
Abstract
Study Design
Randomized controlled trial with minimum of 5-years follow-up.
Objective
The purpose of this study is to evaluate the peri- and postoperative complications rates, ectopic bone migration, and reoperation rates, and secondly evaluate the 5-year patient reported outcomes (PROs), in patients treated with decompression and non-instrumented posterolateral fusion with ABM/P-15 or allograft.
Methods
Patients with degenerative spondylolisthesis were enrolled in a Randomized Clinical Trial and randomized 1:1 to either ABM/P-15 or allograft bone. Patient Reported Outcomes were collected at 5-year follow-up, and patients were invited to a clinical follow-up including a computed tomography scan (CT) to evaluate signs of osteolysis, ectopic bone formation, and bone migration.
Results
Of 101 subjects enrolled in the primary study, 83 patients were available for the 5-year follow-up. We found a statistically significant difference in back pain and Oswestry Disability Index between groups. Fifty-eight patients agreed to participate in the CT study. Sixty percentage in the ABM/P-15 group vs 30% in the allograft group was classified as fused (P = .037). There were no differences in complications, reoperation-, or infection rates between the 2 groups. We found 2 patients with migration of graft material. Both patients were asymptomatic at minimum 5-year follow-up.
Conclusion
Our study indicated that complication rates are no higher in patients treated with ABM/P-15 than allograft. We found significantly higher fusion rates in the AMB/P-15 group than in the allograft group, and patients in the ABM/P-15 group reported less back pain and lower disability score at 5-year follow-up.
Introduction
Lumbar spinal stenosis (LSS) is one of the most common indications for spinal surgery. 1 Surgical spinal decompression is offered to regain walking capacity and reduce pain. When instability is present, or in cases where postoperative instability is expected, concomitant fusion is often considered. 2 In order to minimize surgical stress, as well as reduce the risk of reoperations due to risk of implant failure, 3 many Scandinavian countries chose to treat elderly patients who require lumbar posterolateral fusion with uninstrumented fusion. 4
To obtain fusion, autologous bone remains “The Gold Standard” graft since the first reports in 1911 on the use of autologous bone grafts by Fred Albee 5 treating Pott’s disease and Russell Hibbs 6 treating progressive spinal deformity. However, limitations posed by autologous bone grafts include increased surgical time and donor site morbidity.7,8 In addition, in elderly patients, the quantity and quality of locally harvested autologous bone obtained from the decompression is often inadequate to obtain fusion. 9
In an attempt to avoid peri- and postoperative complications in harvesting autologous donor bone, nonstructural allograft has been used in Scandinavia for decades. However, harvesting and utilizing allograft is labor intensive as it has to be processed, and the donor must be screened at least twice for potential contagious diseases.10,11 Another drawback is the numerous reports on inferior fusion rates compared to autograft. 12 For these reasons, a readily available bone graft extender, enhancer or substitute would be a welcome addition to the available options for the spine surgeons performing fusions. Giannoudis et al 13 emphasizes the importance of stability, osteoinductive, osteogenetic, and osteoconductive properties in the fusion site to generate optimal conditions for achieving a solid fusion.
There have been several attempts to develop an efficient and safe substitute. Recombinant BMP protein was approved in 2002 for surgery of the anterior lumbar spine to promote bone fusion. 14 Since then, several products have been made available and tested in humans. In 2008 Wong et al 15 published a case series of 5 patients where they suspected the use of recombinant BMP as the cause of ectopic bone formation in the spinal canal. A year later in 2009 the first reports of increased in wound-related complications were published. 16 More recent papers describe complications and cancer risk after usage of recombinant BMP-2.17,18
An anorganic bovine-derived hydroxyapatite matrix combined with a synthetic 15 amino acid residue (ABM/P-15, Peptide Enhanced Bone Graft), has been introduced as a substitute for autologous bone graft. Several studies have been published reporting similar or superior outcomes compared to autograft.19-22
The purpose of this study is to evaluate the peri- and postoperative complications rates, formation of ectopic bone, osteolysis, and reoperation rates, and secondly evaluate the 5-year patient reported outcomes (PROs), in patients treated with spinal decompression and non-instrumented posterolateral intertransverse fusion with ABM/P-15 or allograft.
