
Abstract
Study Design
Retrospective Cohort Study
Objective
Cervical radiculopathy meeting operative criteria has traditionally been managed using anterior cervical discectomy and fusion (ACDF). However, cervical disc arthroplasty (CDA) and posterior cervical foraminotomy (PCF) are also reasonable options. This study aimed to assess differences in postoperative outcomes among patients undergoing multi-level ACDF, CDA, or PCF comparing medical/surgical complications and healthcare utilization parameters.
Methods
Patients who underwent multi-level ACDF, CDA, or PCF between 2012 and 2019 were identified from the American College of Surgeons National Surgical Quality Improvement Project (ACS-NSQIP) database. Patients were stratified based on procedure type and propensity score matched to resolve baseline differences. ANOVA was performed to identify differences in medical complications, surgical complications, and healthcare utilization metrics.
Results
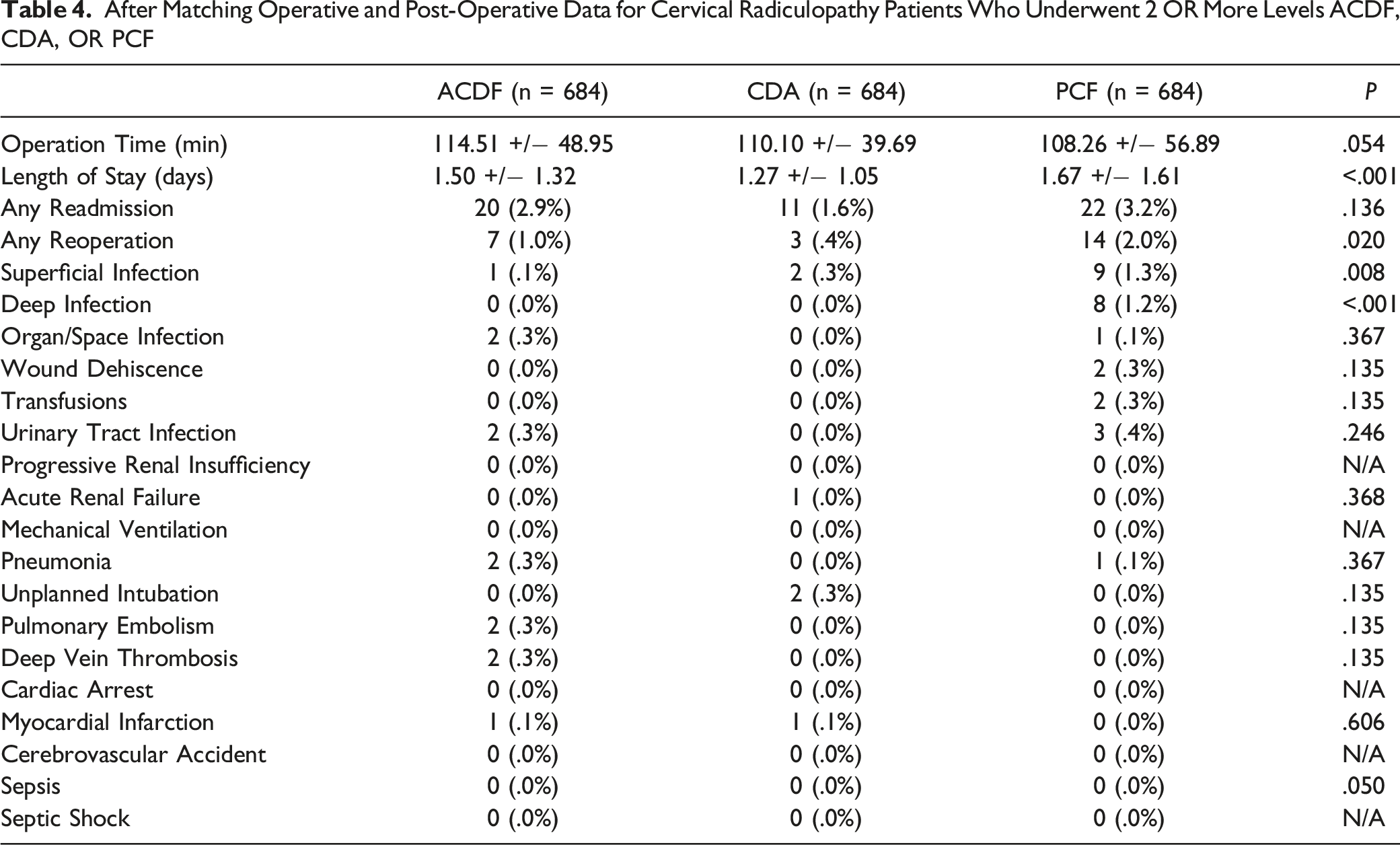
A total of 31 344 patients who underwent an eligible procedure were identified (ACDF: n = 28 089, CDA: n = 1748, PCF: n = 1507), and 684 patients remained in each group following propensity score matching. Patients undergoing multi-level PCF were found to experience longer lengths of hospital stay (PCF: 1.67 ± 1.61 days, ACDF: 1.50 ± 1.32 days, CDA: 1.27 ± 1.05 days, P < .001), higher rates of reoperation (PCF: 3.2%, ACDF: 1.0%, CDA: .4%, P = .020), superficial infection (PCF: 1.3%, ACDF: .3%, CDA: .1%, P = .008) and deep infection (PCF: 1.2%, ACDF: 0%, CDA: 0%, P < .001). There were no outcome differences between multi-level ACDF and CDA.
Conclusions
Patients undergoing multi-level PCF were at increased risk for longer hospital stay, re-operation, and infection relative to those undergoing ACDF and CDA. Future research should aim to uncover the precise mechanisms underlying these complications, as well as analyze long term outcomes.
Level of Evidence
III
Keywords
Introduction
Cervical radiculopathy is a debilitating condition characterized by upper arm pain accompanied by sensory deficits in about 85%, reflex deficits in about 71%, and motor deficits in 68% of patients.1,2 The most common causes of such presentations are cervical disc herniations leading to posterolateral or intra-foraminal impingement, and diminished disc height with degenerative changes to the uncovertebral joints secondary to cervical spondylosis.3,4
