
Abstract
Study Design
Randomized controlled trial.
Objectives
To compare the effect of posterolateral fusion (PLF) and posterior lumbar interbody fusion (PLIF) on sagittal radiographic parameters in patients with low-grade isthmic spondylolisthesis. Additionally, to explore the correlation between changes in these parameters and clinical outcomes.
Methods
Forty-six consecutive patients with single-level low-grade isthmic spondylolisthesis were initially enrolled. They were randomly assigned to undergo either PLF or PLIF. Patients were followed up for at least 24 months. Radiographic outcomes included pelvic incidence, pelvic tilt, sacral slope, lumbar lordosis, sagittal vertical axis, T1 pelvic angle, slip angle, slip degree and disc height. Clinical outcomes were assessed by the Oswestry Disability Index (ODI) and visual analogue scale (VAS).
Results
Four participants were lost to follow-up. Of the remaining 42 patients, 29 were female. The mean age was 40.23 ± 10.25 years in the PLF group and 35.81 ± 10.58 years in the PLIF group. There was a statistically significant greater correction of all radiographic parameters in the PLIF group. The ODI and VAS improved significantly in both groups, with no significant differences between the two groups. Changes in the ODI and VAS were significantly correlated with changes in disc height, slip angle and lumbar lordosis.
Conclusions
In patients with low-grade isthmic spondylolisthesis, PLIF demonstrates superior efficacy compared to PLF in correcting sagittal radiographic parameters. Nevertheless, this distinction does not seem to influence short-term clinical results. Restoring disc height, correcting the slip angle, and reestablishing normal lumbar lordosis are crucial steps in the surgical management of isthmic spondylolisthesis.
Keywords
Introduction
Isthmic spondylolisthesis is a condition in which there is a forward slippage of one vertebra over the one below due to a defect in the pars interarticularis. This condition can lead to spinal instability, resulting in chronic low back pain and disability. The exact cause of isthmic spondylolisthesis is still undetermined; however, abnormal spinopelvic parameters play an important role not only in the development of isthmic spondylolisthesis but also in its progression.1-4
Posterior lumbar interbody fusion (PLIF) and posterolateral lumbar fusion (PLF) are commonly performed for the treatment of low-grade single-level isthmic spondylolisthesis, both of which aim to restore spinal stability and alleviate symptoms. However, the optimal surgical technique for this condition is still debated, and the effect of these techniques on sagittal radiographic parameters remains unclear.
Several studies have compared PLF and PLIF for the treatment of isthmic spondylolisthesis, primarily focusing on fusion rates and clinical outcomes.5-11 However, only a few reports have explored the comparison between the two techniques in terms of their effect on sagittal radiographic parameters or their clinical correlation, and none of them were randomized controlled trials.12-14 There is growing evidence suggesting that radiographic sagittal parameters play a significant role in the surgical outcome of spinal fusion procedures. Proper sagittal alignment helps distribute the load across the spinal column and pelvic girdle, reducing the risk of complications such as adjacent segment disease, implant failure, and pseudarthrosis.15-17 To the best of our knowledge, this study is the first randomized controlled trial that aims to compare sagittal radiographic parameters after PLF and PLIF in patients with single-level low-grade isthmic spondylolisthesis and to study the correlation between changes in these parameters and clinical outcome.
Patients and Methods
Trial Design and Registration
This prospective randomized controlled trial received approval from our institutional review board (17100676) and was registered with ClinicalTrials.gov on March 15, 2019 (identifier: NCT03877341). The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants provided written informed consent before enrollment in the study. This study was reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Participant Selection
Between April 2019 and February 2021, 46 consecutive patients were enrolled in the study. The inclusion criteria were adult patients with low-grade (Meyerding Ι, ΙΙ) single-level isthmic spondylolisthesis who failed to respond to conservative treatment for more than 6 months. Patients with degenerative spondylolisthesis, multiple-level spondylolisthesis, high-grade spondylolisthesis (Meyerding ΙΙΙ, IV, V), previous lumbar spine surgery, lumbar scoliosis, or other spinal disorders that could affect the study outcomes were excluded. The final follow-up of the last patient was completed in February 2023.
Sample Size, Randomization and Blinding
Sample size calculation was carried out using OpenEpi software. 18 The estimated sample size was 46 participants, with a 5% level of significance and 80% statistical power. The participants were randomly assigned to one of the two surgical techniques using a computer-generated randomization sequence, with an allocation ratio of 1:1 in fixed blocks of 2. This allocation sequence was enclosed in sequentially numbered, opaque, sealed envelopes. The principal investigator opened the envelope the day before the surgery and informed the surgeon of the patient’s assigned group just before the surgery. Patients remained unaware of their assignment until after the surgery. To mitigate potential bias in evaluating clinical and radiographic outcomes, we took measures to ensure that the surgeons did not participate in the assessment of these outcomes. Although it was unfeasible for the assessors to remain blinded to the type of intervention visible in radiological images, they were entirely detached from the treatment process. This intentional segregation of roles significantly minimizes the probability of bias in the evaluation of patient outcomes. The primary statistical method to address the primary outcomes is per-protocol analysis.
Surgical Procedure
Patients underwent either PLF or PLIF. All surgeries were performed by two experienced spine surgeons, and each surgeon performed both procedures following standardized protocols. In both groups, the same pedicle screw-rod system was utilized, and bone graft was harvested from the iliac bone. In-situ fusion was not performed, and efforts were made to achieve reduction. Reduction was facilitated by the utilization of reduction screws and, in some cases, by performing partial resection of the caudal facets. In the PLF group, meticulous decortication of the transverse process and the lateral aspect of the facet joints was carried out before inserting pedicle screws. Morselized cancellous bone graft along with a bone block placed above it were positioned on the intertransverse membrane, bridging both transverse processes. In the PLIF group, the procedure involved disc evacuation and thorough endplate preparation. Cancellous bone graft was densely packed into the disc space before inserting a kidney-shaped PEEK (polyetheretherketone) cage from one side. Patients in both groups followed the same postoperative treatment and rehabilitation protocols. No postoperative external support was used in either group. Patients were followed up for at least 24 months.
