
Abstract
Study Design:
Prospective observational study.
Objective:
In ACDF, graft failure and subsidence are common complications of surgery. Depending on the cervical fixation, different biomechanical characteristics are applied on the grafts. This aims to describe the incidence of cervical spacer failure in patients with cervical degenerative condition according to the cervical fixation method and sagittal balance.
Method:
From November 2011 to December 2015, 262 patients who underwent cervical spine surgery were enrolled prospectively. Patients were divided into 3 groups based on fixation method: anterior plate/screw (APS), posterior lateral mass screw (LMS), pedicle screw (PPS) groups. Serial X-rays and CT scans were utilized to evaluate radiologic outcomes.
Results:
Mean patient ages were 56.1 years in the APS group, 61.5 years in the LMS group, and 57.6 years in the PPS group (P = 0.002). Allospacer failure was most common in the APS group, compared to the LMS and PPS groups (chi-square, P = 0.038). Longer fusion level was associated with greater allospacer failure (Baseline 2 level surgery; Odds ratio (OR) 3.4 in 3 level, 15.2 in 4 level, P = 0.036,0.013). Higher T1 slope was correlated with less allospacer failure (OR 0.875, P = 0.001). ORs of allospacer failure in the LMS and PPS groups were 0.04 and 0.02, respectively, (P = 0.01, 0.01), compared with the APS group.
Conclusion:
This study was able to show that allospacer failure in multi-level ACDF surgery is more common with a longer fusion length, less postoperative T1 slope, and an anterior plate-screws technique. Pedicle screws provided the best biomechanical stability among the 3 constructs.
Introduction
Degenerative cervical spine conditions very commonly manifest from simple neck pain and progress to more debilitating signs and symptoms of myelopathy. These conditions are initially treated conservatively with medication, nerve blocks, and/or therapy. Surgery is undertaken in patients with severe symptoms or after failure of conservative measures.1-3 There are different surgical options available, with the ultimate goal of relieving cord compression and achieving adequate stability.1,2
Anterior cervical discectomy and fusion (ACDF) is performed as the gold standard for the treatment of degenerative cervical disc disease. 1 Numerous complications, including donor site pain, infection, and graft or cage subsidence, have been reported with the commonly used tricortical autologous bone grafts and titanium polyetheretherketone cages.1,4-6 Meanwhile, multilevel ACDF utilizing allografts has been shown to be as effective as that with autologous bone grafts, while avoiding the associated donor site morbidities. 7 Combined anterior-posterior surgeries may be performed if more extensive decompression or a more stable construct is needed.3,8,9
From a biomechanical point of view, the incidences of allospacer-related problems, such as subsidence, breakage, and dislodging, are expected to differ with anterior plating, posterior lateral mass screws, and pedicle screws. Finite element model analysis has shown that allospacer failure is less frequent in posterior fixation surgeries. 10
In this study, we investigated the incidence of postoperative allospacer-related radiologic outcomes based on the fixation method. We also analyzed the radiologic parameters related to the sagittal profile of the cervical spine as prognostic factors for allospacer failure.
Materials and Methods
This study was approved by the Institutional Review Board of the authors’ hospital. From November 2011 to December 2015, 406 patients who underwent multi-level cervical spine surgery (anterior and combined anterior-posterior surgery) were prospectively enrolled.
The patients who had less than 1 year of postoperative follow up were excluded from the study. Finally, 262 patients and 777 segments were enrolled and investigated. The mean follow-up period was 22.8 ± 5.3 months. Major diagnoses included cervical spinal stenosis (215 patients), cervical disc herniation (31 patients), and ossified posterior longitudinal ligaments (16 patients). All patients were treated with anterior discectomy and fusion using cervical allospacers fixed with anterior plate/screws (APS) (129 cases), posterior lateral mass screws (LMS) (74 cases), or posterior pedicle screws (PPS) (59 cases). A total of 117 (44.7%) patients underwent 2-level surgery, 74 patients (28.2%) underwent 3-level surgery, and 71 patients (27.1%) underwent 4-level surgery.
Surgical Indications and Technique
All patients who failed conservative treatment or those who presented with severe radiculopathy and/or myelopathy were recommended to undergo surgery. In all cases, the posterior longitudinal ligament was removed through cervical discectomy with an anterior approach, and the posterior one-fourth of the uncinate process was also removed. The proper size of Allobone cervical spacer (CORNERSTONE TM ASR, Medtronic Sofamor Danek, Inc., Memphis, TN, USA) was selected with great care, between 6-7 mm in height and 12-14 mm in anterior-posterior diameter, depending on the original disc height and tension after insertion of the allospacer. 11 Trial insertion was performed under guidance of a C-arm, during surgery, to prevent over-distraction of the segment or insertion of oversized allospacers. ACDF using allograft spacer insertion was performed between C3 and C7.
