
Abstract
Study design
Single centre, cross-sectional study.
Objectives
The objective is to report the prevalence of spondylolisthesis and retrolisthesis, analyse both conditions in terms of the affected levels and severity, as well as identify their risk factors.
Methods
A review of clinical data and radiographic images of consecutive spine patients seen in outpatient clinics over a 1-month period is performed. Images are obtained using the EOS® technology under standardised protocol, and radiographic measurements were performed by 2 independent, blinded spine surgeons. The prevalence of both conditions were shown and categorised based on the spinal level involvement and severity. Associated risk factors were identified.
Results
A total of 256 subjects (46.1% males) with 2304 discs from T9/10 to L5/S1 were studied. Their mean age was 52.2(± 18.7) years. The overall prevalence of spondylolisthesis and retrolisthesis was 25.9% and 17.1% respectively. Spondylolisthesis occurs frequently at L4/5(16.3%), and retrolisthesis at L3/4(6.8%). Majority of the patients with spondylolisthesis had a Grade I slip (84.3%), while those with retrolisthesis had a Grade I slip. The presence of spondylolisthesis was found associated with increased age (P < .001), female gender (OR: 2.310; P = .005), predominantly sitting occupations (OR:2.421; P = .008), higher American Society of Anaesthesiology grades (P = .001), and lower limb radiculopathy (OR: 2.175; P = .007). Patients with spondylolisthesis had larger Pelvic Incidence (P < .001), Pelvic Tilt (P < .001) and Knee alignment angle (P = .011), but smaller Thoracolumbar junctional angle (P = .008), Spinocoxa angle (P = .007). Retrolisthesis was associated with a larger Thoracolumbar junctional angle (P =.039).
Conclusion
This is the first study that details the prevalence of spondylolisthesis and retrolisthesis simultaneously, using the EOS technology and updated sagittal radiographic parameters. It allows better understanding of both conditions, their mutual relationship, and associated clinical and radiographic risk factors.
Highlights
1. The prevalence of spondylolisthesis and retrolisthesis was 25.9% and 17.1% respectively. Spondylolisthesis occurs frequently at L4/5 (16.3%), and retrolisthesis at L3/4 (6.8%). Majority of the patients with spondylolisthesis had a Grade I slip (84.3%), while all those with retrolisthesis had a Grade I slip. 2. The presence of spondylolisthesis was found to be associated with increased age of subject (p < 0.001), female gender (OR 2.310; p = 0.005), predominantly sitting occupations (OR = 2.421; P = 0.008, higher American Society of Anaesthesiology grades (P = 0.001), and lower limb radiculopathy (OR = 2.175; P = 0.007). 3. Patients with spondylolisthesis had larger Pelvic Incidence (P < 0.001), Pelvic Tilt (P < 0.001), and Knee alignment angle (P = 0.011), but smaller Thoracolumbar junctional angle (P = 0.008), and Spinocoxa angle (P = 0.007), while retrolisthesis was associated with a larger Thoracolumbar junctional angle (P = 0.039). These findings likely reflect the primary pathology and compensatory mechanisms in whole body balancing. 4. Associations between level-specific spinopelvic parameters lumbar incidence, lumbar tilt, and lumbar slope and vertebral translations at the corresponding levels reflect the importance of recognizing force mechanics in the spine. 5. The use of EOS technology and updated sagittal radiographic parameters in this study allowed the understanding of both conditions, their mutual relationship, and associated clinical and radiographic risk factors. It will lay the platform for future management of both conditions.
Introduction
Spondylolisthesis and retrolisthesis describe the forward and backward translation of a vertebra with reference to its adjacent lower vertebra respectively. While the epidemiology and pathophysiology of spondylolisthesis may have been extensively studied1-3, retrolisthesis is less known 4 . This could be due to a relatively lower prevalence5,6, or its more quiescent nature which results in a paucity of evidence demonstrating its clinical significance 6 . The underlying causes for both conditions may differ 7 , hence resulting in them often being studied separately. However, both conditions require a nett force to translate one vertebra over another, which may indicate that biomechanically these 2 conditions may be related. Therefore, it would be necessary to report the prevalence of both conditions together, and document their clinical and radiological risk factors.
The rapidly evolving concepts in adult spinal deformity surgery have highlighted the importance of realigning the sagittal profile of the spine8,9. Considerations in spinal realignment include assessment of a deformity using the sagittal vertical axis (SVA), and the pelvic incidence (PI) – lumbar lordosis (LL) discrepancy, as well as appreciating the extent of spinopelvic compensation using the pelvic tilt (PT)9,10. Retrolisthesis, which was once regarded as a possible form of spinal instability of unknown significance 11 , is now being increasingly recognized today as a compensatory process which occurs in patients with positive sagittal imbalance9,11. With a greater forward lean of the spine in ageing, or following various spinal pathologies, retrolisthesis may occur in an attempt to keep the body balance within the cone of economy12,13.
To our knowledge, this is the first epidemiological study that investigates the prevalence of spondylolisthesis and retrolisthesis simultaneously using the modern EOS® technology, which is the current gold standard modality for taking true-to-proportion and true-to-axis whole body images for the assessment of spinal alignment14,15. Although previous studies have reported on the epidemiology of these conditions, no prior study have been carried out to investigate their relationship with whole body radiographic parameters, which is pivotal in the understanding of adult spinal deformity today. This study also aims to identify associated clinical and updated radiological risk factors in both conditions.
Methodology
Study Design
This was a single centre, cross-sectional study on the prevalence of degenerative spondylolisthesis and retrolisthesis in the thoracolumbar and lumbar spine using the EOS® technology (EOS® imaging, Paris, France) 16 , with identification of associated risk factors. All images within the centre were obtained using the EOS® technology. This study is approved by the local ethics board committee. Informed consent was obtained from each patient for inclusion in the study.
Study Population
We enrolled all first visit patients seen at the spine centre over a 1-month period. Patients with spinal scoliosis, either diagnosed clinically by a positive Adam’s forward bend test, or radiologically with coronal Cobb angle measurements >10° shown on EOS, were excluded from the study sample. This is to avoid misinterpretation of sagittal and coronal plane deformities due to spinal rotation. As a result, a total of 256 subjects (136 women and 120 men) out of 275 were enrolled.