Outcome Measures
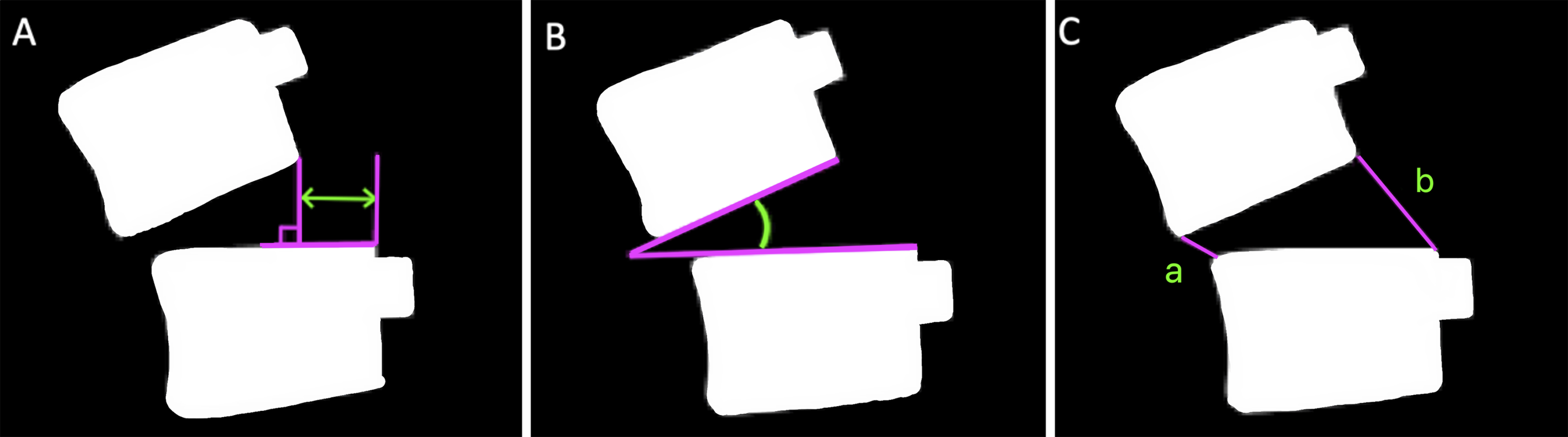
The primary outcome was the mean change in spinopelvic and deformity parameters (postoperative values- preoperative values). Secondary outcomes were: (1) the correlation between changes in spinopelvic and deformity parameters, and (2) the correlation between changes in sagittal radiographic parameters and clinical outcomes. Clinical outcomes were assessed using VAS and ODI questionnaires completed by the patients preoperatively and at the latest follow-up visit. Radiographic parameters were obtained from standing anteroposterior and lateral whole-spine radiographs performed preoperatively, immediately postoperatively and at the latest follow-up. For the lateral radiographs of the whole spine, the patients were instructed to stand upright in a relaxed position with the fingertips resting on the clavicle and the knees fully extended. The following spinopelvic parameters were measured: pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), sagittal vertical axis (SVA) and T1 pelvic angle (TPA) (Figure 1). The deformity parameters included: slip angle (SA), slip degree (SD) and disc height (DH) (Figure 2). All radiographic measurements were made using Surgimap Spine, a dedicated and validated software (Nemaris, Inc., New York, NY, USA).
19
After undergoing two training sessions on how to perform the measurements, two trained investigators independently conducted the measurements and the average of the two measurements was adopted. Analyzing the average values helped reduce potential errors in the measurements. The fusion status was assessed at the latest follow-up. Solid fusion was confirmed by identifying a continuous fusion mass on CT scans and/or observing a mobility of less than 4° on dynamic lateral radiographs.
20
Spinopelvic parameters. (A) Local parameters: PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; LL, lumbar lordosis. (B) Global parameters: SVA, sagittal vertical axis; TPA, T1 pelvic angle. Deformity parameters in isthmic spondylolisthesis. (A) Slip degree, (B) Slip angle, (C) Disc height (a + b/2).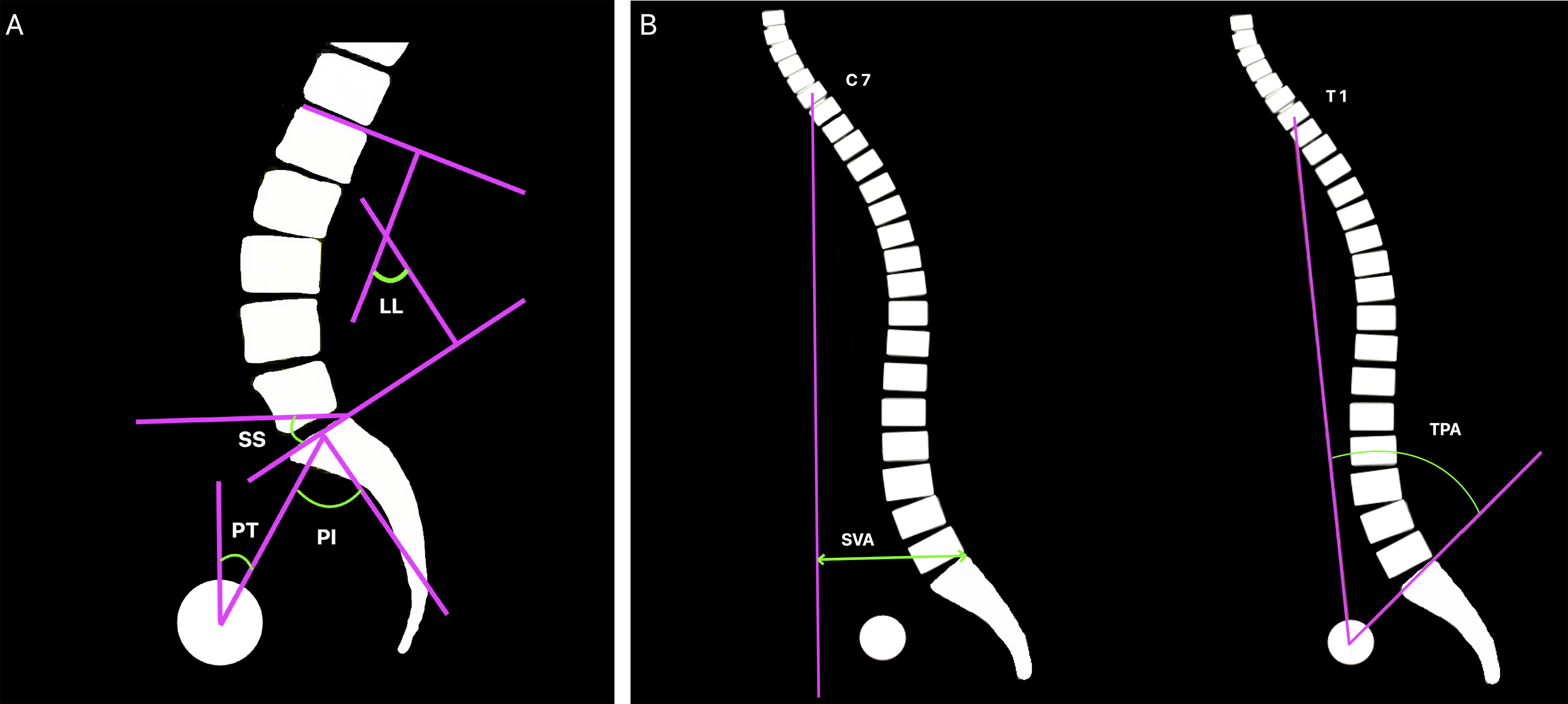
Statistical Analysis
Data were analyzed using GraphPad Prism for macOS version 9.5.0 (GraphPad Software, San Diego, CA, USA). Continuous data were expressed as mean ± SD while nominal data were expressed as frequency (percentage). Chi2-test was used to compare the nominal data of different groups in the study while unpaired t test was used to compare the means of the two groups. Paired t test was used to compare preoperative and follow-up assessments of the same group. The correlation of changes in ODI and VAS with changes in different parameters was determined by Pearson correlation. The level of confidence was kept at 95%; hence a P value <.05 indicated a significant association.
