
Abstract
Study Design
Systematic literature review.
Objectives
In this study we assessed evidence for the use of osteobiologics in single vs multi-level anterior cervical discectomy and fusion (ACDF) in patients with cervical spine degeneration. The primary objective was to compare fusion rates after single and multi-level surgery with different osteobiologics. Secondary objectives were to compare differences in patient reported outcome measures (PROMs) and complications.
Methods
After a global team of reviewers was selected, a systematic review using different repositories was performed, confirming to PRISMA and GRADE guidelines. In total 1206 articles were identified and after applying inclusion and exclusion criteria, 11 articles were eligible for analysis. Extracted data included fusion rates, definition of fusion, patient reported outcome measures, types of osteobiologics used, complications, adverse events and revisions.
Results
Fusion rates ranged from 87.7% to 100% for bone morphogenetic protein 2 (BMP-2) and 88.6% to 94.7% for demineralized bone matrix, while fusion rates reported for other osteobiologics were lower. All included studies showed PROMs improved significantly for each osteobiologic. However, no differences were reported when comparing osteobiologics, or when comparing single vs multi-level surgery specifically.
Conclusion
The highest fusion rates after 2-level ACDF for cervical spine degeneration were reported when BMP-2 was used. However, PROMs did not differ between the different osteobiologics. Further blinded randomized trials should be performed to compare the use of BMP-2 in single vs multi-level ACDF specifically.
Keywords
Introduction
Back and neck pain are a growing problem in the developed world. In 2015 it was the fourth major cause of years lost to disability worldwide. 1 Although most episodes of back and neck pain are short, mild and self-limiting, for severe and persistent cases operative interventions are utilized. For severe neck pain with or without radiculopathy, the most widely used procedure is anterior cervical discectomy and fusion (ACDF). In the US alone, over 150 000 ACDF procedures are performed annually, which is expected to increase to over 170 000 procedures by 2040. 2 The outcomes of this procedure are generally good, with fusion rates over 90%, and a subjective improvement in 73.7% of patients. 3 However, for multi-level cases, results are less favorable, with revision rates up to 35% within the first 2 years after surgery. 4
In order to increase the fusion rate in ACDF, multiple graft materials promoting bone-growth have been proposed. However, most of these ‘osteobiologics’ have not found their way into common practice. This is probably due to the different regulatory and reimbursement aspects in different countries, in addition to their relative novelty. Their effective use in clinical practice is thus reduced. To this end the members of the AO Spine Knowledge Forum Degenerative 5 are committed to producing a spine osteobiologics classification and guideline (AO-GO). The aim is to develop a framework to evaluate the level of evidence supporting the use of bone grafts and osteobiologics. This guideline will help surgeons to understand the quality of the information that is provided for each product used.
In order to gather the evidence for this framework, a series of systematic reviews were performed. These systematic reviews spanned 13 different subjects focusing on the use of osteobiologics in ACDF. The current review focused on the evidence for the use of osteobiologics in single vs multi-level ACDF.
Methods
Search Strategy
The systematic review was registered into the PROSPERO 6 database under number CRD42020199006. A PICO answering the main question was drafted by the team lead and co-lead and discussed with the entire review team via video conferencing. The PICO was subsequently reviewed by the AO-GO core team, to be able to seamlessly integrate it with the other 12 systematic reviews performed, in relation to the guideline development. The full PICO can be found as a supplemental document, Table 1. In short, we included adult patients between ages 18 and 80 years old with herniated or degenerative cervical neck discs. Exclusion criteria were: history of tumor; infection; spinal cord injury; trauma or fracture; skeletally immature patients or patients with scoliosis or other cervical deformity. Intervention was multi-level ACDF with cage and/or anterior plating and the use of an osteobiologic (see supplemental documents, Table 2). The comparator was single level ACDF with cage and/or anterior plating combined with iliac crest bone graft (ICBG) or allograft. Our primary outcome measure was fusion, determined either by CT or flexion/extension X-rays. Secondary outcome measures were patient reported outcome measures (PROMs). Only articles published after 2000 were considered for review.
This PICO was used to build a search string for Pubmed/Medline, Embase and Cochrane repositories, by professional librarians from the institution of the lead investigator. The complete search strings and search results are available under Supplementary material 1-4. Search results were imported into Mendeley Reference manager and duplicates were removed. Then, reviewers were divided into 2 teams (BQ+JH and RY+GR) based on time-zone congruency, to both screen half of the titles and abstracts. Any possible conflict was to be resolved first within the team and if there was no consensus found within the team, by the senior investigator. After the selection of articles eligible for full-text review, all full-text articles were retrieved through library sources. Both review teams then proceeded to screen full-text articles that had been selected by the other team and vice versa (crossover design) to limit possible reviewer selection bias. During the full-text review, the references in the articles were also screened for possible eligibility (snowballing). Again, any possible conflict was to be resolved first within the review team and if necessary, by the senior investigator.