Depending on the severity of spinal cord compression and related myelopathic symptoms, the surgical approach was selected as either anterior surgery fixation with plate/screws (fixed type, unicortical screw) (ATLANTIS VISION® Elite Anterior Cervical Plate System, Medtronic Sofamor Danek, Inc., Memphis, TN, USA) or combined anterior-posterior (AP) surgery including decompressive laminectomy.12-14 A biomechanical study showed that the use of a short plate, with a plate to adjacent disc distance of more than 4 mm, and a screw angle insertion of more than 16 degrees has the highest mechanical stability, compared to different APS implant placement techniques. 15 In cases of combined anterior-posterior surgery, posterior fixation methods were preferentially selected using lateral mass screws and pedicle screws (VERTEX® Reconstruction System, Medtronic Sofamor Danek, Inc., Memphis, TN, USA) based on preoperative CT scans. In patients with a cervical pedicle diameter less than 3.5 mm or an anomaly of the vertebral artery, the LMS technique was selected. Postero-lateral fusion using autolamina bone harvested during decompressive laminectomy was added in posterior surgery cases. It is important to note that in the authors’ country, South Korea, the government only allows posterior fixation, with either lateral mass screws or pedicle screws, in combined anterior and posterior surgeries with very limited exceptions.
Evaluation of Radiologic Parameters and Functional Outcomes
From lateral cervical, whole spine X-rays and MRI scans, 16 cervical sagittal balance parameters, including C2-7 cervical lordosis (CL), C2-7 sagittal vertical axis (SVA), T1 slope, neck tilt, and thoracic inlet angle (TIA), were measured by blinded, independent, orthopedic spine surgeons on 2 occasions (intra-class correlation = 0.912, P value = 0.002). These parameters were previously proven to be correlated with surgical outcomes.17,18
Fusion was assessed through lateral and neutral flexion and extension radiographs and CT scans at the last follow up. Nonunion was determined based on instability greater than or equal to 2 mm in the interspinous distance on flexion-extension lateral radiographs.1,19 The absence of continuity in the fusion mass between the vertebral body and allospacers was also considered to indicate fusion failure with nonunion based on CT scans.20,21