Results
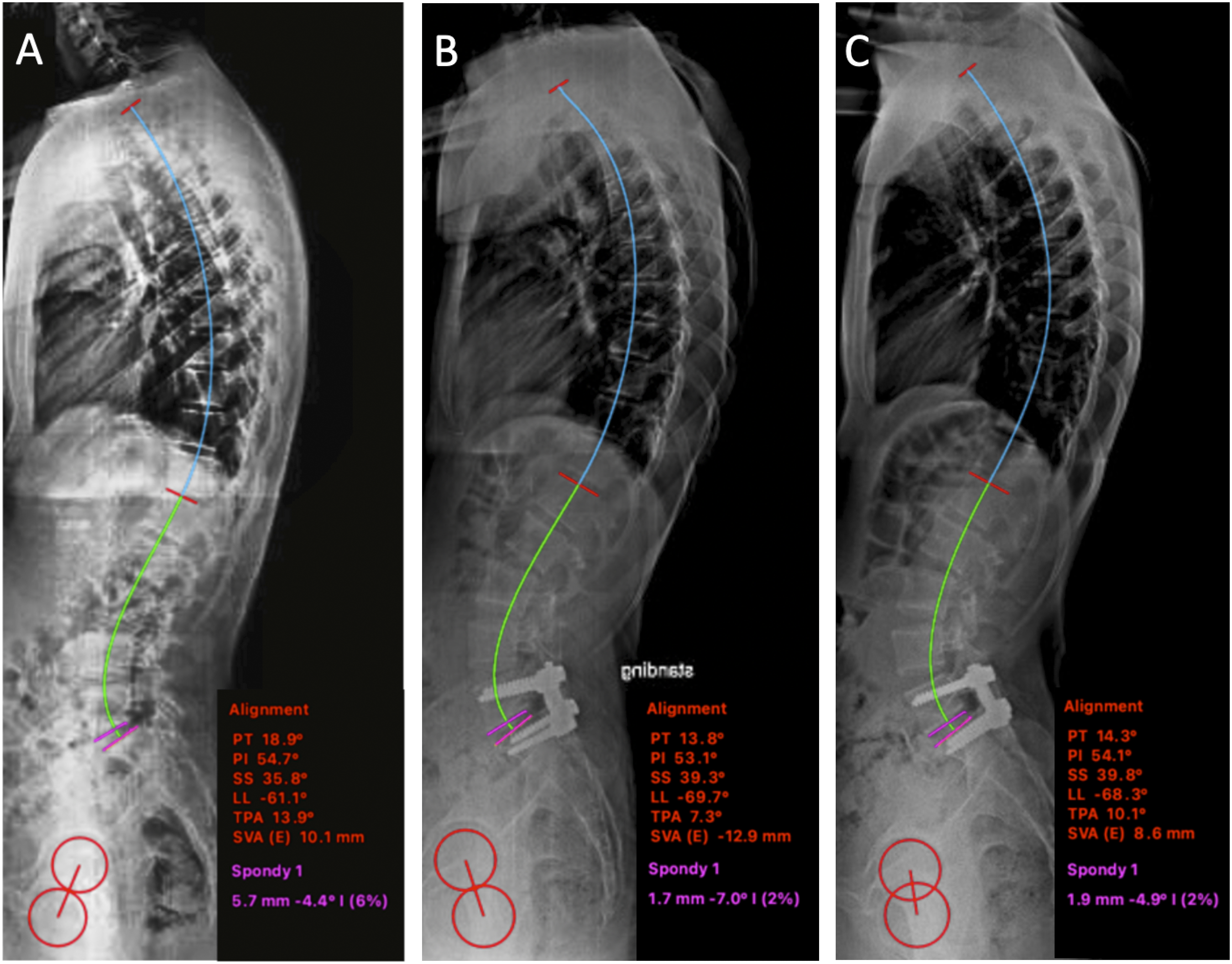
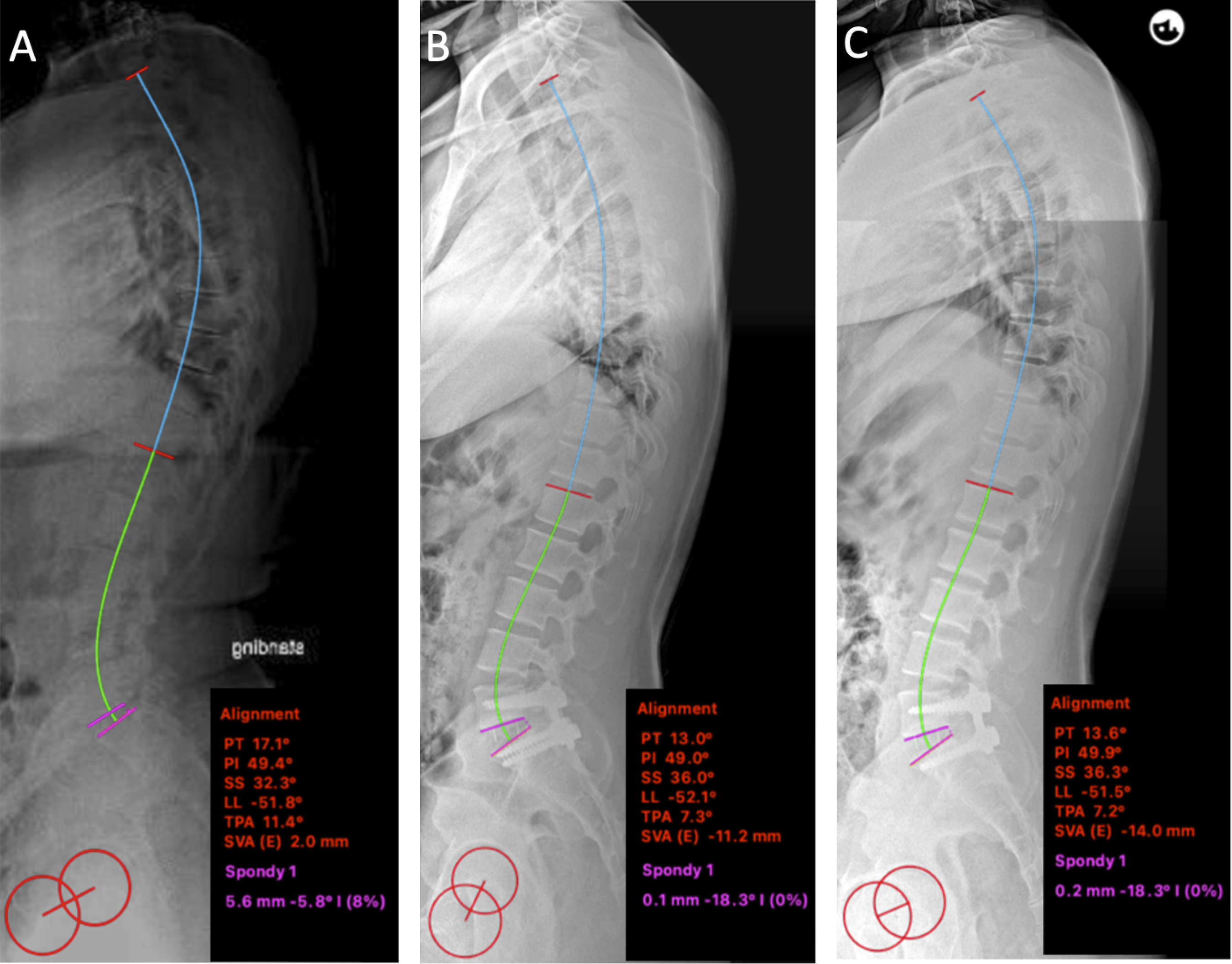
During the study, four participants were lost to follow-up. Among them, one participant unfortunately passed away due to complications from COVID-19 unrelated to the surgical procedure. The remaining three participants could not be reached for follow-up, rendering their data unavailable for analysis. A total of 42 patients were included in the final analysis, with 21 patients in each group (Figure 3). Representive cases are shown in Figures 4 and 5. Flow diagram of the study