For ∼75% of patients, cervical radiculopathy is self-limiting and the symptoms resolve over time without intervention. 5,6 However, non-operative management is often trialed in an effort to provide pain relief and alleviate patient symptoms. 7 Conservative treatment modalities that have demonstrated some efficacy include pharmacologic therapies such as nonsteroidal anti-inflammatory drugs, neck immobilization using cervical collar, mechanical traction, physical therapy, and steroid injections.8‐12 Despite these measures, up to one third of patients continue to experience symptoms after 6 weeks of treatment and are considered for referral to a spine surgeon. 13
There are several surgical procedures available to address cervical radiculopathy, which can be broadly categorized into anterior and posterior approaches. The anterior surgeries include anterior cervical discectomy and fusion (ACDF) and cervical disc arthroplasty (CDA), while the posterior procedure is a posterior cervical foraminotomy (PCF). 14 ACDF is one of the most commonly performed spine surgeries and is considered to be the standard surgical treatment for cervical disc disease 15 . Although it offers excellent outcomes, ACDF is associated with perioperative complications such as dysphagia and hematoma formation, decreased range of motion, nonunion and delayed complications such as adjacent segment disease. 16 In contrast, CDA is a relatively novel procedure that gained popularity in the U.S. market within the last 2 decades, with the purported benefits of maintaining physiologic motion and minimizing adjacent segment degeneration. 17 The surgical technique is essentially identical to ACDF with the principal exception being the implantation of a disc arthroplasty device instead of an intervertebral graft following discectomy. 18 While typically asymptomatic, CDA can result in complications such as heterotopic ossification and osteolysis, increasing the risk for spinal segment fusion and device subsidence, respectively. 19 Lastly, PCF involves enlarging the neuro-foramen by removing a portion of the involved facet joint with/without disc removal in order to decompress the nerve root causing the patient’s symptoms. 20 Similar to the aforementioned surgical approaches, PCF also offers favorable outcomes for the treatment of cervical radiculopathy, reducing common risks associated with the anterior approach such as implant-related complications and dysphagia. 21 However, it also requires posterior muscle dissection which can lead to increased intra-operative bleeding, pain, and wound/nerve complications.