The types of allospacer failure were as follows: (1) subsidence, defined as a more than 3 mm decrease in anterior or posterior height, compared to the immediate postoperative height;1,22 (2) breakage, crack or collapse of the allospacer; and (3) dislodgement, movement of the allospacer more than 2 mm, compared to the initial postoperative position (Figure 1).
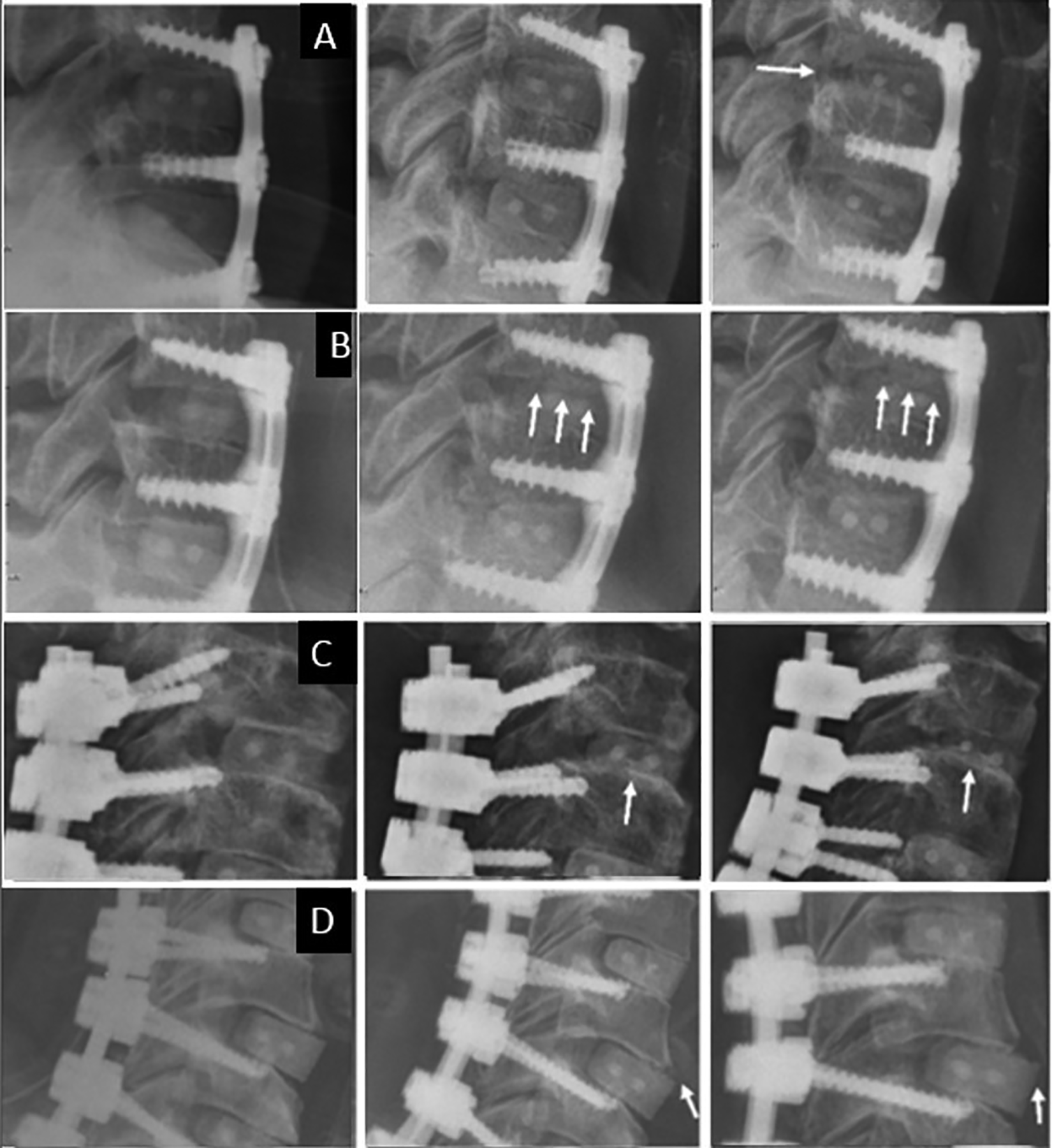
Patterns of allospacer failure on X-ray. A, Subsidence in anterior plates and screws. B, Allospacer breakage in anterior plates and screws. C, Subsidence in lateral mass screws. D, Dislodgement of allograft spacers in cervical pedicle screws.
Neck Disability Index (NDI) and Euro-QoL-visual analogue scale (VAS) scores were recorded during the initial preoperative evaluation and during postoperative follow up at 3 months and 1 year.18,23
Statistical Analysis
Basic statistical tests, including independent t test, ANOVA, and chi-square test, were used to evaluate significant differences between the APS, LMS, and PPS groups and between the allospacer failure and non-failure groups in terms of radiologic parameters and demographic factors. Post-hoc analysis by the Benjamini and Hochberg’s false discovery rate-Controlling method was also used to confirm statistical difference between groups. The backward multiple logistic regression analysis was used to calculate odds ratios (OR) of allospacer failure between possible influencing parameters, such as age, sex, radiologic parameters, and fixation method. All statistical analyses were performed using SPSS 22.0 statistics package (SPSS, International Business Machines Corp., NY, USA). P values less than 0.05 were considered statistically significant.
Results
Mean patient ages were 56.1 years in the APS group (range, 44-80 years), 61.5 years in the LMS group (range, 41-79 years), and 57.6 years in the PPS group (range 42-80) (P = 0.002, ANOVA). Other demographic comparisons are shown in Table 1. The presence of myelopathy, duration of symptoms, fusion length, and distribution of allospacer failure were significantly different among the APS, LMS, and PPS groups.
Comparison of Demographic Characteristics Between the 3 Patient Groups.