Radiographic Examination
Following clinical assessment by the attending spine specialist, all subjects underwent anteroposterior and lateral whole body radiographs using EOS® technology. This technology is the current gold standard modality for taking true-to-proportion and true-to-axis whole body images for the accurate assessment of spinal alignment 14,15.
To promote standardization, pictorial charts demonstrating how to position for the EOS imaging were displayed by the EOS® machine. Uniformity of this posture was further reinforced through standardized verbal instructions given by the radiographer as follows: “stand as straight as possible without leaning forwards or backwards, and touch your collarbones with your fingers”. All images were performed by trained radiographers with over 3 years of experience in EOS® technology.
Data Collection
A review of electronic medical case records was conducted for all patients identified in the study. Clinical data obtained include patient demography (age, gender, ethnicity, occupation), American Society of Anaesthesiology (ASA) Physical Status Classification, and symptomology (presence of previous or ongoing axial back pain or lower limb radiculopathy). The subjects’ occupations were categorised into ‘predominantly standing’ or ‘predominantly sitting’.
Radiographic Measurements
The radiographs obtained were stored on the hospital’s secured server and accessed using Centricity Enterprise Web version 3.0 (GE Medical Systems Information Technologies, Barrington, IL, USA) for measurements of spinal parameters. Measurements were performed by 2 independent and blinded spine surgeons, and an average of their readings was recorded.
Vertebral translation was deemed to be present if the translation was measured to be ≥3mm. The radiographic outcomes measures include: 1. Presence or absence of spondylolisthesis and retrolisthesis; 2. The level affected; 3. Severity assessment of both conditions using Meyerding’s classification . Other radiographical covariates measured can be divided into 4 main categories of assessment and include: 1. Global spinal alignment; 2. Regional spinal angles; 3. Spinopelvic angles, and 4. Lower limb angles.
For global spinal alignment, Sagittal Vertical Axis (SVA) was measured as the horizontal offset between the imaginary sagittal C7 plumb line and the posterosuperior corner of the S1 vertebral body. T12SVA measures a similar offset but uses an imaginary plumb line from T12 instead.