While outcomes from ACDF, CDA, and PCF have been studied for single-level procedures, 22 there is a paucity of literature comparing them in the context of multi-level procedures. To offer patients, the most optimal treatment option for multi-segment cervical radiculopathy, it is important to identify any significant disparities among these surgical approaches. To this end, this study aims to determine differences in postoperative outcomes among patients undergoing multi-level ACDF, CDA, and PCF by evaluating: (1) 30-day postoperative medical complications; (2) surgical complications and (3) healthcare utilization parameters (reoperation, readmission, and length of stay).
Methods
Study Design and Data Sources
Cervical radiculopathy patients who underwent multi-level ACDF, CDA, or PCF (defined as >1 level) between January 1st, 2012 and December 31st, 2019 were retrospectively identified from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. Created and validated by surgeons, ACS-NSQIP currently serves as a leading national quality improvement database that provides incredible utility to researchers due to its data collection from patients who undergo major surgeries in over 500 centers in North America. 23 The ACS-NSQIP database encompasses risk-adjusted and case-mixed adjusted information for important patient variables, including patient demographics (sex, age, race, and body mass index (BMI)), American Society of Anesthesiologists (ASA) physical status class, existing comorbidities, and complications spanning up to 30 days post-operation. ACS-NSQIP captures major complications including any readmissions or reoperations, superficial surgical site infections (SSI) that involve only the skin or subcutaneous tissue of the incision, deep SSI (involving fascial and muscle layers), organ/space infections (infections involving any anatomy that was opened or manipulated during surgery apart from incision), sepsis (systemic inflammatory response syndrome with documented infection) and septic shock (sepsis with documented organ and/or circulatory dysfunction), renal complications, cardiac dysfunction, and wound dehiscence. 24 Standard definitions of complications are established by the central NSQIP to ensure uniform adherence among cooperating surgical centers. This study did not necessitate Institutional Review Board (IRB) approval nor individual consent as any patient data was presented in a de-identified manner through a publicly available dataset.
Study Population
Patients were identified as having undergone multi-level ACDF, CDA or PCF by the current procedural terminology (CPT) codes. Multi-level ACDF cases were identified with CPT code 22 551 with the addition of a single or multiple 22 552 codes and with CPT code 22 554 with the addition of a single or multiple 22 585 codes. Multi-level CDA cases were identified with CPT code 22 856 with the addition of a single or multiple 22 858 codes. Multi-level PCF cases were identified with CPT code 63 020 with the addition of a single or multiple 63 035 codes. Following the identification of patients who underwent multi-level ACDF, CDA, or PCF, exclusion criteria were applied. Additional procedure CPT codes identified patients who underwent only a singular level of fusion, those who underwent fusion from a posterior approach, and those who received additional concomitant spinal procedures, such as vertebral corpectomy, decompression, or removal of an artificial disc. These patients were subsequently excluded.
