
Abstract
Study Design
Retrospective Case control Study.
Objectives
To analyze the effect of diffuse idiopathic skeletal hyperostosis (DISH) on the occurrence of new thoracolumbar vertebral fragility fractures (VFFs) at different ages.
Methods
A retrospective analysis of 564 patients, including 189 patients who presented with new-onset thoracolumbar VFFs and 375 patients without spinal fractures, was performed in 4 age groups (50-59 years, 60-69 years, 70-79 years, and 80+ years). DISH was diagnosed based on computed tomography findings, and the Mata score of each disc space level combined with the maximum number of consecutive ossified segments (MNCOS) for each patient was recorded. Data were compared between the fracture and control groups, and odds ratios (ORs) were calculated for each of the 4 age groups using logistic regression.
Results
Both the crude ORs and the adjusted ORs of DISH for VFFs decreased with age, with statistical significance shown in the 50-59 years group (crude OR = 4.373, P = 0.017; adjusted OR = 7.111, P = 0.009) and the 80+ years group (crude OR = 0.462, P = 0.018; adjusted OR = 0.495, P = 0.045). The Mata scores and the MNCOS were significant risk factors for VFFs (P < 0.05) in the 50-59 years group, but they were protective factors in the 80+ years group, which was more significant in the T11/12–L5/S1 subsegment.
Conclusions
The effect of DISH on the occurrence of thoracolumbar VFFs is complex, and in patients above 50 years, it changes from a risk factor to a protective factor with increasing age.
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a systemic disease characterized by ossification of ligaments and attachment points. 1 It has an estimated prevalence between 10% and 40%,2-5 depending on the classification criteria. Based on radiographic features, Resnick et al defined DISH as ossification and calcification of the anterior longitudinal ligament over 4 adjacent vertebrae, preservation of the intervertebral disc space, and absence of changes in the apophyseal or sacroiliac joints. 6 Many factors, including genetic, metabolic, hormonal, inflammatory, and signal transduction pathway derangements, have been implicated in its pathogenesis and mechanical influences.7,8 The prevalence of DISH is expected to increase in the coming decades as a result of longer life expectancy, combined with a worldwide increase in metabolic syndrome.
Due to altered spinal biomechanics caused by the formation of continuous bridges between vertebrae, DISH is thought to be positively associated with vertebral fracture prevalence even after a minimal injury, independent of the changes in bone mineral density (BMD) or other factors such as age, body mass index (BMI), diabetes status, and years of smoking.9,10 DISH leads to a 10-fold increased risk of unstable spinal fractures11,12 with longer length of hospital stay 13 and higher mortality. 14 A previous study reported a prevalence of 33.9% of DISH in patients with vertebral fractures. 13 Recently, several studies have investigated the impact of DISH on vertebral fragility fractures (VFFs).4,15-19 One of them showed that age and DISH were independently associated with an increasing prevalence of VFFs. 17 However, no significant differences in VFFs risk were found between DISH and controls in the cohorts of Pini et al,18,19 Katzman et al 4 and Diederichs et al. 16 This inconsistency highlights the complexity of the relationship between DISH and VFFs. Although DISH is an age-dependent condition and its prevalence rapidly increases with age, 20 age-related changes in the effects of DISH on VFFs remain largely unknown.
The first aim of our study was to observe the extent of DISH involvement and the degree of intervertebral ossification with age. The second aim was to investigate how DISH affects the occurrence of thoracolumbar VFFs at different ages, based on computed tomography (CT) scans.
Materials and Methods
This study was approved by the Ethics Committee of Zhejiang Provincial People's Hospital Approval NO.2023(158). The requirement for informed consent was waived by the Ethics Committee owing to the retrospective nature of the study.
Study Subjects
This retrospective study was conducted in Zhejiang Provincial People's Hospital. Through picture archiving and communication system (PACS), the study subjects were screened from all patients aged >50 years who underwent CT scan covering complete T1/2–L5/S1 intervertebral space levels at the radiology department from July 2019 to July 2021. We established a fracture group consisting of patients diagnosed with new-onset VFFs, and a control group consisting of patients without thoracolumbar spinal fractures based on the following inclusion and exclusion criteria.
The inclusion criteria for the fracture group were as follows: thoracolumbar spinal magnetic resonance (MR) scan suggesting the presence of new-onset VFF; CT scan within 15 days before or after the onset; BMD results within 15 days before or after the onset.
The inclusion criteria for the control group were as follows: BMD results within 1 year before or after the CT scan; and the patient did not develop a thoracolumbar VFF for at least 2 years after the CT scan, as confirmed by follow-up CT, MR, or telephone counseling.
The exclusion criteria for both the fracture and the control groups were as follows: long-term bedridden patients; patients with old spinal fractures; patients after spinal surgery; spinal malignant tumors, infections, ankylosing spondylitis, metabolic bone diseases other than osteoporosis; Significant scoliosis or vertebral slippage; poor image quality.
Initial subject selection was carried out by a radiologist with 10 years of experience, combined with the opinion of experts on the diagnosis of new-onset VFF. Eventually, a senior radiologist (20 years of experience) reviewed all of the included subjects.
