
Abstract
Objective
This study aimed to evaluate the efficacy and safety of vertebroplasty versus posterior pedicle screw fixation combined with vertebroplasty in treating stage III Kummell’s disease without neurological deficits.
Method
A systematic literature search was conducted across six databases. A meta-analysis of prospective and retrospective studies meeting the inclusion criteria was conducted using Review Manager 5.4.1.
Results
Eight studies (one prospective, one randomized control trial, and six retrospective) involving 409 patients were included. Vertebroplasty demonstrated advantages over posterior pedicle screw + vertebroplasty in operative time (weighted mean difference: −83.22 min; 95% confidence interval: −97.70 to −68.73; p < 0.05), blood loss (weighted mean difference: −158.65 mL; 95% confidence interval: −219.99 to −97.31; p < 0.05), and hospital stay (weighted mean difference: −5.64 days; 95% confidence interval: −7.36 to −3.92; p < 0.05). No significant differences were observed in Cobb’s angle (weighted mean difference: 1.28°; 95% confidence interval: −0.21 to 2.78; p > 0.05), relative anterior vertebral height (weighted mean difference: 2.98%; 95% confidence interval: −4.15 to 10.11; p > 0.05), cement leakage (13.2% vs. 8.5%; odds ratios: 1.67; 95% confidence interval: 0.86–3.24; p > 0.05), or wound infection (0% vs. 4.88%; odds ratios: 0.28; 95% confidence interval: 0.07–1.15; p > 0.05).
Conclusion
Both vertebroplasty and posterior pedicle screw + vertebroplasty are effective for treating stage III Kummell’s disease without neurological deficits. Vertebroplasty offers superior perioperative outcomes with reduced surgical trauma and hospital stay.
PROSPERO registration number: CRD420251031065.
Background
Kummell’s disease (KD) is characterized by vertebral ischemic necrosis leading to intravertebral vacuum clefts, vertebral collapse, pseudoarthrosis, and kyphosis within weeks to months of injury.1–3 Neurological symptoms may arise from spinal stenosis. Current management follows Li’s three-stage classification.2,4
Stage I: No vacuum cleft on imaging; vertebral height compression <20%. Stage II: Height compression >20% with intact posterior wall. Stage III: Severe collapse with posterior wall rupture, vertebral cleft signs on magnetic resonance imaging, and potential neural compression.
Although percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP) is effective in treating stages I–II KD,5,6 optimal management for stage III KD without neurological deficits remains controversial. 7 Open reduction and internal fixation are preferred when neurological deficits exist.8–11
However, select stage III patients exhibit dural/nerve root compression without neurological symptoms, 12 posing challenges for surgical strategy selection. VP (minimally invasive) and posterior pedicle screw (PPS) + VP (provides spinal stability) are common options, although the risk of cement leakage associated with VP and the risk of perioperative complications associated with PPS + VP require consideration. PPS + VP can improve the broken vertebral body height and kyphosis deformity 13 but has some drawbacks, including long surgical trauma and perioperative complications. 9
Recent studies report comparable efficacy of VP and PPS + VP for treating stage III KD without neurological deficits.8,14–16 Two studies14,16 also suggested that VP had certain advantages in terms of surgery duration, blood loss, and postoperative complications.
Currently, the treatment options for stage III KD without neurological deficits are controversial due to the limited studies on the comprehensive analysis of this disease. Therefore, a larger sample size and higher-level evidence-based medical studies are needed to support decision-making. 14 This meta-analysis synthesizes evidence based on the existing data to guide clinical strategy.
Methods
Evidence resource
In this study, the meta-analysis was performed using a literature search, inclusion and exclusion criteria, outcome measures, quality assessment, and statistical analyses, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-2020 guidelines. 17 The observational protocols of this study included prospective randomized control trials (RCTs) or retrospective comparative studies.
Literature search strategy
In the current study, literature was searched irrespective of the country’s language or publication type. The electronic databases, including PubMed, Web of Science, Cochrane Library, China National Knowledge Infrastructure, Wanfang Data, and China Science and Technology Journal Database, were searched from the beginning until 1 March 2023. The MeSH terms and their combinations, which were searched in [Title/Abstract], were as follows: Kummell, Kümmell, avascular osteonecrosis of a vertebral body, vertebral osteonecrosis, intravertebral vacuum cleft, delayed vertebral collapse, and compression fracture nonunion. The references of all the retrieved studies, review articles, and abstracts of conferences were also manually searched.