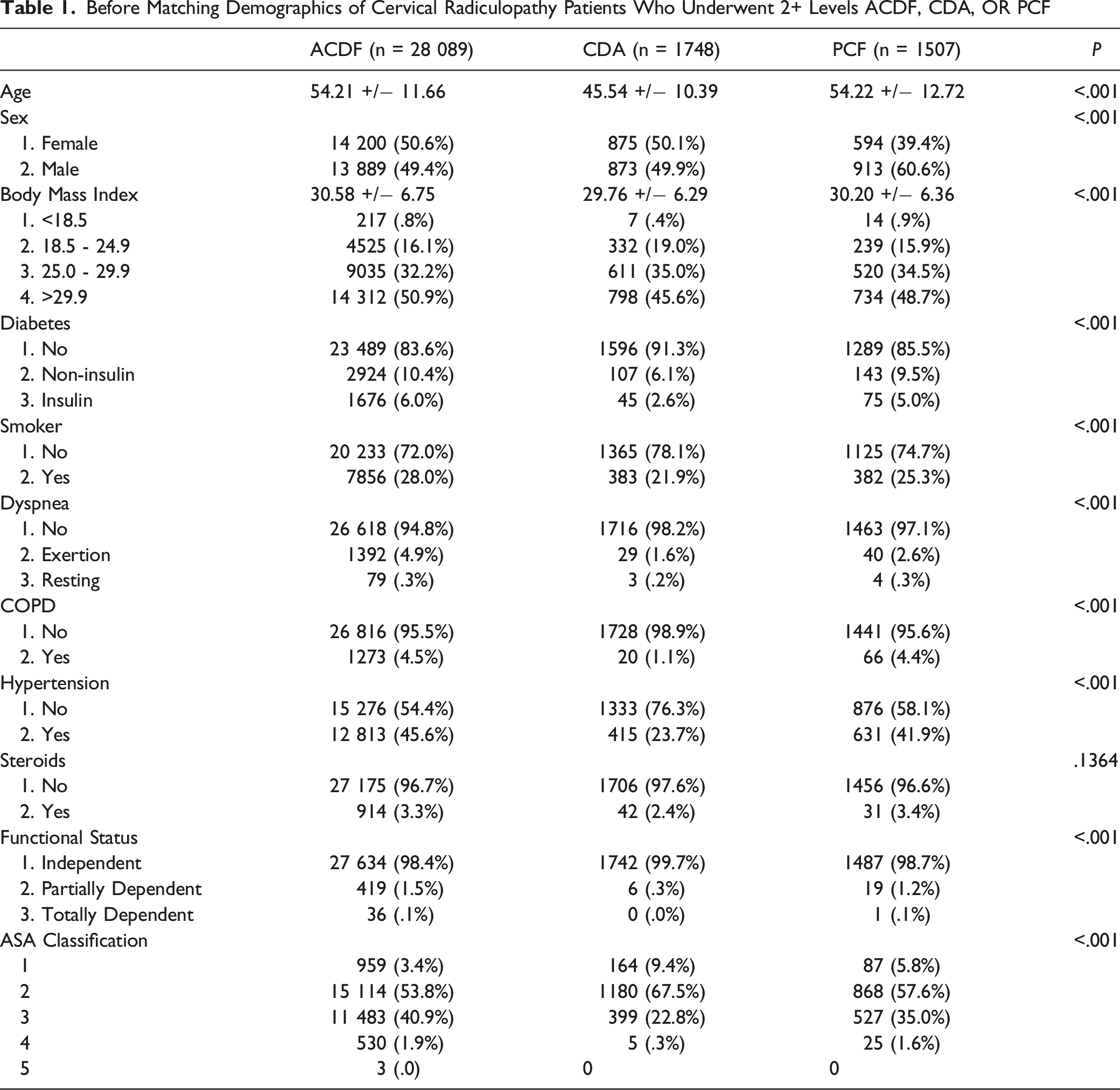
Before Matching Demographics of Cervical Radiculopathy Patients Who Underwent 2+ Levels ACDF, CDA, OR PCF
Outcomes of Interest
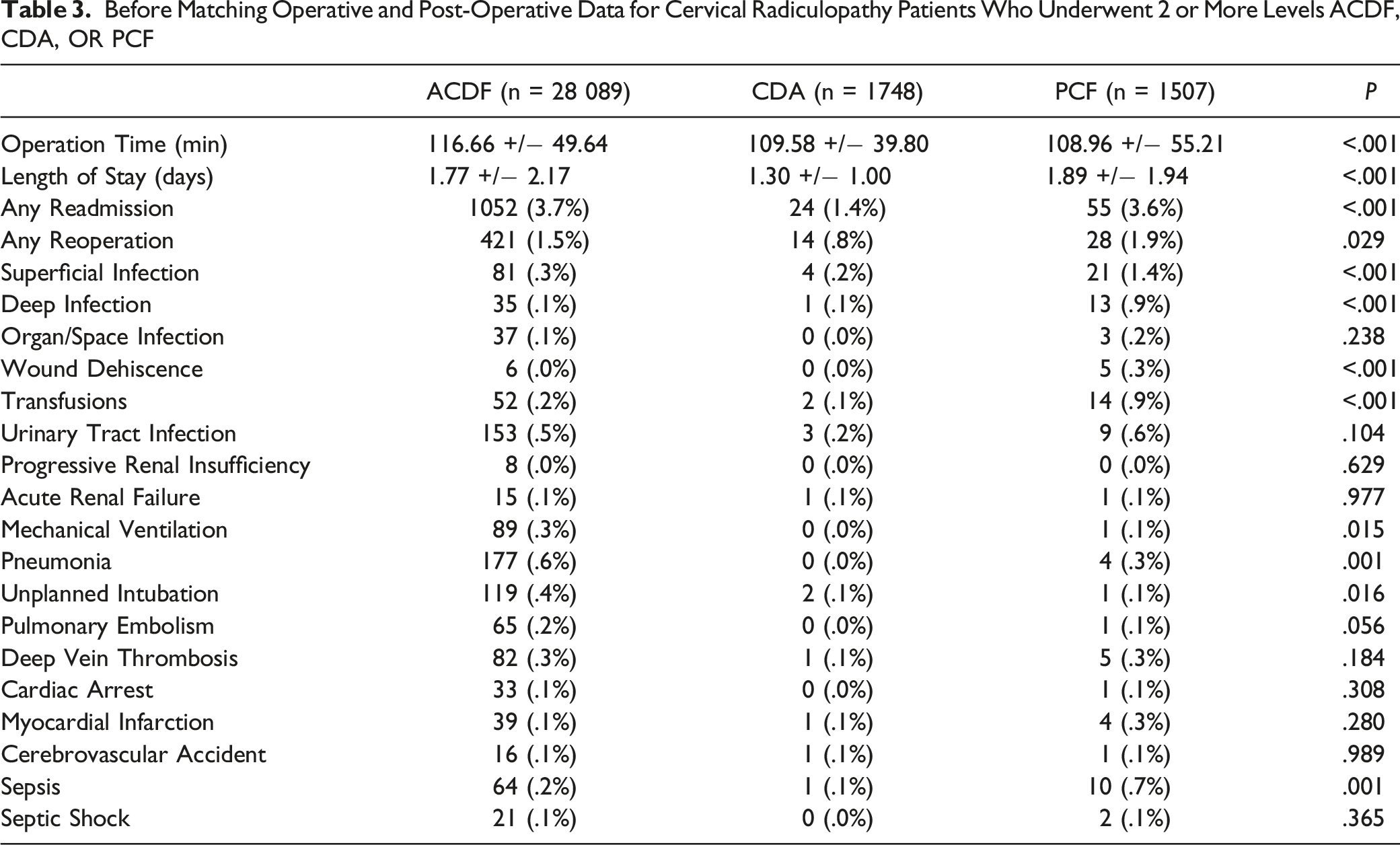
Primary outcomes of interest were: operative time, length of stay, 30-day readmission and 30-day re-operation. Secondary outcomes of interest were 30-day postoperative complications, which included superficial infection, deep infection, organ/space infection, wound dehiscence, as well as renal complications (urinary tract infections, progressive renal insufficiency, acute renal failure), cardiopulmonary complications (use of mechanical ventilation >48 hours postoperatively, pneumonia, unplanned intubation, cardiac arrest, myocardial infarction), thromboembolic complications (postoperative transfusions, pulmonary embolism (PE), deep vein thrombosis (DVT), cerebrovascular accident (CVA) and septic complications (sepsis, septic shock).
