
Abstract
Study Design:
Imaging parameter study.
Objective:
Though lumbar alignment is better evaluated using standing radiograph than supine magnetic resonance imaging (MRI), few studies have researched this. Our study aimed to observe the correlation and difference in alignment between standing radiograph and supine MRI, and assess whether the change of position affects the lumbopelvic parameters.
Methods:
We analyzed 105 patients, measuring lumbar lordosis (LL), sacral slope (SS), pelvic tilt (PT), and pelvic incidence (PI). Inter- and intraparameter analyses were performed to identify any difference between standing radiograph and supine MRI. Statistical differences between the lumbopelvic parameters were compared.
Results:
There was excellent interobserver agreement for each parameter (interclass correlation coefficient > 0.75), and significant differences were observed in each parameter between radiograph and MRI (P < .05). Strong correlations were noted between the equivalent parameters in radiograph and MRI, both SS and PI were strongly correlated with LL in radiograph and MRI image, both PT and SS were strongly correlated with PI in radiograph and MRI image (r = −1.0 to −0.5 or 0.5 to 1.0).
Conclusion:
Supine MRI obviously underestimated the measurements of lumbopelvic sagittal alignment parameters in standing radiograph. Therefore, standing lumbar radiographs should be obtained preoperatively in all surgical patients, not only supine MRI. In addition, we observed that PI was not a constant morphological parameter.
Introduction
The sagittal balance parameter of spine-pelvis has been a hot spot in spine surgery. With the increasing incidence of lumbar degenerative diseases, sagittal alignment analysis of lumbar vertebrae shows that most lumbar degenerative diseases are closely related to sagittal imbalance. 1 Restoration and reconstruction of physiological curvature is the basis for maintaining the normal lumbar biomechanical function. Studying the characteristics of sagittal sequence in physiological state and lumbar degeneration trend can assist doctors in reconstructing the lumbar sagittal alignment through surgery, which may be helpful to reduce the degeneration of adjacent segments. 2 However, the process of lumbar sagittal degeneration is affected by many factors. The mechanism of spinal compensation is complex, and the current cognition is still limited. Thus, further research on the focus is needed.
Nowadays, though most spine surgeons usually acquire weight-bearing radiographs in surgical planning and clinical practice, there are some surgeons who use only preoperative magnetic resonance imaging (MRI) for laminectomy, posterior lumbar interbody fusion, minimally invasive spine surgery, and so on. This may not be deliberate and comprehensive enough. However, as long as there is no evidence that weight-bearing radiograph is essential for evaluation of standing lumbar alignment, we have reason to consider that lumber MRI is sufficient in preoperative examination. As we all know, lumbar radiographs are taken in standing position, while supine position is used for MRI, and whether there is correlation or differences in the parameters obtained from the 2 methods still needs to be revealed.
Some studies have assessed the sagittal alignment of lumbar spine and reported the correlation in lumbar sagittal alignment parameters between different radiographic modalities or positions.3-5 In addition, several scholars performed evaluations using kinematic or positional MRI.6,7 Nevertheless, too much time is spent in conducting multiple MRI examinations, which makes it difficult for physicians to obtain immediate results. Thus, when evaluating the condition according to imaging studies, spine surgeons still mainly use standing radiograph and supine MRI. There have been studies expounding the differences between images with different weight-bearing conditions in cervical sagittal alignment parameters; however, few studies reported that in lumbopelvic parameters. Our aim was to explore the correlation and difference between lumbar radiograph and MRI, and evaluate whether the waist position affects lumbopelvic parameters.
Materials and Methods
Patient Case and Parameters
We obtained institutional review board approval from our ethics committee to perform this study, and informed signed consents were provided by all participating subjects. Patients treated for lumbar symptoms with a full set of weight-bearing lumbar radiographs and MRI images in database records of our hospital from January 1, 2019, to December 31, 2019, were included and analyzed retrospectively. Cases with presence of instrumentation in lumbosacral area were excluded, for it might have an objective impact on measurements. Nondegenerative spine pathologies, such as Scheuermann or camptocormia causing a stiff global kyphosis, were also excluded. All participants were required to have available clinical data, including demographic characteristics, chief complaints, spinal cord and neurological function, and treatment history. According to the criteria, a total of 105 consecutive patients were involved.