Inclusion and exclusion criteria
The available prospective, RCT, and retrospective comparative studies demonstrating the comparison between VP and PPS + VP were searched. As the results of PVP and PKP-based meta-analyses of RCTs showed no significant differences between the groups,5,18,19 the studies employing PVP or PKP for KD without neurological deficits were included in this study. All these studies analyzed at least one of the quantitative or qualitative outcomes in this comparison. Furthermore, editorials, review articles, case reports, incomplete data, experimental animal studies, and basic studies were excluded from this study.
Outcomes of interest
Surgical outcomes, radiographic measurements, and adverse events were the primary outcomes of this study. In case of availability of sufficient data, the observations and comparisons were made at different time points.
Surgical outcomes were measured by observing the time of operation, loss of blood during the operation, and time of hospital stay for observation. Radiographic indices included Cobb’s angle (kyphotic wedge angle) and relative anterior vertebral height (AVH). The worst events observed included the leakage of bone cement and infection of wounds. Secondary outcomes included measures of clinical efficacies such as postoperative pain and function. Visual analog scale (VAS) and Oswestry Disability Index (ODI) were used to measure postoperative pain 20 and postoperative function. 21
Quality assessment
The level of evidence observed in the studies was rated based on the criteria of the Centre for Evidence-Based Medicine, University of Oxford, UK. 22 Cochrane risk-of-bias tool and modified Newcastle–Ottawa scale were used to assess the methodological quality of the RCTs 23 and retrospective studies,24,25 respectively. The assessment was based on three factors: selection of patients, comparison of the study groups, and assessment of outcome. Overall, the evidence rating of the included studies was comparatively low. We did not conduct the GRADE (Grading of Recommendations Assessment, Development and Evaluation) evaluation. In this meta-analysis, retrospective studies were rated as high, medium, and low grades using the abovementioned scale (Table 1). RCTs and prospective studies, which received a high rating, were considered of high quality.
Characteristics of the included studies.
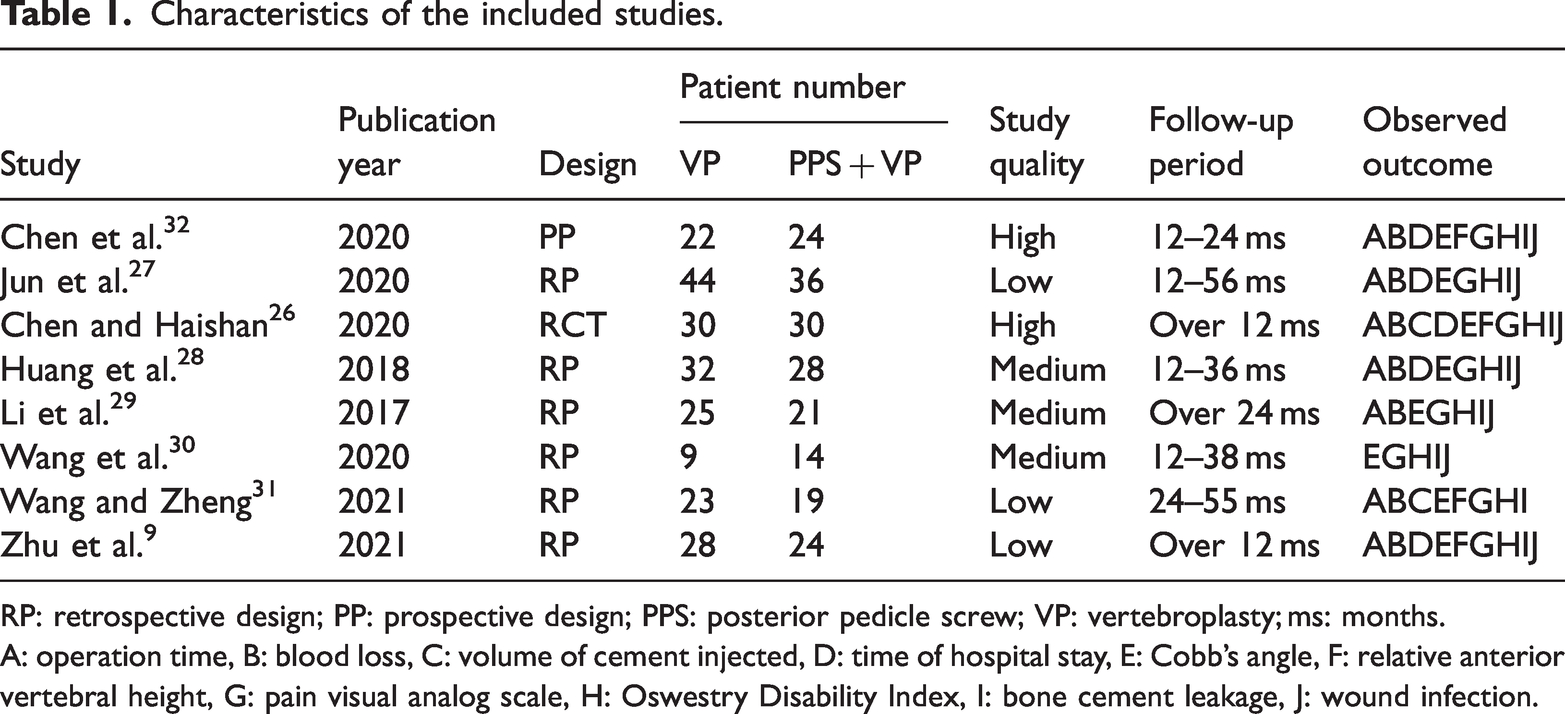
RP: retrospective design; PP: prospective design; PPS: posterior pedicle screw; VP: vertebroplasty; ms: months.
A: operation time, B: blood loss, C: volume of cement injected, D: time of hospital stay, E: Cobb’s angle, F: relative anterior vertebral height, G: pain visual analog scale, H: Oswestry Disability Index, I: bone cement leakage, J: wound infection.
Statistical analysis
Review Manager 5.4.1 (Cochrane Collaboration, Oxford, UK) was used to perform the meta-analyses. The continuous and dichotomous variables were measured using weighted mean difference (WMD) and odds ratios (OR), respectively. All the results were reported with 95% confidence intervals (CIs). Standard deviations were calculated using the technique described previously by Hozo et al. 33 for the studies expressing the mean and range values of the continuous data. The chi-square test was used to assess the statistical heterogeneity between the studies. A p value of <0.10 was considered statistically significant, and heterogeneity was quantified using the I2 statistics. The random-effects model was used if heterogeneity was present among the studies; otherwise, the fixed-effects model was used. 23
Subgroup analysis was performed by recording the postoperative Cobb’s angle using VP versus PPS + VP in the diseased vertebra with cement fixation and the diseased vertebra with cement and screw fixation, respectively. The publication bias was shown, and a funnel plot was presented using the subgroup analysis.
PROSPERO registration
This study was registered post-study at PROSPERO registry: registration number CRD420251031065.
Results
Evidence synthesis
In the final analysis, eight studies involving 409 cases (213 vs. 196 cases for VP vs. PPS + VP), which met the inclusion criteria, were included in this study, as shown in Figure 1. All the studies were full-text articles. Two authors showed 100% agreement on study selection and 95% agreement on quality assessment. The disagreements were resolved by consulting with the chief physician in our department.

