
Abstract
Study design
Systematic review.
Objective
To evaluate the lowest possible age to resect an HV in very young patients with a congenital deformity.
Methods
We sought to retrieve all studies reporting age at HV excision in patients with congenital scoliosis. Studies written in English were included. No publication date restrictions were imposed. A search of the PubMed and LiLacs databases was conducted. Additionally, a hand search was performed to supplement the database search.
Results
We found 140 articles. Twenty two studies were included into the final assessment. There was considerable heterogeneity in the included studies, both regarding age and the surgical techniques used. There was also a broad spectrum of recommendations regarding suggested age for treatment. The youngest patient undergoing resection and fusion was 3 months of life at the time of surgery.
Conclusion
How young a patient could and should be submitted to HV resection surgery is still a matter of debate in the literature. Prophylactic surgery might be a proper treatment for young children with congenital scoliosis before malformation becomes a deformity, adding no additional neurological, vascular, or anesthesia-related complications. The defect can be treated early while the deformity is treated late.
Keywords
Introduction
Hemivertebra (HV) is a formation defect produced during embryonic development. Congenital scoliosis, with an incidence between 0.5 and 1 per 1000 births, has the potential to eventually become progressive. Scoliosis due to HV may be considered a severe, generally progressive, condition, associated with coronal and sagittal spine imbalance. If left untreated, HV can develop into an unacceptable deformity. 1 The HV-related deformity has a variable prognosis, mostly associated with growth itself, because of which it may rapidly progress from a mono-segmental malformation into a broad spinal deformity.
In children, the potential development of the coronal and sagittal congenital spinal deformity is related to different variables: type and location of the defect, number of malformed vertebrae, number of healthy incorporated vertebrae, and the potential growth of the patient. 1 It has been demonstrated that patients with segmented, multiple, unilateral non-sequential or adjacent bilateral, or bilateral distant HV associated with a contralateral bone bar have the worst prognosis, with a higher risk to develop more severe curves, trunk decompensation, and neurological involvement, especially when the kyphosis component is predominant. 1
The age of the patient is an important variable as the HV-related deformity often deteriorates rapidly during the adolescent growth spurt. It is only at skeletal maturity that vertebral growth plates fuse and, theoretically, the potential of increasing deformity ceases. A fully segmented and isolated HV between T1 and T4 may increase 1°per year, between T5 and L1 1.4°per year, between L2 and L4 1.7°per year, and when located in the lumbosacral region 1.5°per year. 2 Fully segmented/non-incarcerated HVs have normal growth plates and tend to require early/prophylactic surgical treatment to prevent significant deformity. 3
In young children early surgery may prevent the development of local deformities and secondary structural or non-structural curves. 4 It has been suggested that preventive treatment might be recommended before the spine begins to decompensate, before the primary curve incorporates healthy vertebrae, and before secondary curves become structural. 5 There is scarce information on surgical outcomes related to timing of surgery in children under age 10 years with congenital scoliosis and a long-term follow-up.
The aim of this study was to evaluate the lowest possible age to resect an HV in very young patients with a congenital deformity reported in the literature.
Methods
We sought to retrieve all studies reporting age at HV excision in patients with congenital scoliosis, with or without the use of different instrumentation techniques. Studies written in English were included. No publication date restrictions were imposed. Studies involving participants with non-congenital scoliosis were excluded. A search of the PubMed and LiLacs databases was conducted. A combination of the search terms, including medical subject headings (MeSH), pertaining to congenital scoliosis “hemivertebrae resection,” “hemivertebrae excision,” “congenital scoliosis,” and “children” was used. Additionally, a hand search was performed to supplement the database search. Information was extracted regarding study design, recommended age at surgery, treatment method, postoperative results, patient characteristics, and follow-up. All data were then collated and summarized.