according to the CONsolidated Standards of Reporting Trials (CONSORT). A 35-year-old man with isthmic spondylolisthesis L5-S1. (A) Preoperative lateral radiograph. (B) Immediate postoperative lateral radiograph after PLF L5-S1 (C) Lateral radiograph at the latest follow-up. A 27-year-old man with isthmic spondylolisthesis L5-S1 (A) Preoperative lateral radiograph. (B) Immediate postoperative lateral radiograph after PLIF L5-S1 (C) Lateral radiograph at the latest follow-up.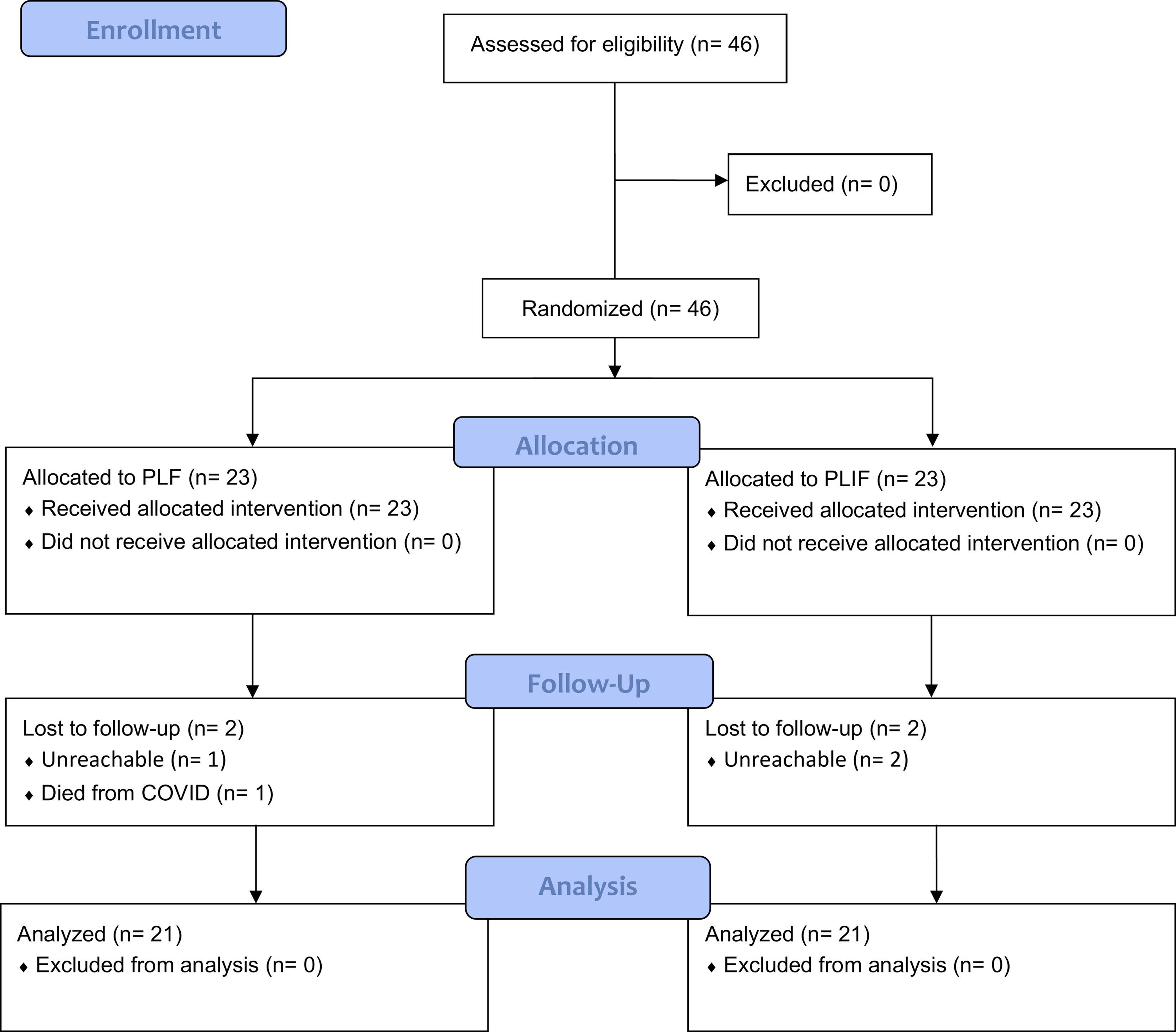
Demographic and Operative Data of Both Groups.