Flow diagram of the studies identified, included, and excluded as per the PRISMA guidelines.
Characteristics of the eligible studies
One prospective, 32 one RCT, 26 and six retrospective studies27–31,34 were included (Table 1). The retrospective analysis included case–control studies comparing similar number of cases. Regarding latest articles, six studies26,27,30–32,34 published after 2020 were included. The studies involving KD patients without neurological deficits were included. All the studies reported both the pre- and postsurgery data with over 1-year follow-up. The number of resulting indices ranged from five to nine.
Quality of the included studies
The studies included in this study were of low quality. Real randomization was used in an RCT. 26 The RCTs recorded the method of randomization but not the blindness of the information in the study. Seven studies were single center-based, and one study was multiple center-based. Three studies28,30,32 reported the informed consent from the included patients, and four studies28–30,32 reported the approval of the ethics committee of their respective hospitals. All the studies mentioned the duration of follow-up and exhibited low follow-up bias due to the intact data. One study 29 described the methods for the handling of missing data and intention-to-treat analyses.
Primary outcomes
The results of the meta-analysis comparing VP and PPS + VP are listed in Table 2.
Results of meta-analysis from comparison of vertebroplasty vs. posterior pedicle screw combined with vertebroplasty.

df: degrees of freedom; CI: confidence interval; VP: vertebroplasty, PPS: posterior pedicle screw; WMD/OR: weighted mean difference/odds ratio; AVH: anterior vertebral height.
Statistically significant results are shown in bold.
Odds ratio.
Surgical outcomes
The time of operation, blood loss, and hospital stay were used to analyze the surgical outcomes. The operation time and blood loss were recorded in seven studies,26–29,31,32,34 whereas the time of hospital stay was recorded in five studies.26–28,32,34 VP was identified to be superior to PPS + VP in terms of operation time (WMD: −83.22, 95% CI: −97.70 to −68.73, p < 0.05; Figure 2), blood loss (WMD: −158.65; 95% CI: −219.99 to −97.31; p < 0.05; Figure 3), and hospital stay (WMD: −5.64; 95% CI: −7.36 to −3.92; p < 0.05; Figure 4).