Statistical Analysis
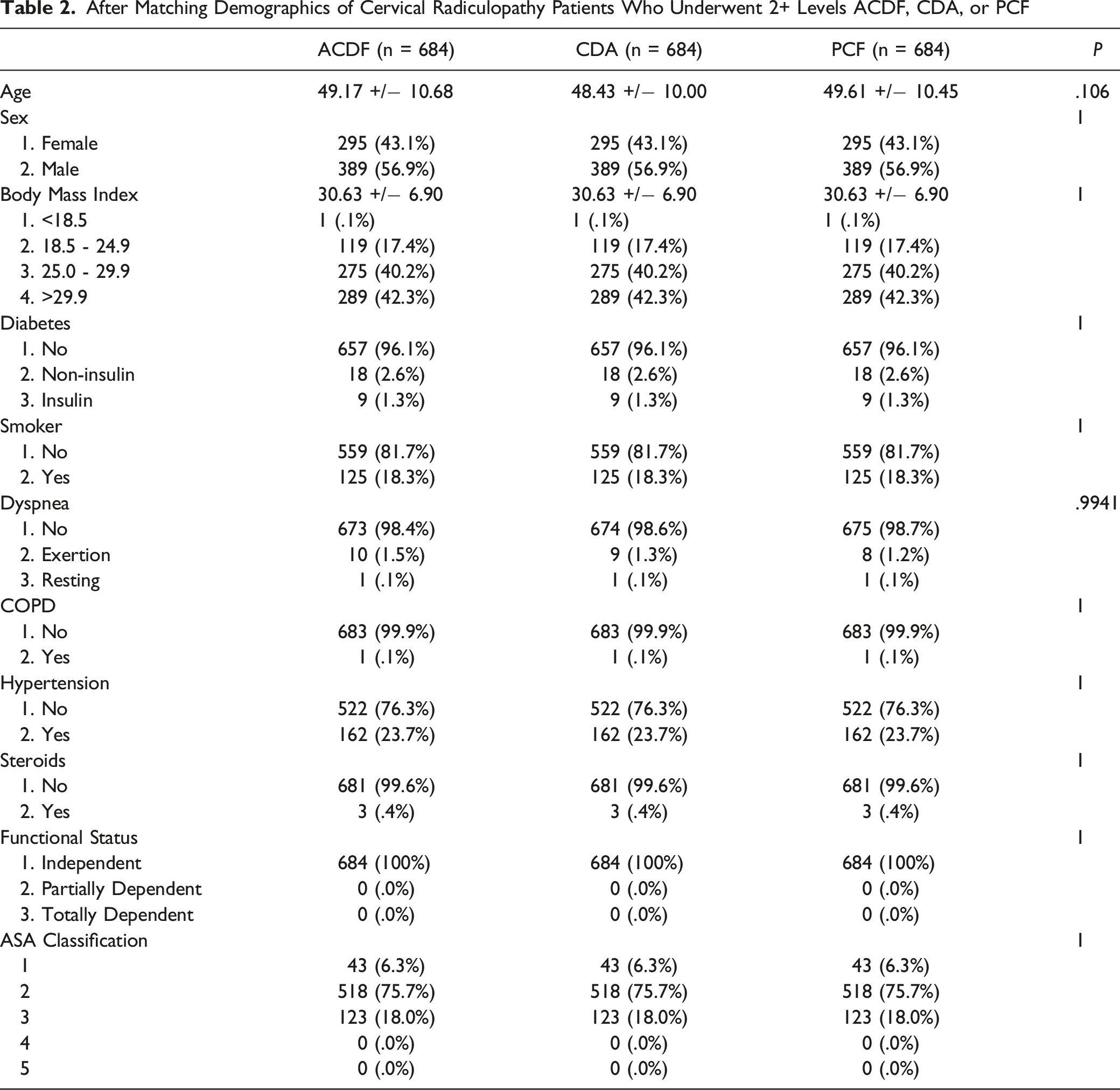
Univariate analysis identified the distribution of patient demographics, existing comorbidities and patient outcomes among patients undergoing multi-level ACDF, CDA, or PCF. Statistically significant differences in baseline patient demographics, existing comorbidities, steroid use, functional status and ASA classification were resolved using propensity score matching (1:1:1). The propensity score-matching process included the following variables: age, sex, BMI category, diabetes, smoking status, and the presence of chronic obstructive pulmonary disease (COPD), hypertension, overall functional status, and ASA classification. The propensity score-matching process was then followed by a comparison of outcomes. As appropriate, Fisher’s exact test and Chi-square tests were utilized to analyze differences in the counts and percentages of categorical variables, such as readmissions, reoperations, and medical/surgical complications. Analysis of variance (ANOVA) was utilized to analyze differences in the means ± standard deviations (SDs) of continuous variables, such as operative time and length of stay. All tests were 2 tailed with an alpha level of .05 (significance level at P < .05).