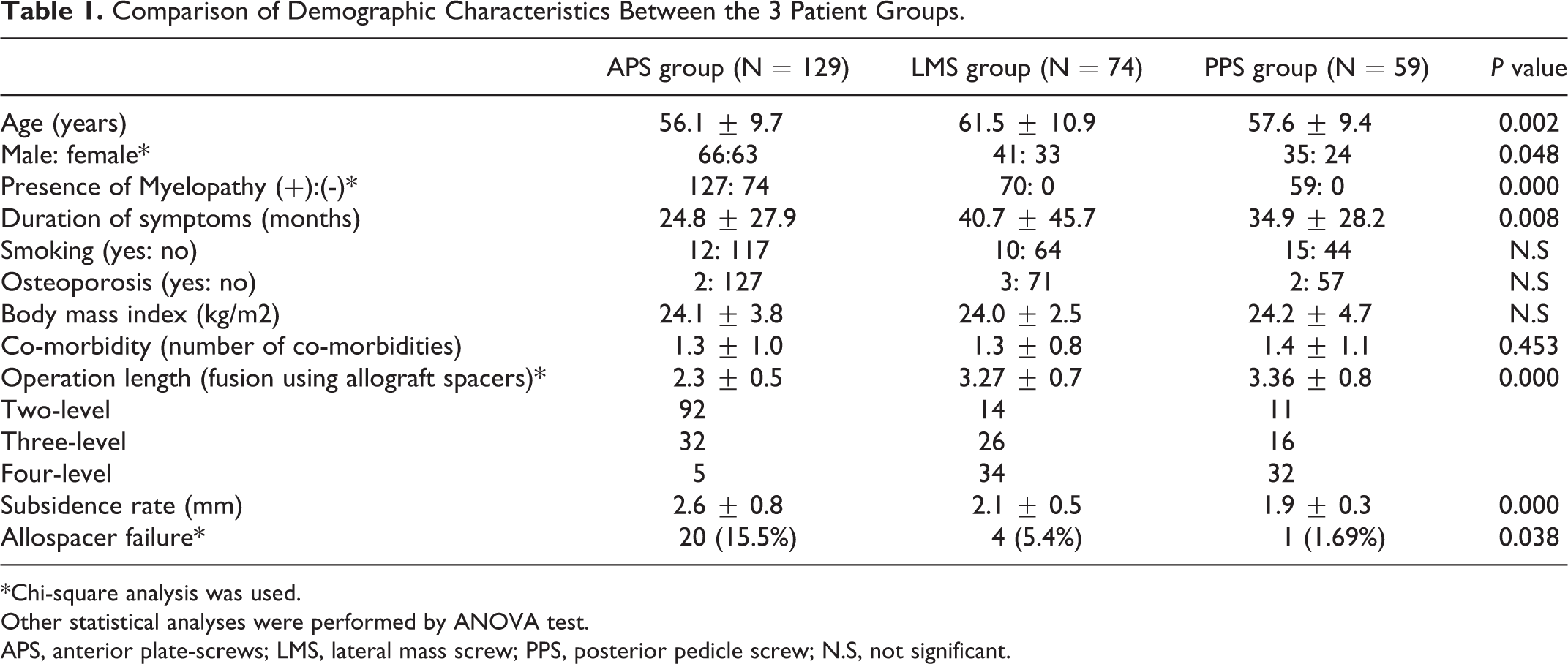
*Chi-square analysis was used.
Other statistical analyses were performed by ANOVA test.
APS, anterior plate-screws; LMS, lateral mass screw; PPS, posterior pedicle screw; N.S, not significant.
In post-hoc analysis, operation length in the APS group was significantly shorter than that in other groups (P = 0.000). Duration of symptoms in the LMS group were significantly higher than those in the APS groups (P = 0.008).
The fusion rates at 1-year follow-up were 91.5% (9 cases of nonunion out of 129 cases) in the APS group and 100% in the LMS and PPS groups, which had autolamina postero-lateral fusion added to the procedure. Among the non-union patients, 2 who experienced breakage and subsidence at the same time underwent posterior fixation with pedicle and lateral screws and posterior fusion, which ultimately led to fusion. The mean NDI scores in all patients were 24.0 ± 12.5 preoperatively, 8.4 ± 7.8 at 3 months postoperatively, and 9.8 ± 8.6 at 1 year postoperatively (P = 0.000, ANOVA). The mean EQ-VAS scores for general health status were 52.2 ± 21.4 5 preoperatively, 88.4 ± 9.4 at 3 months postoperatively, and 85.4 ± 13.4 at 1 year postoperatively. (P = 0.000, ANOVA) There were no statistical differences in NDI or EQ-VAS scores among the APS, LMS, and PPS groups or between the allospacer failure and non-failure groups.
Radiologic Parameters of Cervical Spine Sagittal Balance
Measured values of the radiologic parameters and a comparison thereof among fixation (APS, LMS, and PPS) and allospacer failure (failure and non-failure) groups are presented in Table 2. There were no significant differences in radiologic parameters according to fusion length. When comparing allospacer failure, T1 slope at postoperative 1 year was significantly higher in the non-failure group than in the failure group (31.5 ± 7.0 vs. 23.9 ± 9.5, P = 0.000, independent t test). Comparing the allospacer failure and non-failure groups, the amount of postoperative change in T1 slope was significantly different when measured on images taken at 3 months postoperatively (−1.8 ± 11.7° vs. 3.2 ± 10.9°, P = 0.03). No other parameters were significantly different, including postoperative 1 year measurements.
Comparison of Radiologic Parameters Between Groups.