Forest plot and meta-analysis of operation time. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
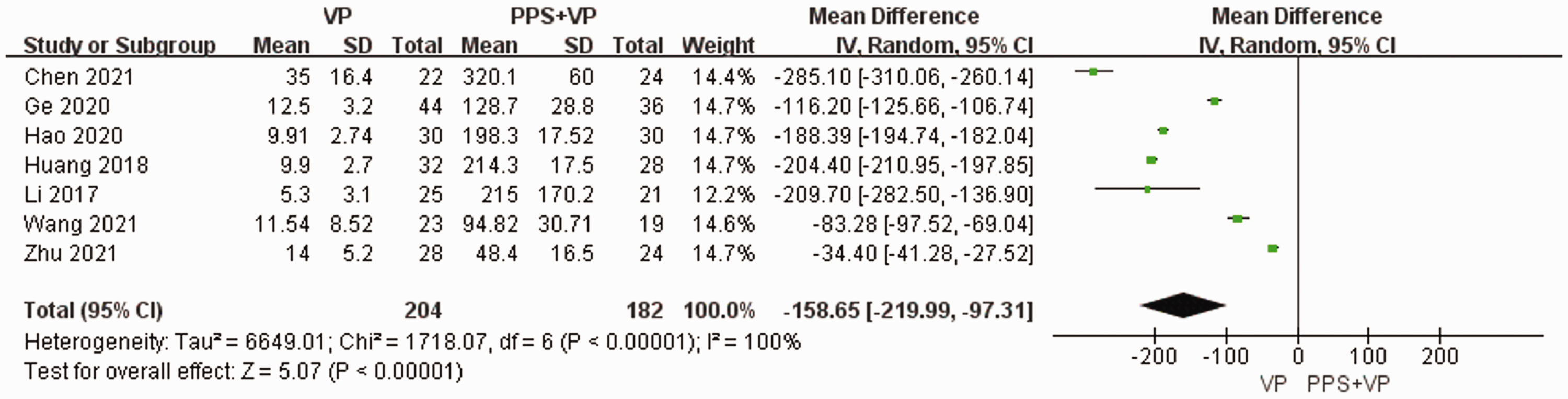
Forest plot and meta-analysis of blood loss. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.

Forest plot and meta-analysis of length of hospital stay. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
Radiographic measurements
Radiographic measurements were recorded before and after surgery using Cobb’s angle and AVH. The changes in Cobb’s angle after operation were reported in all eight studies, two studies27,32 reported the changes after 1 year of operation, and seven studies26,28–32,34 reported the changes at the final follow-up. The changes in the relative AVH after operation and at final follow-up were reported in four studies.26,31,32,34 The pooled data of the eight studies were analyzed and showed no significant differences in Cobb’s angle between the VP and PPS + VP groups in 864 cases (WMD: 1.28; 95% CI: −0.21 to 2.78; p > 0.05), as shown in Figure 5. The comparison of relative AVH also showed no statistically significant differences (WMD: 2.98; 95% CI, −4.15 to 10.11; p > 0.05), as shown in Figure 6.

Forest plot and meta-analysis of postoperative Cobb’s angle. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.