Finally, for the fracture group, a total of 189 patients (137 females and 52 males) with acute VFFs were enrolled and divided into 4 groups according to the age at onset: 23 cases in the 50-59 years group, 50 cases in the 60-69 years group, 57 cases in the 70-79 years group, and 59 cases in the 80+ years group. Consecutive patients who had never had a spinal fracture were included in the control group, with approximately 2 patients selected for each patient from the appropriate age group of the fracture group (a total of 375 cases, including 46 cases in the 50-59 years group, 101 cases in the 60-69 years group, 114 cases in the 70-79 years group, and 114 cases in the 80+ years group). The reasons for CT scans in the control group were as follows: 21 for trauma, 98 for other acute conditions, 43 for chronic back pain, 157 for other chronic complaints, 31 for malignant tumor follow-up, and 25 for cancer screening. All imaging data were retrieved from PACS. The patients’ age, sex, weight, height, and BMD data were obtained from the hospital information system. The flowchart of patients selection and grouping is shown (Figure 1). Flowchart of subject selection and grouping.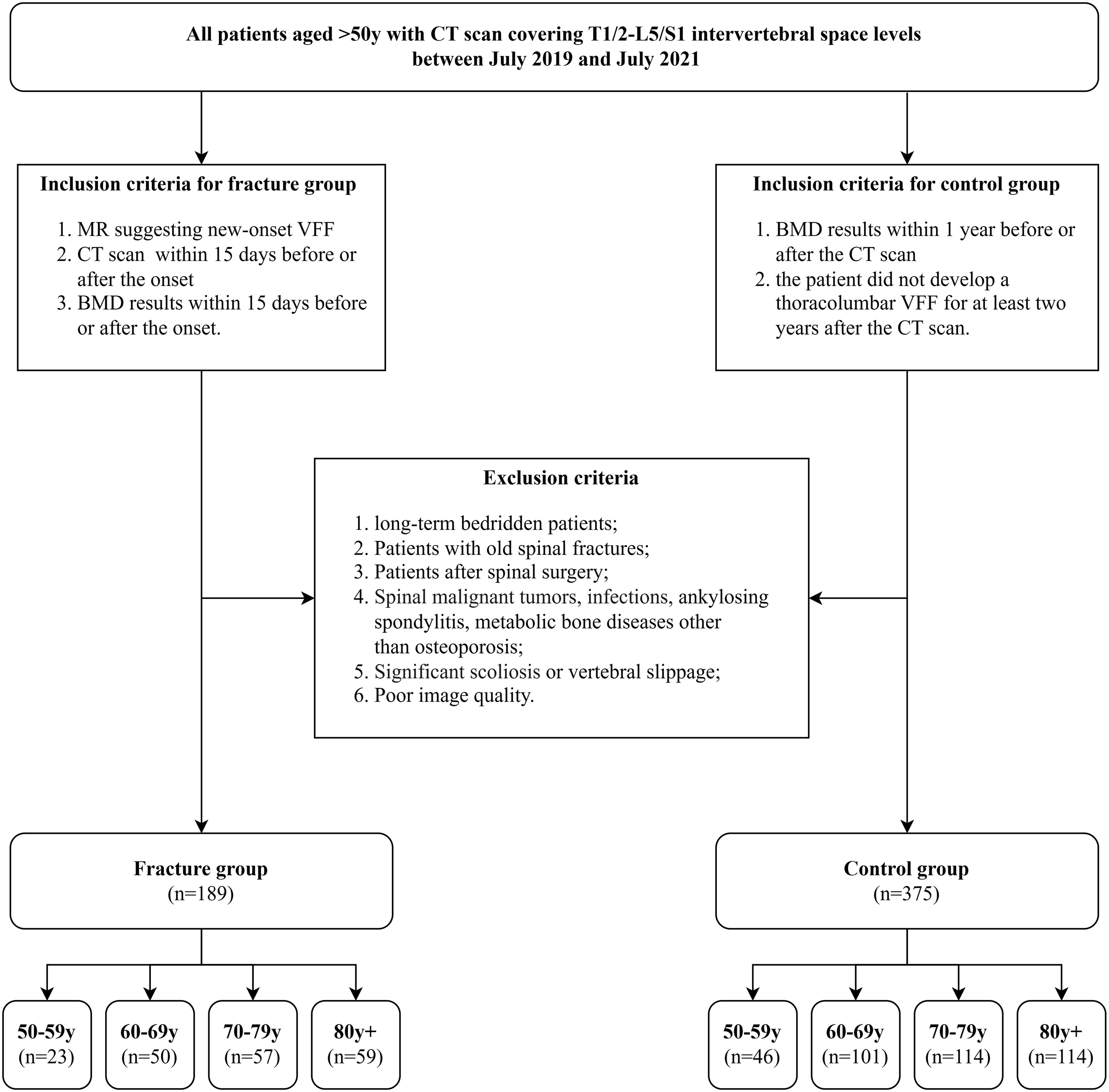
Diagnosis of New-Onset VFFs
A new-onset VFF was defined as a low-energy fracture, ie, the one that resulted from a fall from standing or lower height, or that occurs unintentionally. This fracture was identified by its hyperintensity on a T2-weighted fat-suppressed sequence of spinal MR scan, as determined by an orthopedic surgeon (for the clinical history) and a senior musculoskeletal radiologist (for the MR images).
Diagnosis of DISH and Assessment of Intervertebral Ossification
Mata et al
21
developed a semiquantitative scoring system to grade the ossification at each disc space level from 0 to 3 (0 = no ossification; 1 = ossification without bridging; 2 = ossification with incomplete bridging; and 3 = complete bridging of the disc space). The distinction between scores 1 and 2 was referred to that defined by Murakami et al,
22
while score 4 was introduced for severe ossification and extensive bridging of >1 cm in thickness according to Diederichs et al
16
(Figure 2). In accordance with Mata et al.
21
the presence of DISH was defined as scores 2, 3, or 4 at three or more consecutive disc space levels. The Mata score for ossification of the disc space level: 0 = no ossification; 1 = ossification without bridging; 2 = ossification with incomplete bridging; 3 = complete bridging of the disc space; 4 = severe ossification and extensive bridging of more than 1 cm in thickness.
The maximum number of consecutive ossified segments (MNCOS) was defined as the number of bone bridges with consecutive Mata score of 2, 3, or 4, and if there were more than 1 segment that met the condition within an observation range, the longest one was taken.
The patients were classified as DISH (+) or DISH (−) based on the diagnosis of DISH. The Mata score of each disc space level from T1/2 to L5/S1 and the MNCOS were documented for each patient.
The Resnick and Niwayama criteria 1 target DISH in its end stage. The Mata scoring system facilitates evaluation of the degree of intervertebral flowing osteophytes regardless of whether the Resnick diagnostic criteria for DISH are met. The Mata score represented the severity of intervertebral ossification, while the MNCOS represented the extent of the intervertebral bridging ossification.
Semiquantitative ratings of the Mata scoring system were obtained by 2 authors (radiologists with 4 and 10 years of experience) who were blinded to each other’s assessment. In case of disagreement, a senior radiologist (20 years of experience) made the final decision.
BMD Measurements
Areal BMD measurements of the L1–L4, hip, and femoral neck were obtained using a dual-energy X-ray absorptiometry (DXA) machine. Because the BMD of the lumbar spine is significantly affected by osteophytes and ligamentous ossification, the lowest T-score of the 3 aforementioned measurement sites was selected as ‘BMDmin’ for this study.
Imaging
All CT studies were performed on Siemens definition AS 128 (Siemens, Germany) or Philips Brilliance 16 (Philips Medical Systems, Eindhoven, Netherlands). The scanning parameters were as follows: tube voltage, 120 kV; tube current, adaptive; slice thickness, from 1.0 to 2.0 mm. The scanning range covered the T1/2–L5/S1 intervertebral space levels (continuous scanning ranges were not necessary, separate chest and abdominal scans were allowed). Images were reconstructed using the bone algorithm, reformatted in multiplanar planes.
All MR studies were performed on Siemens Avanto 1.5 T (Siemens, Germany) or Phillips Ingenia 3.0 T (Philips Medical Systems, Eindhoven, Netherlands). A slice thickness of 4 mm was used, including conventional sagittal T1-weighted and sagittal T2-weighted fat-suppressed imaging. The scanning range depended on the patient’s chief complaint, and either thoracic (covering T1–T12), lumbar (covering L1–L5), or thoracolumbar (covering T1–L5) spine protocol was permitted.
Statistical Analysis
The normality of distribution was tested using the Kolmogorov-Smirnov test and normal Q–Q plots. The t test or Mann–Whitney U test was used for the comparison of continuous variables, and the chi-square test was used for the comparison of categorical data between the 2 groups. The correlation between DISH-related parameters and age groups was tested by the Spearman’s rank correlation coefficient. The crude odds ratio (OR) of DISH for VFFs was calculated using univariate logistic regression analysis. The adjusted ORs of DISH and relevant variables for VFFs were reported with adjustment for age, sex and BMDmin using multivariate logistic regression analyses for each age group. Logistic regression analyses were conducted separately for each age group to investigate the interaction between DISH and age within each group. Statistical analyses and statistical chart drawing were performed using IBM SPSS Statistics for Mac, version 26.0 (Armonk, NY, USA), GraphPad Prism for Mac, version 9.4.1 (GraphPad Software, San Diego, California, USA) and Microsoft Excel, Office 2016 (Microsoft Corporation, Washington, Redmond, USA). A two-sided P-value of <0.05 was considered statistically significant.
