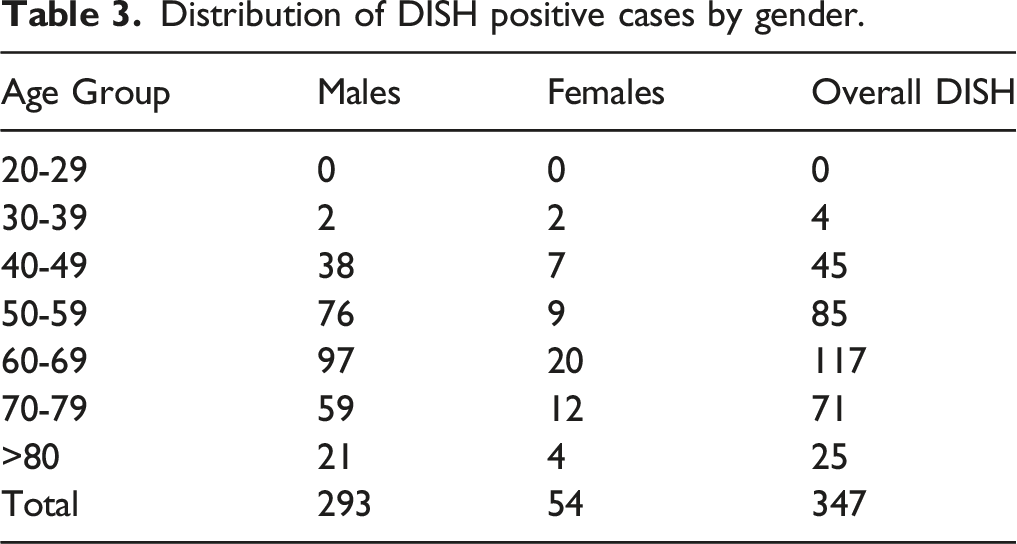
Distribution of DISH positive cases by gender.
Distribution of DISH
We found that the most common segment involved in DISH was the thoracic spine (245 of 347, 70.6%), followed by the equal involvement of the thoracolumbar spine (38 of 347, 10.9%) and the whole spine (38 of 347, 10.9%). Ossification in the cervical or lumbar region was always associated with ossification in the thoracic region (Figure 5). DISH distribution based on spinal segment involvement.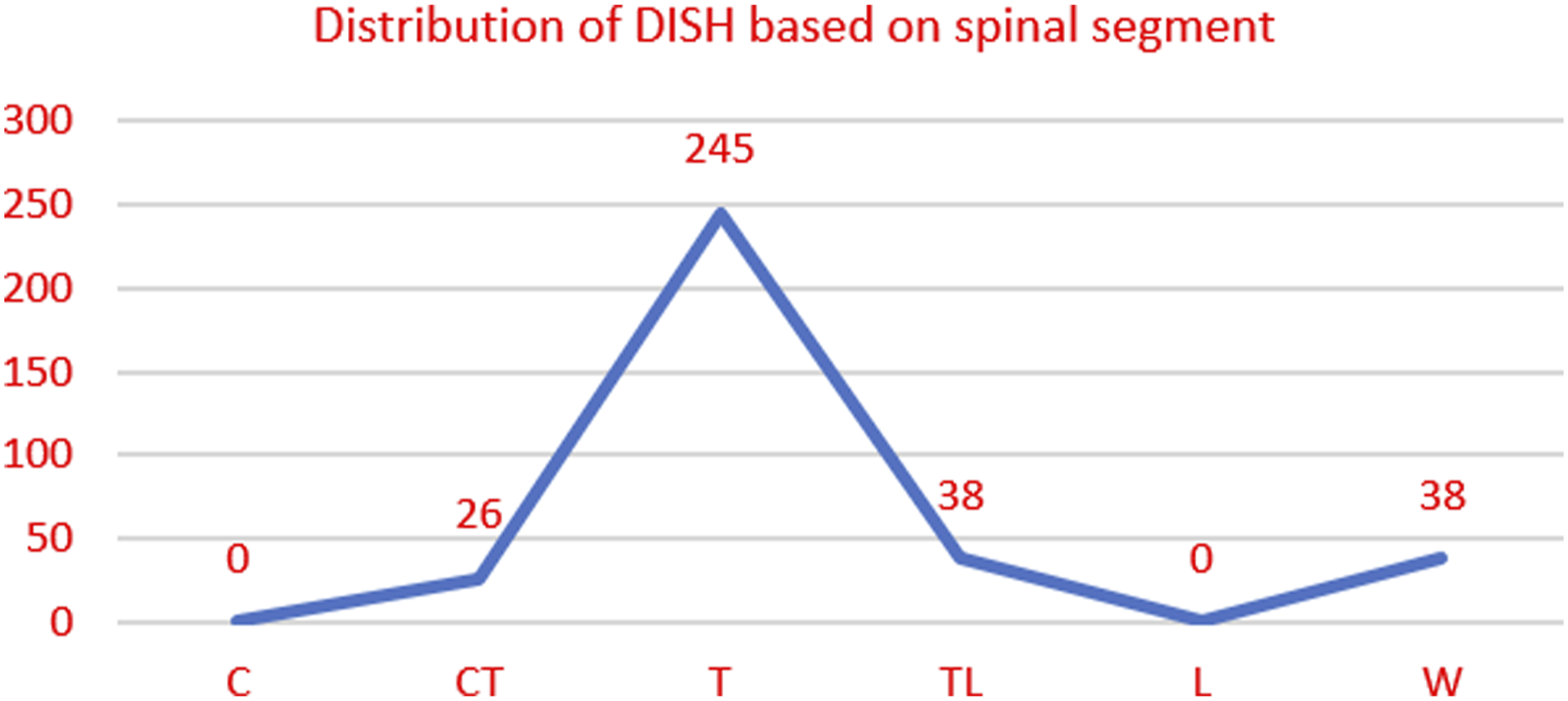