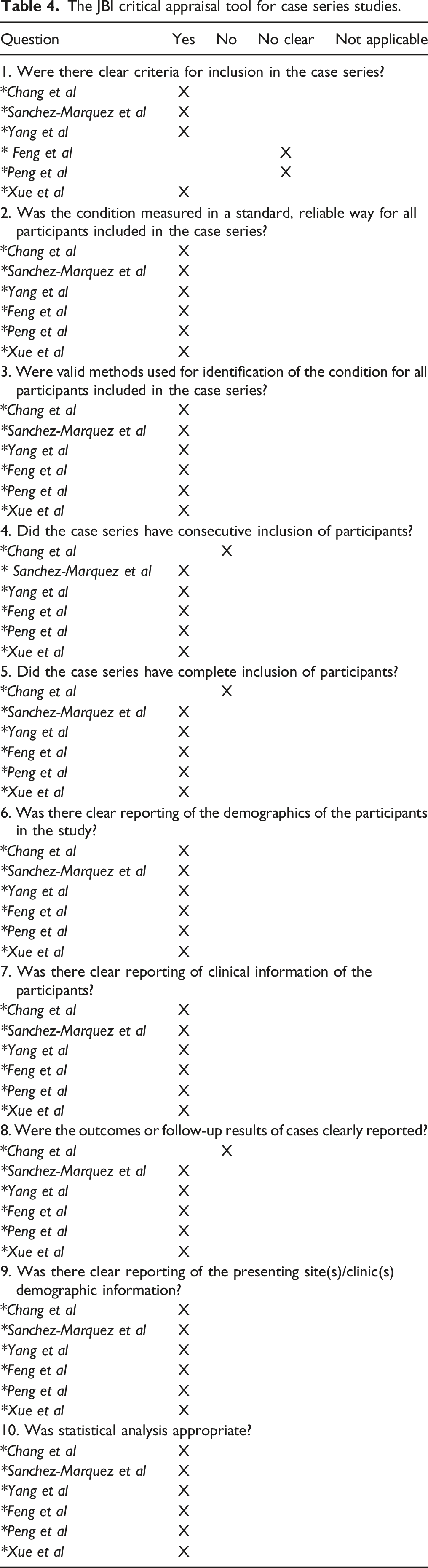
We found 140 articles. Articles in languages other than English (14), those without web page availability (4), review papers or case reports (21), and those not mentioning age at surgery (64) were excluded. Ten (10) other studies referring to HV localization only were also excluded. Of the remaining articles (27), five did not assess age at surgery and finally, 22 studies were included into the assessment of treatment (Figure 1). Additionally, critical subanalysis of the studies that reported posterior HV resection and fusion with pedicular screws was performed. We use the JBI’s tool for assessing case series.
31
Flow diagram for systematic reviews which included searches of databases and registers.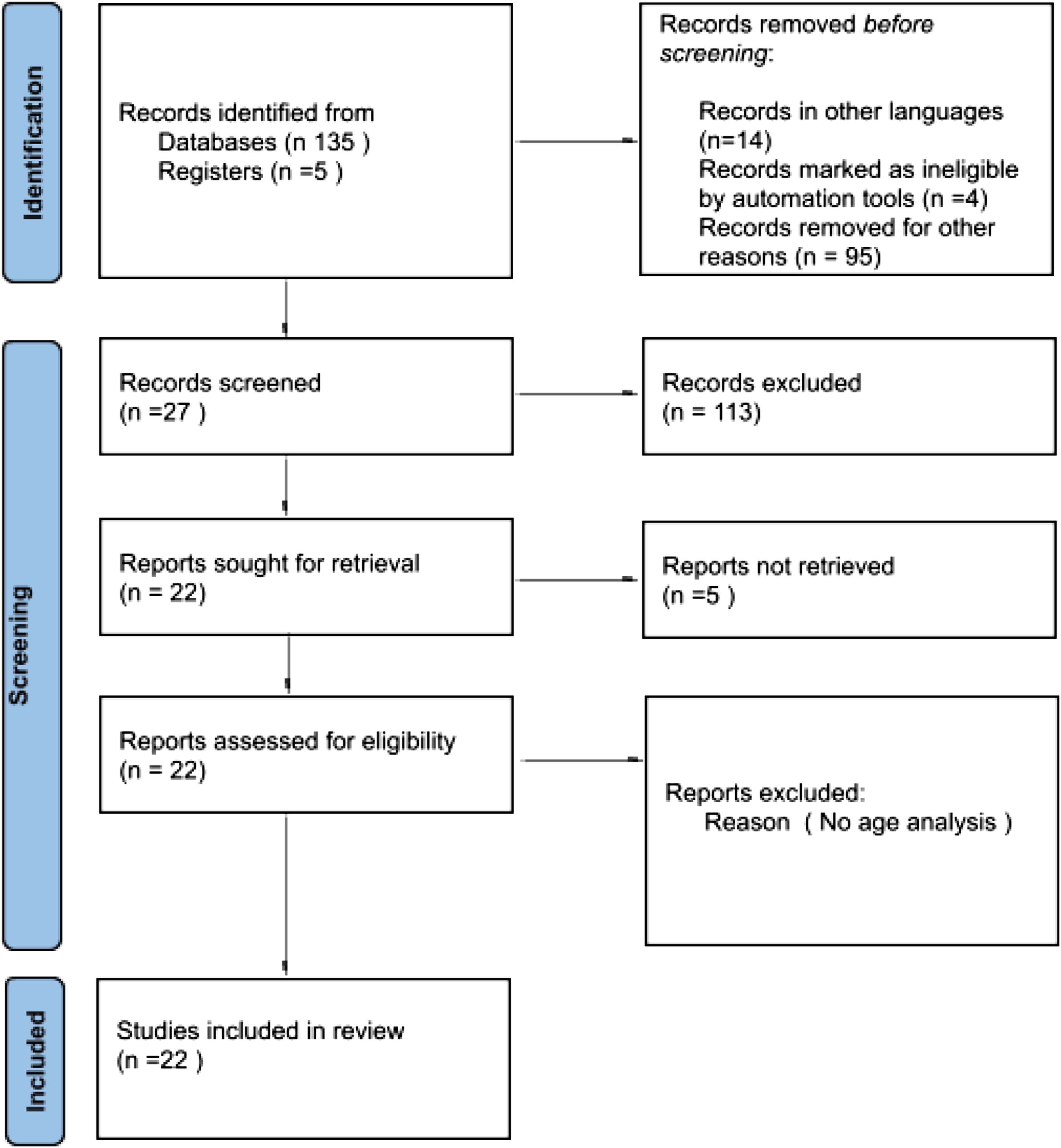
The study was approved by the hospital Institutional Review Board (IRB), because of the systematic review and observational nature of the study IRB waived the informed consent.