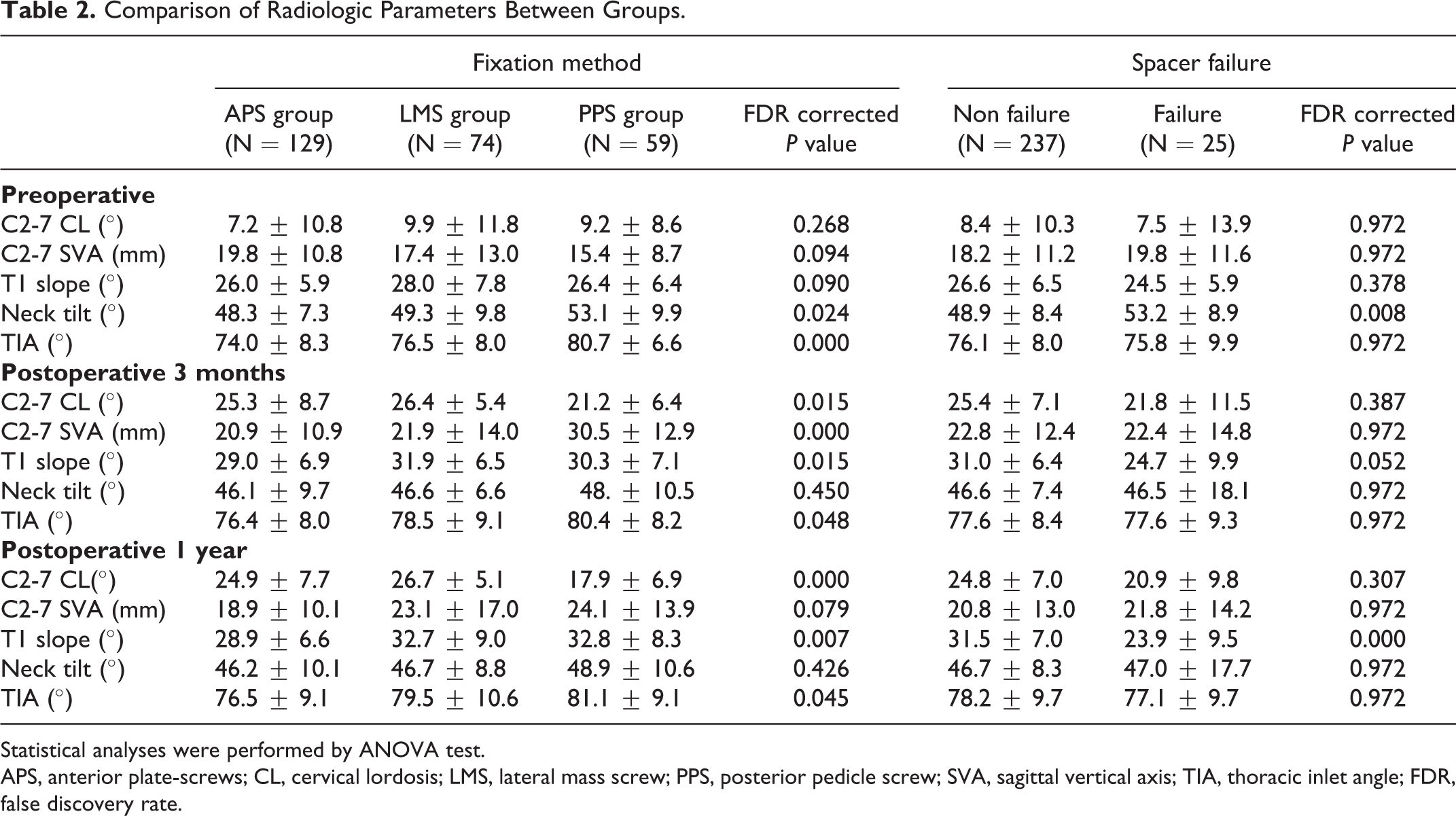
Statistical analyses were performed by ANOVA test.
APS, anterior plate-screws; CL, cervical lordosis; LMS, lateral mass screw; PPS, posterior pedicle screw; SVA, sagittal vertical axis; TIA, thoracic inlet angle; FDR, false discovery rate.
The amounts of C2-7 CL and C2-7 SVA correction in the PPS group (9.8 ± 9.3°, 11.8 ± 17.7 mm) were significantly different, compared with the APS (16.6 ± 13.8°, 3.8 ± 12.8 mm) and LMS groups (15.6 ± 13.5°, 0.1 ± 10.3 mm), at postoperative 3 months (P = 0.021, 0.000, ANOVA). The amounts of C2-7 CL and C2-7 SVA correction in the PPS group (5.0 ± 14.4°, 3.63 ± 16.8 mm) were also significantly different than those in the APS (14.3 ± 14.4°, −3.4 ± 11.5 mm) and LMS groups (15.0 ± 13.2°, 4.1 ± 17.0 mm) at 1 year post-operation, compared to preoperative measurements (P = 0.001, 0.001, ANOVA).