Materials and Methods
This is a minimum 5-year follow-up study on a previously published prospective, randomized, double-blind single center trial in patients undergoing lumbar spinal decompression and non-instrumented posterolateral fusion randomized 1:1 comparing ABM/P-15 (I-Factor ™, Cerapedics, USA) to allograft bone both mixed with local harvested autograft. 22
The study was conducted according to the Consolidated Standard of Reporting of Reporting, the CONSORT guidelines 23 and Danish legislation. Prior to inclusion each patient gave written informed consent for research use and publication of their data. Approval from the Scientific Ethics Committee of the Region of Southern Denmark (S-20120012) was obtained with an extension in 2019. The primary study was registered in ClinicalTrials.gov June 13, 2012 (NCT01618435). Data use approval was acquired from the Danish Data Protection Agency ref nr: 16/1586.
From March 2012 to April 2013, 101 patients aged 60+ with LSS and concomitant degenerative spondylolisthesis (DS) referred to a major Spine Centre were screened for inclusion in a randomized trial. Criterion for inclusion was a slip of at least 3 mm on standing X-rays, regardless of instability on flexion extension X-rays. Standard of care in our institution for treating DS in patients above 60 years was uninstrumented fusion, due to an expected risk of implant failure due to poor bone stock. Patients found eligible were randomized in blocks of 20 with 10 ABM/P-15 and 10 allograft patients in each block. Assignment of the treatment arm was made just prior to surgery in the surgical theater after the patient was anesthetized, allowing both the primary investigator and patient to remain blinded to the treatment arm. Inclusion and exclusion criteria have previous been reported as well as 1- and 2-year patient reported follow-data. 22
Surgical Technique
All patients were decompressed at the affected levels with either a laminotomy or a laminectomy. The fusion bed in posterolateral gutters were prepared by decorticating the transverse processes and packing with surgical sponges to ensure hemostasis prior to grafting procedure. In the allograft group the harvested autograft from the decompression was mixed with morselized fresh frozen femoral head yielding a total of 30 g for each fusion level. In the ABM/P-15 group, the volume of the autologous bone was measured in cc and mixed with an equal amount of ABM/P-15 putty (5 cc or 10 cc). Postoperatively, patients were braced for 3 months with a soft brace.
Patient Reported Outcomes
Demographic data regarding age, height, weight, gender, and co-morbidity were collected from questionnaires prior to surgery. PROs include Visual Analogue Scale (VAS) 24 for back- and leg pain, Oswestry Disability Index (ODI)25,26 and EuroQoL-5D (EQ-5D), 27 PROs were collected pre-operatively on the day of admission and 60 months after surgery by mail.
Complications and Reoperations
Because of concerns with prior bone graft substitutes inducing an inflammatory reaction, data on wound problems, drain output, and infections were collected. Wound complications during admission were obtained from patient records, with “change of bandage due to secretion” as a proxy to account for excessive seroma formation. At 3 months follow-up, patients were asked if they had wound problems that required treatment with antibiotics and/or surgery.
All participating patients were invited to a clinical visit, minimum 5 years after surgery, including an interview on any surgical spine procedures since the index surgery. Together with the patient, the clinical charts from the time of surgery were revisited to record any signs of postoperative infection.
A fine-cut CT-scan (.7 mm) of the entire lumbar spine including Th12 and S1 were performed including 3-D reconstructions. Two trained spine surgeons, unaware of which arm the patients were enrolled in, evaluated the CT-scans independently. A continuous osseous bridge extending the intertransverse space was defined as fusion.
Fusion status was decided, if at least one intertransverse space was fused. Status of fusion on each intertransverse space was determined as described by Carreon et al, 28 in case of disagreement, CT-films were reviewed together, and a consensus was reached. Signs of graft migration, ectopic bone formation in the paraspinal soft tissue, or osteolytic zones displayed as erosions of either endplates or vertebral bodies were recorded.
Statistics
All data collected were entered into an EXCEL spreadsheet and exported to STATA for statistical analysis. Statistical analysis was done using STATA 15 (StataCorp., College Station, TX). Normally distributed continuous variables were compared using unpaired t-tests and Wilcoxon–Mann–Whitney and Kruskal Wallis test were used for non-normally distributed continuous variables. Chi2 or Fisher’s exact test was used to determine differences in proportions between the 2 treatment groups. Significance level was set at P-value <.05.