Results
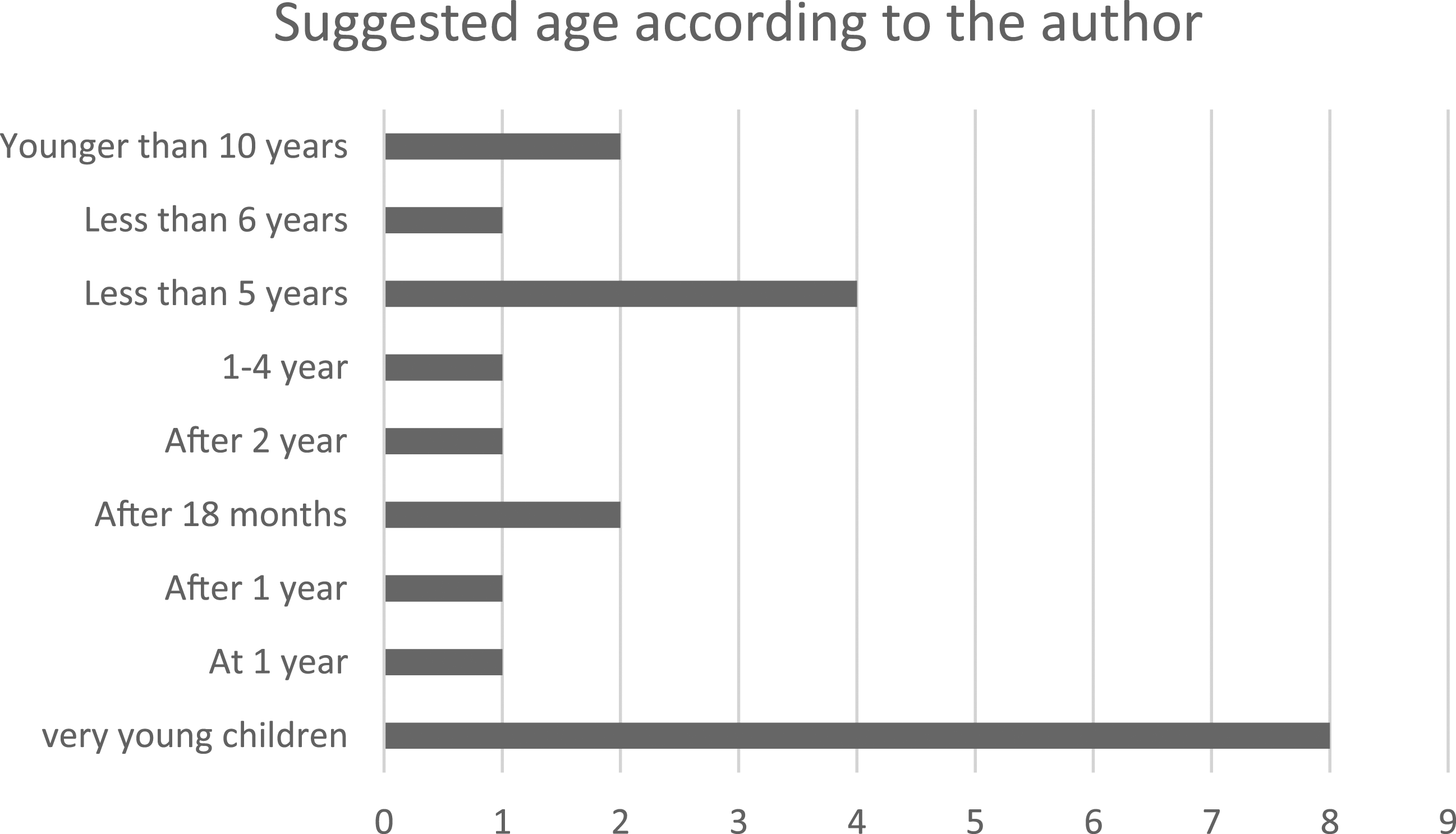
There was considerable heterogeneity in the included studies, both regarding age (Figure 2) and the surgical techniques used. There were large differences in sample size among studies as well. There was also a broad spectrum of recommendations regarding