Results
A total of 31 344 cervical radiculopathy patients undergoing multi-level ACDF, CDA or PCD were identified (See Table 1). Of these, 28 089 patients were identified to have undergone multi-level ACDF, with a mean (±SD) age of 54.21 (±11.66) years, a BMI of 30.58 (±6.75), and a slight female majority (50.6%). 1748 patients were identified to have undergone multi-level CDA, with a mean (±SD) age of 45.54 (±10.39) years, a BMI of 29.76 (±6.29), and a slight female majority (50.1%). 1507 patients were identified to have undergone multi-level PCF, with a mean (±SD) age of 54.22 (±12.72) years, a BMI of 30.20 (±6.36), and a male majority (60.6%). Univariate analysis showed significant differences among the age, sex, and BMI of the cohorts, as well as among existing comorbidities, including diabetes (P < .001), smoking status (P < .001), dyspnea (P < .001), COPD (P < .001), hypertension (P < .001), functional status (P < .001), and ASA classification (P < .001), but not steroid use (P = .1364).
After Matching Demographics of Cervical Radiculopathy Patients Who Underwent 2+ Levels ACDF, CDA, or PCF
Before Matching Operative and Post-Operative Data for Cervical Radiculopathy Patients Who Underwent 2 or More Levels ACDF, CDA, OR PCF
After Matching Operative and Post-Operative Data for Cervical Radiculopathy Patients Who Underwent 2 OR More Levels ACDF, CDA, OR PCF
Discussion
To our knowledge, this is the first study investigating and comparing outcomes among the 3 most common multi-level surgeries performed for symptomatic cervical radiculopathy. Our initial hypothesis was that there would be no difference in postoperative outcomes among the ACDF, CDA, and PCF cohorts, as corroborated by a meta-analysis on the topic. 25 However, the analysis conducted in this retrospective cohort study demonstrated that compared to ACDF and CDA, multi-segment PCF is associated with significantly prolonged length of hospital stay and increased rates of reoperation and infection including superficial skin infection and deep infection. This is consistent with the findings reported by Ng et al., who detected similar trends in reoperation and infection following single-level PCF. 22 Contrary to their additional discovery of differences in operative time based on procedure type, however, we found no other significant differences in outcomes.
The limitations of the present study are primarily 2-fold: stemming from its design as a retrospective cohort study and from its use of the data available through the ACS-NSQIP database. First, our study results rely on data available in the NSQIP database, identifying patients through Current Procedural Terminology codes regardless of their diagnosis. To this end, coding errors can be present, although NSQIP has been well-established for its robust and consistent auditing resulting in <1.8% inter-rater variability. Second, the CPT codes available were binary in nature (single-level and multi-level) and were unable to distinguish between different multi-level procedures. This is important to consider when ACDF involving multiple levels have high rates of pseudarthrosis and increased nonunion rates, and varies based on the number of fused segments (eg 0-10% for single-level and up to 50% for 3-level constructs) 15 . To this end, single-institution studies may allow for more precise discernment of multi-level procedures, although they would likely lack the statistical power of this study. In addition, as a retrospective cohort study, the study lacks completely randomized data, and is therefore subject to selection bias. In other words, without randomization, this study has poor control over pre-existing covariates and confounders, which makes it a possibility that patient demographics among the multi-level ACDF, CDA, and PCF groups had differed at baseline. To address this limitation, propensity score matching identified patients from each of the 3 groups with similar baseline characteristics. This was confirmed with a P-value greater than .05 in patient demographics or comorbidities among the patients in each group, suggesting there were no statistically significant differences in baseline characteristics. Secondly, the study’s use of the ACS-NSQIP database allowed analysis of outcomes within a 30-day period after operation but lacked outcomes that were followed over a longer term. Furthermore, the study was limited only to the complications defined and made available by NSQIP, which lacked information on complications more specific to surgery on the cervical spine, as detailed earlier, such as dysphagia and adjacent segment disease. 16 Future research efforts may aim to analyze longer-term complications as well as complications specific to cervical spine surgery.