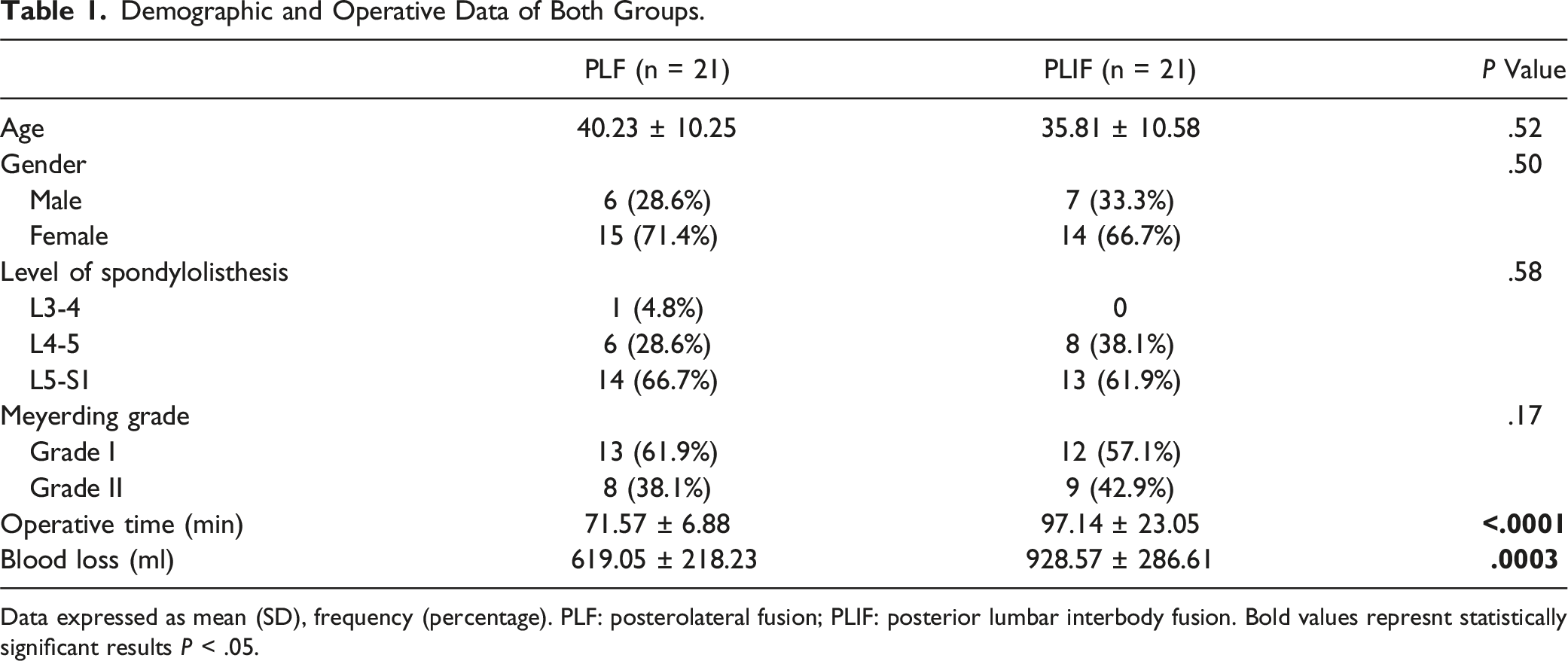
Data expressed as mean (SD), frequency (percentage). PLF: posterolateral fusion; PLIF: posterior lumbar interbody fusion. Bold values represnt statistically significant results P < .05.
Changes in Spinopelvic Parameters.
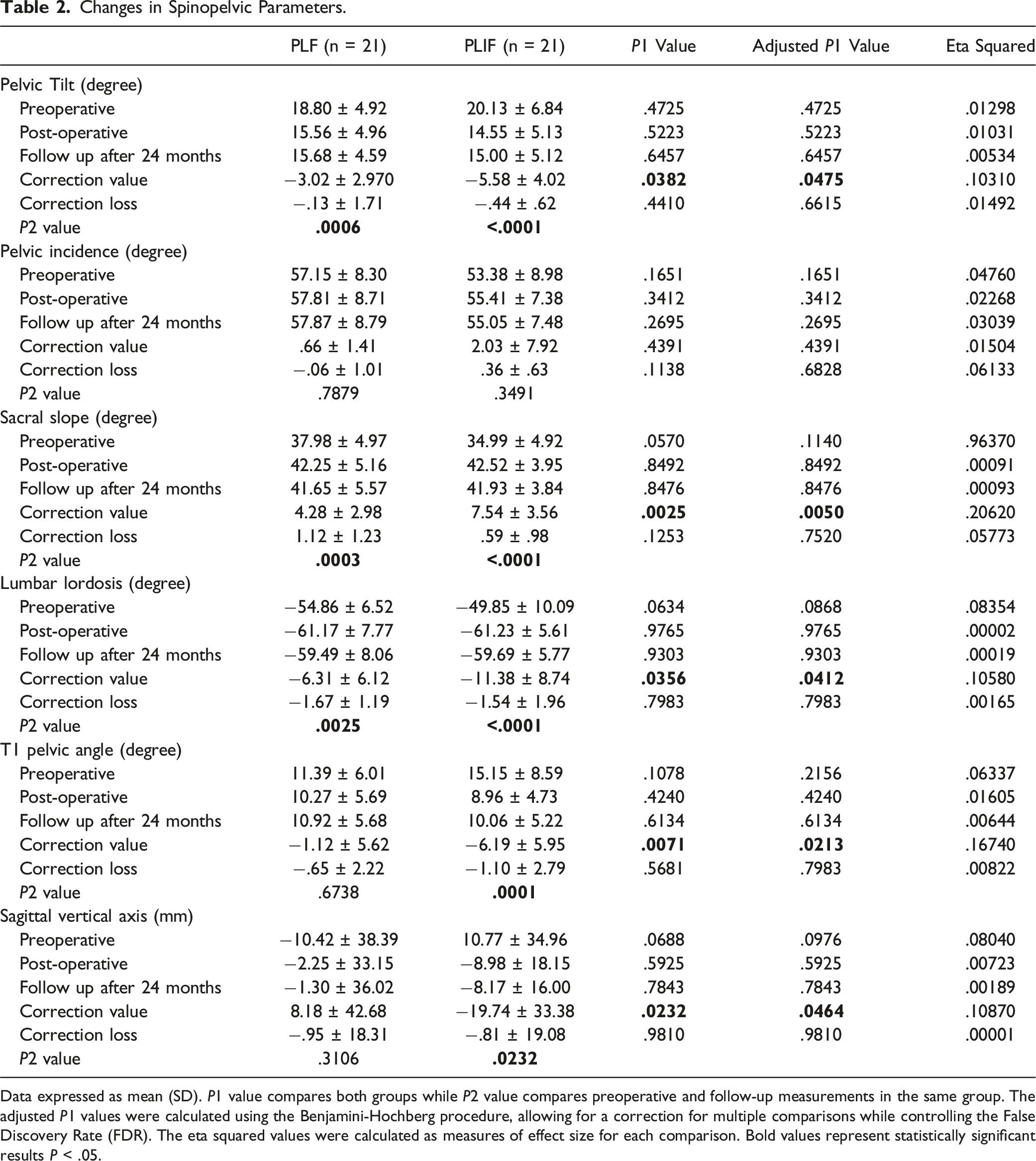
Data expressed as mean (SD). P1 value compares both groups while P2 value compares preoperative and follow-up measurements in the same group. The adjusted P1 values were calculated using the Benjamini-Hochberg procedure, allowing for a correction for multiple comparisons while controlling the False Discovery Rate (FDR). The eta squared values were calculated as measures of effect size for each comparison. Bold values represent statistically significant results P < .05.
Changes in Deformity Parameters.