Results
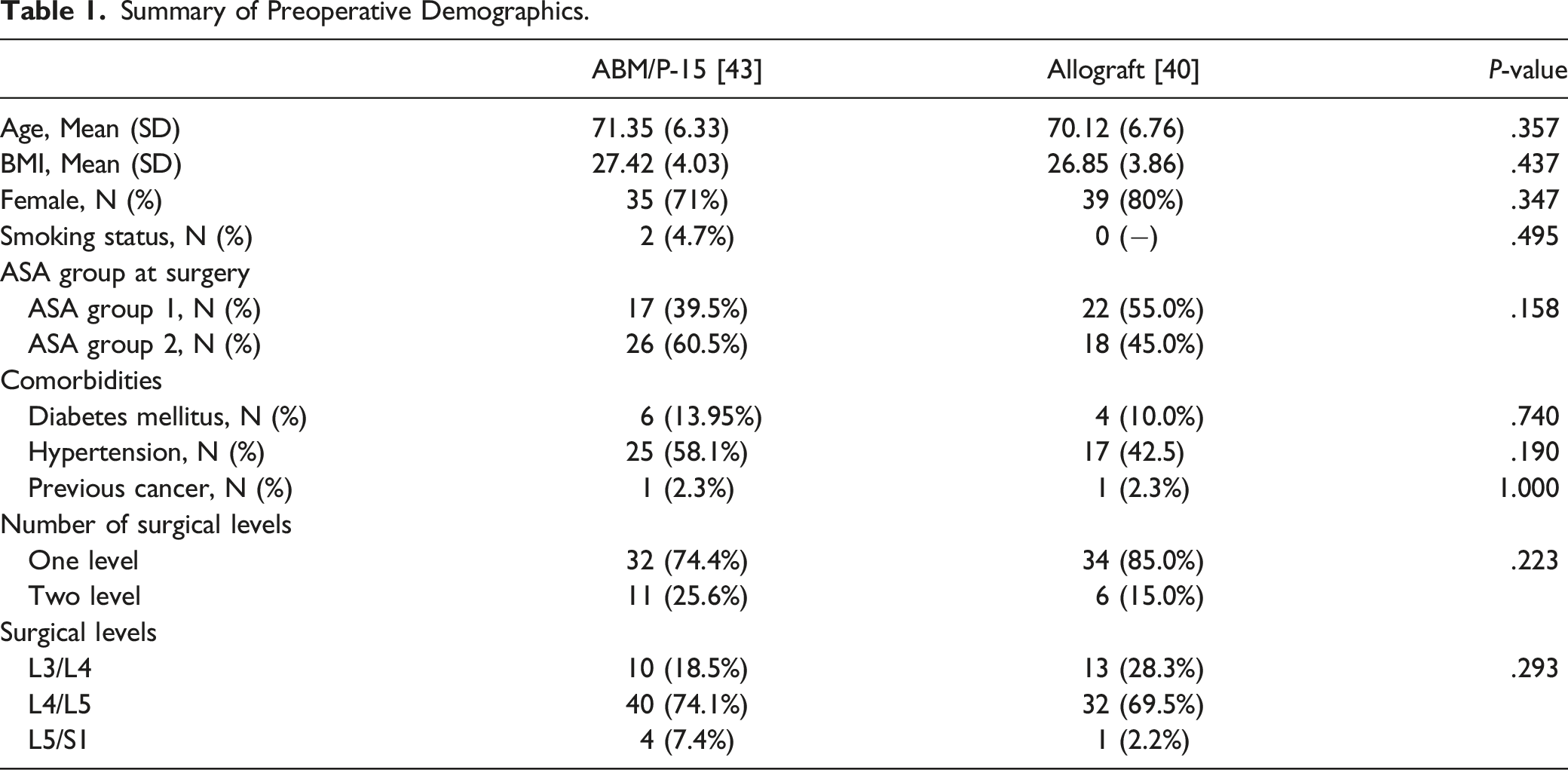
Summary of Preoperative Demographics.