Allospacer Failure
Patterns of allospacer failure, theoretical schematic diagrams, and clinical results are presented in Figures 1 and 2 and in Tables 3 and 4. There were no differences between the failure and non-failure groups in terms of age, duration of symptoms, fusion length, presence of myelopathy, and sex distribution. The mean subsidence values during follow up were 3.8 ± 1.0 mm in the allospacer failure group and 2.2 ± 0.5 mm in the non-failure group (independent t-test, P = 0.000). In post-hoc analysis, subsidence in the APS group was significantly greater than that in the LMS and PPS groups (P = 0.000, 0.000) (Table 1). In multiple regression analysis, the ORs of allospacer failure based on possible influencing factors were analyzed (Table 4). The 3- and 4-level surgeries were correlated with an increased incidence of allospacer failure, compared to the 2-level surgery (P = 0.036,0.013). An increase in postoperative T1 slope was correlated with a decreased incidence of allospacer failure (P = 0.001). Among fixation methods, both the LMS and PPS groups demonstrated significantly lower ORs of allospacer failure, compared to the APS group (P = 0.010, 0.010).
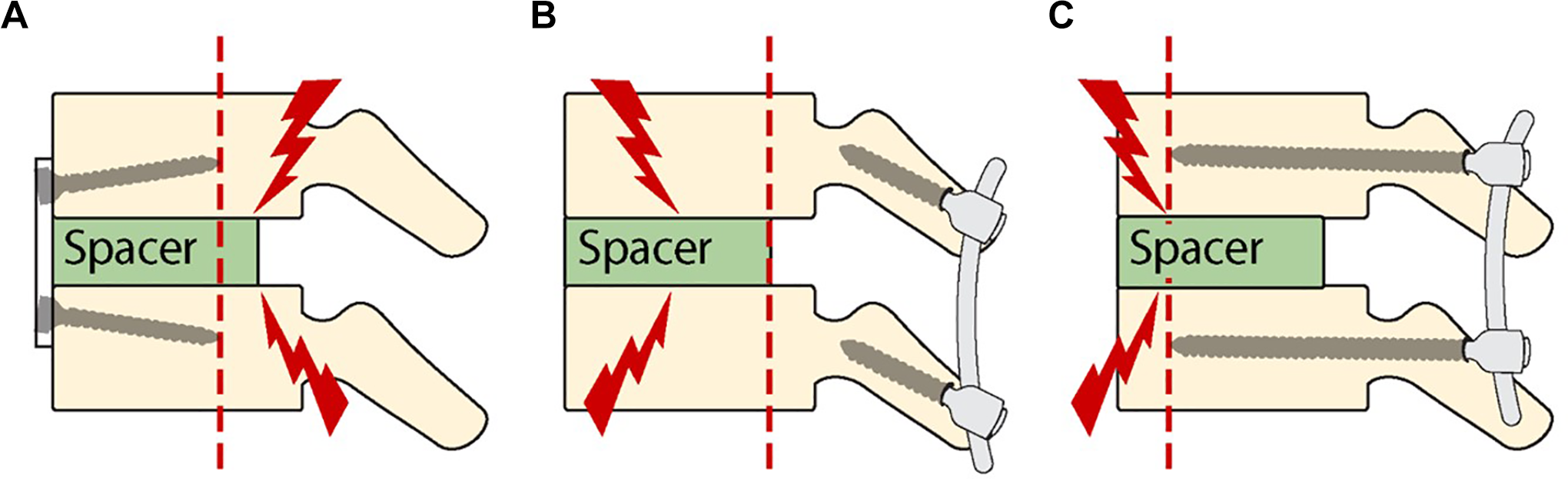
Schematic diagram of each fixation method and possible screw failure areas. A, Anterior plate/screw fixation shows a portion of the allospacer that could not be covered by screw fixation. B, Lateral mass screws fixation mainly prevents the posterior disc height from decreasing. C, Pedicle screw fixation covers all 3 columns of the cervical spine, although most of the anterior portion of the allospacer might not be covered.
Distribution of Allospacer Failure Type.