Standing lumbar radiographs were conducted with upper arms in a lifting position so as to avoid obscuration or overlapping shadows, while lumbar MRI were performed as usual in a neutral supine position. The interval between performing the 2 imaging studies should not exceed 2 months in order to prevent deviation caused by disease progression.
A resident of our department who did not participate in the later statistics and analysis collected these cases from the database. Two independent expert spine surgeons were selected to assess imaging studies and measure parameters separately as they were unaware of the identity of the patients and the treatment they received. The following lumbopelvic sagittal alignment parameters were assessed on both radiographs and MRI images: (1) lumbar lordosis (LL), measured as the angle subtended between tangents of T12 lower endplate and S1 sacral endplate; (2) sacral slope (SS), measured as the angle subtended between tangent of S1 endplate and horizontal line; (3) pelvic tilt (PT), defined as the angle between the vertical and a line from the center of the femoral heads to the midpoint of the sacral endplate; and (4) pelvic incidence (PI), defined as the angle subtended between a line perpendicular to the sacral plate at its midpoint and a line connecting this point to the axis of the femoral heads. The pelvic incidence was derived from the following formula: pelvic incidence = pelvic tilt + sacral slope (Figure 1).8,9

Lumbopelvic sagittal alignment parameters.
Statistical Analysis
All lumbopelvic sagittal alignment parameters were measured using Picture Archiving and Communication System (PACS), and Statistical Packages of Social Sciences (SPSS) software (version 22.0) was used to analyze the collected data. The interobserver reliability of the lumbopelvic parameters was tested by using interclass correlation coefficient (ICC; 2-way mixed effect model, in which people effects are random, and measures effects are fixed), 10 and the values were expressed with a 95% confidence interval (CI). The range of ICC was (0,1); larger values represented better agreement. Levels of agreement for ICC were divided into 3 grades, with ICC values 0.00 to 0.40 considered poor agreement, 0.40 to 0.74 fair to good agreement, and 0.75 to 1.00 excellent agreement (Table 1).11,12
Level of Agreement for Interclass Correlation Coefficient (ICC) Values and Relationship for r Values.
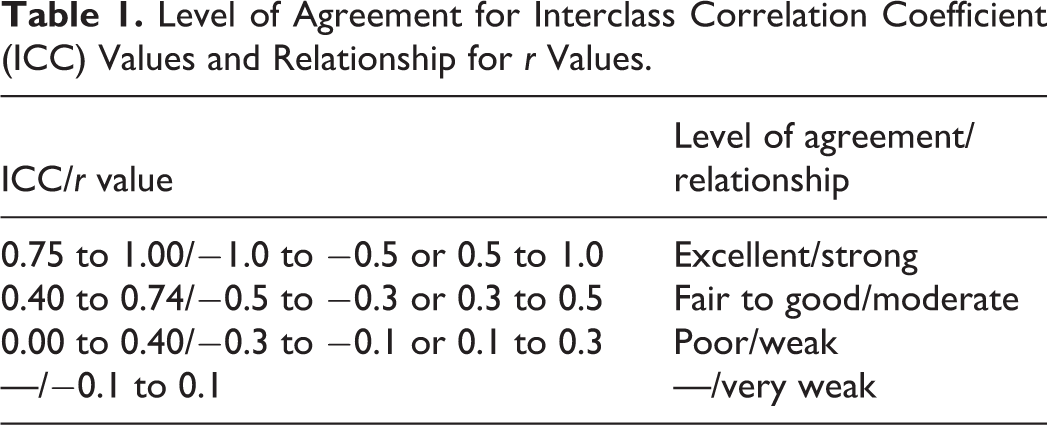
To test the difference in previously mentioned parameters between radiographs and MRI images, pairwise t tests were performed in each data set of the 2 spine surgeons. The Pearson correlation coefficient was used to analyze the correlation in lumbopelvic parameters between the 2 imaging studies, and the values (r) were divided into 4 grades, with −1.0 to −0.5 or 0.5 to 1.0 considered strong, −0.5 to −0.3 or 0.3 to 0.5 considered moderate, −0.3 to −0.1 or 0.1 to 0.3 considered weak, and −0.1 to 0.1 considered none or very weak (Table 1). Meanwhile, P values <.05 were considered statistically significant.