suggested age for treatment (Figure 3). Dispersion age of the different series. Recommendations age according to the authors.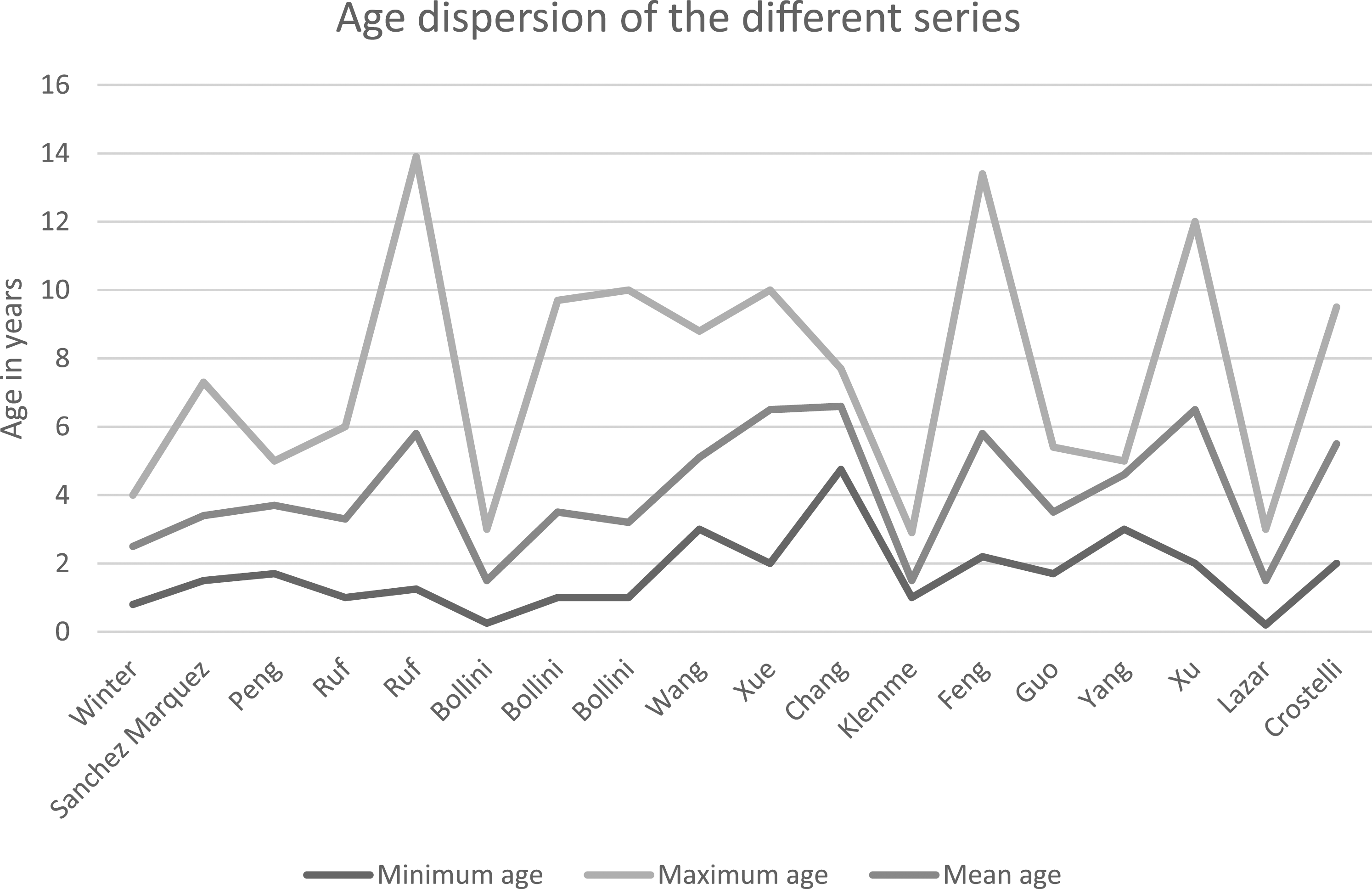
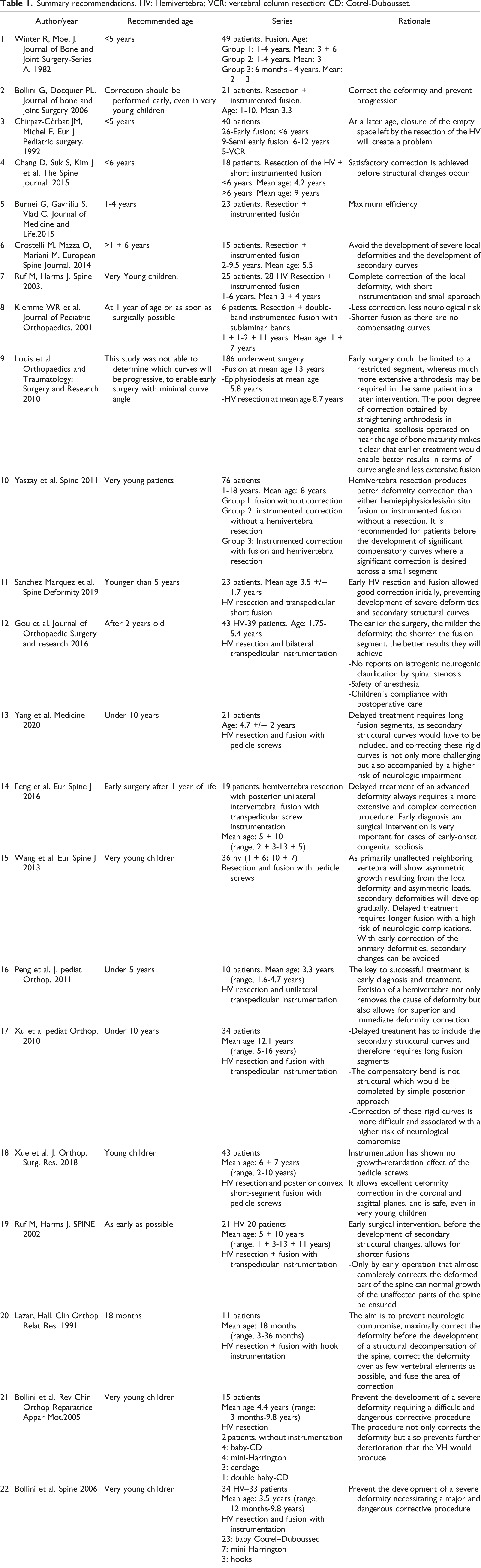
Summary recommendations. HV: Hemivertebra; VCR: vertebral column resection; CD: Cotrel-Dubousset.