For regional spinal alignment, thoracic and lumbar spinal curvatures were performed using the Cobb method. Global thoracic angle (GTA) was taken as the angle between the superior endplate of T1and the superior endplate of T12. Thoracolumbar junctional angle (TLA) was taken as the angle between the superior endplate of T10 and the inferior endplate of L2. Global lumbar angle (GLA) was taken as the inferior endplate of T12 and the superior endplate of S1.
Spinopelvic parameters such as PI, PT and SS, as well as T1-slope were measured using standard methods described in the literature. To ascertain the individual relationship between the vertebra alignment and the hip, the spatial orientation of each vertebra is assessed using lumbar incidence (LI), lumbar tilt (LT) and lumbar slope (LS) as proposed by Hey et al 17 . This is conceptually identical to the PI, PT and SS used for S1 vertebra, such that LI = LT + LS for any given lumbar vertebra.
Femoral alignment angle (FAA) was taken as the acute angle subtended by the femoral axis (midpoint of bicoxafemoral hip center to midpoint of both mid-Blumensaat lines) and the vertical axis (see Figure 1). Knee alignment angle (KAA) was taken as the acute angle between the femoral axis and the tibia axis (midpoint of both mid-tibia plateau to the midpoint of both mid-tibia plafond). Spinocoxa angle (SCA), was taken as the acute angle subtended by the perpendicular to the superior endplate of the inflection vertebra and the femoral axis. The inflection vertebra is defined as the most tilted vertebra on the lateral EOS® image that marks the distal end of the kyphosis and proximal end of the lordosis at the thoracolumbar junction. It is used for the measurements of SCA and Inflection to S1 angle (IL). Sketch diagram showing the differences in sagittal alignment parameters between patients with and without spondylolisthesis.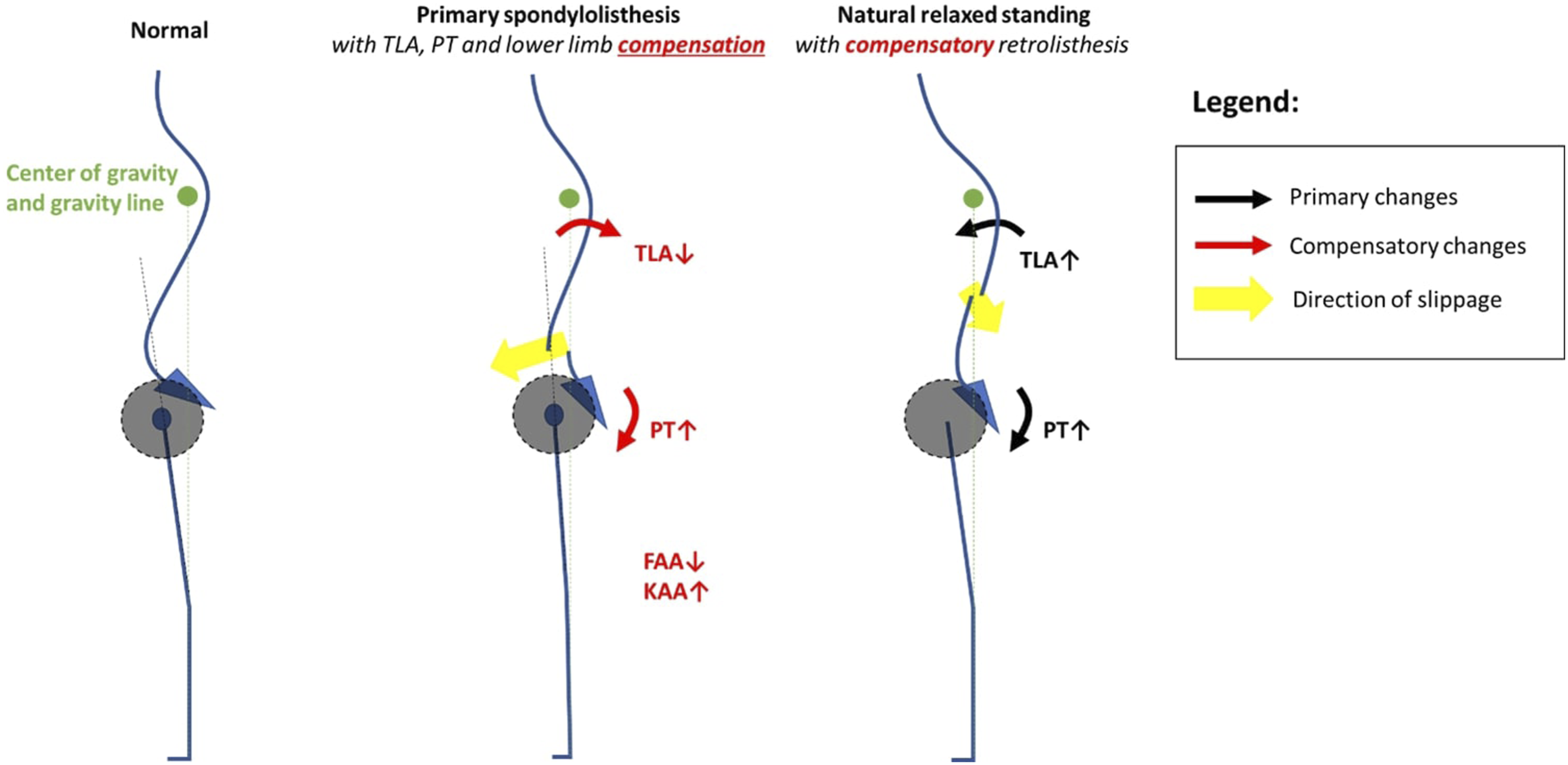
Statistical Analysis
Data collected was compiled in Microsoft Excel 2011 (Version 14.2.4). Two-sided statistical analysis was carried out using Statistical Package for the Social Sciences version 22.0 with significance set at P<.05. Categorical variables are described in percentages and continuous variables as means with standard deviations.
The prevalence of both spondylolisthesis and retrolisthesis, their involved spinal levels and severities were presented. Their associations with the other clinical and radiological parameters were also analysed using univariate Chi Squared and Fisher Exact Test for categorical variables, Mann-Whitney U Test for ordinal variables and, Independent-Samples t-Test for continuous variables.
Results
Sample Characteristics
Overall population sample characteristics
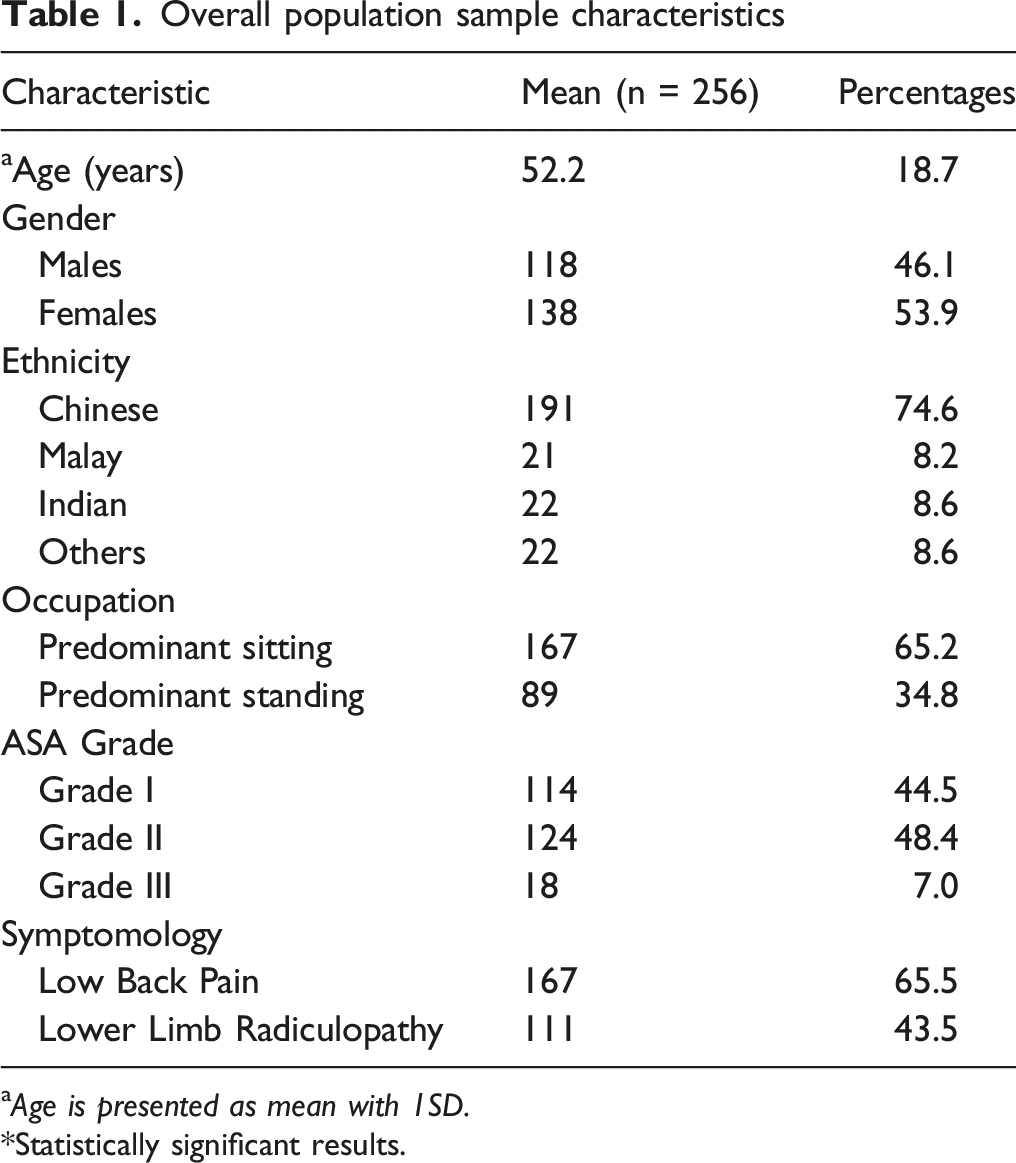
a Age is presented as mean with 1SD.