Results
There were 105 consecutive cases involved in our study, including 47 males and 58 females with a mean age of 63.7 years (range from 38 to 81 years). A total of 1680 measurements for the 4 lumbopelvic parameters were obtained from the 2 spine surgeons.
Interobserver Reliability
Based on reliability analysis of the results, the interobserver agreement of all the lumbopelvic parameters on both radiographs and MRI images was excellent; ICC values of each lumbopelvic parameter on both radiographs and MRI images were calculated as follows: 0.895, 0.866, 0.854, 0.963, 0.847, 0.906, 0.879, and 0.927; and the pairwise mean differences between 2 spine surgeons for all angular parameters on radiographs and MRI images were lower than 2°, which indicated excellent interobserver agreement for all the parameters. The results were considered statistically significant (P < .001; Table 2).
Interobserver Reliability and Pairwise Difference of Each Parameter Between Spine Surgeons.
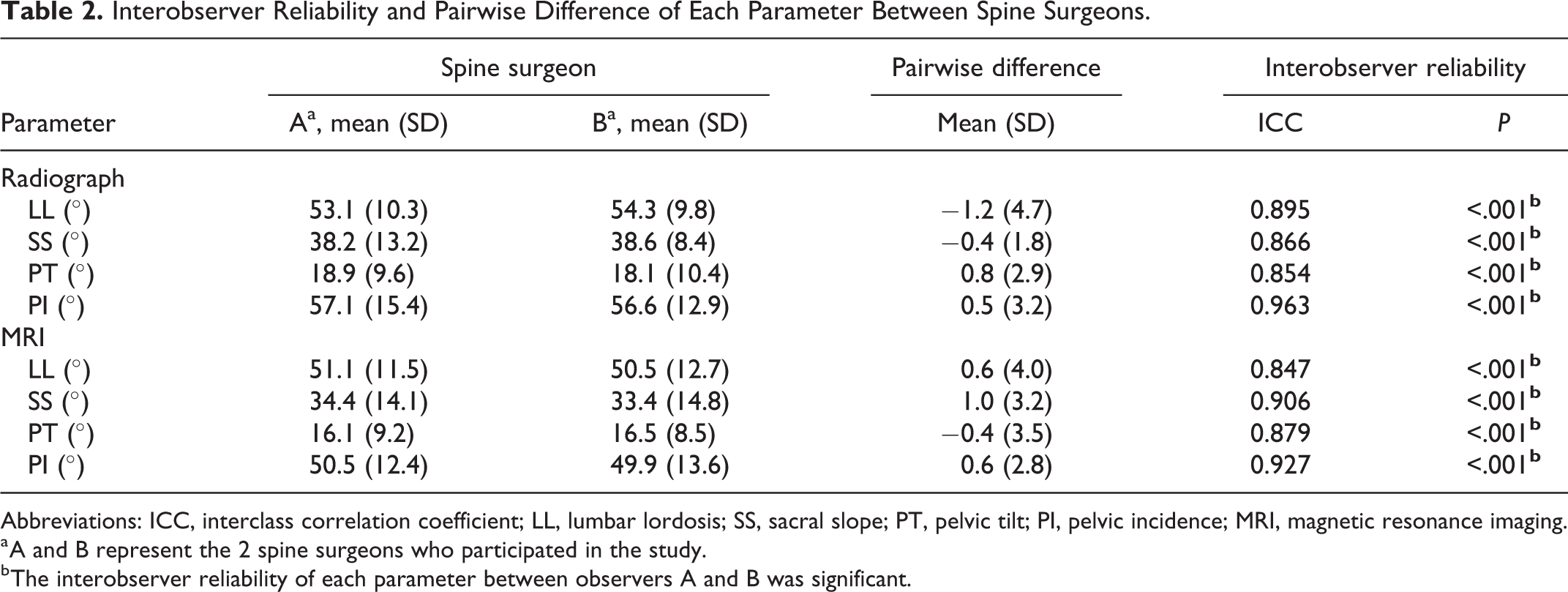
Abbreviations: ICC, interclass correlation coefficient; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; MRI, magnetic resonance imaging.