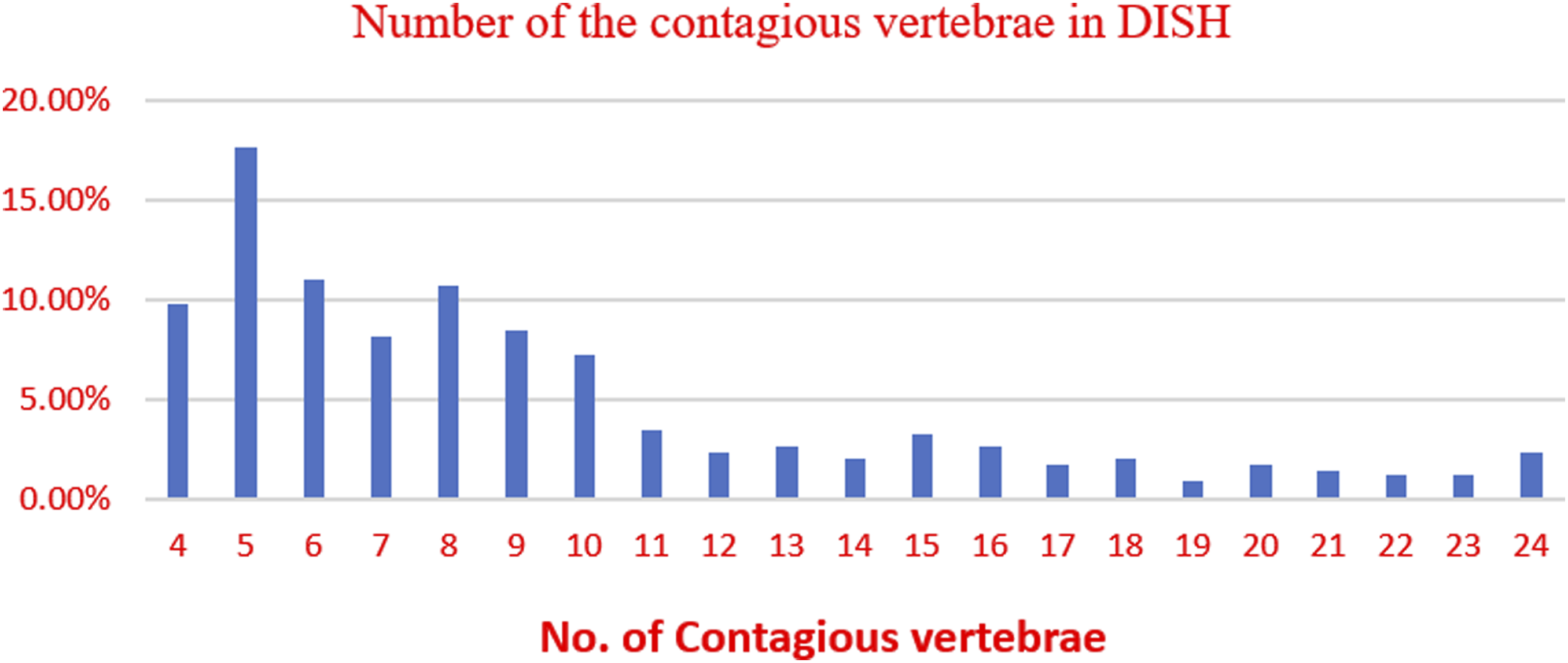
It was observed that the most frequent level involved was T8-T9 (331/347, 95.4%) followed by T9-T10 (319/347, 91.9%) and the most common vertebra involved was T9 (333 of 347 cases, 96%) followed by T8 (327 of 347, 94.2%) and T10 (313 of 347, 90.2%). The most frequent number of contagious vertebral segments affected was five (17.6%), followed by six (11%) and eight (10.7%), while the average number of vertebral bodies bridged