Results
Comparison of Demographic Information
Comparison of Sex, Age, Height, Weight, and BMDmin Between the Fracture Group and the Control Group.
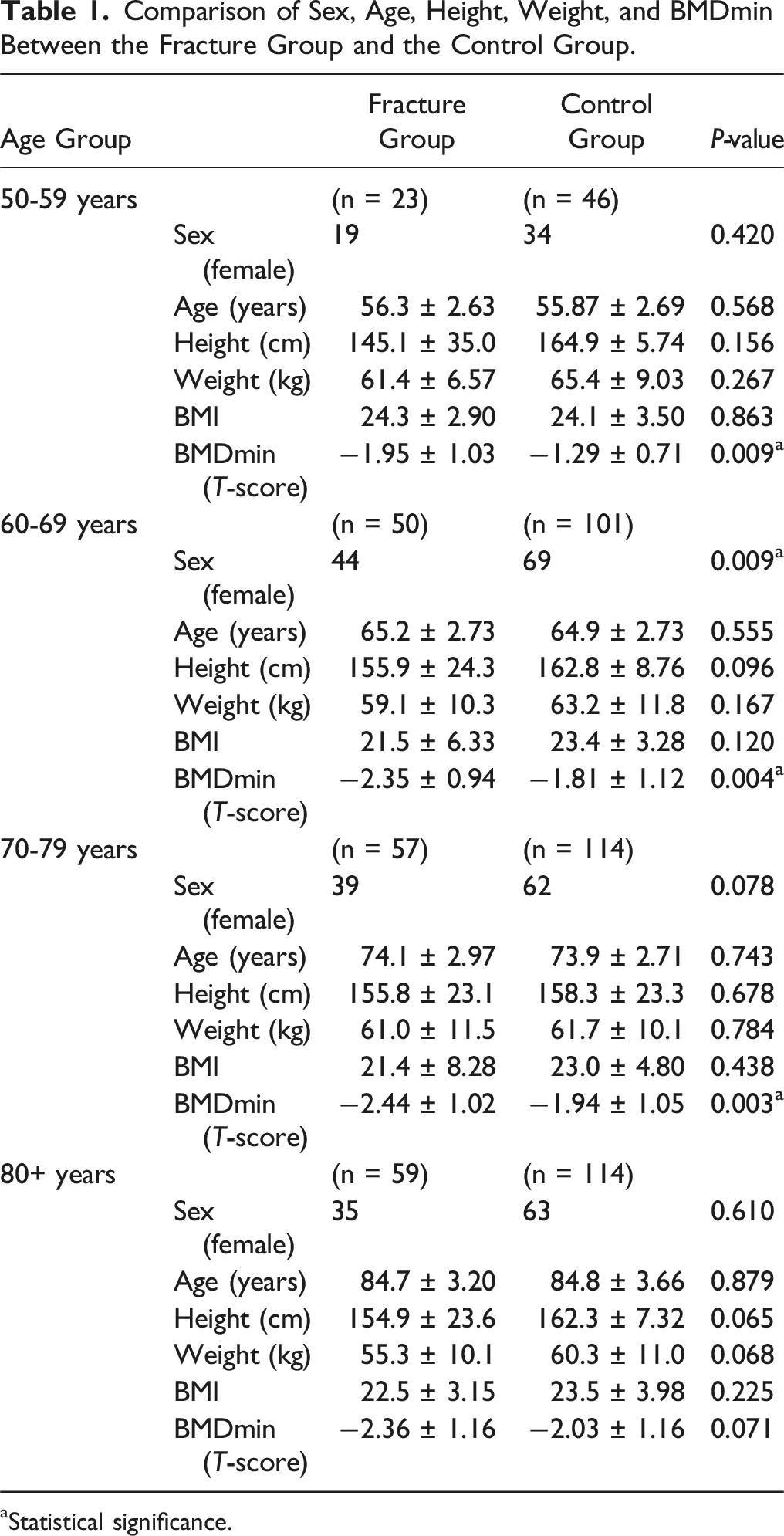
aStatistical significance.
Distribution of New-Onset VFFs in the Thoracolumbar Spine
A total of 231 newly fractured vertebrae were observed in 189 patients with fracture (Figure 3), with the highest occurrence in L1 (28.1%), followed by T12 (17.7%). Among these, 84 fractured vertebrae were found in 71 patients with DISH(+). Most vertebral fractures in the patients with DISH were not in continuous ossified segments (72/84) and a few were located within continuous ossified segments (6/84) or at the head/tail of continuous ossified segments (6/84). Distribution of acute vertebral fragility fractures of the thoracolumbar spine. The X axis refers to the location and the Y axis refers to the count of fractures.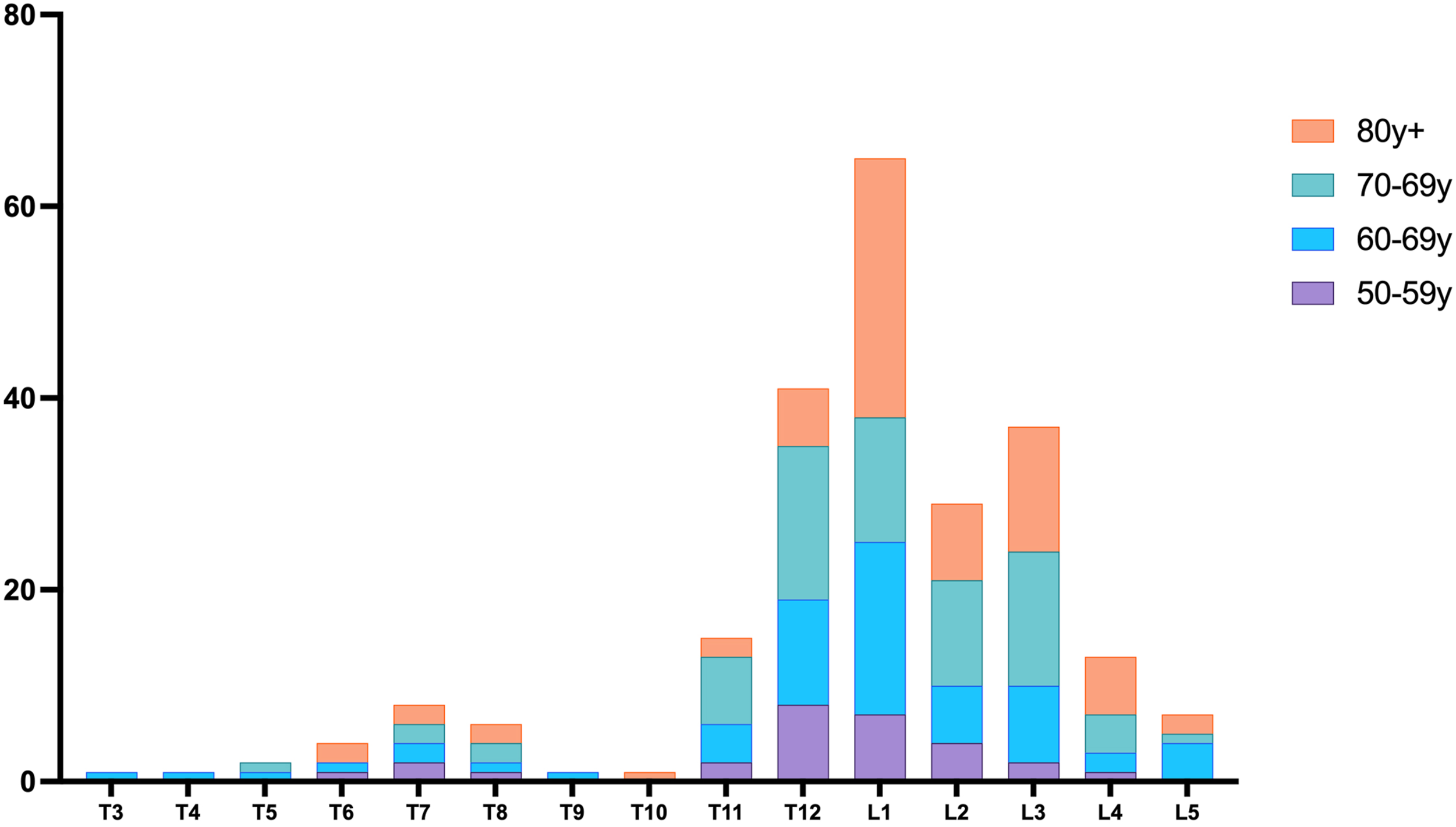
Comparison of the Prevalence of DISH Between the Fracture Group and the Control Group
Significant differences (P < 0.05) in the prevalence of DISH between the fracture group and the control group were observed in the 50-59 years group and the 80+ years group, and the trends were opposite between the 50-59 and 80+ groups (Figure 4). Comparison of the prevalence of DISH between the fracture group and the control group in (a) 50-59 years group, (b) 60-69 years group, (c) 70-79 years group, and (d) 80+ years group. * Statistical significance.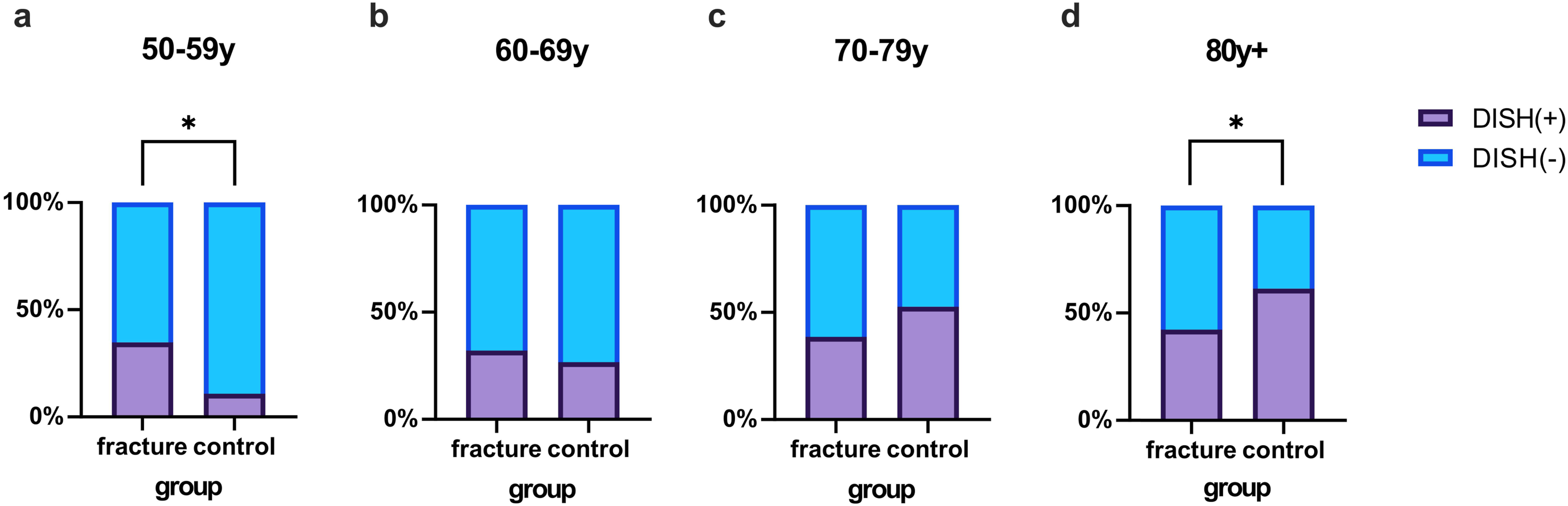