Statistically significant results.
The most common ethnic group was Chinese (74.6%), which is consistent with the nation’s population demographics. The majority of subjects (65.2%) had predominantly sitting occupations. 92.9% of the subjects had ASA grade of Grade I-II. (Table 1). 65.5% and 43.5% of the population have symptoms of low back pain and lower limb radiculopathy respectively.
Prevalence of Spondylolisthesis and Retrolisthesis
Prevalence of Thoracolumbar and Lumbar Spondylolisthesis and Retrolisthesis by spinal levels
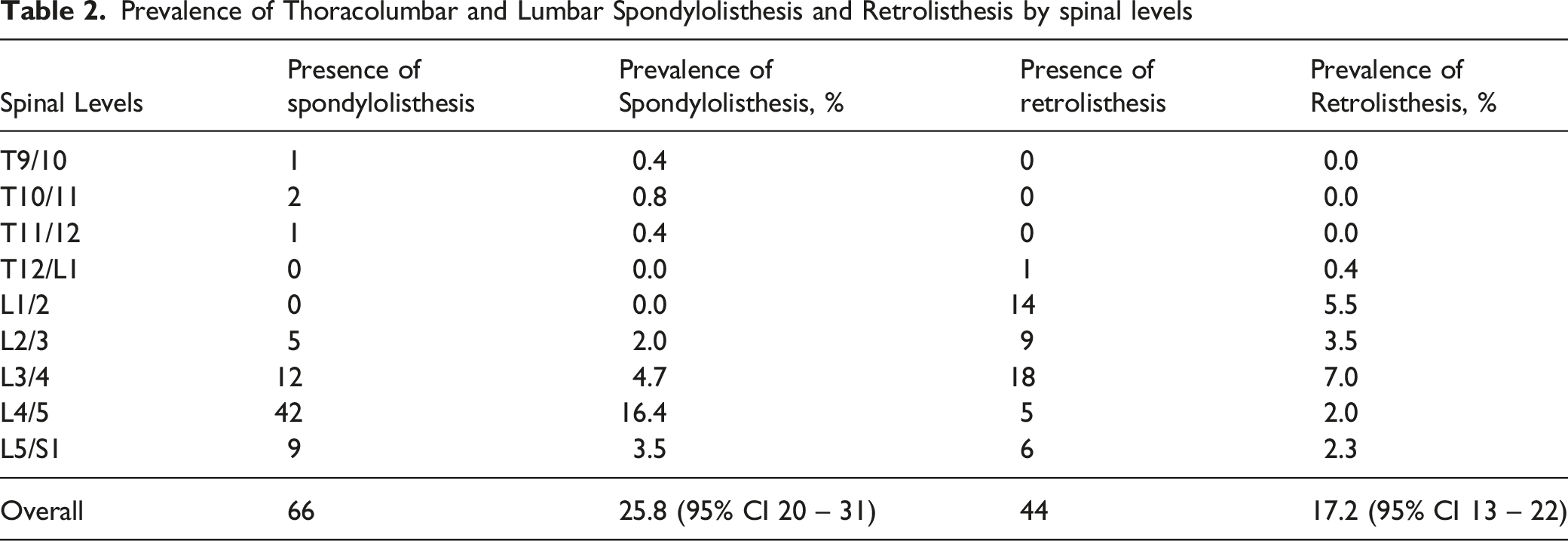
In terms of the level involved, spondylolisthesis occurs frequently at L4/5 (16.4%), followed by L3/4 (4.7%) and L5/S1 (3.5%). Retrolisthesis is more common at L3/4 (7.0%) followed by L1/2 (5.5%) and L2/3 (3.5%) (Table 2). 84.3% of the spondylolisthesis are Grade I (Meyerding’s classification) while the remaining 15.7% are Grade II. All retrolisthesis are classified as Grade I.
Clinical Characteristics of Patients With Spondylolisthesis and Retrolisthesis
Relationship between patient characteristics (stratified) and the prevalence of spondylolisthesis and retrolisthesis
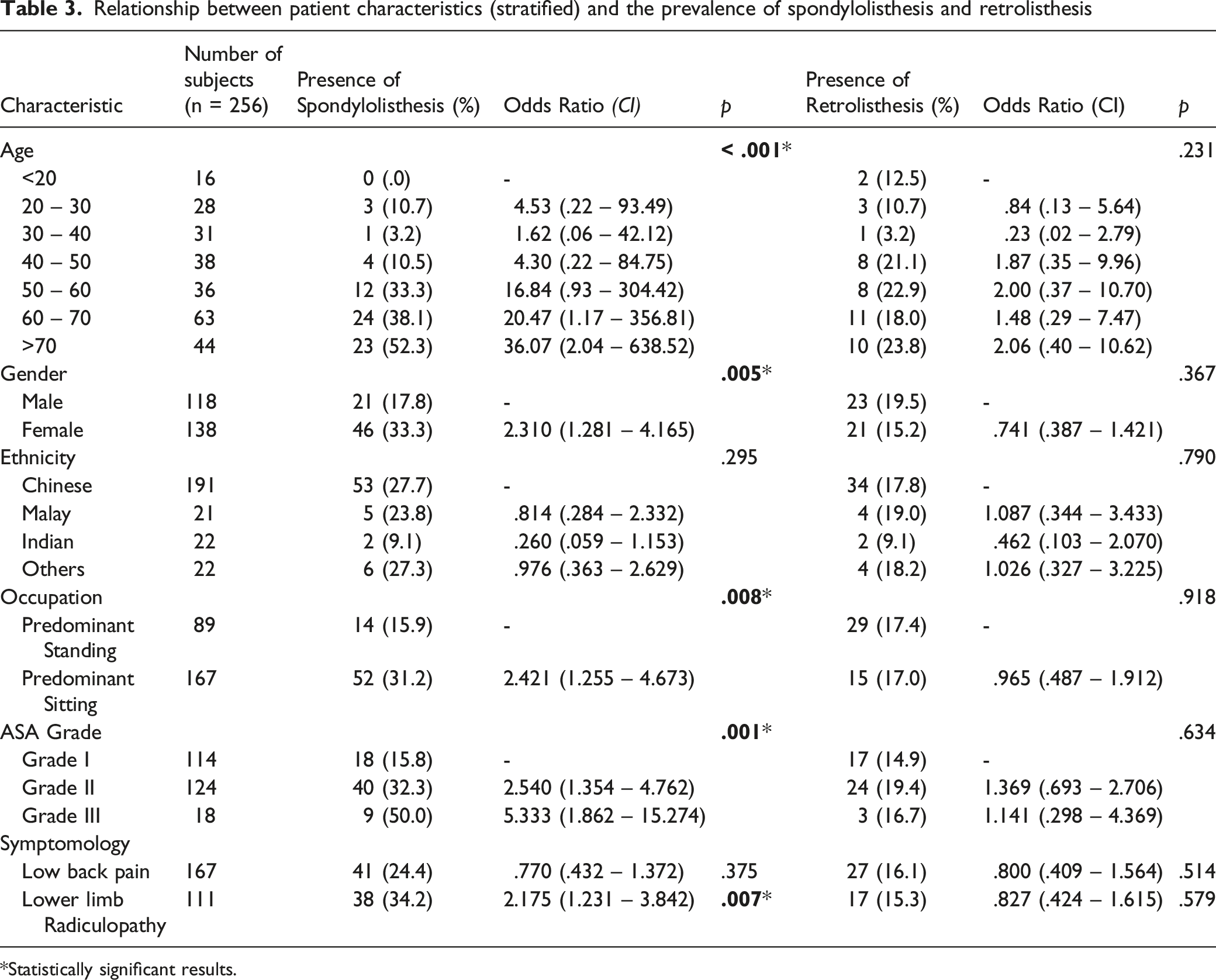
Statistically significant results.