Data Extraction
If a single reviewer deemed a full-text article appropriate for inclusion according to the aforementioned inclusion criteria, studies were assessed for risk of bias according to the GRADE-approach. 7 Data was extracted systematically into a provided study characteristics and demographics table, and a data abstraction table. Study characteristics included study design; evidence level; inclusion- and exclusion criteria; intervention and osteobiologic used; where applicable comparator; patient demographics; follow-up period; data on funding and possible conflict of interests. Abstracted data included: fusion rates; patients reported outcome measures; adverse events; complications and revisions; and possible other notable outcomes. Afterwards, all results from individual reviewers were compounded into a single data table. This table was discussed with the complete team of reviewers via video conferencing to reach consensus about the results of our review. If any data was missing or unclear, the corresponding author was contacted by email in order to provide additional data. Additionally, the data was assessed for suitability for quantitative meta-analysis.
Results
The search strategy identified 1206 articles. After removal of duplicate studies, 957 articles were screened for title and abstract, 50 articles were deemed relevant to the study question and underwent full-text review. Snowballing yielded an additional 8 papers for screening. Full-text review yielded 11 articles which met inclusion and exclusion criteria for this review (Figure 1). Initially this study aimed to investigate 3-4 level fusions as extensively as 1-2 level fusions, however, only very limited data was available for 3-4 level fusions. Therefore, results are restructured comparing single-level vs multi-level fusion. PRISMA flow diagram.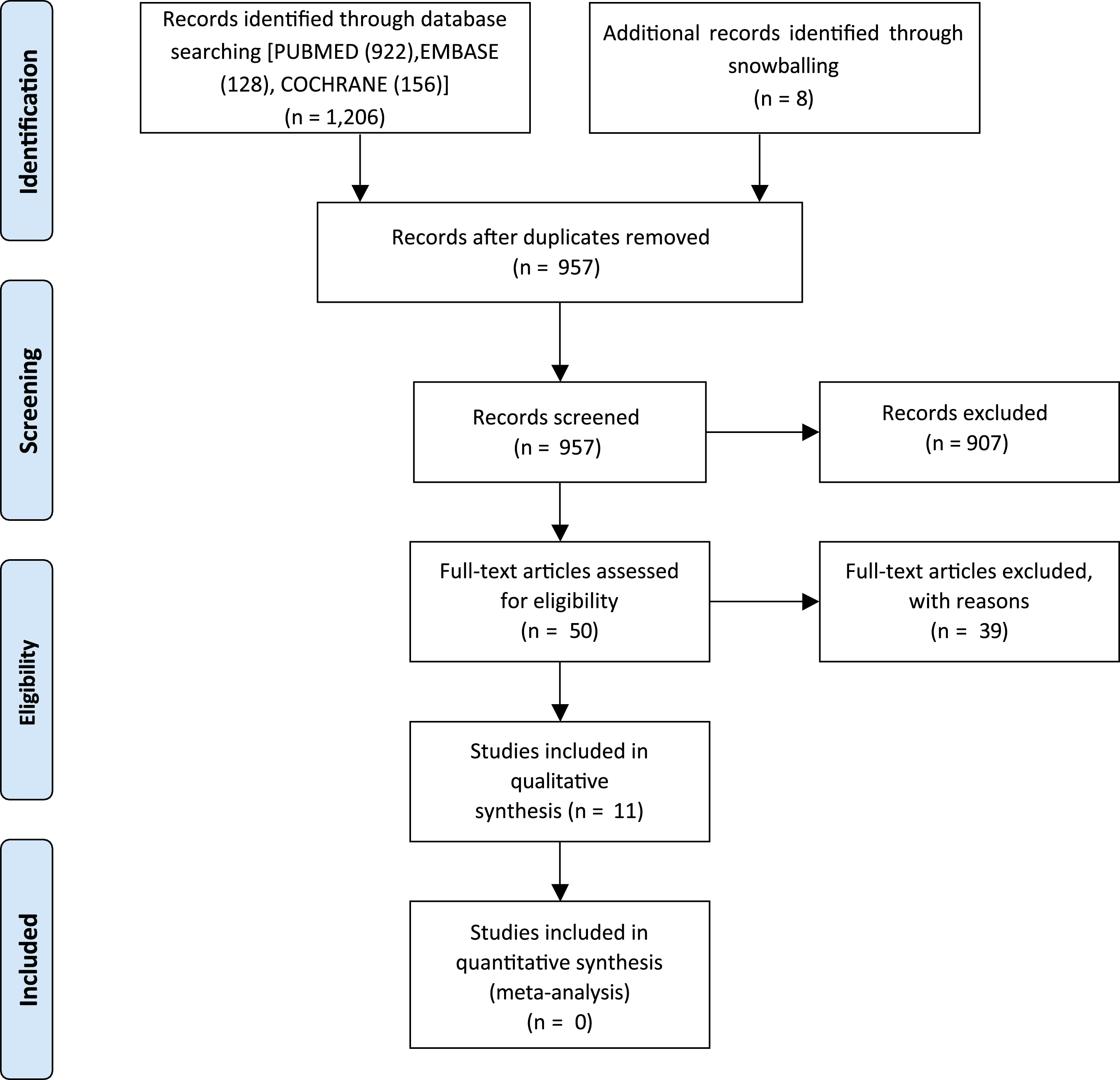
Two studies reported partly on the same cohort of patients.8,9 These papers reported different follow-up points and different outcomes. Both studies were included as 1 cohort and are presented in the results accordingly. For 4 studies,10–13 the corresponding author was contacted for additional data, regarding the results for single-level vs multiple level fusion, either for fusion rates or for PROMs. In 1 case this was provided. Unfortunately, the data was not suitable for quantitative meta-analysis.