Forest plot and meta-analysis of postoperative relative anterior vertebral height. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
Adverse events
Seven studies26–30,32,34 reported the leakage of cement as an adverse event in both procedures. The data obtained through these studies were pooled to assess the leakage in 367 patients and showed no significant differences between the VP and PPS + VP groups (13.2% and 8.5%; OR: 1.67; 95% CI: 0.86–3.24; p < 0.05), as shown in Figure 7. Five studies in the PPS + VP group27–30,32 reported wound infection. However, there was no difference between the VP and PPS + VP groups, as no incidents of wound infection were reported in the VP group (0% and 4.88%; OR: 0.28; 95% CI: 0.07–1.1.5; p > 0.05), as shown in Figure 8.
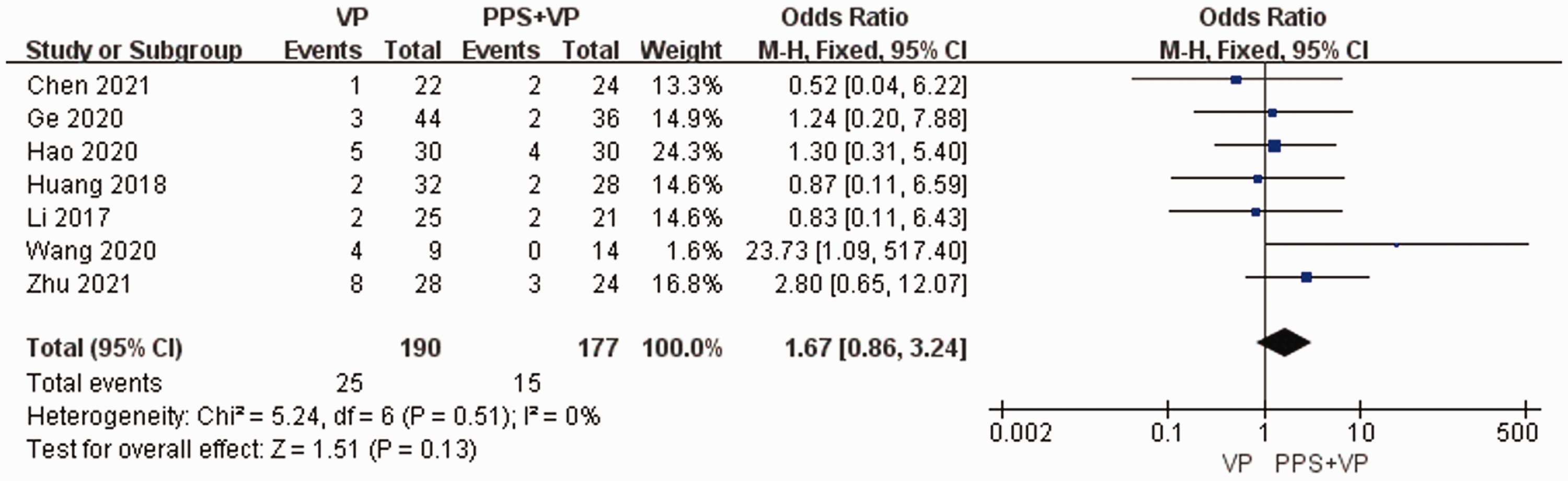
Forest plot and meta-analysis of bone cement leakage. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.

Forest plot and meta-analysis of wound infection. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
Secondary outcomes
Postoperative pain
Postoperative pain was evaluated in eight studies using VAS at different time points, including postoperative, 1-year postoperative, and final follow-up. The data were pooled and analyzed, showing no significant difference in the VAS scores of the VP and PPS + VP groups (WMD: −0.40; 95% CI, −0.99 to 0.19; p > 0.05), as shown in Figure 9.

Forest plot and meta-analysis of postoperative pain VAS score. PPS: posterior pedicle screw; CI: confidence interval; VAS: visual analog scale; VP: vertebroplasty.
Postoperative function
The postoperative function was assessed in all the studies using ODI at different time points, including postoperative, 1-year postoperative, and final follow-up. The analysis of the pooled data also revealed no significant difference in the ODI scores of VP and PPS + VP groups (WMD: −0.54; 95% CI, −2.44 to 1.36; p > 0.05), as shown in Figure 10.

Forest plot and meta-analysis of postoperative function score. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
Subgroup analysis
Subgroup analysis was performed to decrease the statistical heterogeneity and improve the comparability of studies according to the implantation of screws in the diseased vertebra. Due to the limitation of the available data, the postoperative Cobb’s angle between the diseased vertebra with cement fixation studies and diseased vertebra with cement and screw fixation studies was compared, which showed no significant differences in the subgroup analysis (WMD: 1.26; 95% CI, −0.76 to 3.28; p > 0.05), as shown in Figure 11.

Forest plot and meta-analysis of the results of subgroup analysis. PPS: posterior pedicle screw; CI: confidence interval; VP: vertebroplasty.
Publication bias
Figure 12 shows a funnel plot of the studies included in this meta-analysis, which reported the postoperative Cobb’s angle. Half of the included studies lied inside the 95% CIs with near-even distribution around the vertical, which indicated an obvious publication bias.