The presence of spondylolisthesis was found to be associated with increased age of subject (P<.001), female gender (OR 2.31; P=.005), predominantly sitting occupations (OR = 2.42; P=.008) (Table 3). In addition, compared to patients with ASA Grade I, Grade II and III patients have an increased association with spondylolisthesis (P=.001). No significant differences were found between the occurrence of spondylolisthesis and patient ethnicity.
Axial symptoms correlate poorly with spondylolisthesis and retrolisthesis. However, lower limb radiculopathy was found to be associated with lumbar spondylolisthesis (OR = 2.18; P=.007). No significant associations were found for retrolisthesis.
Radiological Characteristics of Patients With Spondylolisthesis and Retrolisthesis
Relationship between radiological parameters and the prevalence of spondylolisthesis and retrolisthesis
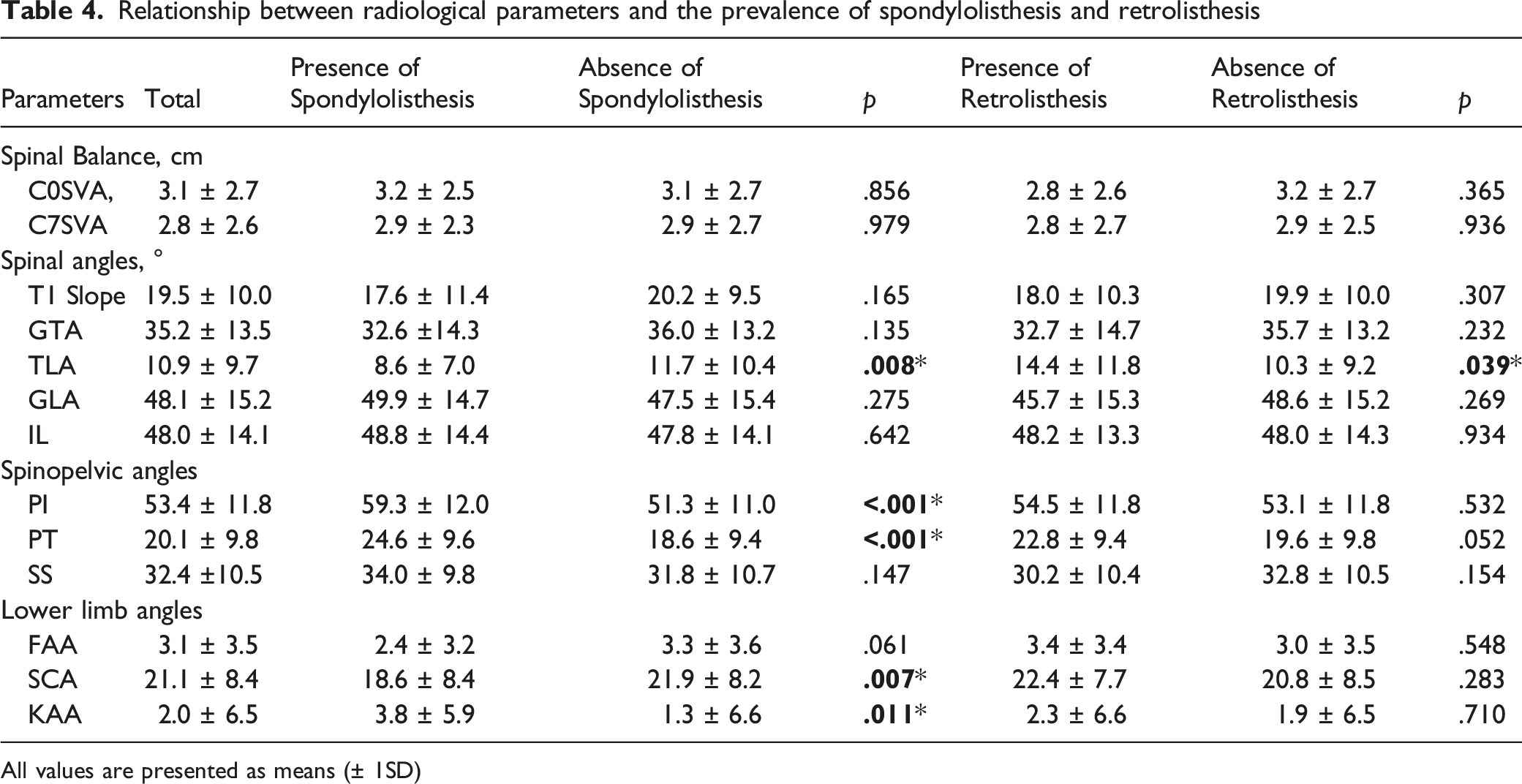
All values are presented as means (± 1SD)
In terms of level-specific spinopelvic parameters and their association with spondylolisthesis and retrolisthesis at the said level, larger L4I and L4S were associated with L3/4 spondylolisthesis (P=.003 and P=.045 respectively) and absence of L3/4 retrolisthesis is associated with L4S (P=.011) but not L4I (P=.062). Larger L5I (P<.001), L5T (P=.001) and L5S (P=.015) were associated with L4/5 spondylolisthesis. A larger SS is associated with absence of retrolisthesis (P=.033).