Quality Assessment
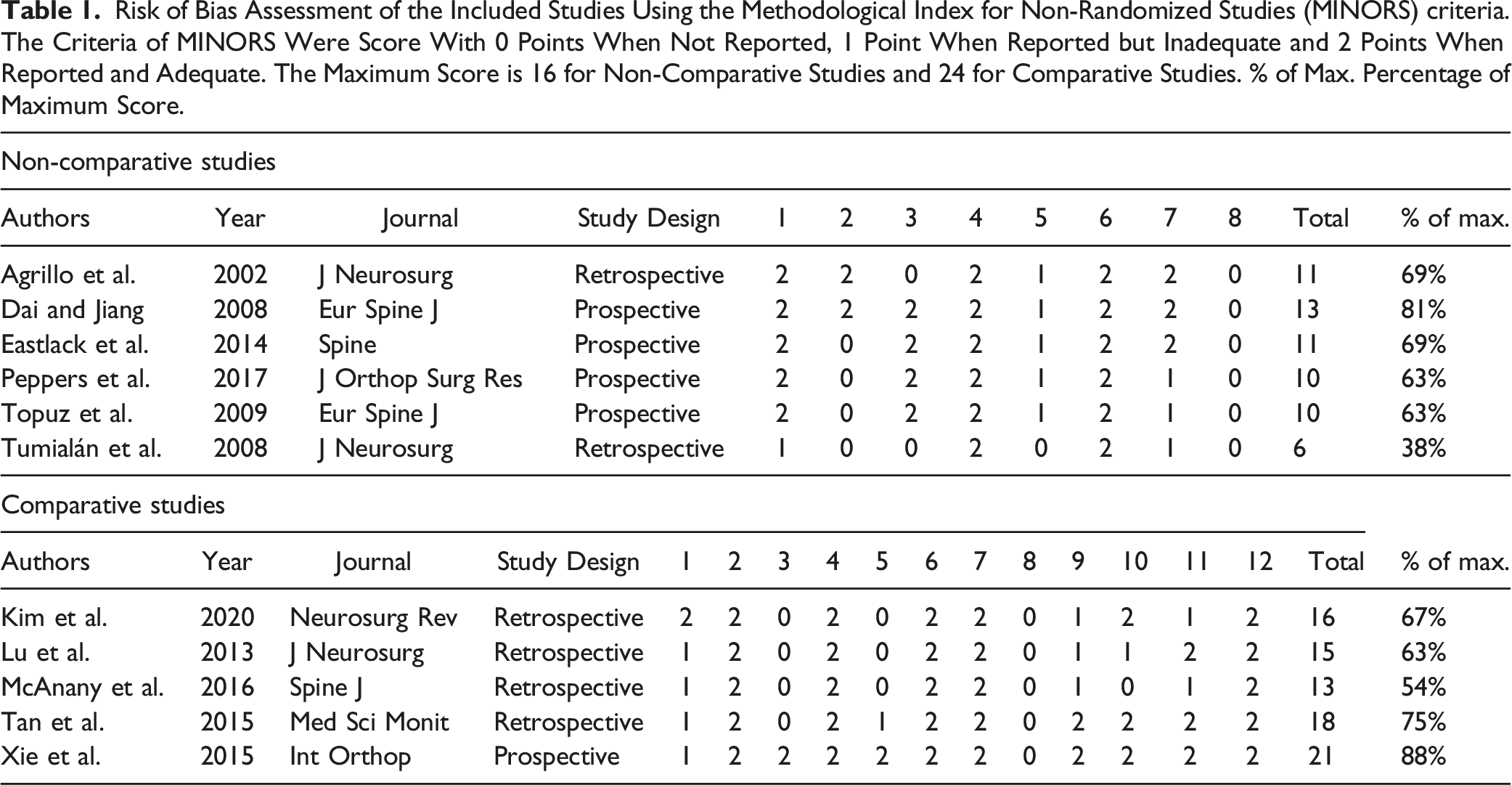
Risk of Bias Assessment of the Included Studies Using the Methodological Index for Non-Randomized Studies (MINORS) criteria. The Criteria of MINORS Were Score With 0 Points When Not Reported, 1 Point When Reported but Inadequate and 2 Points When Reported and Adequate. The Maximum Score is 16 for Non-Comparative Studies and 24 for Comparative Studies. % of Max. Percentage of Maximum Score.