The youngest patient undergoing resection and fusion was reported by Bollini et al. At the time of surgery, the infant was 3 months of life. HV resection was performed by a posterior and anterior approach and instrumentation consisted of compression of the convex side with a Harrington implant. However, the child was operated for pseudoarthrosis at 2 years and again at 9 years postoperatively for implant removal. 6 Lazar and Hall reported a 3-month-old child who underwent HV resection and instrumentation with a pediatric implant. This patient preoperatively had lower-limb weakness, hyperreflexia, and abnormal urodynamic studies. The patient was followed-up for 16 months, after which the implants were removed. Magnetic resonance imaging of the spinal cord showed no abnormalities. The authors recommend early intervention at a mean of 18 months. 7
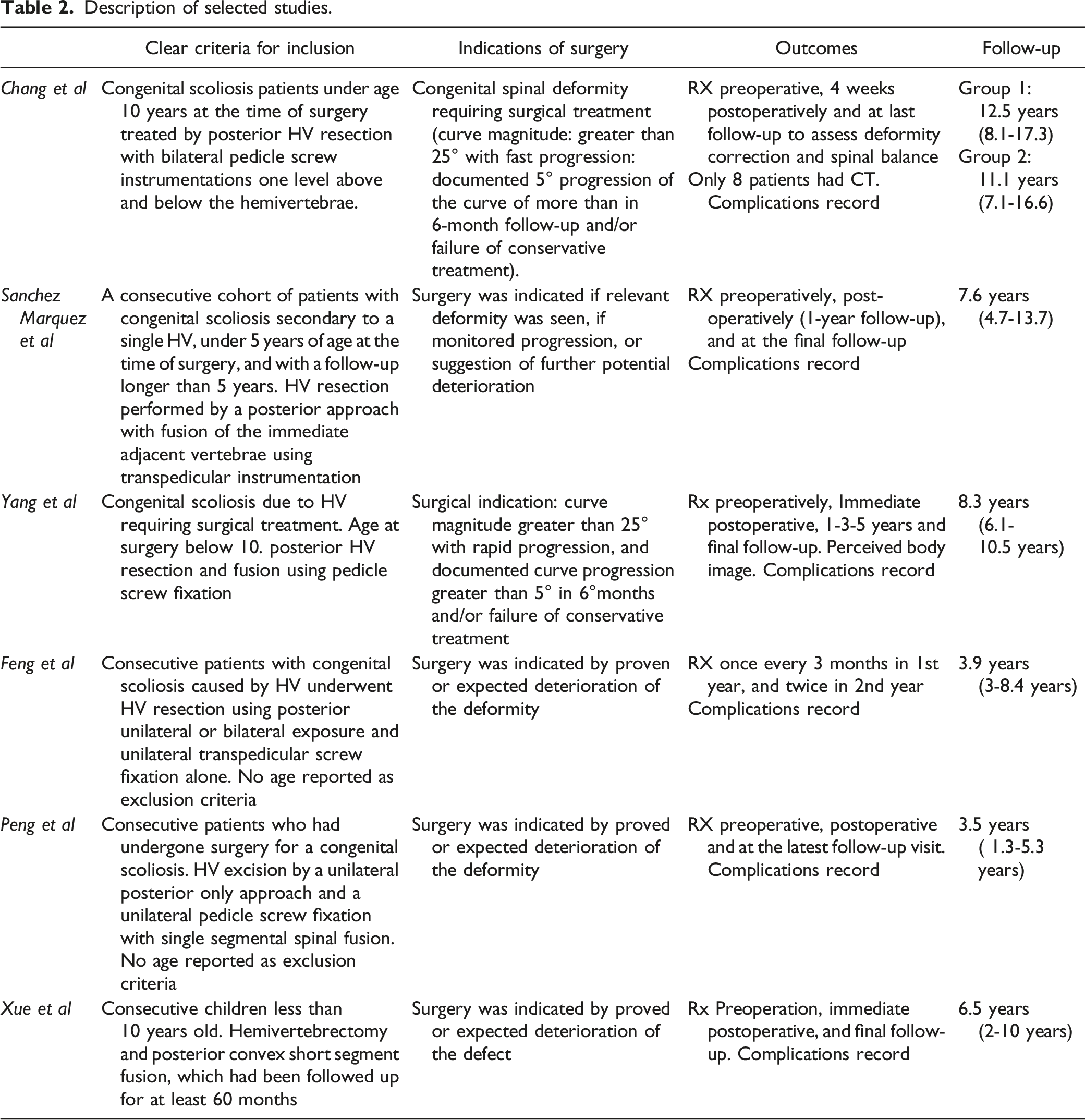
Description of selected studies.