Discussion
Spondylolisthesis and retrolisthesis describe abnormal vertebral translations of the spine in the sagittal plane. The former occurs when a vertebra body translates forward over its caudal counterpart, and the latter occurs with backward translation. Generally, spondylolisthesis is perceived as abnormal, and may lead to symptoms such as back pain and/or leg pain18,19. Hypermobility of the affected segments, which can be further assessed using stress radiography 20 or MRI 21 , can result in a wide range of clinical presentations 22 . Several radiological parameters that predict the progression of spondylolisthesis, can be used to guide management –1) the slip angle which essentially measures the angle difference between endplates of 2 involved vertebra23,24, 2) the sacral inclination which can be regarded as a variant of the slip angle as it uses the longitudinal axis of the sacrum instead of the superior endplate 23 , and 3) the lumbosacral angle aka sacral slope 25 . In the presence of symptoms that are refractory to conservative management, especially in patients with high risk of disease progression, surgery is often necessary 25 . The recommended surgery involves decompression of neural structures with or without instrumented fusion of the affected spinal segment26,27. This has been shown in the SPORT trial to demonstrate superior results compared to non-operative management up to 4 years 28 .
The prevalence of spondylolisthesis in the general population has been reported to be between 6 to 10%, and varies depending on the type of spondylolisthesis and imaging modality used29,30. The prevalence of this condition in a random community sample via non-weight bearing CT studies was found to be 11.5% 31 . In our study, the prevalence was expectedly higher (25.8%) due to our population sample which recruits pooled patients visiting a tertiary healthcare center. An Osteoporotic Fractures in Men Study (MrOS) study conducted on elderly men found the prevalence of spondylolisthesis to be even higher at 31% 32 . However, this could be attributable to the differences in prevalence found across age groups29,33 and gender 33 . Nevertheless, the use of EOS in this study allowed accurate assessment of whole-body radiographic parameters to give the best analysis of risk factors associated with both conditions. Retrolisthesis, unlike spondylolisthesis, is less studied and its true value unknown 4 . This is the first, and largest study that uses EOS imaging to investigate the prevalence of retrolisthesis, which we found to be 17.1%. Contrary to an earlier study, this prevalence is higher and may again be attributed to differences in the studied populations 34 .
Our study showed that spondylolisthesis and retrolisthesis are more prevalent in older ages, which may be attributed to its association with spinal degeneration 35 . Unsurprisingly, higher ASA grades which are expected in the older age groups, are also found to be associated with spondylolisthesis 36 . When age increases, the spine goes into progressive kyphosis with recruitment of compensatory mechanisms to keep itself balanced 12 . The sudden increase in prevalence of spondylolisthesis in patients above 50 years old is likely reflective of exhausted physiological reserves, with acute worsening of the condition. This is supported by the concomitant findings of sagittal compensation such as increased PT (P < .001) and KAA (P = .011), and SCA (P = .007) in patients with spondylolisthesis37,38 (Figure 1). The prevalence of retrolisthesis, on the other hand, is seen in all age groups and increases gradually with age, suggesting its possible compensatory role in sagittal balancing rather than being the primary pathology39-42. Unlike spondylolisthesis which is often a pathological problem resulting from shear forces residing in the lordotic lumbar spine43,44, as well as forward bending postures and activities 45 , primary retrolisthesis is less common as minimal postures or activities drive the spine backwards. Increased TLA in patients with retrolisthesis are suggestive of adaptive changes following prolonged natural standing 41 or sitting postures40,41 where the patient employs posterior ligamentous complex to balance and conserve energy. This shifts the body’s centre of gravity backwards likely resulting in a backward shear force on the thoracolumbar and upper lumber vertebrae.
Females were found to have an increased prevalence of spondylolisthesis as compared to males. This may be due to the influence that hormones have on ligamentous laxity 46 . This is analogous to female patients with adolescent idiopathic scoliosis, where ligamentous laxity has also been identified as a possible contributing factor 47 . The association between lower limb pain with spondylolisthesis but not with lower back pain likely reflects the non-specificity of the latter symptom 31 , such that having a spondylolisthesis does not necessarily explain the cause of low back pain. However, lower limb pain which is often concordant with stenosis at the level of spondylolisthesis likely explains the symptoms and localises the pathology 46 . This emphasizes the need to ascertain the true cause of low back pain even in the presence of a degenerative spondylolisthesis before instituting surgical treatment.