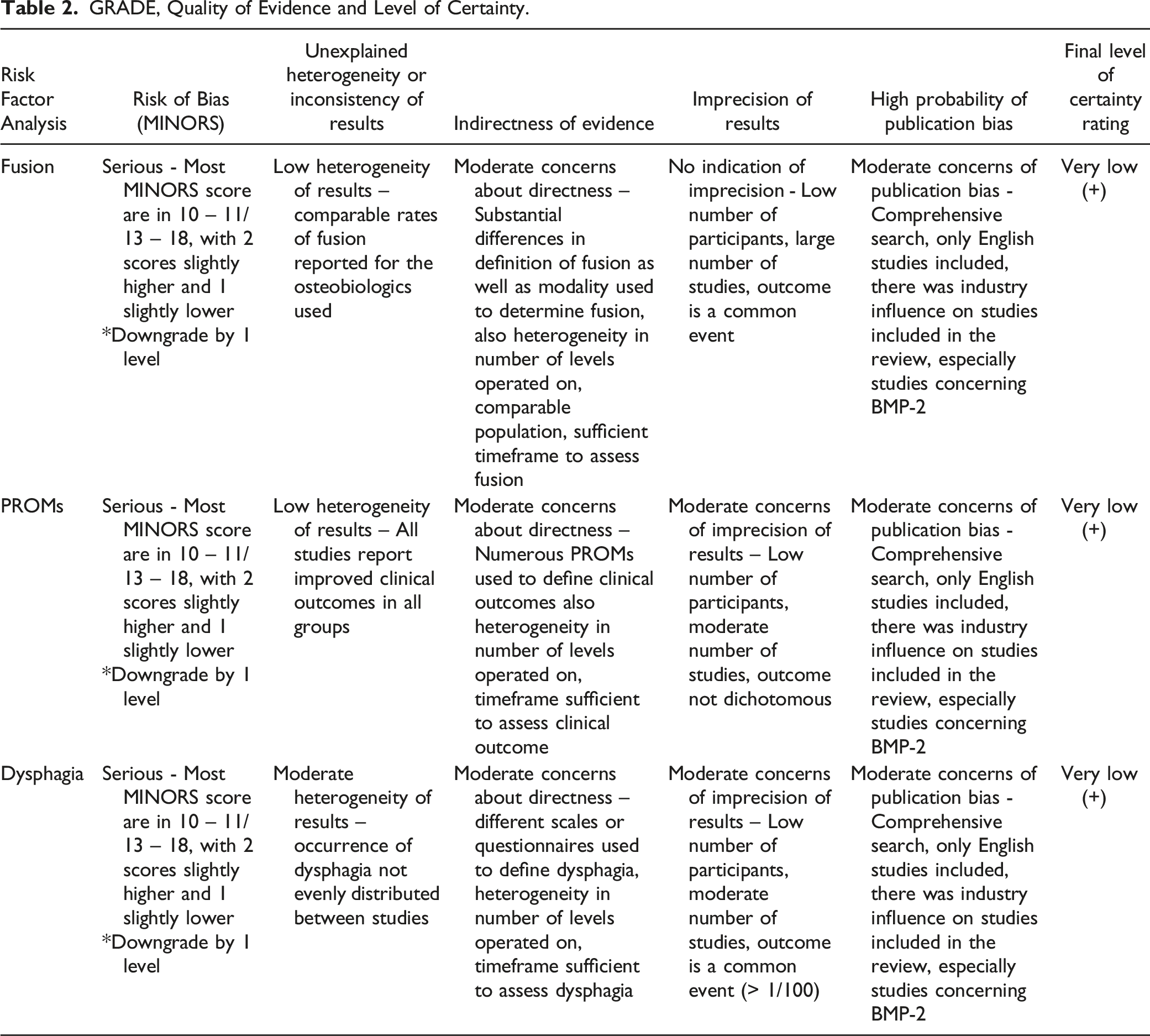
GRADE, Quality of Evidence and Level of Certainty.