Frequency of DISH Involvement at Each Disc Space Level
For each age group in the fracture group and the control group, the frequency (%) of DISH involvement at each disc space level is shown in Figure 5. In the younger age groups, DISH mainly affected the thoracic spinal segments, while in the older age groups, there were also cases of lumbar involvement; however, there were some differences between the fracture and control groups. Frequency distribution of DISH involvement at each disc space level in various age groups of (a) the fracture group and (b) the control group. The X axis refers to the disc space level, and the Y axis refers to the percentage of patients involved by DISH in certain disc space level compared to the total number of patients in a certain age group.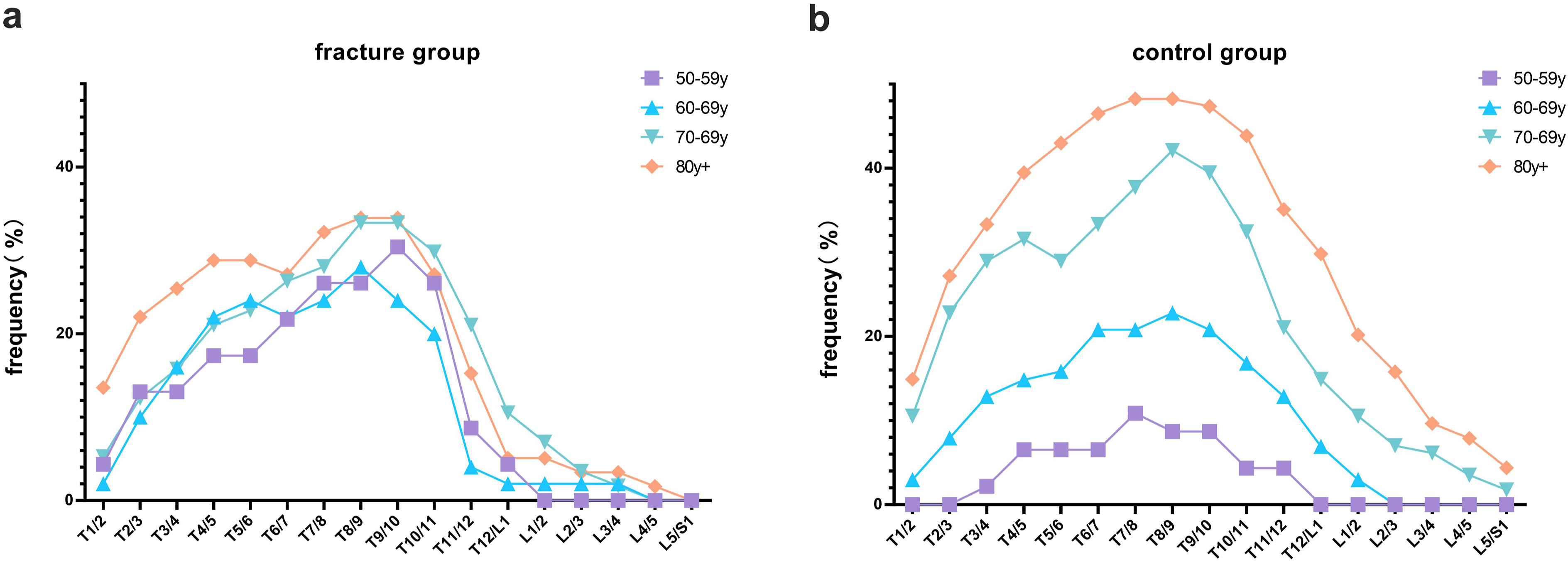
In the fracture group, the most commonly DISH-affected segments were T9/10 in the 50-59 years group, T8/9 in the 60-69 years group, and T8/9–T9/10 in the 70-79 and 80+ years groups. The frequency distribution showed a rapid decline from T10/11 to T11/12 in the 50-59 and 60-69 years age-groups and from T10/11 to T12/L1 in the 70-79 and 80+ age-groups.