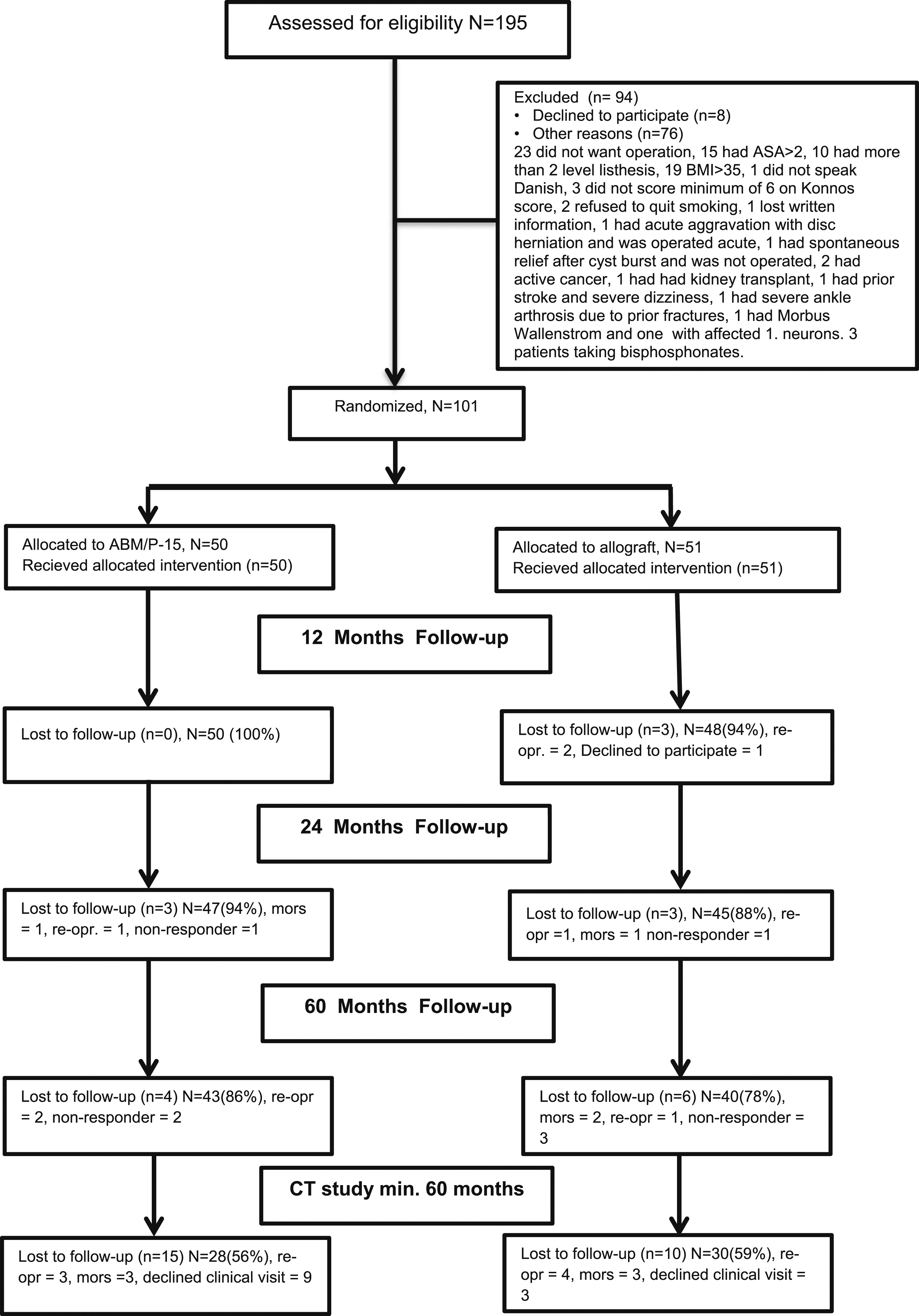
Enrollment, randomization, and follow-up.