Fusion Rates
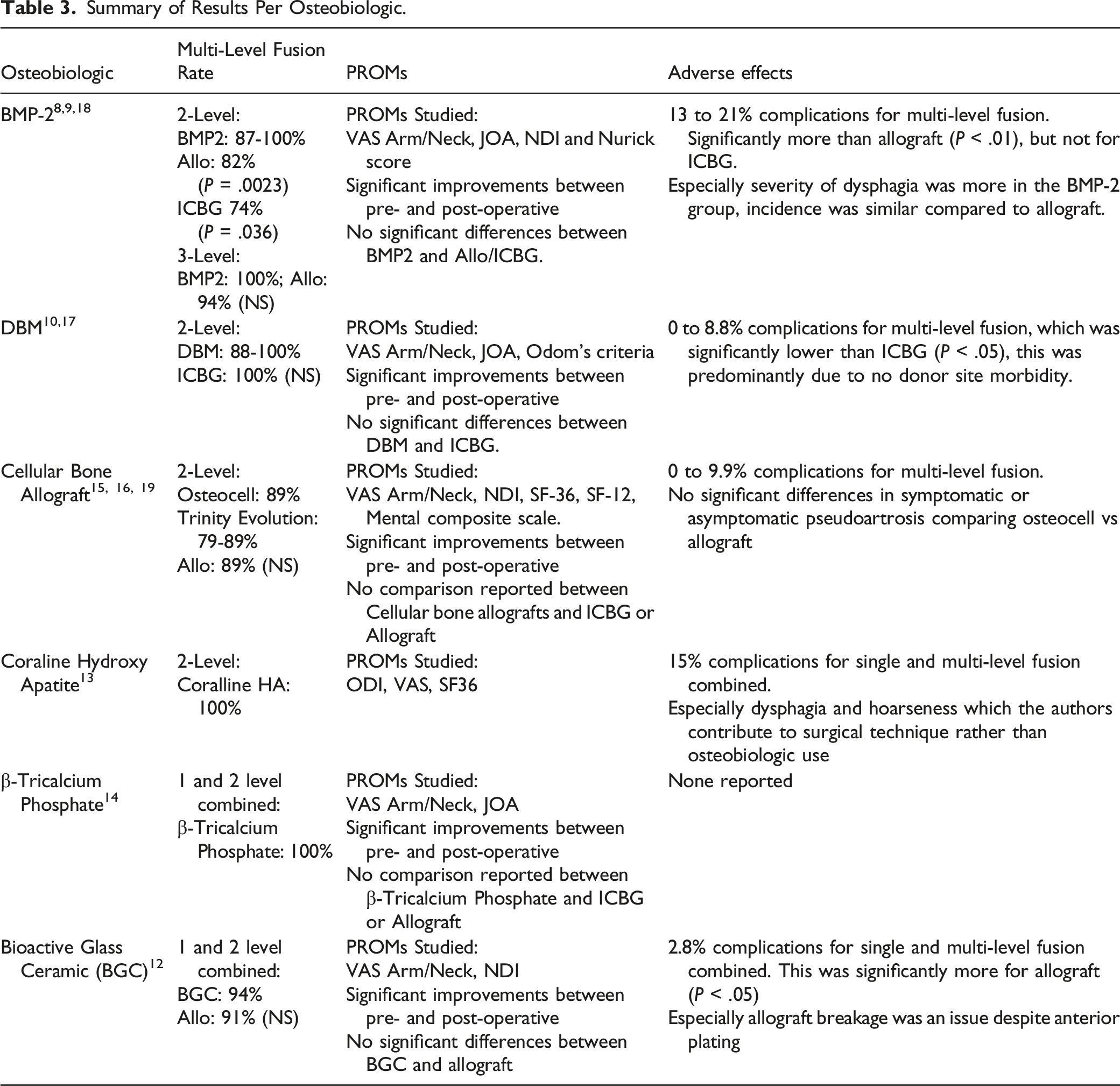
Summary of Results Per Osteobiologic.
BMP-2
Three studies described fusion rates for single and multi-level ACDF with the use of BMP-2.8,9,18 The fusion rates among these studies varied from 87.7% to 100%. No differences were noted for single vs multi-level cases. BMP-2 dosage differed in all studies where Lu et al. reported .7-2 mg of rhBMP-2 per level, Tumialan et al. did not report dosage, we expect it to be the same as Lu et al. as it is the same cohort. Tan et al. used .9 mg of rhBMP-2 per level.
Tumialán et al. and Lu et al. reported a 100% fusion rate for all patients who underwent ACDF with the use of BMP-2.8,9 Moreover, Lu et al. observed 100% fusion in the 2- and 3-level BMP-2 groups vs an 82% and 94% fusion rate in the allograft groups, respectively. A significant difference was noted for 2-level fusion, in this retrospective matched cohort (P = .0023). The cohort of Tumialán et al. and Lu et al. also presented results of a 4-level fusion group containing less than 10 patients,8,9 these results were excluded due tot the small group size.