Publication bias of the included studies. WMD: weighted mean difference; SE: standard error.
Discussion
This meta-analysis represents the largest comparative evidence synthesis to date regarding surgical interventions for stage III KD without neurological deficits. Although the overall quality of the included studies was limited, our findings demonstrated that both VP and PPS + VP yield comparable long-term radiographic and functional outcomes.
VP confers significant advantages in perioperative efficiency, including reduced operative time, diminished intraoperative blood loss, and shorter hospitalization. However, Cobb’s angle, relative AVH, cement leakage, wound infection, postoperative pain, and postoperative function showed no differences between the VP and PPS + VP groups. Considering the different technical features of VP and PPS + VP, the surgeon will choose what they are good at. Therefore, there is a lack of effective comparison between VP and PPS + VP. The limitation of the meta-analysis is fewer studies and cases.
According to Li’s three-stage principle of KD, stage III causes neurological symptoms. However, most of the patients at stage III had no neurological deficits, which might be related to the extent of the posterior vertebral rupture or larger spinal canal. The differences in the mode of cement leakage in KD from the acute osteoporotic vertebral compression fracture (OVCF) under PVP operation might be due to other factors. 35 Jun et al. 27 also reported that the distribution of cement in KD was closely diffused to the superior and inferior endplates but showed lumpy distribution in the OVCF.
There were no differences in the results of postoperative pain and function during the 1-year follow-up. However, the VP group displayed better surgical outcomes and shorter hospital stay. In addition, VP could relieve pain more effectively from 1 to 7 days postsurgery. This suggested that VP and posterior fixation were effective and safe for the treatment of stage III KD without neurological deficits.
Furthermore, the correction of local kyphosis and anterior height of the vertebral body showed no differences between the two groups during the 1-year follow-up. We found that KD is a disease of nonunion fracture with stiff bone at the edge of the crack, which can limit the restoration of the kyphosis of the vertebral body.12,36 In addition, restricted postoperative bracing and regular antiosteoporosis treatment could maintain the curvature of the spine. 37
Wound infection did not occur in the 132 patients with VP. However, among the 123 patients with posterior fixation, 6 cases of wound infection were observed. It was suggested that wound infection resulting from longer operation time and greater blood loss could increase the length of hospital stay; however, this could not be compared between the two groups.
In the duration selected for the literature search in the meta-analysis, two studies with fewer patients were also identified. Zhan et al. 14 and Lu et al. 16 conducted meta-analyses of three to four studies and reported that the VP and PPS + VP groups gained similar clinical outcomes. Both these studies showed that there was no statistical significance in the VAS score, ODI score, and local vertebral Cobb’s angle between the VP and PPS + VP groups. Zhan et al. 14 also reported that indices such as operation time, intraoperative blood loss, and perioperative complications were better in the VP group, similar to the results in the present study. The latest study reported retrospectively that PKP had better early clinical outcomes, increased fractured vertebral height, decreased blood loss, and less surgical trauma compared with pedicle subtraction osteotomy combined with long-segment fixation in stage III KD without neurological symptoms. 38
Currently, prospective studies on KD treatment are insufficient. The results of the literature search mainly included reviews and case reports on the pathogenesis of KD. Studies focusing on the diagnosis and treatment of KD are limited. Therefore, the updated meta-analysis of the studies is indispensable for clinicians.
Post-study registration may have introduced bias to our results and is a limitation of this study.
Conclusions
VP and PPS + VP are viable options for treating stage III KD without neurological deficits. Although both yield similar long-term radiographic and functional outcomes, VP offers advantages in operative efficiency and reduced surgical trauma. Higher-quality prospective studies are warranted to validate these findings.
Footnotes
Acknowledgements
I would also like to thank my tutors Xiaolin Shi for his valuable guidance throughout my studies.
Authors contributions
X.S. and B.T. designed the study. S.H. and Y.Y. conducted literature searches. B.T., S.H., and H.Z. performed analyses. All authors reviewed the manuscript.
Data availability statement
Data were extracted from published studies. The systematic data and images were created by Review Manager 5.4.1.
Declaration of conflicting interests
All authors declared that they have no conflict of interest.
Funding
This study was supported by Zhejiang Province Natural Science Foundation (LBY22H270005), National Natural Science Foundation of China (82204829), Zhejiang Provincial Chinese Medical Foundation (2025ZR130, 2024ZR090), Zhejiang Provincial Medical Foundation (2025KY097), and CACM Young Talent Program (CACM-2023-QNRC2-B27).