continuously was 9.2. The distribution based on inter-vertebral level and the number of contagious vertebrae is shown in Figures 6 and 7, respectively. DISH Distribution based on Level of the spine involved. Number of the contagious vertebrae involved in DISH.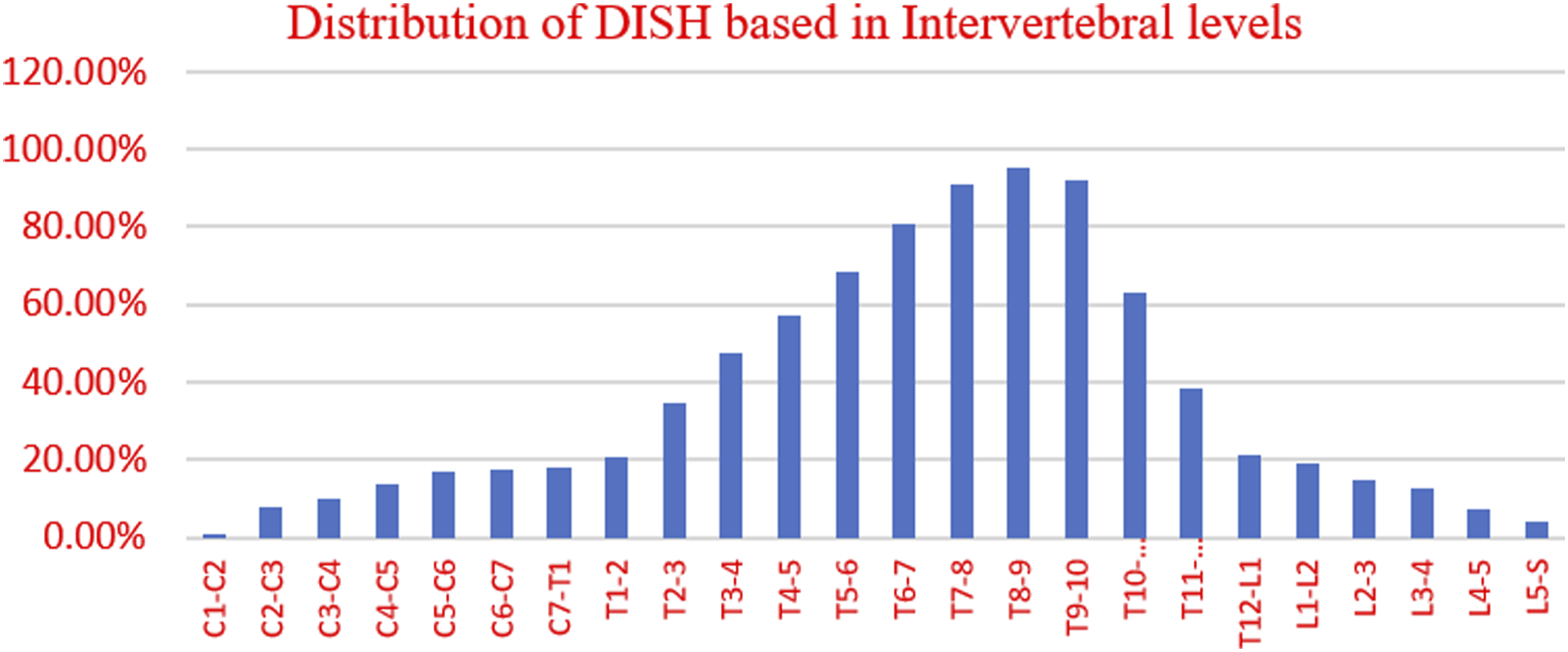
Location of DISH on Axial CT Images
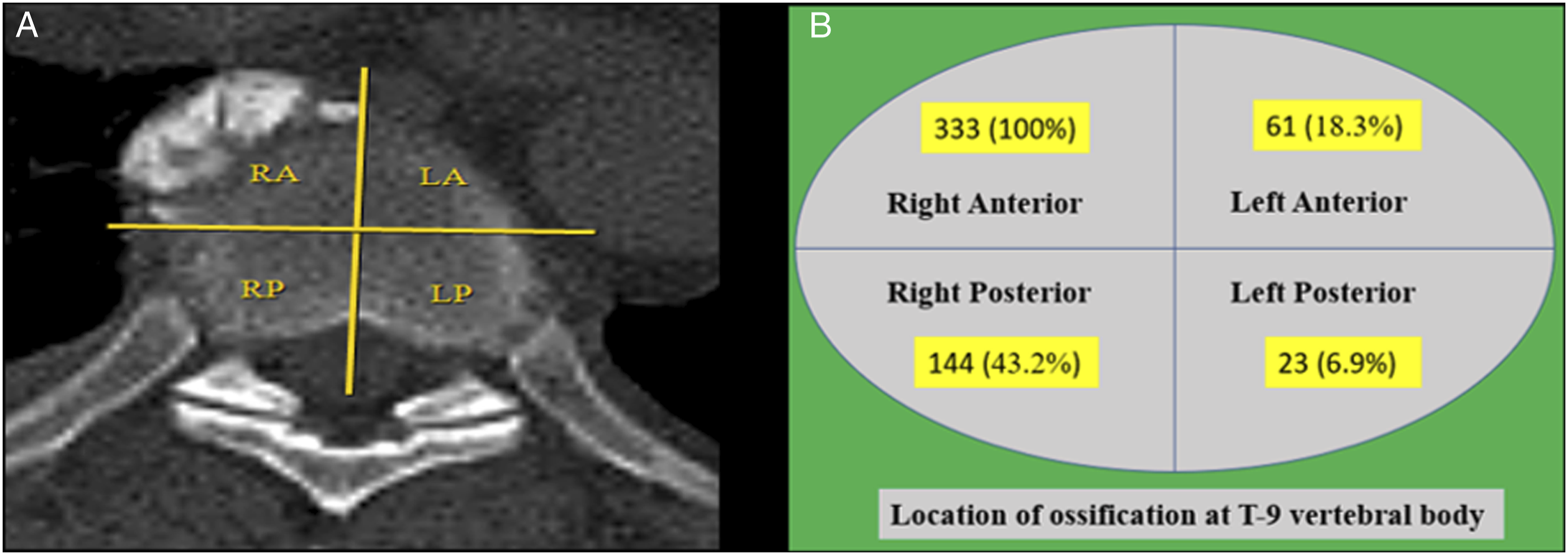
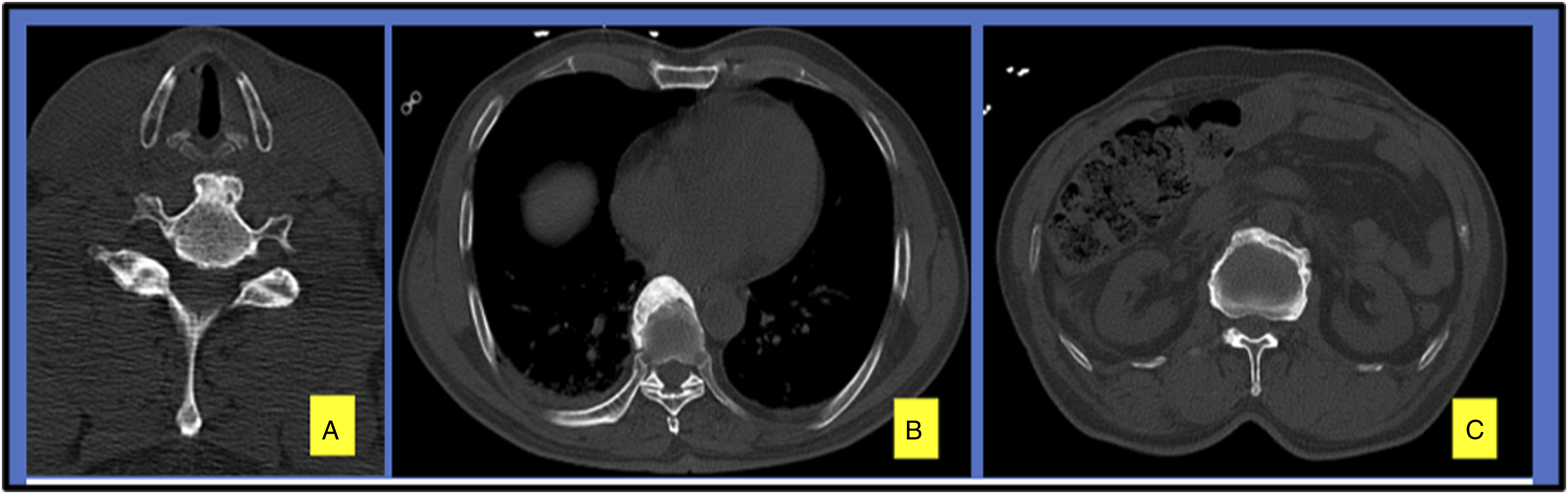
i. Thoracic spine: T9 vertebra being most commonly involved was used as the reference for the Thoracic spine DISH, and the anterior aspect of the vertebral body was divided into 4 areas (Figure-8a). All the cases involving T9 had ossification over the right anterior area (333 of 333, 100%), followed by the right posterior (144 of 333 cases, 43.2%), left anterior (61 of 333 cases, 18,.3%) and left posterior areas (23 of 333 cases, 6.9%) (Figures 8A, 8B, and 9B). ii. Cervical spine: In all the patients with DISH involving the cervical spine, ossification was noted over the anterior aspect of the vertebral body along the midline (Figure 9A). iii. Lumbar Spine: Ossification in the lumbar spine was seen on the entire anterior aspect of the vertebral body (Figure-9c). (A) An axial image of the T9 vertebral body divided into 4 areas shows ossification over the right anterior area of the vertebral body. (B) Statistical information demonstrating DISH ossification at the T9 vertebral body. Images depicting the location of ossification in the cervical spine (A), thoracic spine (B), and lumbar spine (C).