In the control group, as age increased, the frequency (%) of DISH involvement in thoracic segments gradually increased and the involvement of the lumbar spine also increased. The frequency distribution of the control group exhibited a bell-like shape with a slightly smoother curve than that of the fracture group. Peaks were observed at T7/8 in the 50-59 years, at T8/9 in the 60-69 and 70-79 years, and at T7/8–T8/9 in the 80+ years groups.
According to the apparent variation in the occurrence of vertebral fractures and the frequency of DISH involvement, the thoracolumbar spine was divided into 2 subsegments: T1/2–T10/11 and T11/12–L5/S1.
Association Between DISH-Related Parameters and Age Groups in the Fracture and Control Groups
The comparison of Mata scores of each disc space level among the 4 age groups and the MNCOS of the 4 age groups are shown in Figure 6. Spearman’s rank correlation coefficients between DISH-related parameters and age groups were calculated separately for the fracture group and the control group, with both groups including participants of all ages. (Table 2). Comparison of the Mata scores of each disc space level among the four age groups in (a1) the fracture group and (a2) the control group. Comparison of the MNCOS among the four age groups in the fracture group and the control group (b). Spearman’s Rank Correlation of DISH-Related Parameters Across Age Groups, Separately Analyzed in Fracture and Control Groups. aStatistical significance.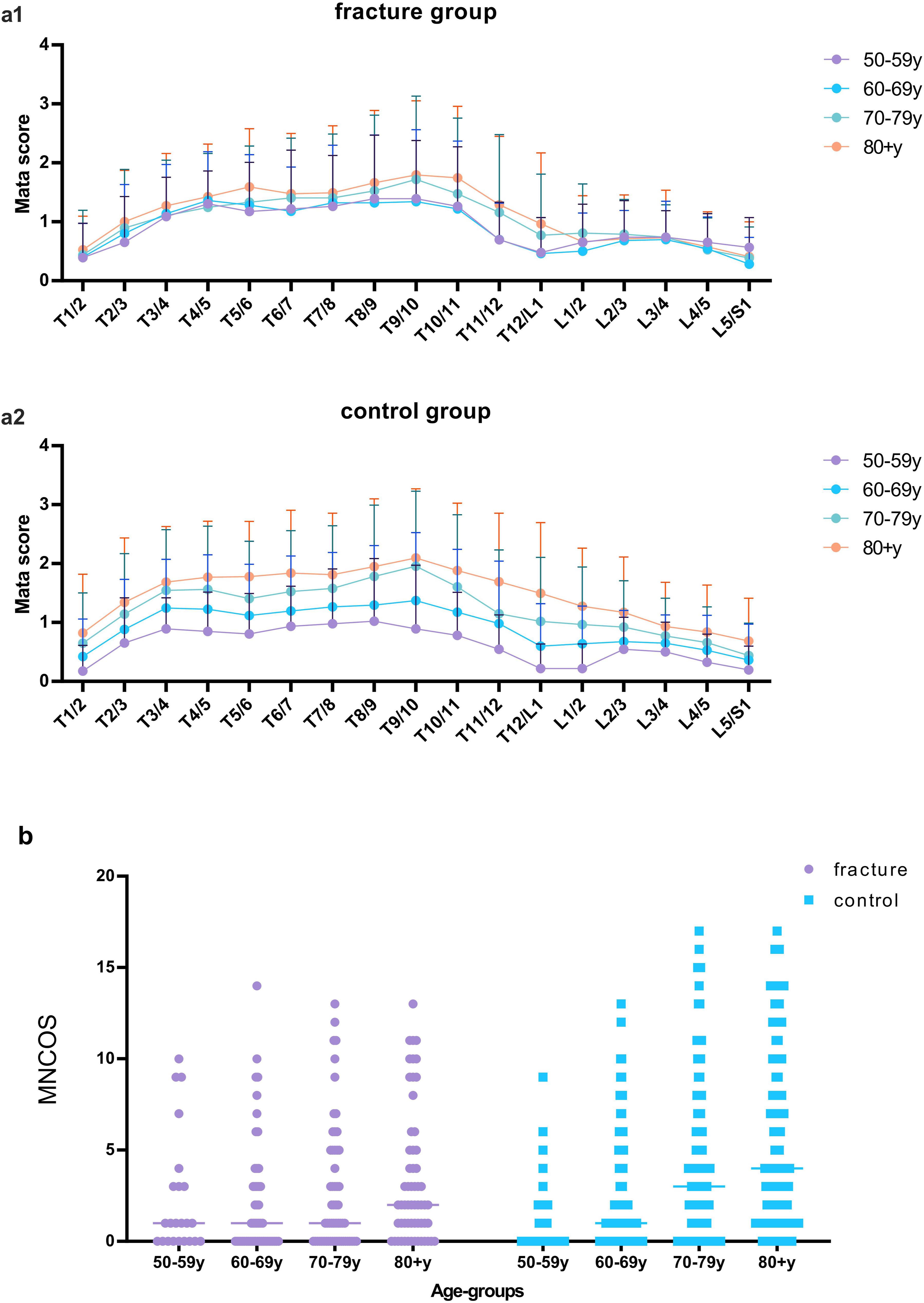