While it is possible that both spondylolisthesis and retrolisthesis vary somewhat in terms of aetiology, the result of vertebra translation should depend on the similar force principles. A forward-directed nett force should lead to spondylolisthesis and a backward-directed nett force retrolisthesis. Determinants of these forces include the posture and activities of the patient40,48-50, which in turn influences the force magnitude on each lumbar vertebra. In our study, the higher prevalence of spondylolisthesis from L3/4 to L5/S1 levels and retrolisthesis from L1/2 to L3/4 further substantiates this point. Since lordosis occurs in the lumbar spine particularly the lower segments regardless of posture, and lower segments have a positive slope angle, under the pull of gravity, forward vertebral translation naturally ensues (Figure 2). Cranial to the apex of the lumbar curve, which usually resides in L3/4, an opposite force vector results in backward vertebral translation. Moreover, when sitting posture of the spine is considered, more forward force is generated (Figure 2). This has been shown in studies comparing standing and sitting postures40,41,51,52 and explains the higher prevalence of spondylolisthesis in predominantly sitting occupations found in this study. Diagrammatic representation of the proposed mechanisms that results in spondylolisthesis.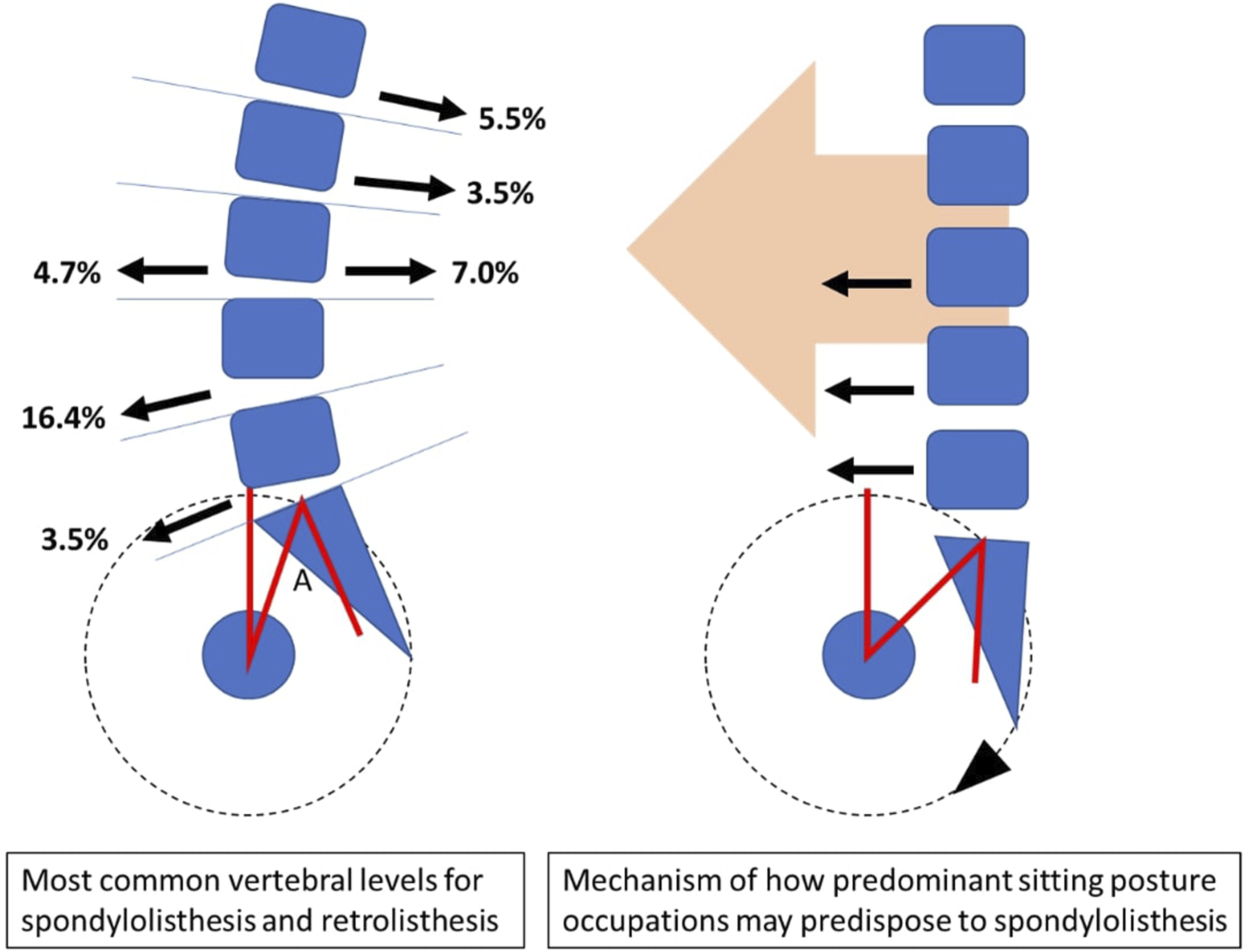
In this study, PI is found to be higher in patients with spondylolisthesis as compared to those without (P<.001). This suggests that individual-specific pelvic morphology is a risk factor for this condition 53 . In addition, increased PT was also found to be associated with spondylolisthesis. Although PT varies with posture40,41,45 and its increase is likely contributed by spinopelvic compensation mentioned earlier54,55, a paradoxic concomitant increase in SS, which should behave reciprocally, reinforces that this increase is likely to be also contributed by pelvic morphology. This can be further explained by the equation PI = PT + SS 56 , where patients with a large PI naturally bears a larger PT and SS. Further findings of larger L5I (P<.001), L5T (P=.001) and L5S (P=.015) associated with L4/5 spondylolisthesis substantiates this hypothesis. Failure to observe similar phenomenon in other intervertebral levels is likely due to the low prevalence of spondylolisthesis at those levels.