In a retrospective study Tan et al. 18 evaluated fusion rates of 2-level ACDF with ICBG+ BMP-2 vs ICBG and reported an 87.7% fusion rate for the ICBG+BMP-2 group, while a significantly lower fusion rate of 74% was reported in the ICBG group (P = .036). Mean time-to-fusion was 82.6 days in the BMP-2 group, contrasting to a significantly longer mean time-to-fusion of 93.2 days in the ICBG group (P = .013). However, authors did not elaborate on how they determined such a specific time-to-fusion, so considerable bias might contribute to this difference.
Demineralized bone matrix
Two studies used demineralized bone matrix.10,17 The rates of fusion per subject for these studies varied from 88.6% to 94.7% at 12 months and 88.6% to 100% at 24 months. The RCT by Xie et al. compared this to ICBG for which it found a fusion rate of 100% at both time-points. No difference was found for 1-level vs 2-level cases in their RCT. 10
Cellular bone allograft
Three studies reported on the use of 2 different brands of cellular bone allograft (Osteocel and Trinity Evolution®).15,16,19 At 12 months, McAnany et al. (Osteocel) and Peppers et al. (Trinity Evolution®) reported fusion rates at 12 months for 2-levels of 89.4 and 89.3%, respectively.16,19 Additionally, McAnany et al. reported 86.2% for single level fusion at 12 months. At 24 months, Eastlack et al. (Osteocel) reported 91.8% fusion for 1-level and 79.5% fusion for 2-level surgery, 15 this difference was not statistically tested.
Other osteobiologics
Agrillo et al. reported on the use of coralline hydroxy apatite, and found 100% fusion at 12 months for both 1-level and 2-level cases. 13 Dai and Jiang reported on the use of β-Tricalcium Phosphate and found 100% fusion already at 6 months follow up, regardless of the use of anterior plating. 14 Kim et al. reported on the use of a bioactive glass ceramic cage filled with cortical bone fragments that were removed during decompression, and found a fusion rate of 73% at 12 months follow up and 94% at 24 month follow up. 12 No significant differences were found with allograft at both time-points. Unfortunately, no differences were reported between 1 and 2 level cases.
Patient Reported Outcome Measures
A variety of patient reported outcome measures was used in the identified articles. The most frequently used included visual analog scores (VAS) for neck and/or arm pain (n = 6); Neck Disability Index (NDI) (N = 4); and Japanese Orthopedic Association (JOA) score (N = 3).
BMP-2
The study by Tan et al. and the cohort by Lu et al. and Tumialan et al. both reported patient reported outcome measures and all showed significant improvement between pre- and postoperative timepoints for: VAS neck and arm; NDI; JOA; and Nurick scores, respectively.8,9,18 Otherwise, no significant differences were found when comparing the BMP-2 groups with the control groups or when analyzing single-level vs multi-level surgeries.
Demineralized bone matrix
Both studies involving demineralized bone matrix reported significant improvement between pre- and postoperative timepoints for: Odom’s criteria; VAS neck and arm; and JOA.10,17 No data on comparing single to multi-level surgeries was reported. There were no significant differences between the DBM groups and the ICBG control group in the RCT by Xie et al. 10
Cellular bone allograft
The studies by Peppers et al. and Eastlack et al. both reported significant improvement to NDI and VAS scores for neck pain after 12 months and 24 months, respectively. Furthermore, Peppers et al. showed a significant increase in SF-36 score after 6 and 12 months. Eastlack et al. reported significant increases in SF-12 and VAS arm pain at 24 months. The study by McAnany et al. did not include any PROMs. No comparison of single vs multi-level patients was carried out.
Other osteobiologics
Dai and Jiang found significant changes in VAS neck/arm and Japanese Orthopedic Association score between pre-operative and postoperative. However, for these outcome measures, they did not see any additional changes between 3 months up to 24 months. Kim et al. found significant changes in VAS Arm/Neck and NDI. For none of these studies there was any effect reported for single-level vs multi-level cases.
Complications, Adverse Events, Revisions
Overall, there was heterogeneous reporting of complications, adverse events and revisions. With 3 studies reporting no adverse events occured,14,16,17 up to 21% complications, carefully described and categorized.