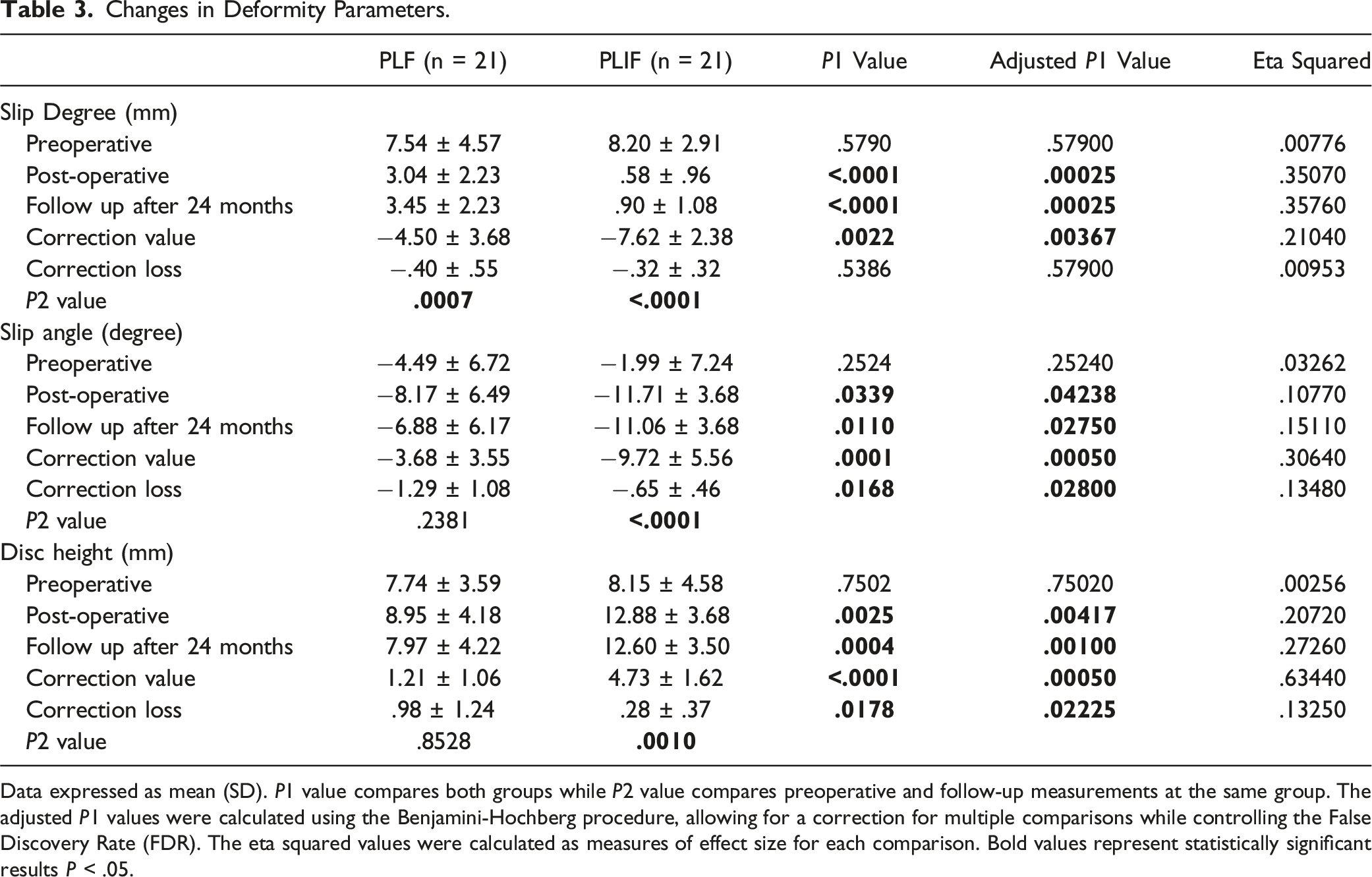
Data expressed as mean (SD). P1 value compares both groups while P2 value compares preoperative and follow-up measurements at the same group. The adjusted P1 values were calculated using the Benjamini-Hochberg procedure, allowing for a correction for multiple comparisons while controlling the False Discovery Rate (FDR). The eta squared values were calculated as measures of effect size for each comparison. Bold values represent statistically significant results P < .05.
Clinical Outcomes of Both Groups.
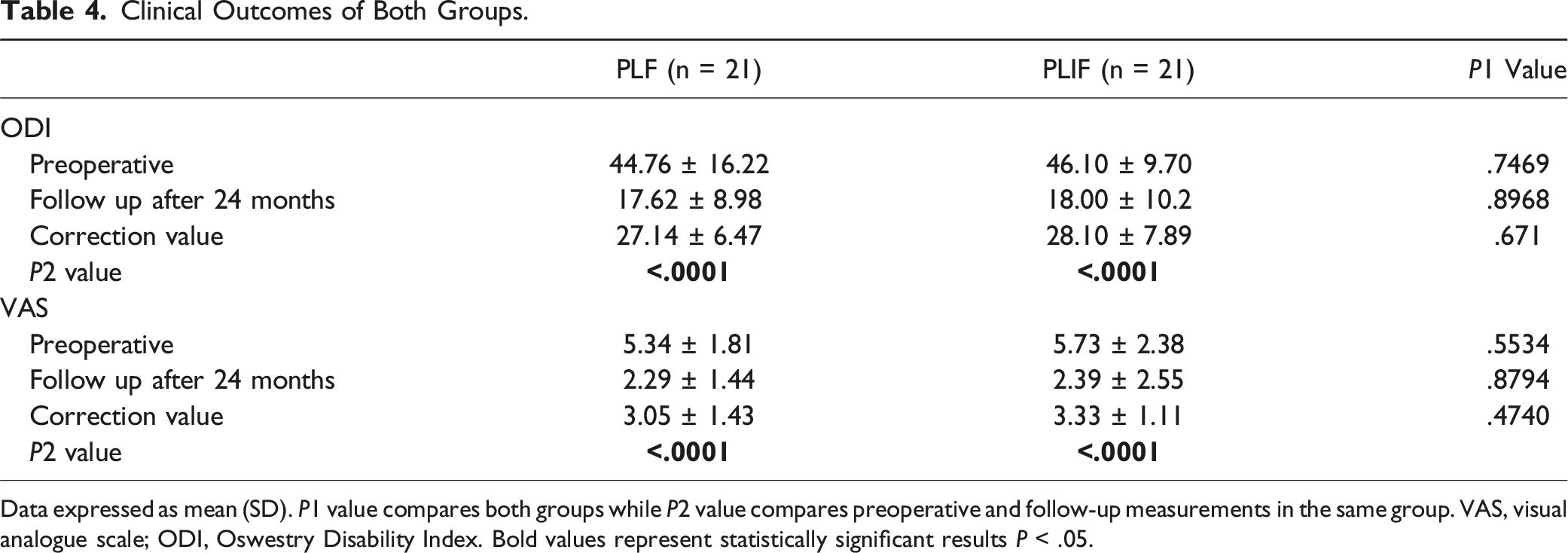
Data expressed as mean (SD). P1 value compares both groups while P2 value compares preoperative and follow-up measurements in the same group. VAS, visual analogue scale; ODI, Oswestry Disability Index. Bold values represent statistically significant results P < .05.
Correlation Between Changes in Spinopelvic Parameters and Deformity Parameters.