A larger L4I and L4S, being associated with spondylolisthesis (P=.003 and P=.045 respectively), is concordant with the existing literature which supports the association between slope angles and spondylolisthesis
57
. The presence of retrolisthesis in association with a smaller L4S (P=.011), as well as a smaller SS (P=.033) is interesting and may be due to postural changes in sitting that stresses the spine in pelvic retroversion. From a clinical perspective, the authors hypothesize that tilt angles are more at risk of slippage in the more cranial vertebrae could be due to the rather horizontal sacral slope (Figure 3). On the contrary, slope angles appear important at L3/4 and L4/5 levels due to the proximity of vertebra to the gravity line
48
. Only a trend towards SS predicting L5/S1 spondylolisthesis is observed could be related to the relative stiffness at the L5/S1 level in some patients due to transitional vertebra58,59 and iliolumbar ligaments
60
. Diagrammatic representation of how level-specific spinopelvic parameters LI, LT and LS may influence the occurrence of spondylolisthesis or retrolisthesis at common levels.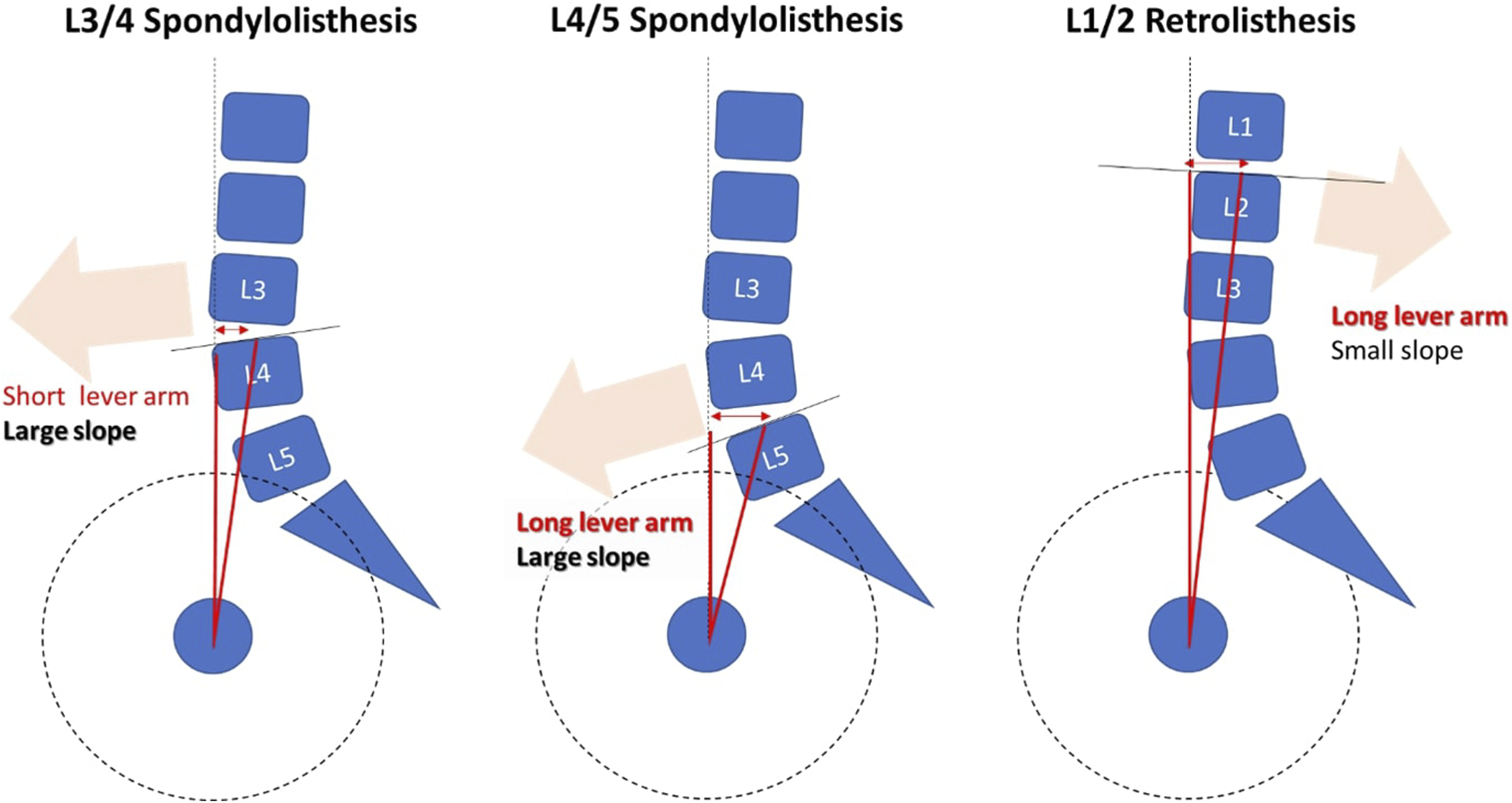
There are 3 limitations to this study. First, despite having a large sample size of 256 patients, this study was insufficiently powered to conclude if spondylolisthesis predisposes to cranial level retrolisthesis. This would be interesting since retrolisthesis can be a physiological phenomenon alone, or a compensatory mechanism for forward sagittal spinal imbalance 42 where spondylolisthesis could have influenced the opposite translation of the cranial vertebrae. In order to resolve this, future larger scale studies with patients that have high grade spondylolisthesis and substantial forward imbalance can be performed. Second, the sole usage of standing lateral radiographs for identification of spondylolisthesis and retrolisthesis may not reflect the true behaviour of vertebral translation, which may vary with changes in spinal alignment. Flexion-extension stress radiographs or imaging in other postures, such as seating, may improve the detection of unstable spondylolisthesis and provide additional information useful for clinical decision making and surgical planning 20 . In fact, as alignment changes from standing to sitting, the prevalence may change 61 . Nonetheless, we hypothesize that sitting occupations predisposes to spondylolisthesis but future large, powered studies are required to confirm this finding. Thirdly, in our cohort study, there were no high-grade spondylolisthesis. As low-grade spondylolisthesis is much more common, our study focuses on low-grade spondylolisthesis 62 .
In conclusion, this is the first study that documents the prevalence of spondylolisthesis and retrolisthesis simultaneously using the EOS technology, which is the gold standard radiological modality for the study of spinal and whole body alignment. It allows the further appreciation of both conditions, their mutual relationship, and associations with other clinical and radiological parameters. The information obtained incorporates the current state-of-art concepts in adult spinal deformity such as sagittal imbalance, compensatory mechanisms, and the potential clinical impact of postural variations. This study will continue to lay the platform for further studies of both conditions.
Footnotes
Acknowledgement
We thank Dr Lin Shuxun (Department of Orthopaedic Surgery, Ng Teng Fong General Hospital) for useful discussion and contributing to the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study is approved by the local ethics board committee: NHG Domain Specific Review Board (DSRB): 2016/01 102.