a A and B represent the 2 spine surgeons who participated in the study.
b The interobserver reliability of each parameter between observers A and B was significant.
Lumbopelvic Parameters
The mean lumbopelvic parameters were 53.7 ± 8.1° (LL), 38.4 ± 12.8° (SS), 18.5 ± 10.4° (PT), and 56.9 ± 15.6° (PI) in radiographs, while those in MRI images were 50.8 ± 12.4° (LL), 33.9 ± 14.6° (SS), 16.3 ± 8.8° (PT), and 50.2 ± 16.7° (PI), respectively. The pairwise t tests indicated significant differences in LL (P < .05), SS (P < .001), PT (P < .05), and PI (P < .001) between radiographs and MRI images (Table 3).
Pairwise Differences of Lumbopelvic Parameters Between Radiograph and MRI.
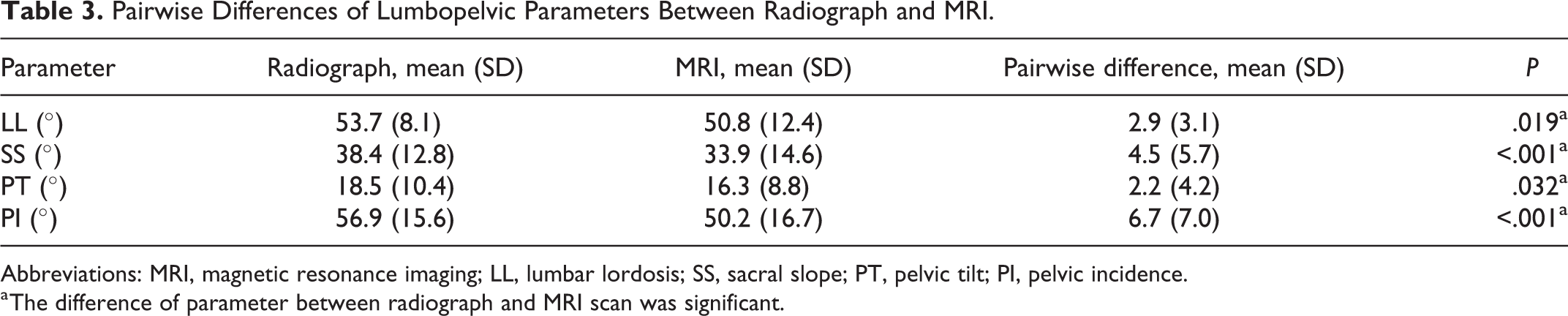
Abbreviations: MRI, magnetic resonance imaging; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence.
a The difference of parameter between radiograph and MRI scan was significant.
Correlations of Parameters
On performing Pearson analysis, we found that each lumbopelvic parameter in radiographs were basically correlated with the same parameter in MRI images, with all their r values higher than 0.5. In addition, there were other strong correlations of parameters as follows: both SS and PI were strongly correlated with LL in radiograph and MRI image; PT was strongly correlated with SS in radiograph and MRI image (Table 4).
Correlations of Parameters in Radiograph and MRI.