Co-Existence of OPLL, OLF, and Aortic Calcification
Aortic calcification was significantly higher in patients with DISH (78 of 347 cases, 22.5%) than without DISH (43 of 1468 cases, 2.9%) (P-value < .001). OPLL was found in 13.26% (46 of 347 cases) of patients, while OLF was seen in 4.9% (17 of 347) of patients with DISH (Figure 10). Concomitance of other ossified lesions in DISH.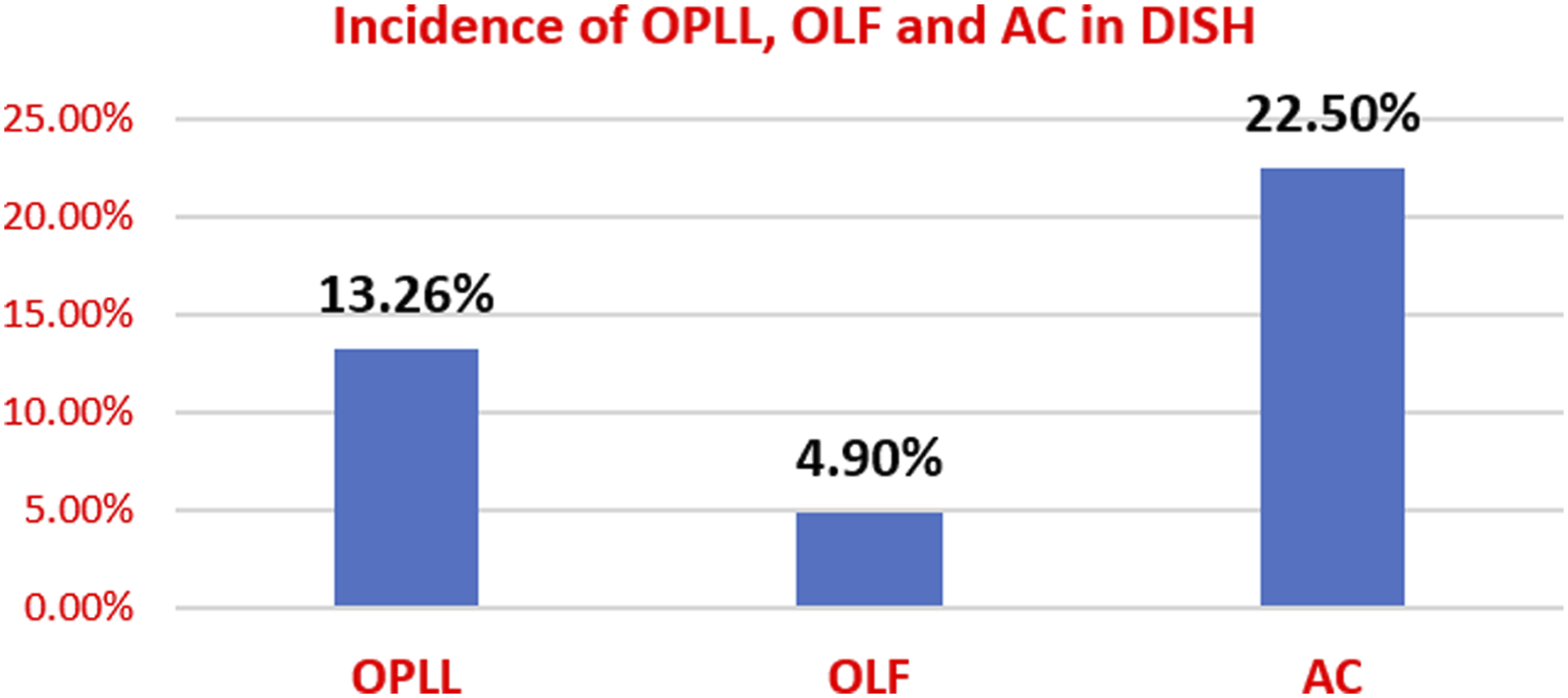
Co-Morbidities With DISH
Of the 1815 patients included in the study, data concerning the medical comorbidities of 1674 (92.2%) patients was available in the hospital records. These patients were further grouped into: i. Group I (Patients with DISH) - consists of 317 patients. ii. Group II (Patients without DISH) - consists of 1357 patients.