In recent years, various studies have begun exploring outcomes following PCF. One such study by Witiw et al. utilized a propensity score matching methodology like this paper to compare PCF and ACDF and also found a higher infection rate in the PCF cohort. 26 Another retrospective cohort study found posterior approaches in general to be a risk factor for superficial and deep surgical site infections, as consistent with the findings in this paper. The authors surmised that this might be due to the relatively decreased vascularity and lymphatic drainage of the posterior spine compared to the anterior spine, which may diminish the clearance of incidental bacterial contamination. 27 This elevated incidence can be attributed to a variety of characteristics, including procedural factors such as instrumented surgeries, multi-level surgeries, open exposures, lack of local antibiotic usage, increased estimated blood loss, and longer surgeries. One study suggested that the extensive muscle dissection required for posterior approaches might be to blame, which can de-vascularize paraspinal muscles and predispose the patient to a deep infection. Retractors used in posterior spinal surgery can also compress the paraspinal musculature and cause ischemia-induced infections. 28 Some patient characteristics such as diabetes, history of postoperative wound infection, obesity, smoking, radiation exposure, and cancer have also been found to be associated with increased infection rates, although the precise mechanism and contribution of these factors have yet to be uncovered.27‐30 While many of these risk factors are not modifiable, taking judicious measures such as preparation of the surgical site and drapes with alcohol foam, and/or considering insertion of an additional suprafascial drain in obese patients or placement of powdered antibiotic such as vancomycin into the wound in addition to administering standard perioperative intravenous antibiotics may decrease the incidence in patients predisposed to infections. 31
Contrary to our findings on the other hand, 2 studies comparing patients who underwent ACDF or PCF found no differences in reoperation rates at the index level within 2 years following the initial surgery.32,33 While intraoperative complications such as hematomas, infections, and cerebrospinal fluid leaks secondary to dural puncture can necessitate a revision procedure, the most common indications are recurrent disc herniation in PCF and inadequate decompression. 29 Patients could also be counseled to reduce or avoid spinal loading in the immediate postoperative period in order to minimize the risk of disc reherniation. 29
Fortunately, there has been an increasing amount of literature published that has delved into the comparison between PCF and other procedure types, as well as between open and minimally invasive approaches. Although these have been exclusive to single level spinal surgeries, they offer novel perspectives that surgeons can benefit from when risk-stratifying their patients. For instance, the advent and increasing utilization of minimally invasive and endoscopic approaches, especially in the context of PCF, can reduce the incidence of both infection and reoperation in the future by minimizing tissue exposure, contamination, and disruption.25,35 In addition, open posterior exposures are associated with neck and shoulder pain/spasm, 36 and using minimally invasive approaches can therefore minimize these undesirable outcomes. 37 On the other hand, it has quite a few limitations and potential complications that must be considered prior to patient selection. When performed without arthrodesis for example, there is concern for iatrogenic cervical spine instability following facetectomy. 39 Similar to the findings in the current study, Lin et al. also found a significantly increased rate of reoperation in their PCF cohort relative to the ACDF and CDA cohorts. 40 Lastly, a paper published shortly prior to the submission of the current study reported shorter operative time for minimally invasive PCF and greater estimated blood loss with no postoperative improvement in arm pain for open PCF patients compared to ACDF and CDA groups. 41 Thus, all things considered including the pre-existing literature as well as the findings from this study, a cautious risk-benefit analysis should be carried out prior to choosing PCF for patients, and when possible, minimally invasive approaches should be utilized.
Conclusion
In conclusion, the present study suggests that patients with cervical radiculopathy who underwent multi-level PCF experience longer length of stay, higher rates of reoperation as well as higher rates of superficial and deep infection 30 days after operation than those who underwent treatment via multi-level ACDF or multi-level CDA. As this study now adds to the literature that suggests an association between the posterior approach and higher rates of infection, future efforts should be made to elucidate the precise mechanism behind this phenomenon. Additionally, future studies should analyze postoperative complications on a longer time scale as well as complications specific to those most associated with surgery of the cervical spine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.