BMP-2
Complication rates between 12% and 21.6% were reported in studies using BMP-2. The most frequently noted complication was dysphagia. Contrasting results were published when comparing the incidence of dysphagia between the BMP-2 and control groups. Tan et al. 18 did not report a difference, while Tumialán et al. and Lu et al. did.8,9 Tumialán et al. reported severe dysphagia requiring PEG tube placement in 1.5% of the patients, 2 of whom underwent 3-level ACDFs, 1 had a 2-level operation (all BMP-2). They described an increasing number of clinically significant dysphagia cases for multi-level cases as well, 1% in single level, 3.2% in 2-levels and 19.4% in 3-level cases (again al BMP-2). Lu et al., partly reporting on the same cohort, noted a significantly higher complication rate in the 2-level fusion group, and no difference in the 3-level fusion group when comparing BMP-2 group to the control group (12% vs 0% and 14% vs 19% respectively). Moreover, significantly severe dysphagia (SWAL-QOL scale) was seen in the 2-level BMP-2 group than the control group (.778 vs .318). However, the incidence of dysphagia was not higher in the BMP-2 group than in the control group (29% vs 32%). The severity and incidence of dysphagia in the 3-level fusions did not differ (severity: .73 vs .714 and incidence: 46% vs 50% respectively).
Demineralized bone matrix
The complication rate in the studies concerning DBM varied between 0% and 8.6%.10,17 No reoperations or revisions were noted. For none of these studies there was any effect reported for single-level vs multi-level cases.
Cellular bone allograft
Eastlack et al. reported a postoperative complication rate of 4.4%. Moreover, reoperations were performed in 2.2% of patients. 15 In the study by McAnany et al. 7% of patients underwent revision for symptomatic non-union. 19 Additionally, 5.3% of the patients had asymptomatic non-unions and did not require intervention. No other complications were observed. Peppers et al. did not report any complications or reoperations. 16 For none of these studies there was any effect reported for single-level vs multi-level cases.
Other osteobiologics
Agrillo et al. reported no implant related complications or additional surgeries. Transient hoarseness or swallowing deficit was observed in 6.7%, respectively 8.9% of the patients. 13 Kim et al. observed significantly less implant related failures for the glass cage group compared to the allograft group. 12 One case (2.8%) of screw loosening was reported in the glass cage group, while 2 cases (5.7%) of screw loosening and 5 cases (14.3%) cage breakage were noted in the allograft group. Dai and Jiang reported no implanted-related complications or additional surgeries. 14 For none of these studies there was any effect reported for single-level vs multi-level cases.
Other Notable Outcomes
In studies that reported this, length of stay, operative time and blood loss was higher in multi-level cases as compared to single-level. Although no statistical analysis was performed, this is to be expected, with more exposure comes longer operating time and subsequent blood loss. Xie et al. reported significantly shorter operating time, and reduced blood loss when comparing the CS/DBM group to the ICBG group, mostly related to the harvesting of the ICBG. 10 Lu et al. found a weak correlation (correlation coefficient .166, P = .046) between the total dose of BMP-2 used and dysphagia score. 8 Kim et al. reported a significantly higher incidence >3 mm cage subsidence in the allograft group (43%) when compared to the glass cage group (19%). 12 The 2 studies that investigated changes in cervical lordosis did not detect any changes between: pre- and postoperatively; demineralized bone matrix and ICBG; or single-level and multi-level surgery.
Discussion
This systematic review included eleven studies reporting on the use of different osteobiologics in single vs multi-level ACDF. For 2-level surgery, the highest fusion rates were seen in the groups where BMP-2 or DBM were used, comparable to, or slightly outperforming autologous iliac crest bone graft and allograft. At the same time, patient reported outcome measures outcomes did not differ between the different groups of osteobiologics. Overall, the articles reviewed had a considerable risk of bias, and since these results could not be tested in a meta-analysis due to heterogeneity, conclusions should be regarded cautiously and within the context of the low quality of evidence.
Fusion Rates
In the current review the reported fusion rates for all osteobiologics were high and comparable to previously reported fusion rates for single and multi-level ACDF.20,21
Part of the challenge of comparing fusion rates is due to different studies using conflicting criteria to consider fusion as successful. Additionally, a number of different methods of assessing fusion, either by CT-scan or dynamic radiographs, was used. Furthermore, in only half of the included studies independent observers or radiologists evaluated fusion, adding a possible bias to the results.
Previously, attempts were made to standardize the assessment of fusion22,23 and this review should prove as an additional stimulus to formulate a standardized method for fusion assessment.
The variability in post-operative use of a cervical collar or immobilization proved an additional difficulty in comparing the fusion rates of included studies. Since there is no consensus on the effect of a collar on fusion rates or functional outcomes, 24 this too may prove to be a possible bias.
Lastly, there was a considerable amount of heterogeneity in the use of anterior plating in the included studies. Previous studies showed significantly higher fusion rates when anterior plates were being used in single and multi-level ACDF.25,26 The effect of anterior plates may obscure the effect of the different osteobiologics in this review.
Patient Reported Outcome Measures
Functional results improved significantly when compared to baseline values in all studies in the present review. However, none of the studies reported a difference in clinical outcome when the osteobiologic group was compared to the control group. Additionally, either no comparison of single vs multi-level surgery was carried out, or no difference was observed when a comparison was made.