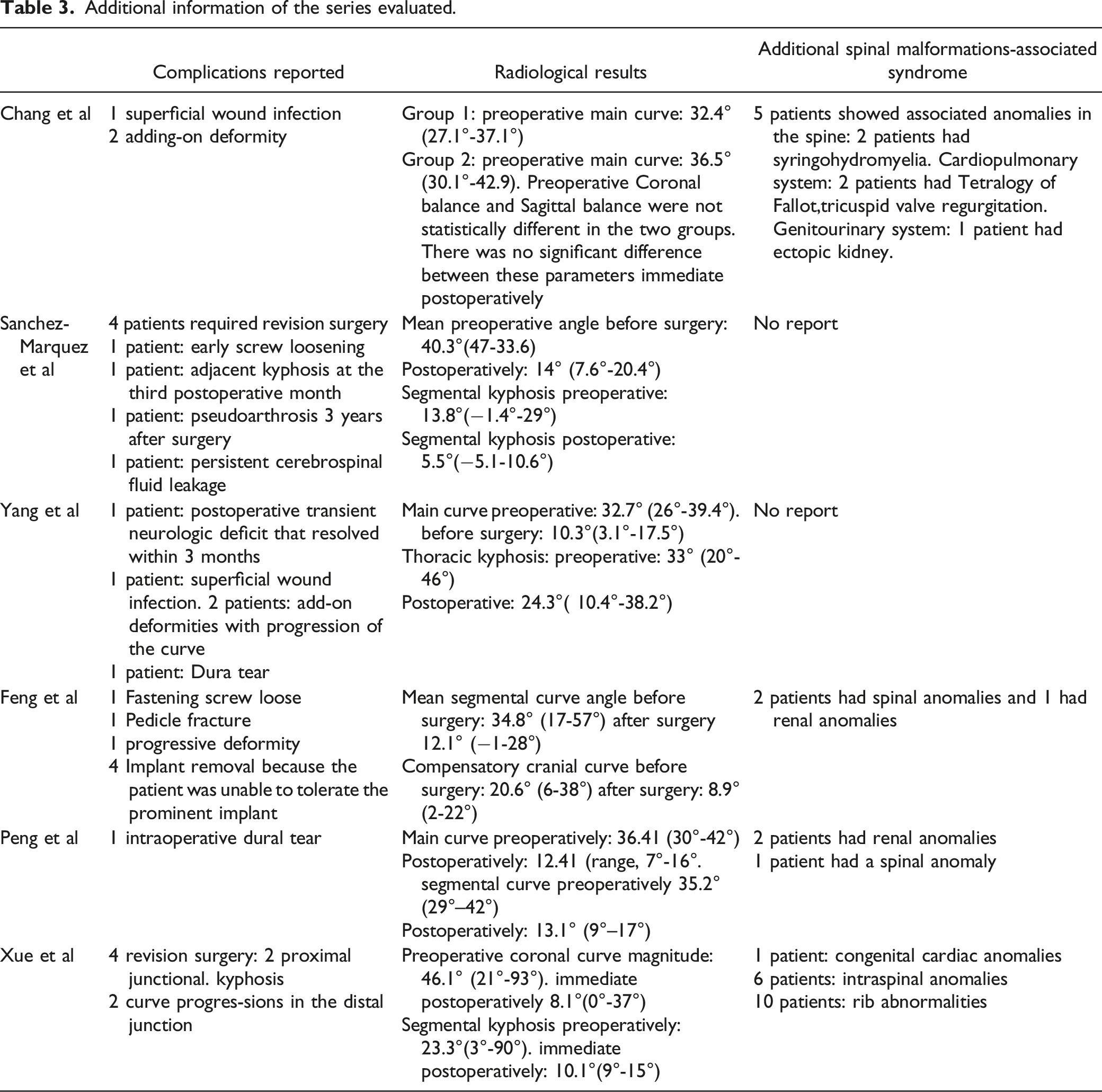
Additional information of the series evaluated.
The JBI critical appraisal tool for case series studies.