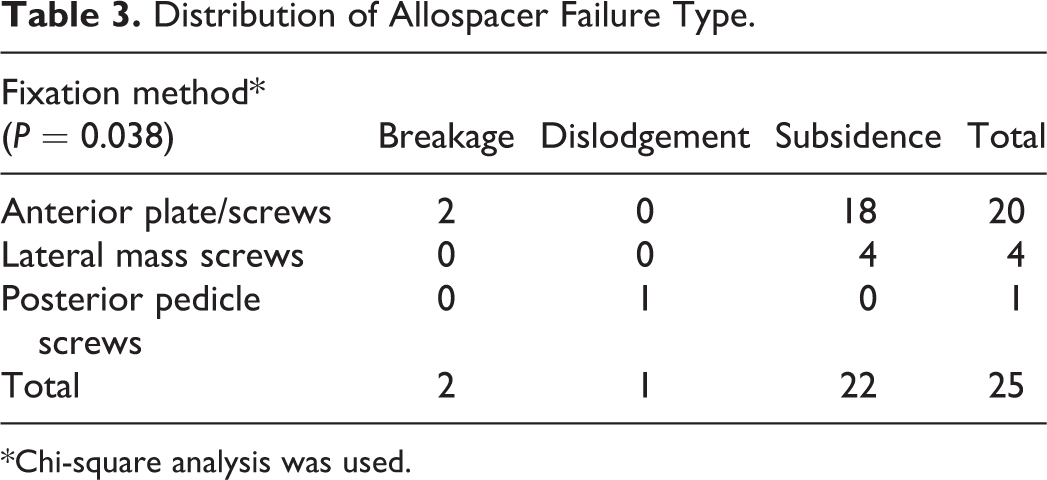
*Chi-square analysis was used.
Multiple Logistic Regression Analysis for Allospacer Failure.
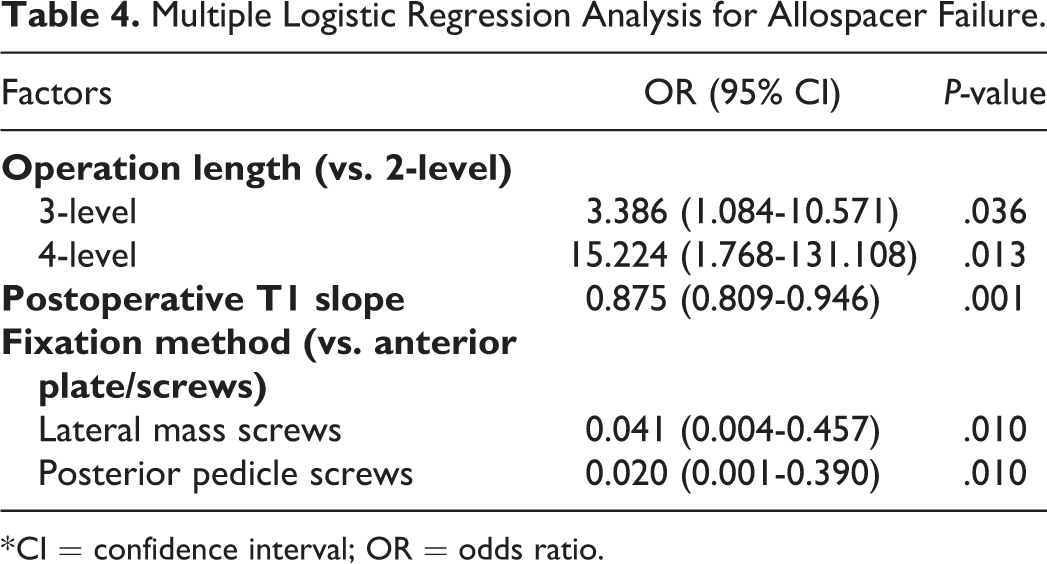
* CI = confidence interval; OR = odds ratio.
Discussion
Graft failure is a major concern in ACDF surgery using a stand-alone cage or reinforcement with anterior plates and screws.22,24 Age, plate use, and other related factors, such as a greater number of surgically treated levels and use of oversized cages, could affect graft subsidence. 22 In a recent study, Woo et al. noted graft collapse in 28.8% and subsidence in 4.5% of patients who underwent 2-level ACDF.25,26
In a biomechanical study comparing stress distribution and subsidence risk of APS, LMS, and PPS techniques, PPS gave the best mechanical stability, showing equal distributions of stress on the construct. 10 The buttress effect of anterior plate and screws prevents collapse between the vertebral body and allospacers. 27 However, it still has the mechanical weakness of load-sharing in the posterior column of the vertebral body, noted especially on extension, as shown in Figure 2. 10
Combined anterior and posterior surgery is commonly used to achieve better outcomes than anterior surgery only, including better correction of sagittal balance, a higher rate of fusion, and fewer complications. 12 In posterior surgery, lateral mass screws could provide mechanical support against the reducing force of the posterior disc height, which is improved after insertion of the allospacer. As shown in Figures 1 and 2, subsidence in the LMS group elicited a greater decrease in anterior disc height, compared to posterior disc height. Theoretically, pedicle screws could provide support from the posterior to the anterior column and could allow for better load sharing, compared to LMS.10,28 Also, pedicle screws are well known to have stronger pull-out strength and support than LMS.29,30 Pedicle screws have been shown to have better strength even after cyclic loading and a lower incidence of screw failure at the screw-bone interface. 31
In patients undergoing anterior cervical spine surgery, a small amount of subsidence has been shown to be beneficial to achieve bony fusion. However, an increased amount of subsidence has detrimental effects: it can cause changes in spinal geometry, decreases in the foraminal space, and screw failure. 22 ACDF with rigid plating lessens the severity of subsidence, making it an effective procedure in patients with more than 2 levels of ACDF, with no need for additional procedures. 32 As expected, allograft subsidence was common in the APS and LMS groups. Instead of subsidence, allospacer dislodgement was observed in the PPS group, which could have resulted from greater load sharing of the PPS construct.28,33 Most cases resulted in bony union without subsidence; however, in one patient, it was not sufficient to secure the axial load to hold the allospacer in its original position until fusion occurred. This suggests that certain amounts of subsidence and axial load bearing are essential to achieve successful fusion between the vertebral body and grafts. 22
In a recently published article by Kwon et al, they were able to show stress distributions on the fixation device and bone interface. The authors demonstrated differences in the effects of 3 fixation methods on the allospacers, vertebral body and implants used. Ultimately, the results indicated that PPS has the best mechanical stability, except in flexion, providing the lowest risk of subsidence. Finite element model analyses in the study also showed high risk areas of failure for each of the 3 procedures: the screw-cancellous bone interface in APS, the screw-posterior element bone contact area (medial part of the screw hole) in LMS, and the screw-bone insertion site in PPS. 10 Except for pedicle screws, all of these could result in fixation loss and allospacer failure.