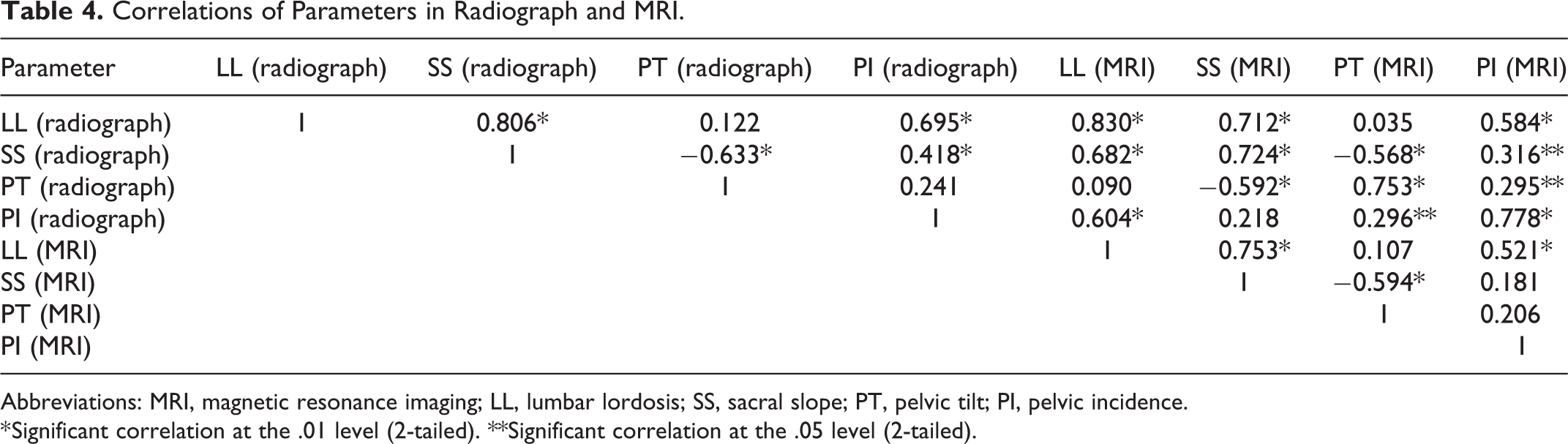
Abbreviations: MRI, magnetic resonance imaging; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence.
* Significant correlation at the .01 level (2-tailed). **Significant correlation at the .05 level (2-tailed).
Discussion
To evaluate lumbar alignment, it is essential to take into account the position when performing imaging examinations. Physicians should notice the weight of upper part of the body, which adds compressive force to vertebrae in standing lumbar radiograph, while supine MRI is not affected by body weight. 13
According to our results, with regard to standing radiograph and supine MRI, we discovered a controversial finding that PI was not a constant morphological parameter (no significant difference between radiograph and MRI). Previous researches differed in whether PI remains constant in different positions. Mac-Thiong et al 9 pointed out that each individual has a specific PI, which remains constant, and proposed the geometric relationship, PI = PT + SS. Other scholars suggested that PT, SS, and LL are affected by different positions and postures, but the constant value of PI should not be affected by any factors.14,15 But, in contrast, Park et al 4 reported a decrease of PI from standing to supine, which could be explained by more retroverted pelvic bone (higher PT) and more vertically oriented sacral endplate (higher SS). To find the reason for our result, we analyzed the detailed case history of all participants and found that 32% of patients had pain in sacroiliac joint, which indicated sacroiliac joint dysfunction, and thus weight-loading in standing might increase the PI by affecting the unstable sacroiliac joint.
In our study, both SS and PI were strongly correlated with LL in radiograph and MRI image. Since the definition of PI in 1992, 8 many studies have found a significant correlation between PI and lumbar sagittal morphology. In recent years, scholars have also realized that the spatial position and anatomy of the pelvis can significantly affect the sagittal alignment of the spine under normal or pathological conditions, and determine the LL to a large extent, that is, the pelvis changes LL through the change of SS, and then affects the lumbopelvic sagittal balance. 16 SS determines the curvature of the lumbar spine; a sacral plate closer to horizontal (ie, smaller SS) always represents a smaller LL. However, SS is position-dependent and varies with pelvic retroversion (increase in PT) in malaligned patients. Unlike SS, PI is a morphological parameter that is unique to each individual and has a strong positive correlation with LL. 17
Although there is a positive correlation between PI and LL, SS and LL, and those parameters are widely used in clinical practice, based on the feedback from the 2 spine surgeons, we believe that it is difficult to accurately determine the position of the midpoint of the sacral endplate when evaluating the patients with unclear S1 endplate, domed sacrum, and severe degeneration. At the same time, the correlation regression coefficients and constants summarized in domestic and foreign literature are quite different. Therefore, the linear relationship and regression formula between those lumbopelvic parameters are still controversial.