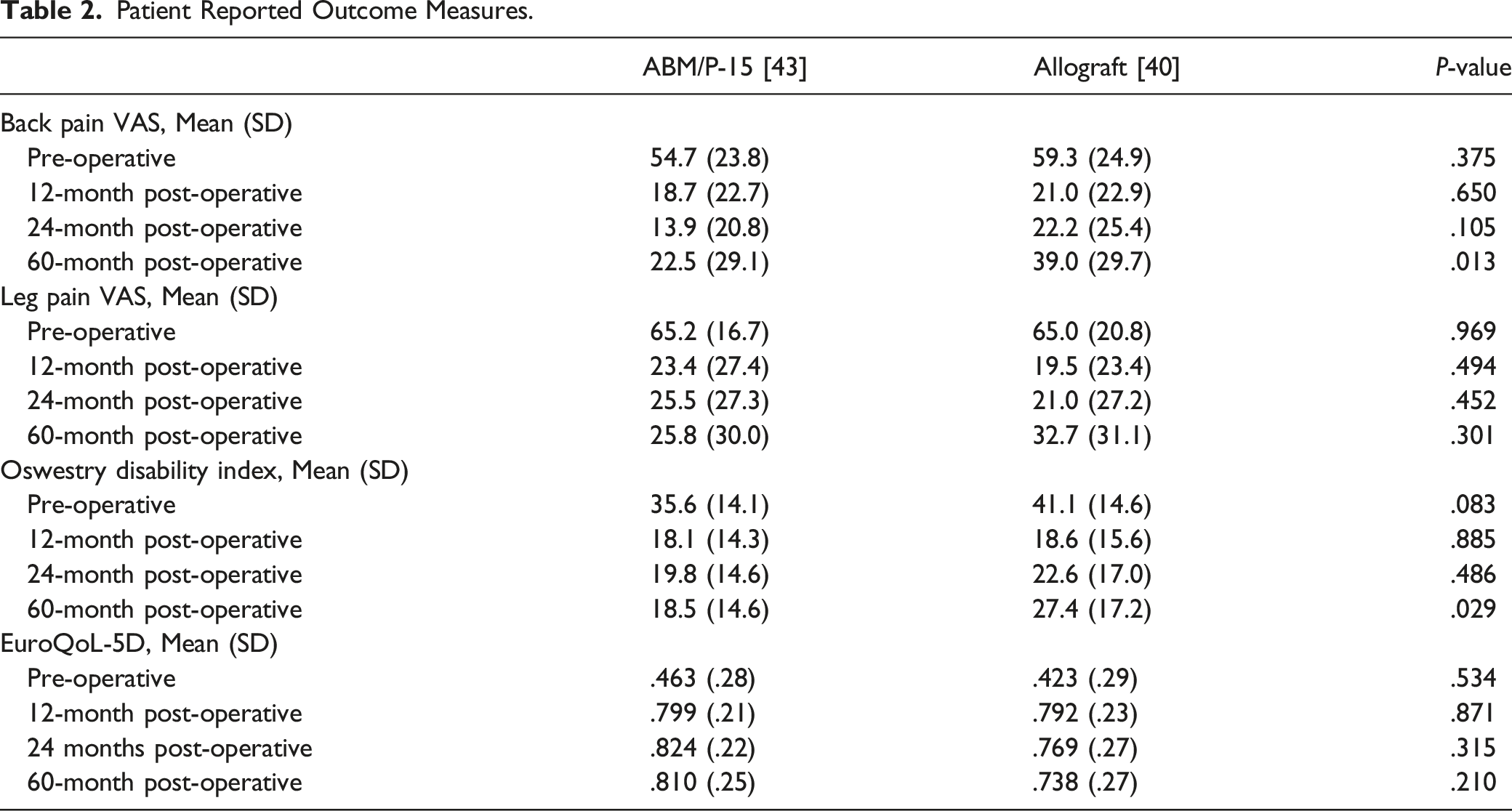
Patient Reported Outcome Measures.
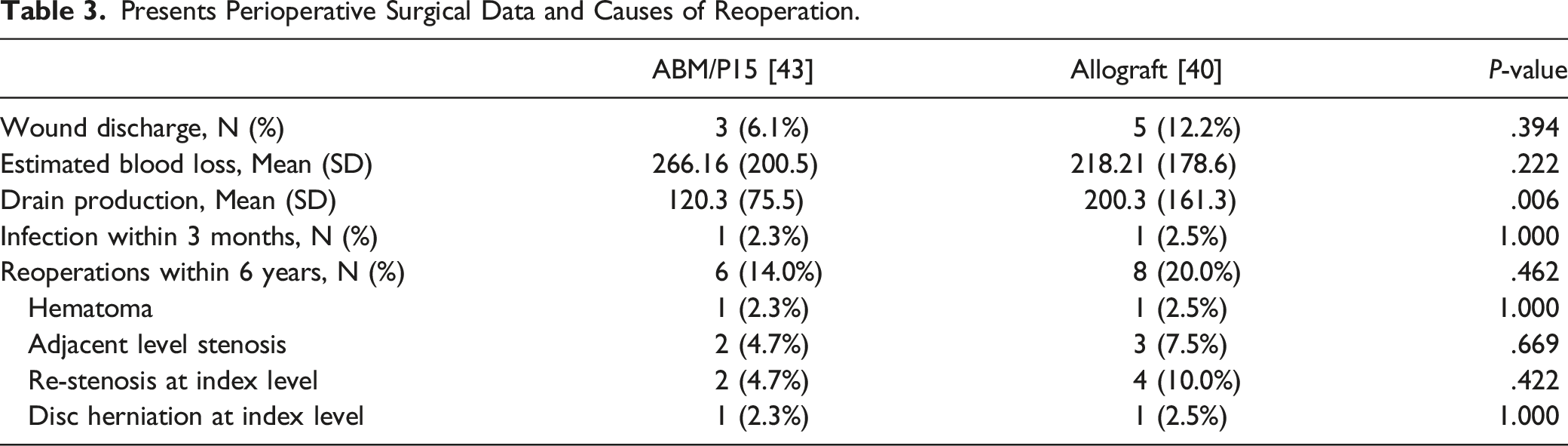
Presents Perioperative Surgical Data and Causes of Reoperation.