Discussion
We identified different factors that may be helpful to determine the minimum age at HV resection and fusion in congenital spinal deformity. It has been documented that around the age of 2 years, the bone structures are more easily identifiable. In addition, it is possible to predict acceptable bony fusion, and for construction pediatric instrumentation is available. 13
On the other hand, anesthesia-associated risks when submitting a young child to a surgical procedure were evaluated. Pulmonary developmental stability usually occurs only after the first year of life. Operating room electroencephalography and its sophisticated algorithm to predict the child’s consciousness state during anesthesia is limited before the first year of life as well. 14
Chang et al demonstrated that surgical treatment before the age of 6 years resulted in significantly better deformity correction with no negative effect on the growth of the vertebral bodies or canal compared to the group treated after 6 years of age. Early surgical correction of a congenital HV in children under 6 years of age, before structural changes may occur, effectively achieves a more satisfactory correction without causing complications in contrast with children older than 6 years but under 10 years of age. 9
Guo et al conducted a study in 39 patients aged between 1 + 8 and 5 + 5 with 43 HV treated with posterior hemivertebra resection and transpedicular instrumentation. They reported no major vascular or neurological complications and no pseudarthrosis or symptoms of spinal stenosis during follow-up; however, they did find one pedicle fracture, one rod breakage, and one need for additional surgery because of proximal junctional kyphosis (PJK). In addition, two implants had to be removed because of implant migration. Nevertheless, they recommend to perform posterior hemivertebra resection after the age of 2. 10
Xu et al. 11 and Yang et al. 12 performed HV resection and fusion using pedicle screws in children and found that in patients under 10 years of age the procedure was safe and effective and achieved rigid fixation together with deformity correction. They recommend complete excision of the HV and correction of the spinal deformities before secondary deformity occurs.
Progression of the deformities induced by HV is hard to predict. Several factors need to be taken into account, including HV type, number, and location, patient age, and potential growth. Curve progression may be slow or fast. It accelerates during the peak of puberty and stabilizes with bone maturity. The exact timing when the defect turns into a deformity is a matter of ongoing debate in the literature. This has been suggested to occur before the defect involves more than two adjacent vertebrae. 15 In congenital scoliosis, the Cobb angle is difficult to measure due to distortional end vertebrae and pedicle morphology in the immature spine. Loder et al assessed the inter- and intraobserver variability of the Cobb angle value in congenital scoliosis and found a variability of ±9.6° and ±11.8°, respectively, concluding that angle values with this level of variability cannot be used to determine the need for surgery. 16
In a case series of 50 children with congenital scoliosis due to HV, Chirpaz Cerbat et al found that this malformation was responsible for progressive deformity, largely predominant on the frontal plane. Mean postoperative follow-up was 5 years and 3 months. Three types of surgical procedures were performed: (a) hemivertebra resection, (b) posterior convexity fusion carried out before the age of 6, and (c) convexity fusion performed between the ages of 6 and 12. The postoperative results in children with a follow-up of more than 2 years and optimal resection and angle value showed few complications.
17
Winter and Moe published results of spinal arthrodesis for congenital spinal deformity in 49 patients who were younger than 5 years. The minimum follow-up was 5 years, and 11 patients had completed growth at the final follow-up visit. Posterior arthrodesis alone was found to be effective in most of the patients. They found minimum bending of the fusion mass, almost no lordosis, and minimum effect on torso-lower limb relationships. For congenital kyphosis, posterior arthrodesis was highly effective. 4
On the other hand, based on a series of 10 patients who underwent HV resection and unilateral transpedicular instrumentation, Peng et al suggested that excision of an HV not only removes the cause of the deformity but also allows for superior and immediate deformity correction, concluding that it is a less traumatic, simple, and safe procedure in children under 5 years of age. 18
Bollini et al consider that surgery should be performed as early as possible to avert the development of severe local deformities and prevent secondary structural deformities that would require more extensive fusion. They reported 21 children with lumbar HV and a mean age at surgery of 3 + 3 years, while the youngest patient was 12 months old. 19 Scoliosis and kyphosis can progress with growth in terms of angle value and number of vertebrae included in the main curve. This means that healthy vertebrae may be included in the deformity. In a different case series, the same authors analyzed 34 thoracolumbar HVs in 33 patients. Mean age at surgery was 3.5 years (range, 12 months to 9 + 8 years). Mean follow-up was 6 years (range, 1 year- 14 + 6). Twelve late complications were observed in seven patients. Nevertheless, the authors sustain that early surgery is recommendable, even in very young patients, and preventive of further curve progression due to the HV. Therefore, as soon as there is proof of progression HV, resection should be performed before more adjacent vertebrae become involved in the deformity process. In their opinion the “as soon as possible timing” refers to age younger than 3 years.19-20
Burnei et al performed 23 HV resections with a mean deformity angle value correction rate of 64%. They concluded that HV resection is the treatment of choice and is superior to in situ fusion and hemiepiphysiodesis. Maximal efficiency is obtained if performed at the age of 1-4 years. 21 On the other hand, Ruf and Harms evaluated a series of patients that underwent hemivertebra resection with transpedicular instrumentation. Their youngest patient was 1 + 4 years old at time of surgery. They confirmed that delayed treatment of a major deformity in older children or adults is more likely to involve secondary structural curves and therefore requires longer fusion segments. Correction of these rigid curves is more difficult and associated with a higher risk of neurologic events. The authors concluded that only by early and complete correction of the local deformity can the development of secondary curves be avoided. Hereby, primarily healthy adjacent segments are allowed to develop physiologically. In addition, early correction in young children requires a less invasive approach and short and sufficiently rigid instrumentation.22-23