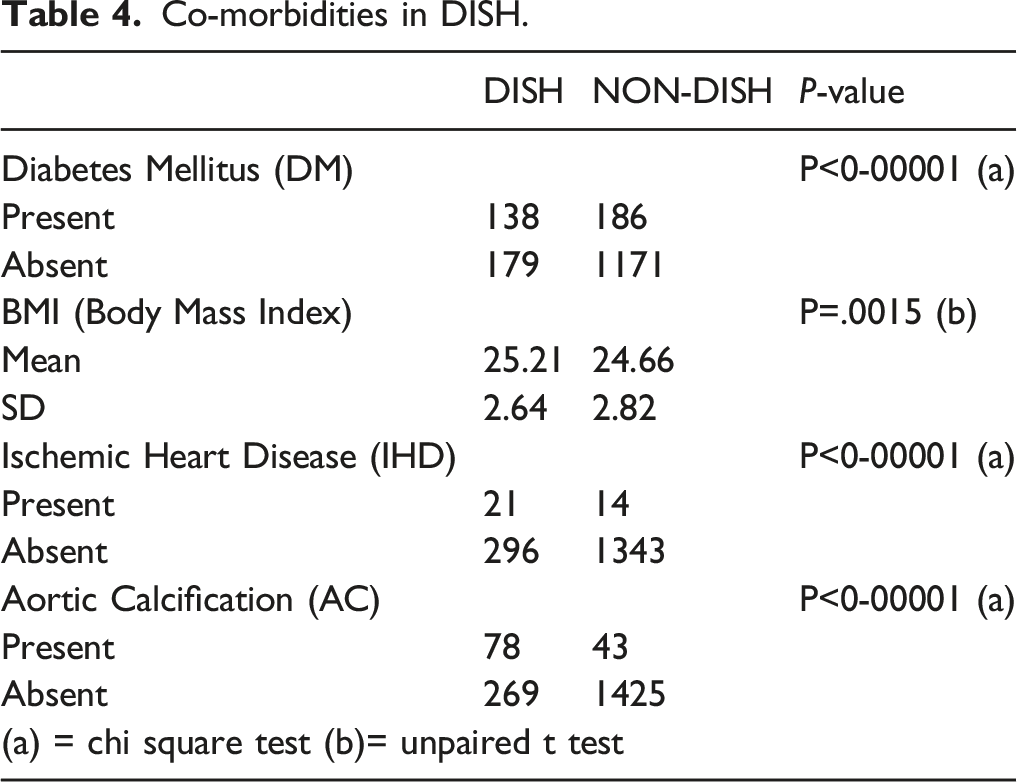
Co-morbidities in DISH.
Discussion
Diffuse idiopathic skeletal hyperostosis (DISH) is a noninflammatory condition predominantly affecting the spine and characterized by ossification of the anterior longitudinal spinal ligament and entheses 11 . DISH is predominantly a disease of the elderly and is rarely diagnosed in middle age. The prevalence of DISH may be determined by a variety of factors, such as patient age, genetic and ethnic diversity, diagnostic imaging techniques, and lifestyle habits 9 .
Various studies on the prevalence of DISH based on CT scans.
DISH is more prevalent among males with male/female ratios ranging between 2:1 and 7:1 7,23. Weinfeld et al reported a DISH prevalence of 25% and 15% in males and women, respectively, after analyzing 2300 individuals 22 . In a population-based survey of Hungarians, Kiss et al found that DISH prevalence was 27.3% in males and 12.8% in women, respectively 25 . Julkunen et al reported a prevalence of DISH in 3.8% of males and 2.6% of women in the general Finnish population 23 . In a cohort of patients in the Netherlands, Westerveld et al more recently found a 17.0% prevalence of DISH 19 . In our study, the reported prevalence of DISH was 20.2% in males and 14.9% in females.