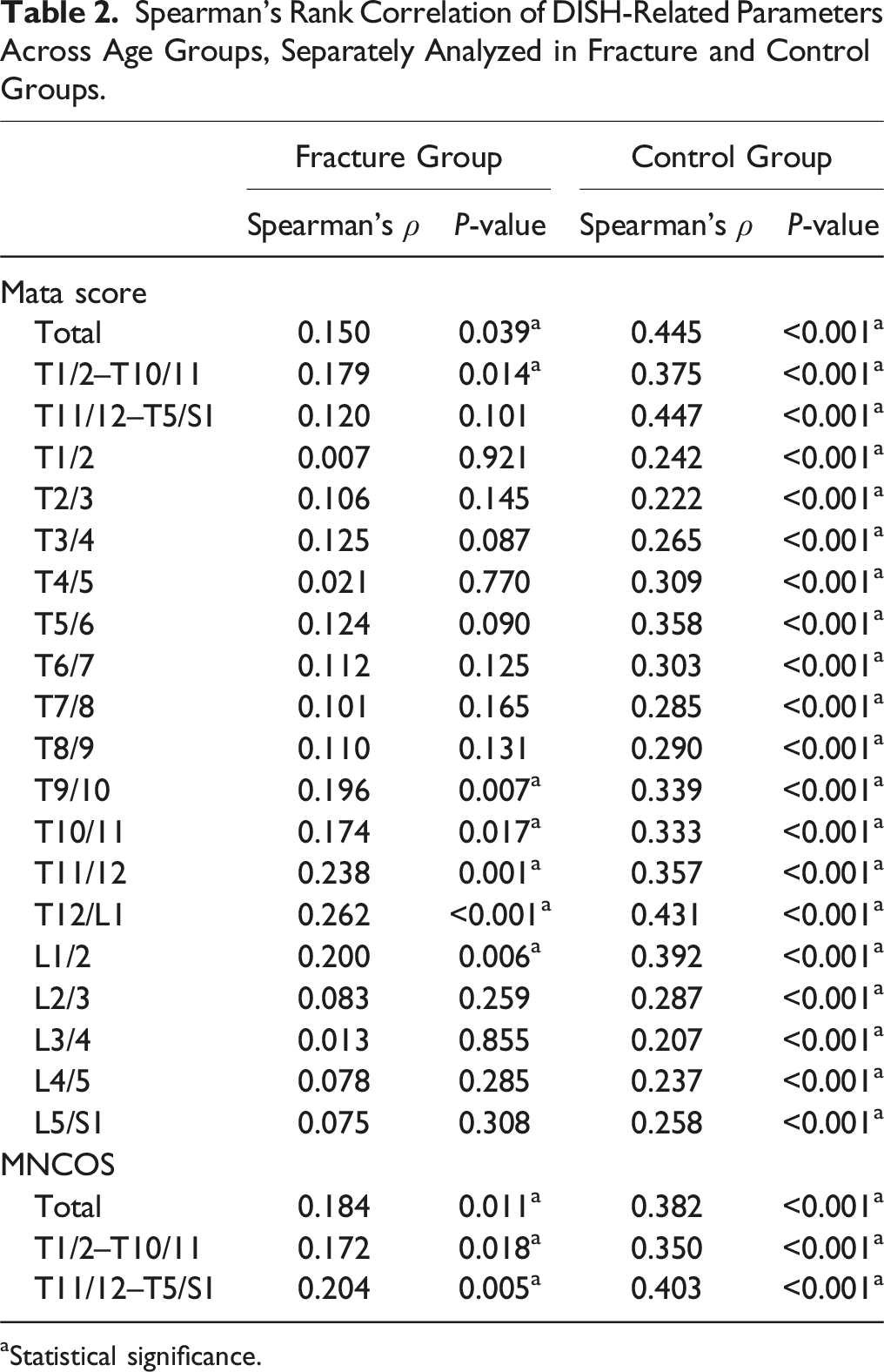
Within the fracture group, the mean Mata scores of the 4 age groups were similar at most spinal levels, with overlapping or intersecting fold lines (Figure 6-a1). The Mata scores of T9/10, T10/11, T11/12, T12/L1, and L1/L2 levels showed extremely weak monotonic correlation with age group (Spearman’s ρ < 0.3, P < 0.05), while the other segments showed no significant correlation (P > 0.05). The median of MNCOS in the age groups 50-59, 60-69, and 70-79 years was the same (Figure 6-b). The correlation between the MNCOS and age group was extremely weak (Spearman’s ρ < 0.3, P < 0.05).
In contrast, in the control group, it was evident that the mean Mata scores gradually increased with age in all of the segments, with the fold lines pulling apart, particularly at the junction of the thoracolumbar spine (Figure 6-a2). The Mata score of each intervertebral level showed weak to moderate monotonic correlation with age group (Spearman’s ρ between 0.207 and 0.447, P < 0.001). The median of MNCOS gradually increased among the age groups 50-69, 60-69, 70-79, and 80+ years (Figure 6-b). The overall MNCOS and MNCOS of 2 subsegments had weak to moderate correlation with age group (Spearman’s ρ between 0.350 and 0.403, P < 0.001).
Crude and Adjusted ORs of DISH and Relevant Parameters for VFFs
The Crude and Adjusted ORs of the Variables.
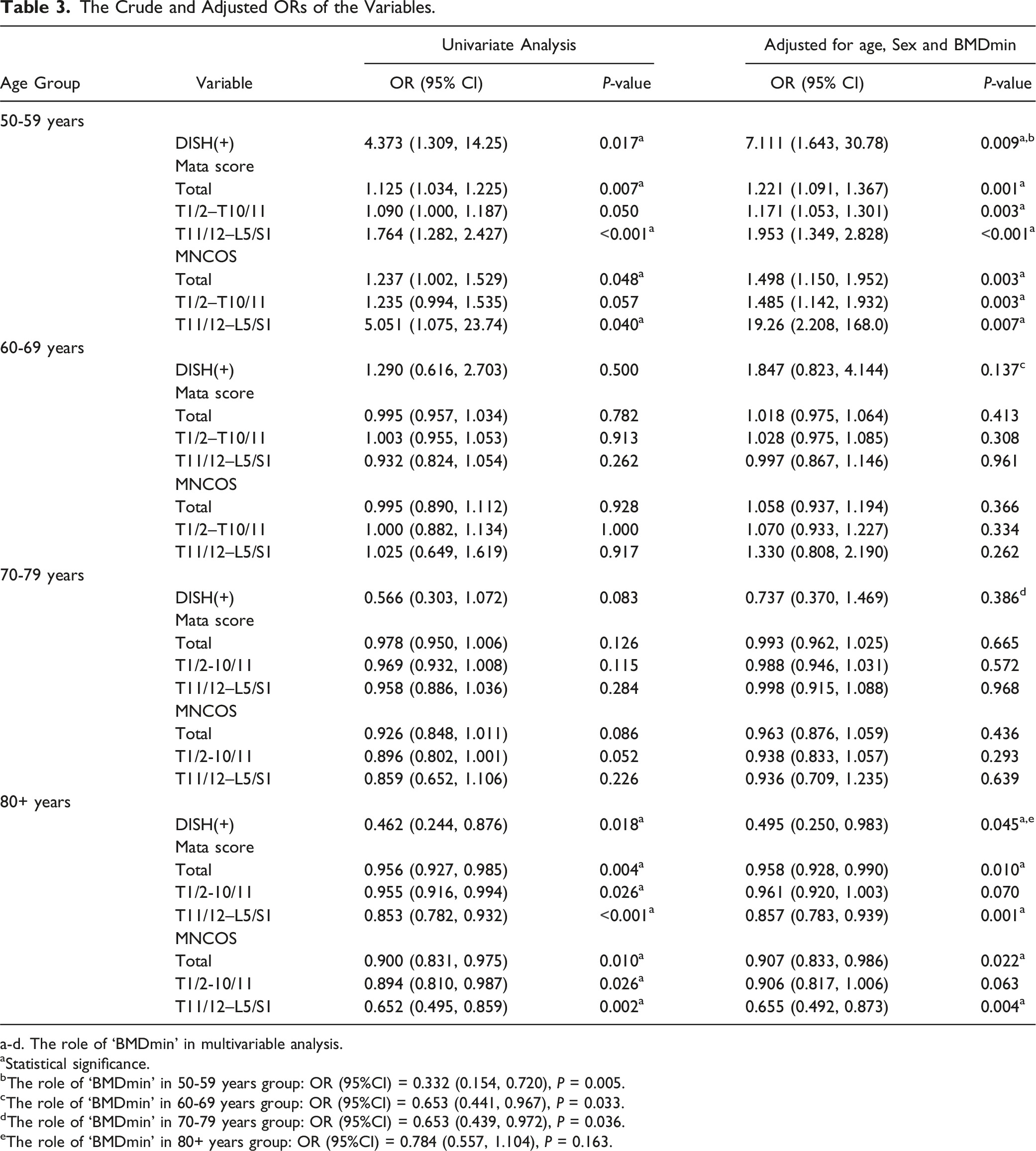
a-d. The role of ‘BMDmin’ in multivariable analysis.