In addition, as previously reported for other imaging modalities, standing and supine positions made significant differences in measurement of LL, SS, and PT. Bernstein et al 18 showed that compared with standing position, the LL value measured on supine position MRI was 6.5° smaller on average, so supine MRI underestimated the LL of patients, and suggested that LL measured on the sagittal MRI and lateral radiograph were significantly correlated. A study by Park et al 4 indicated that LL, SS, and PT values were significantly higher on standing position compared with those on supine position. Our results are similar to these findings. Each participant involved in our study had 2 lumbar segments (L4/5 and L5/S1) with the highest mobility, which made the measurements susceptible to weight-bearing and posture changes.19,20 Compared with supine MRI, this may be the reason for the significant increase of LL in standing radiograph. The LL of supine MRI is smaller than that of standing radiographs even under axial load. 21 In supine position, the lower limbs and body are more likely to be in the same line, besides the back of the body touches the table, which exerts a reaction force on the lumbosacral part. Thus, the decrease of LL and the closer horizontal position of the sacral endplate produce smaller SS in supine position, while PT is significantly smaller in supine position because of the decrease of pelvic retroversion.
Our findings are of clinical significance that it is insufficient preparing only supine MRI of patients for surgeries, and plain radiograph is essential. Different positions have significant influence in lumbopelvic sagittal alignment parameters. Considering supine MRI can more clearly demonstrate the disc, nerve root, spinal cord, and soft tissue around the lumbar spine and pelvis, standing MRI has been developed, though it is not widely used.
The current study has several limitations. First, we did not perform full-length radiographs, which could help in obtaining the whole view of sagittal alignment and make the analysis more comprehensive. Second, the relatively small sample size. Our finding that PI is not a constant morphological parameter is contrary to the widely accepted cognition, and we have explained that the unstable sacroiliac joint may be the influencing factor. Nevertheless, further expanding our sample population will eliminate coincidence as much as possible, or even obtain a definite subversive result. Third, we did not consider dynamic adjustments when measuring the parameters, and all results were acquired under static conditions. There might be an adaptive mechanism, through which gravity may change the correlation between lumbopelvic parameters in standing positions. Finally, varieties of thoracic, iliac, and sacral dimensions that determine the contact area with bed, may influence the position of the lumbar spine in the supine MRI and thus affect the measurements. Therefore, high-quality, large sample, and multicenter studies should be performed in our future clinical work to provide spine surgeons with the best evidence-based information.
Conclusion
There were significant differences between standing radiograph and supine MRI in the measurement of LL, SS, PT, and PI. Supine MRI obviously underestimated the value of lumbopelvic sagittal alignment parameters. Therefore, standing lumbar radiographs should be obtained preoperatively in all surgical patients, not only supine MRI. In addition, we observed that PI was not a constant morphological parameter. However, larger sample and multicenter studies should be performed to improve the accuracy and reliability of the finding, and further clinical correlation should be evaluated in future works.
Footnotes
Authors’ Note
All supporting data can be provided on request to the authors.
Author Contributions
CQX and MCY are co–first authors of this manuscript. CQX designed the study and collected the data. MCY did the data analysis. CQX wrote the manuscript. WM revised the manuscript. All authors read and approved the final manuscript.
Ethical Approval
The case was reviewed by the Longhua Hospital Ethics Committee, and ethical approval was waived as written consent was obtained from the patient.
Informed Consent
Written patient consent was obtained for publication of all aspects of the case including personal and clinical details and images, which may compromise anonymity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.