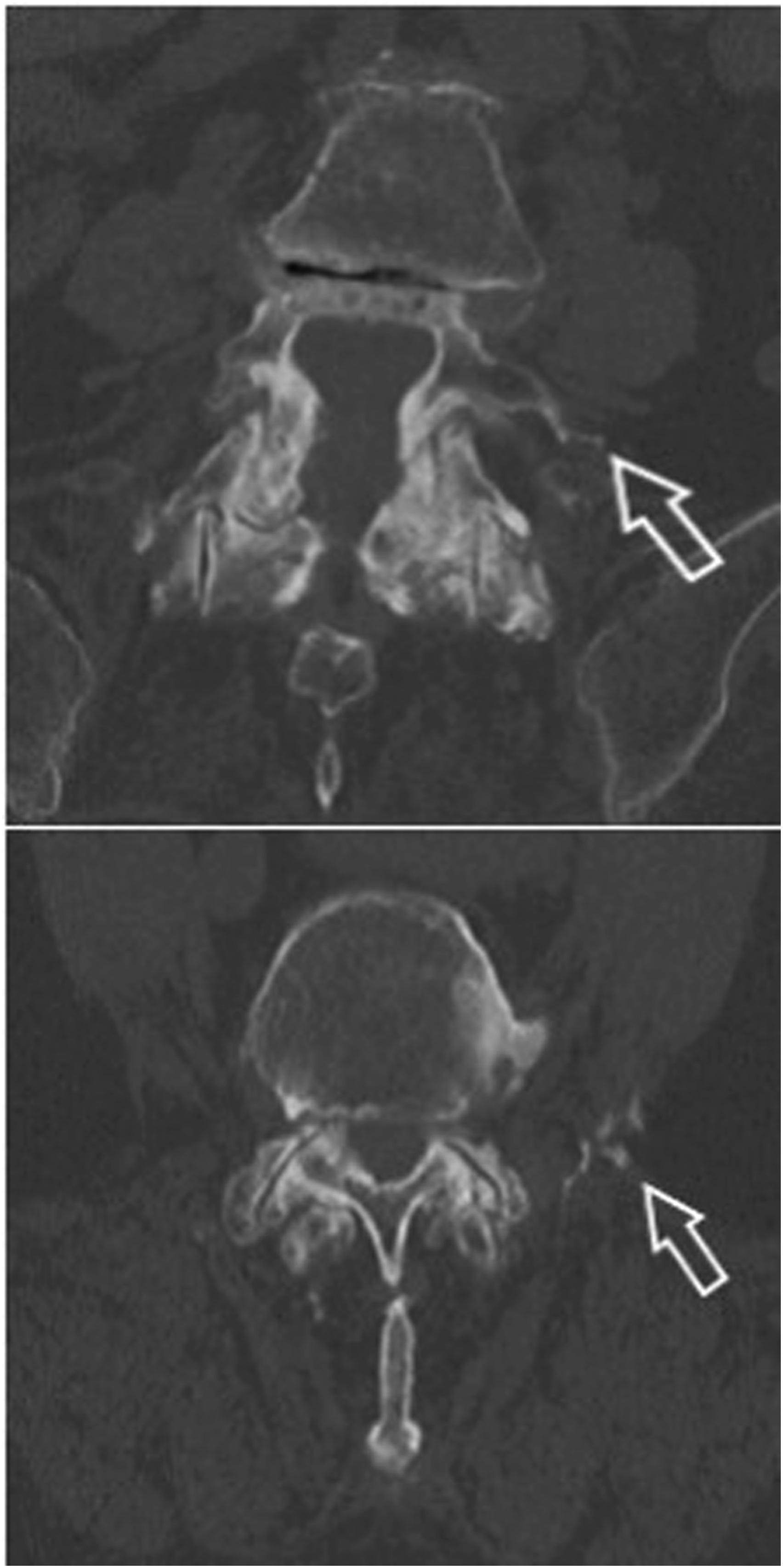
Evaluating the CT-scans performed minimum 5 years postoperative there were no changes in fusion status between the 1 and 5 year CT-scans. No signs of ectopic bone formation or osteolysis were recorded, but 2 patients from the ABM/P-15 group had signs of graft migration. One patient had peri operative bleeding of more than 800 mL and the graft had migrated causing an ossified hematoma which had leaked along the drain (Figure 2). The second patient had bone migration into the psoas from the left transverse process (Figure 3, Table 4). Axial CT scan at 5 year post surgery of patient nr. 1 with calcified hematoma, arrows mark hematoma and calcified drain canal. Upper: Axial CT image obtained at 5 year post surgery. Arrow points to bone migrated anterior at tip of the transverse process. Lower: Coronal CT image at same level. Arrow points to migrated bone caudal to the transverse process. Evaluation of CT-cans 6 years Postoperative.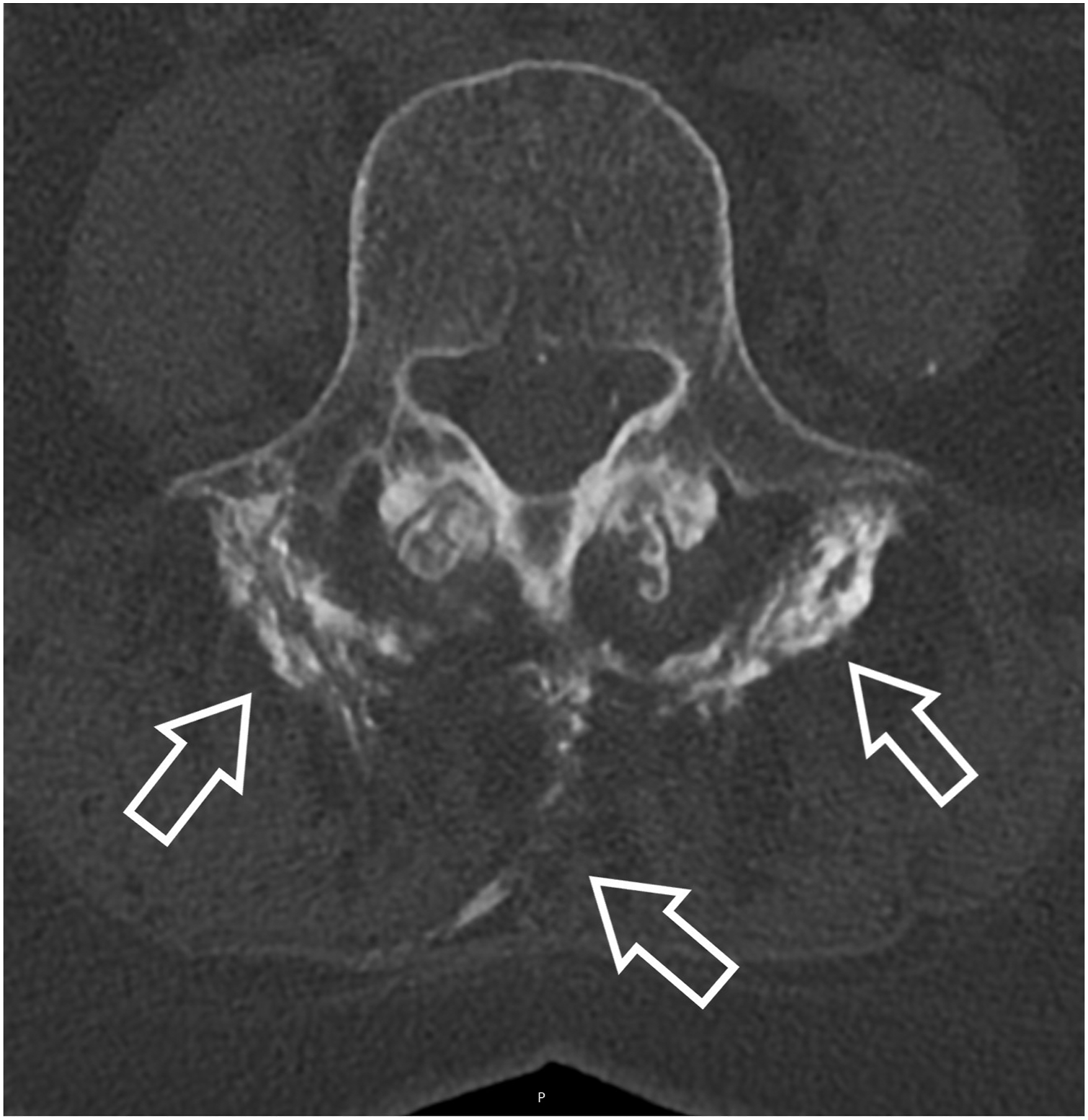

Discussion
In this study, we found no difference in wound complications, reoperation rates and perioperative complications between the 2 treatment groups using data from a randomized controlled trial comparing posterolateral fusion with ABM/P-15 to allograft, with more than 5 years follow-up. Solid fusion was noted on CT-scans in 57% of the ABM/P-15 cohort and 30% in the Allograft cohort.