aStatistical significance.
bThe role of ‘BMDmin’ in 50-59 years group: OR (95%CI) = 0.332 (0.154, 0.720), P = 0.005.
cThe role of ‘BMDmin’ in 60-69 years group: OR (95%CI) = 0.653 (0.441, 0.967), P = 0.033.
dThe role of ‘BMDmin’ in 70-79 years group: OR (95%CI) = 0.653 (0.439, 0.972), P = 0.036.
eThe role of ‘BMDmin’ in 80+ years group: OR (95%CI) = 0.784 (0.557, 1.104), P = 0.163.
The Mata scores and MNCOSs of the total T1/2–L5/S1 and both subsegments were significant risk factors for VFFs in the 50-59 years group. In the 80+ years group, T1/2–L5/S1 total scores and T11/12–L5/S1 subsegment scores were significant protective factors against VFFs. None of the variables showed a statistically significant effect on VFFs in the 60-69 and 70-79 years groups.
The additional logistic regression analysis conducted within each of the 4 age groups showed that the interaction term of age * DISH was not statistically significant in any of the groups (P > 0.05 for all). Figure 7 illustrates the interactive effect of age and DISH status on the predicted probability of VFFs from the logistic regression models. In the 50-59 years age group, DISH(+) was associated with higher predicted probabilities of VFFs occurrence compared to DISH(−) at any age. Conversely, in the 70-79 and 80+ years age groups, DISH(−) was associated with higher predicted probabilities of VFFs occurrence than DISH(+) at any age. However, within the 60-69 years age group, the predicted probability fit lines for DISH(+) and DISH(−) intersect at around 64 years old on the x-axis. The interaction effect of age and DISH status on the predicted probabilities of VFFs within four age groups: (a) 50-59 years group, (b) 60-69 years group, (c) 70-79 years group, and (d) 80+ years group. The X axis refers to age (as a continuous variable), and the Y axis refers to the logistic regression model's predicted probabilities.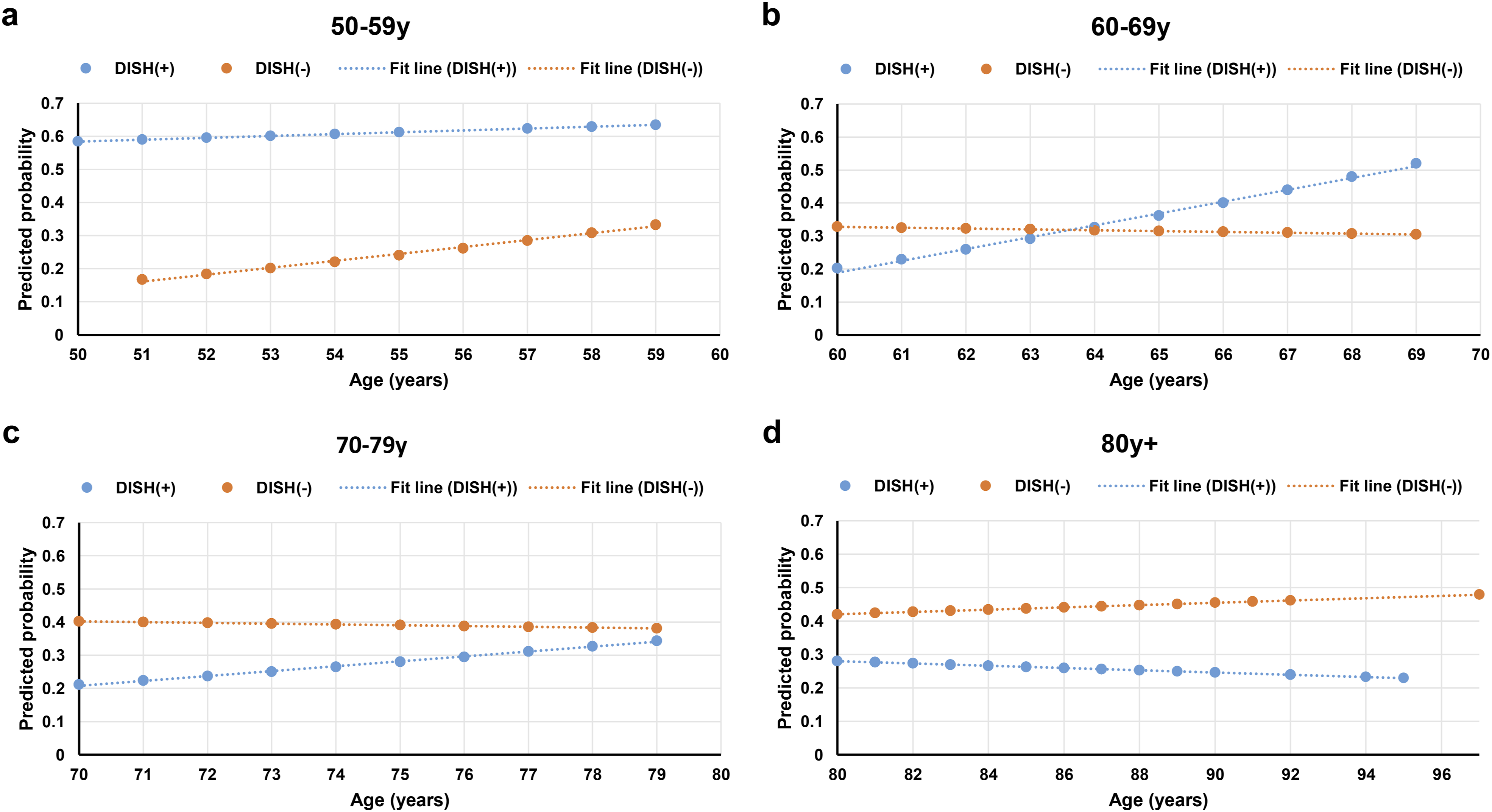
Discussion
The diagnosis of DISH is frequently overlooked by clinicians. This may be due to a lack of knowledge or because of the variability of clinical symptoms associated with DISH. However, diagnosing the presence of DISH is clinically important, as it is associated with the metabolic syndrome, coronary and aortic disease, and respiratory effects. 23
In this study, we found that as age increases and intervertebral ossification progresses, the effect of DISH on the occurrence of new VFFs changes from a risk factor to a protective factor, and this effect is significant in the 2 age extremes (50-59 years, 80+ years) and is independent of BMD. There were no significant findings in the population between 60 and 79 years.