Through multiple logistic regression analyses, we discovered that, among other factors, a higher T1 slope was correlated with a lower incidence of allospacer failure. This indicated that a higher slope produces lordosis that is restored to normal values and is related to physiologic load bearing on the allospacer and posterior facet joints.34,35 In contrast, decreased cervical lordosis related to less T1 slope might affect allospacer failure by increasing the vertical load placed on the allospacer and vertebral body.35,36
Our study had several limitations. First, different surgical indications for anterior surgery and combined anterior-posterior surgery made it difficult to evenly allocate patients into 3 groups. In some of the combined anterior-posterior surgery patients, there was an anatomical abnormality and congenitally narrow pedicle diameter, as observed on preoperative CT scan. Considering this anatomical variety, LMS could be more easily performed in most patients.
Second, we were unable to demonstrate statistical differences in functional outcomes between the allospacer failure and non-failure groups because the number of patients in the allospacer failure group was small. However, it has been reported that subsidence and graft have no apparent impact on successful fusion or clinical outcomes in patients who undergo ACDF.22,37 Lastly, in this study, there were 25 events related to allospacer failure among 262 cases. Usually, in logistic regression analysis, roughly 1/10 of the total number of events could be considered as independent variables (the rule of experience or rule of 10) In other words, in the logistic regression analyses, 10 fold the number events can be expected considering the number of independent variables. However, there is a publication on relaxing the rule of 10 events per variable (EPV). 38 From the article, we could confirm that a total number of 5 to 9 EPV in a sample size of 256 would not differ significantly with an EPV of 10-16 in the same sample size of 256. Contrarily, if the EPV was between 2 to 4, the confidence interval coverage rate could stray away from the 95% range and pose a higher risk of relative bias. We believe the analyses in the present study to be in an acceptable range of analysis with an EPV of 5 (Table 4). Further study including a larger EPV and related analyses should be performed to draw a sounder conclusion.
Despite these limitations, this is the first study to report different patterns of allospacer failure along with cervical radiological parameters, which could potentially result from the biomechanical differences between fixation methods. The main goal of this study was to demonstrate the expected radiologic outcomes of different fixation methods to help surgeons in assessing different parameters at follow up and to explain the possible risks and benefits to patients pre- and postoperatively. All 3 fixation methods may be used in cervical spine surgery, but knowing the possible outcomes would be helpful to both the surgeon and patient.
This study was able to show that allospacer failure in multi-level ACDF surgery is more commonly observed with a longer fusion length, less postoperative T1 slope, and an anterior plate-screws technique. This study can help surgeons in deciding the type of surgery suitable for patients by showing the most likely outcome and pattern of possible failure for each surgical technique. Nevertheless, different surgical indications among fixation methods and no observable differences in functional outcomes should be considered.
Footnotes
Acknowledgments
The authors would like to thank MID (Medical Illustration & Design) for providing support with the medical illustration and professor Hye-Sun Lee for providing support with the extra-statistical analyses, a part of the Medical Research Support Services of Yonsei University College of Medicine.
Authors’ Note
The data will be available upon reasonable request. This study was approved by the Institutional Review Board of the Severance hospital (3-2017-0061).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.