Similar to fusion rate assessment, there is a broad range of patient reported outcome measures used (supplemental document, Table 3), indicating, that there is no consensus on which tool should be used in reporting clinical outcomes in ACDF. 27
Complications, Adverse Events, Revisions
The most reported, and previously studied, complication in the current review is dysphagia, most notably in the BMP-2 studies.
In the cohort studied by Tumialán et al. and Lu et al. severe dysphagia requiring a PEG tube was reported in 3 patients (2 patients with 3-level surgery, 1 patient with 2-level surgery).8,9 Moreover, significantly severe dysphagia, according to the SQAL-QOL scale, was reported in the 2-level BMP-2 group, however the incidence of dysphagia was comparable. Interestingly, the severity and incidence of dysphagia in the 3-level fusion groups did not differ. A possible explanation may be that other factors, beside the use of BMP-2 (surgical exposure, tissue manipulation), induce dysphagia in multi-level ACDF. Furthermore, the authors report reducing the dose of BMP-2 from 2.1 to 0.7mg per level in an attempt to minimize the complications. Unfortunately, they did not report on the positive and negative effects of this dose-reduction. Contrastingly, Tan et al. did not report differences in dysphagia incidence between groups at all. 18
Furthermore, Lu et al. performed a correlation analysis between the total dose of BMP-2 used and the dysphagia score, and reported a weak correlation. This implies that, while the dose of BMP-2 influences the severity of dysphagia, it is only 1 of many factors playing a role in dysphagia after ACDF.
Previously, studies showed that BMP was associated with several airway obstruction related complications in cervical spine procedures, including ACDF.28,29 To this end, in 2008, the Food and Drug Administration issued a warning highlighting the occurrence of airway obstruction related complications when using BMP. 30 A more recent study also reported that BMP was shown to induce significantly more dysphagia 31 when compared to other bone graft substitutes. In the current review this evidence is less explicit, and other factors may play an equal or larger role in the incidence of dysphagia in multi-level ACDF. 32 Conceivably, there are options to mitigate the dysphagia risk in multi-level ACDF such as steroids. 33 However, the occurrence of possibly grave airway obstruction related complications has to be kept in mind when considering the use of BMP-2 in single- or multi-level ACDF.
Revisions were only reported in the studies by Eastlack et al. (2.2%) 15 and McAnany et al. (7%) 20 where patient were treated with a mesenchymal stem cell allograft. However, no data was published on whether the reoperations where single or multi-level ACDF. Previously published results on revision rates after multi-level ACDF show revision rates up to 35%, significantly higher than the results in the current review where osteobiologics were used. 4
Strengths and Limitations
The strength of the current review lies in its methodology. Assessment of articles and data was performed by a number of reviewers independently, and geographic differences and possible bias was minimalized by including reviewers from Europe, Asia and Latin America. Moreover, strictly using PRISMA and GRADE guidelines proved to be an additional strength of this systematic review.
An obvious limitation of the current review is the lack of studies reporting specifically on the effect of osteobiologics on single vs multi-level ACDF. Most included studies did not specify results based on levels treated, except for earlier discussed results, plus the amount of results on 3-level or more than 3-level fusions was very limited. This precludes making stringent recommendations. Furthermore, the included studies almost uniformly possessed a moderately high to high risk of bias. Lastly, the heterogeneity of outcome parameters made performing a meta-analysis impossible.
Conclusion
This systematic review presents preliminary evidence for the use of BMP-2 in 2-level ACDF. However, there appears to be an increase in incidence and severity of dysphagia when BMP-2 is used. Demineralized bone matrix seems to be a reasonable alternative to ICBG if additional graft is needed. Based on the studies included in this review, only limited conclusions can be drawn specifically on single vs multi-level surgeries. Moreover, the results should be regarded cautiously since the GRADE approach rated the level-of-certainty as ‘very low’. Further research should explore the use of BMP-2 in single vs multi-level ACDF, and with attention to airway obstruction related complications. Furthermore, as earlier mentioned, the use of standardized criteria for fusion assessment, patient reported outcome measures and adverse events is necessary to compare outcomes across studies.
Supplemental Material
Supplemental Material - The Use of Osteobiologics in Single versus Multi-Level Anterior Cervical Discectomy and Fusion: A Systematic Review
Supplemental Material for The Use of Osteobiologics in Single versus Multi-Level Anterior Cervical Discectomy and Fusion: A Systematic Review by Jim Hoffmann, Guillermo A. Ricciardi, Ratko Yurac, Hans-Jörg Meisel, Zorica Buser, Bangping Qian, Pieter-Paul A. Vergroesen, and AO Spine Knowledge Forum Degenerative in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.