Nnadi et al concluded that hemivertebra resection should ideally be performed in children around the age of 2 years, when the anatomy is easier to identify because the vertebrae are more ossified, a fusion can be achieved more predictably, and pedicle screw instrumentation can be used. 13 Klemme et al reported the results of a consecutive series of six very young children; mean age at surgery was 19 months (range 13-33). They concluded that despite the recognized growth effects and possible anesthetic risks of spinal surgery in very young children, there are several potential advantages of early surgery. Mainly, surgery of smaller-sized curves requires less correction and less surgical aggression and is associated with a lower neurological risk. Additionally, immature congenital curves may retain some local flexibility and often lack structural compensatory curves. Such curves, therefore, may permit a shorter arthrodesis. 24
Yaszay et al conducted a retrospective multicenter study reviewing 78 patients with a minimum follow-up of 2 years after HV resection. Mean age at surgery was 8 years (range, 1-18 years). The surgical procedures included in situ fusion (group 1), instrumented fusion without hemivertebra excision (group 2), and instrumented hemivertebra excision (group 3). The authors found that by removing the HV, worsening of the primary curves could be prevented. The mean age in the HV group was significantly younger than that in the other 2 groups. Patients who underwent hemiepiphysiodesis were older at the time of intervention and had larger secondary curves as well. As a result, more extensive fusions were performed in the latter group compared to groups 1 and 3 (7 vertebrae vs. 3 vertebrae). HV excision was shown to be safe and effective even in very young patients. 25
Sánchez Marquez et al analyzed 23 patients with a mean age at surgery of 3 + 5 years and a mean follow-up of 7 + 6 years. Their youngest patient was 1 + 8 years at the time of surgery. The authors concluded that early HV resection and transpedicular short fusion allowed good correction of the segmental and secondary coronal curves. They suggest that in very young patients it is important to prevent the development of severe deformities and secondary structural curves. 26 As primarily unaffected neighboring vertebra will show asymmetric growth resulting from the local deformity and asymmetric loads, secondary deformities will develop gradually. Delayed treatment of an advanced deformity always requires a more extensive and complex correction procedure.27-28
In a retrospective study conducted at our hospital, 67 pediatric patients undergoing 78 HV resection procedures were evaluated. Mean age at surgery was 5 + 5 years. The youngest patient was 0 + 8 year old. We suggested that patients may undergo surgery once they are 1 + 6 years old approximately, but there is no evidence to confirm this age limit. Nevertheless, bone volume and size are parameters to take into account in order to successfully remove the HV before it produces greater deformity. 1
Surgery seeks to correct spinal deformity due to HV and prevents the development of a compensatory curve, while conserving sagittal and frontal spinal balance and sparing as many vertebral levels as possible. Four procedures may be recommended, according to the type of HV and especially to patient age: arthrodesis, convex epiphysiodesis, and HV resection with and without instrumentation. The procedure of choice would be HV resection with instrumentation, which provides a 87.5% rate of good results. The procedure is relatively safe, conservative of spinal levels, and without age limit. 8 No negative effects of the pedicle screw instrumentation on vertebral body growth were observed. In the pediatric spine pedicle screws have shown to be safe and no spinal stenosis has been reported. 29 Nevertheless, in a series of 27 children who underwent two-level HV resection and short-segment posterior spinal instrumentation, Piantoni et al 30 found that the youngest patients were more likely to develop trunk imbalance after the peak of puberty. They concluded that this spinal imbalance showed minimal clinical signs or symptoms and no further surgery was needed.
Considering that there is some consensus in the most recent literature, as the best surgical technique is the early posterior early HV resection with bilateral or unilateral pedicular screws, there is no agreement on the ideal age. Despite this, there seems to be agreement between the authors at the time of surgical indication when there is proven or expected deterioration of the deformity.
Our preference is to perform the surgical treatment early. The guiding concept of our treatment is based on removing the defect before greater deformity is produced. We have evaluated the most appropriate age for a child to undergo surgery, taking into account different aspects such as anatomical development, anesthetic management and postoperative care. We usually establish a threshold of 18 months, although it is variable for each child.
There are several limitations to this study. Most importantly, the studies evaluated in this review were highly heterogeneous and conducted over many years including different treatments, fusion techniques, and types of implants leading to a large variability in the results. Nevertheless, this review may shed further light on the best treatment for these children, especially regarding timing.
Conclusions
How young a patient could and should be submitted to HV resection surgery is still a matter of debate in the literature. According to this review, prophylactic surgery might be a proper treatment for young children with congenital scoliosis before malformation becomes a deformity, adding no additional neurological, vascular, or anesthesia-related complications. The defect can be treated early while the deformity is treated late. Further prospective studies with longer follow-up periods are needed to determine the best age to treat children with HV.
Footnotes
Author Contributions
Design of study: SF, BF, LP, CAT, RR, and MN.
Consulting references: SF, LP, and EG.
Participation in draft manuscript: SF, CAT, LP, MN, and EG.
Revise manuscript: SF, CAT, RR, and MN.
Approved the final version of the paper: SF, BF, LP, CAT, RR, EG, and MN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
The study was approved by the hospital Institutional Review Board (IRB), because of the retrospective observational nature of the study IRB waived the informed consent.