The present study also found that the trend of DISH development with age was different between the fracture and control groups. In the fracture group, the frequency of DISH involvement in all spinal segments was similar at different ages with an obvious drop in the thoracolumbar junction. That is, the thoracic segment was much more involved, whereas the thoracolumbar junction and lumbar segment were rarely involved. This ‘drop’ happened to be where VFFs tended to occur. In the control group, the frequency of DISH involvement in all spinal segments gradually increased and the extension of DISH to the thoracolumbar junction and lumbar segment increased with age. The severity of ossification at each disc space level showed gradual upward trends with age in the control group, especially at the thoracolumbar junction, whereas there was less variation among the 4 age groups in the fracture group. These findings are valuable for explaining the subsequent results.
The association between DISH and vertebral fractures has been explored in previous studies that were limited to men16,24 or patients with certain diseases. 17 In some studies, the diagnosis of DISH was based on plain radiographs rather than on CT, which has been shown to be more sensitive for the assessment of structural changes in DISH. 25 Postfracture repair may cause intervertebral bridging 26 ; thus, we excluded patients with old vertebral fractures from our study and limited the time interval between CT scan and VFF onset, attempting to ensure as much as possible that all bone bridges had formed before the onset of VFF. Therefore, this study investigated how DISH affects the occurrence of first-time thoracolumbar VFFs at different age groups based on CT scans.
We found that DISH was an independent risk factor for VFFs in the 50-59 years group, which is consistent with previous studies.13,16,24 It is considered that increased spinal stiffness due to DISH may play a more important role than vertebral BMD in the increased fracture risk. 27 Physiological spinal motion through the facet joints allows flexion, extension, lateral bending, and rotation to distribute forces among multiple mobile segments, whereas intervertebral discs act as shock absorbers between the segments. This is particularly important in dissipating energy from trauma. However, ankylosed segments in DISH inhibit segmental motion, thereby creating long lever arms and causing high stress concentration,28,29 leading to a higher risk for spine fractures even from low-energy trauma such as ground-level falls. Our study also showed that greater severity and length of intervertebral bridging ossification were more likely to cause VFFs in the 50-59 years group. Therefore, early diagnosis of DISH and detection of bridging ossification between vertebrae are beneficial to raise awareness of VFFs and to conduct clinical intervention as early as possible.
Interestingly, we found that DISH became a protective factor against VFFs in people over 80 years of age, and in the analysis of subsegments, we showed that it was more protective against VFFs if there were longer continuous bone bridges and more severe intervertebral ossification of the thoracolumbar junction and lumbar segment.
Evidently, the thoracolumbar junction and the lumbar spine were the sites of higher fracture occurrence, and most vertebral fractures in patients with DISH were not in continuous ossified segments. Therefore, bone bridges involving the thoracolumbar junction and lumbar segment led to a lower probability of VFFs in people over 80 years of age, which may be related to following conditions. First, the bone bridge formation affects local mobility22,30 and thus reduces some of the fragility fractures associated with behaviors such as bending over. Second, the ossification of intervertebral space may actually increase the stability of the spine, which has been suggested by Holton et al. 2 Additionally, some studies have indicated that there may be a correlation between DISH and an increase in BMD.16,27,31 In the present study, ‘BMDmin' showed statistical significance for a risk factor of VFFs in the 50-79 years age group, but failed to demonstrate statistical significance in the 80+ years age group. This may suggest that BMD no longer plays a significant role in people over 80 years old, and the occurrence of DISH in this context may be protective in a spine with low bone density. The influence of DISH on VFFs is multifaceted and requires further investigation to gain a deeper understanding of the relationship between DISH and vertebral BMD, bone strength and spinal stability across diverse age groups. Although the present study indicates that DISH may have a protective effect on VFFs for the over-80s, it does not prove that DISH is beneficial. DISH may present with radiculopathy, myelopathy, restricted spine movements, dyspnoea, or dysphagia.32-34 Moreover, DISH is usually associated with various metabolic disorders like diabetes mellitus (DM), obesity, hyperinsulinemia, and atherosclerosis, with an increased risk of cardiovascular morbidity. 35
Our study did not identify a statistically significant association in the population aged 60-79 years old. This may be attributed to the fact that the prevalence or severity of DISH in this age group is moderate. Nevertheless, the ORs for DISH as a risk factor for VFFs reversed directions in the 70-79 years group compared to those <70 years. Although the interaction analysis of DISH * age conducted in various age groups did not show statistical significance, the visualization graph for the 60-69 age group specifically indicates a potential shift in the relationship between DISH status and the risk of VFFs around this age range. Admittedly, the lack of statistical significance in our analysis may be due to the limited sample size, underscoring the need for further research with a larger cohort and stricter control of confounding variables.
The main limitation of this study is its retrospective study design. Selection bias might exist, and other clinic factors associated with DISH and vertebral fractures were difficult to collect comprehensively. When follow-up image data at appropriate time intervals cannot be obtained in the PACS system, we used telephone consultation for follow-up of the control group to confirm that they did not develop VFFs. Considering that older patients may have a reduced pain sensation compared to younger patients, this is another limitation. In addition, the sample size was not large. Future studies should employ a larger sample size and prospectively investigate the factors related to the fracture risk in the study population. Nevertheless, as DISH is insufficiently understood, we believe that the present study offers new and relevant information to enhance our understanding of the characteristics of DISH.
Conclusion
DISH developed with age, and in patients aged >50 years, the effect of DISH on the occurrence of VFFs changed from a risk factor to a protective factor with increasing age. In 50-59-year-old population, the severity and extent of intervertebral bridging ossification positively correlated with the risk of VFFs. As the thoracolumbar junction and lumbar intervertebral bridging ossifications increased with age, they became a protective factor for reducing the occurrence of thoracolumbar VFFs in people over 80 years old. This study suggests that early diagnosis of DISH is beneficial and calls for research on the relationship between DISH and vertebral bone strength as well as spinal stability in the elderly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Natural Science Foundation of China (Grant No. 82302303).
Ethical Statement
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.