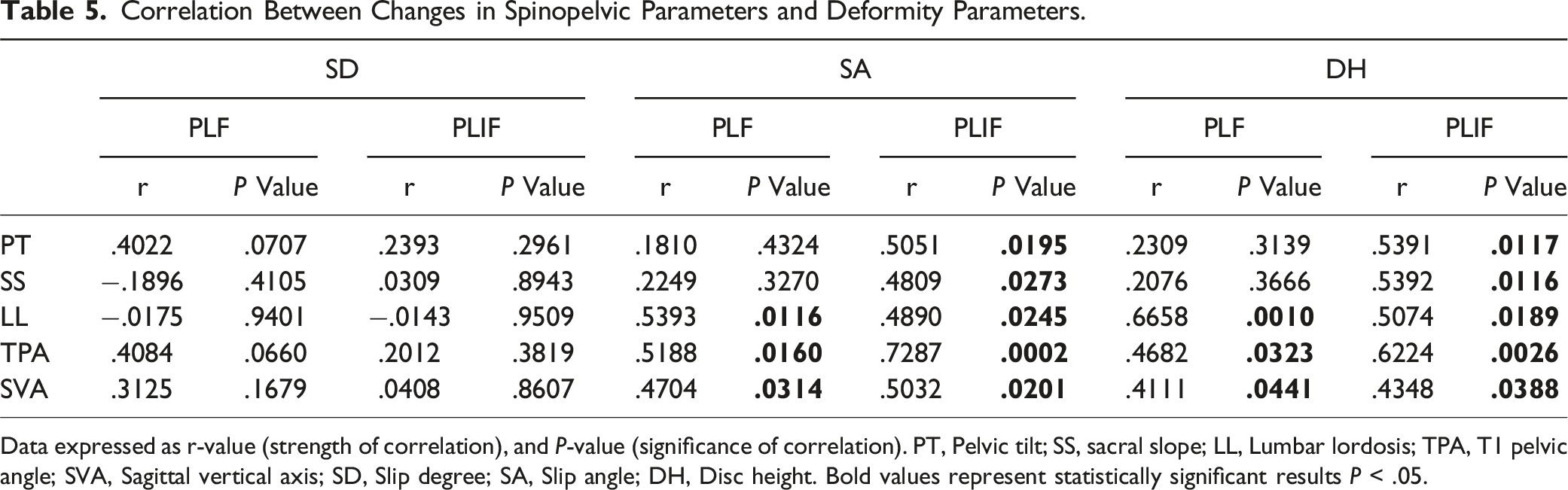
Data expressed as r-value (strength of correlation), and P-value (significance of correlation). PT, Pelvic tilt; SS, sacral slope; LL, Lumbar lordosis; TPA, T1 pelvic angle; SVA, Sagittal vertical axis; SD, Slip degree; SA, Slip angle; DH, Disc height. Bold values represent statistically significant results P < .05.
Correlation Between Changes in Clinical Outcomes and Changes in Radiographic Parameters.
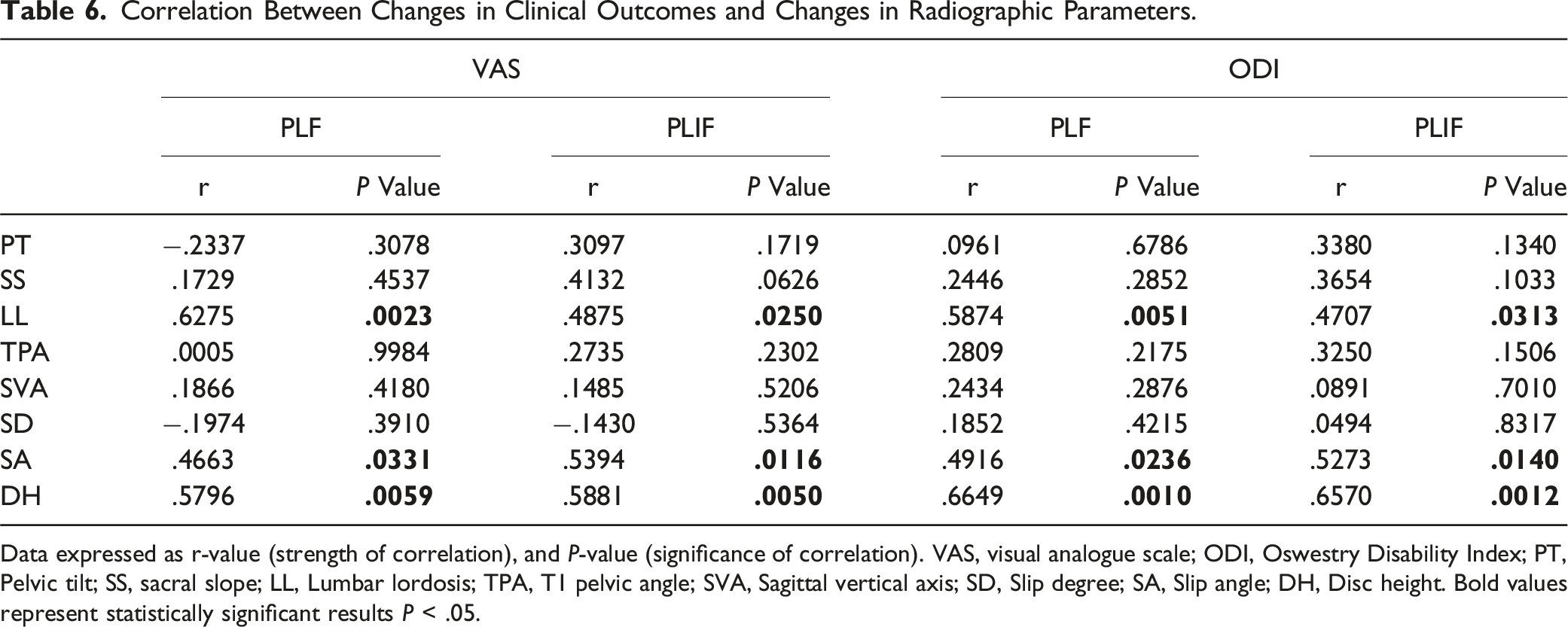
Data expressed as r-value (strength of correlation), and P-value (significance of correlation). VAS, visual analogue scale; ODI, Oswestry Disability Index; PT, Pelvic tilt; SS, sacral slope; LL, Lumbar lordosis; TPA, T1 pelvic angle; SVA, Sagittal vertical axis; SD, Slip degree; SA, Slip angle; DH, Disc height. Bold values represent statistically significant results P < .05.
Fusion was confirmed in 19 out of 21 patients (85.71%) in the PLF group and in 20 out of 21 patients (95.24%) in the PLIF group; however, the difference in fusion rates between the two groups was not statistically significant (P = .5991).