DISH is a disease in the elderly population. The age of the study population definitely affects the prevalence rate. Most previous studies included a population above 40 years with an average of 65 years 7,18,19,22,24, whereas in our study we included subjects above 20 years with a mean age of 47.5 years, which will reflect a more accurate prevalence rate. The prevalence of DISH increased with age and the highest prevalence was seen above 80 years (45.5%), followed by the 70-79 years group (45.2%).
The thoracic spine is the most common location for DISH. According to Hiyama et al, the majority of the ossification took place in the middle and lower thoracic spine, particularly at T8 (88%), T9 (91%), and T10 (85%) 9 . DISH was also reported to often occur at T7-10 by Hirasawa et al and Kagotani et al 24,26. According to Hirasawa et al 24 , more than 80% of DISH occurred at T8/9 or T9/10, which may indicate an anatomical effect. Because T8 is virtually at the top of the physiological spinal kyphosis, these vertebrae are vulnerable to compressive mechanical stress. In the thoracic spine, DISH has the propensity to occur over the right anterior portion, opposite to the pulsating aorta. In the cervical spine, ossification is seen along the midline of vertebral bodies as carotid artery pulsation on both sides is thought to protect against the development of ossification over the lateral aspect. In the lumbar spine, diffuse involvement of the anterior aspect of the vertebral body is seen. As a result of mechanical stress, DISH appears to originate mostly from the thoracic spine and may extend to the cervical and/or lumbar spine. Our study demonstrated that T9 is the most commonly involved vertebra (333/347, 96%). On the axial CT image, the T9 vertebral body was divided into four areas to evaluate the location of ossification. We noted that all the cases involving T9 had ossification over the right anterior area (333/333, 100%) followed by the right posterior area, which was consistent with the results of Hiyama et al 9 .
As per the literature, several metabolic, genetic, and constitutional factors may be related to the condition, although their presence is not necessary to make the diagnosis of DISH. These, in particular, include obesity, a high waist circumference ratio, hypertension, diabetes, hyperinsulinemia, dyslipidemia, increased levels of growth hormone, elevated levels of insulin-like growth factor 1, hyperuricemia, and hereditary factors 6 . According to a study by Mader et al, people with DISH usually have metabolic syndrome, which increases their risk of cardiovascular morbidity 27 . In our study, DM was seen among 43.5% of individuals with DISH and 13.7% of individuals without DISH (P < .001). The mean BMI among the individuals with DISH was 25.21 ± 2.64 and in those, without DISH it was 24.66 ± 2.82 (P-value = .001), which reflected that a strong association is present between DISH and comorbidities like DM and high BMI, which is consistent with the studies by Fujimori et al 28 and Mori et al 17 . Studies done by Orden et al 29 and Pariente-Rodrigo et al 30 found a significant association between aortic sclerosis or calcification in DISH patients. In our study, we noted that aortic calcification was significantly higher in the patients with DISH (22.5%) than in those without DISH (2.9%) (P-value<.001), and history of IHD was present in 6.6% of individuals with DISH and in 1% of those without DISH (P-value<.001).
There were a few limitations to the current study. First, the study population was taken from a tertiary care center which created sample selection bias. Second, the polytrauma patients tended to be of a younger age group and were more likely to be males hence they might not represent the general population. Third, this was a retrospective study and we could not assess progressive changes in DISH due to the aging process, and data on insulin levels and lipid profile was not available, hence the association with hyperinsulinemia, and dyslipidaemia could not be derived. Fourth, the study does not provide a clinical correlation with ligament ossification. Despite the limitations, our study’s results revealed important epidemiological data regarding patients with DISH, its characteristics, and its association with medical co-morbidities and other ossified lesions.
Conclusion
The overall prevalence of DISH based on whole spine CT was 19.1%. The prevalence rate increases with age, with a higher preponderance among males. The most common spinal segment involved was T8-T9, while the most common vertebra involved was T9. In the patients with DISH, the incidence of OPLL was 13.3% and OLF was 4.9%. DISH was found to have a significant association with DM, obesity, IHD, and aortic calcification.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.