Discussion
Isthmic spondylolisthesis encompasses deformities such as forward slippage, kyphotic SA, and DH loss. It is also associated with alterations in normal spinopelvic parameters. Several studies have emphasized the importance of correcting these deformity parameters and restoring normal spinopelvic alignment for favorable surgical outcomes.15-17,21,22 However, the impact of PLF and PLIF on spinopelvic parameters remains inadequately defined, particularly in determining which procedure could best correct these parameters. Furthermore, there is limited understanding of the correlation between changes in spinopelvic and deformity parameters, specifically when identifying which deformity parameters have the greatest influence on pelvic parameters. In this study, we compared the effect of PLIF and PLF on spinopelvic and deformity parameters. Additionally, we investigated the correlation between these parameters as well as their correlation with clinical outcomes.
Feng et al 13 conducted a prospective study comparing PLF and PLIF in low-grade isthmic spondylolisthesis patients. They noted significant improvements of all spinopelvic and deformity parameters in the PLIF group, while in the PLF group, significant improvements were observed only in PT, SS, and SD. Additionally, when comparing the postoperative measurements of both groups, LL, DH and SA were significantly better in the PLIF group.
In the present study, substantial improvements were noted in all spinopelvic and deformity parameters within the PLIF group postoperatively and at the latest follow-up. Meanwhile, within the PLF group, statistically significant improvements were observed only in PT, SS, LL, and SD. These findings align with those from Feng et al 13 study, indicating that both procedures have the capacity to restore the physiological status of local spinopelvic parameters (PT, SS and LL). The improvement of these parameters has been correlated with positive clinical outcomes,23,24 which could explain the similar short-term clinical outcomes observed in both groups. However, there is a distinction between the two procedures. PLIF can address all deformity parameters (SA, SD, and DH), while PLF is capable of correcting only SD. This discrepancy primarily arises from the superior capability of PLIF to correct kyphosis and restore disc height with the use of interbody cages. Previous studies suggest that restoration of adequate DH and correction of SA are crucial for preventing adjacent segment degeneration.25,26 Our study primarily investigated the short-term outcomes. Further, longer follow-ups are required to ascertain whether both fusion techniques exhibit differences concerning the development of adjacent segment degeneration.
When comparing the postoperative measurements of both groups, only the deformity parameters (SA, SD and DH) were significantly better in the PLIF group. However, when comparing the means of correction (postoperative values− preoperative values), both spinopelvic and deformity parameters showed a significantly higher correction in the PLIF group compared to the PLF group. Comparing the postoperative measurements may not capture the full picture of the intervention’s effectiveness, while the change score approach (postoperative values − preoperative values) provides a more comprehensive understanding of the impact of the treatment on the participants’ outcomes. Additionally, when comparing the means of correction loss (last follow-up values- postoperative values), SA and DH showed significantly less correction loss in the PLIF group. This difference is attributed to the use of interbody cages in the PLIF group, which support the anterior column and aid in preserving the attained correction. Therefore, PLIF is more powerful than PLF in correcting both spinopelvic and deformity parameters and in sustaining the correction of deformity parameters. However, this disparity does not appear to impact short-term clinical outcomes. It is essential to emphasize that further studies involving extended follow-up periods are necessary to ascertain whether this distinction will influence long-term clinical results.
Regarding the correlation between changes in spinopelvic parameters and deformity parameters, several noteworthy findings have emerged from previous research. Park et al 12 reported that changes in DH showed a significant positive correlation with changes in LL and SVA, and they highlighted the restoration of DH as the most crucial step in surgical treatment. Similarly, Feng et al 13 found a significant positive correlation between changes in SD and DH and changes in LL within the PLIF group. In contrast, Boachie-Adjei et al 21 suggested that the correction of SA, not SD, was more important for restoring sagittal balance and a better biomechanical environment for fusion. Additionally, Godde et al 27 reported that correction of SA and LL using a wedge-shaped cage should be performed to restore normal sagittal alignment.
In our study, changes in SA and DH showed a significant positive correlation with changes in spinopelvic parameters (LL, SVA and TPA) in both groups. These findings emphasize the importance of restoring DH and SA for better correction of spinopelvic parameters. On the other hand, complete reduction, as measured by SD, is not as important as restoration of DH and SA. These results are consistent with those from Boachie-Adjei et al 21 and Godde et al 27 studies.
Regarding the clinical outcome, in the present study, both the ODI and VAS improved significantly at the final follow-up, with no significant difference between the PLIF and PLF groups. These findings align with the conclusions drawn from the majority of previous studies.5,6,8-11,28 However, Farrokhi et al 7 described a significantly greater improvement in the ODI for patients treated with PLF than for those who underwent PLIF for IS. Conversely, Behzadnia et al 14 reported a significantly greater improvement in VAS in the PLIF group.
Additionally, our study further investigated the correlation between changes in sagittal radiographic parameters and clinical outcomes and revealed a significant positive correlation between changes in ODI and VAS with changes in SA, DH and LL in both groups. These findings suggest that SA, DH, and LL are the most crucial radiographic parameters influencing the clinical outcome following surgical treatment of isthmic spondylolisthesis.
Limitations
The COVID-19 pandemic significantly affected healthcare access, posing difficulties in participant enrollment and consistent follow-up. This disruption serves as the main cause behind the primary limitations of this study: the relatively small study population and the short follow-up duration. Hence, it is crucial to conduct prospective multicenter studies involving larger participant cohorts and extended follow-up periods to thoroughly examine the effect of radiographic parameters correction on long-term clinical outcomes. Another limitation of the study is that a per-protocol analysis was conducted, excluding patients who deviated from the protocol. This approach may introduce attrition bias and potentially exaggerate the treatment effect. However, this limitation was proactively addressed by initially calculating the sample size while considering potential dropouts. Moreover, similar dropout rates between study arms were observed, indicating that dropout was not disproportionately affecting one group over the other. Additionally, the reasons for missing data were thoroughly investigated and found to be unrelated to the treatment or outcome under study. Comparison of baseline characteristics between participants with missing data and those with complete data revealed no systematic differences, suggesting minimal risk of bias. Furthermore, the exclusion of missing participants did not significantly impact treatment effect estimates, and the missing data mechanism was deemed ignorable. Sensitivity analyses confirmed the robustness of the findings. Thus, despite the per-protocol analysis approach, several measures were taken to mitigate potential biases and ensure the integrity and validity of the conclusions. Despite these limitations, this study possesses distinctive strengths. This is the first randomized controlled trial to compare sagittal radiographic parameters following PLF and PLIF for patients with low-grade isthmic spondylolisthesis. Additionally, it establishes the correlation between changes in these parameters and clinical outcomes.
Conclusion
In patients with low-grade isthmic spondylolisthesis, PLIF demonstrates superior efficacy compared to PLF in correcting sagittal radiographic parameters. However, this disparity does not appear to impact short-term clinical outcomes. Changes in SA and DH exhibited a significant positive correlation with changes in spinopelvic parameters. Consequently, complete reduction as measured by SD is not as important as restoration of DH and SA for achieving superior correction of spinopelvic parameters. Furthermore, changes in DH, SA and LL correlated significantly with changes in ODI and VAS; thus, restoration of disc height, correction of the slip angle and reestablishment of normal lumbar lordosis are the most important steps in the surgical treatment of isthmic spondylolisthesis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.