As previously reported, both cohorts showed statistically and clinically relevant improvement from baseline to 2-year follow-up. Although we found significantly lower backpain in the ABM/P-15 group, both groups had worse backpain at 60 months follow-up than at 24 months follow-up. There was a deterioration in all PROs in the allograft group from 24 month to 60 month follow-up. The deterioration in PROs in both groups may be due to lack of achieving a solid fusion in both groups, predominantly in the allograft group compared to the ABM/P-15 group.
Axelsen et al 29 found extensive caudal or ventral migration of the graft material at all levels treated with ABM/P-15 in a sheep model, most likely due to lack of structural support of the graft material. In 8 of the 22 levels treated, fusion was achieved in spite of the migration of graft material. When evaluating migration rates and fusion in a human model, we found 1 case of ventral migration of bone, at the tip of the cranial transverse process, in the ABM/P-15 group, and none in the allograft group.
Oxborrow and Sundarapandian 30 reported a case of heterotopic ossification, in an 8 year old patient after posterolateral thoracolumbar fusion and excessive seroma discharge from the wound drain. In our study, we had 1 patient with excessive per operative bleeding where a subcutaneous calcified hematoma was found on CT-scans at both 1 and 5 year follow-up. The calcified hematoma had no impact on the clinical outcome of the patient at either follow-up point and the patient had no wound complications or signs of infection postoperatively.
A concern was raised with regards to wound complications due to excessive seroma formation in patients treated with ABM/P-15. 31 In a letter to the editor A. Demetriades and H. Shekhar reports the use of ABM/P-15 involve 3% of wound complications, including excessive seroma formation, wound discharge and subsequent infection. 31 Requiring treatment with antibiotics. As reported, we found excessive wound discharge in 6 patients (11.8%) in the allograft group, and in 3 patients in the ABM/P-15 group (6%). We found a significantly greater drain output in the allograft group, compared to the ABM/P-15 group, although this is probably not clinically relevant. In our cohort we found that one patient in each group received antibiotics as treatment for superficial infection within the first 3 months after surgery, none required revision surgery due to deep infection.
There are weaknesses to this study. Despite an overall high 5-year follow-up rate there were variations in the response rates to the different outcome items. Of the 83 patients available for follow-up, only 70% agreed to undergo an additional CT-scan. Further both the patients and authors of the present study were un-blinded after the 2-year follow-up data was processed. Standing full-length radiographs were not available to assess the impact of sagittal parameters on PROs and re-operation rates. The strengths of the study were the RCT design, a very homogenous group of participants with regards to the diagnosis, all patients having LSS due to degenerative lumbar spondylolisthesis and no difference in baseline demographics.
In conclusion, our study indicated that complication rates are no higher in patients treated with ABM/P-15 than allograft. We found a statistically significant difference in backpain and disability between the groups at minimum 5-year follow-up and a higher fusion rate in the AMB/P-15 group. Although we found a tendency towards higher reoperation rates in patients who had allograft, compared to ABM/P-15 at 6 years after surgery, this difference was not statistically significant. In the 2 cases with minor bone migration, none were symptomatic at any follow-up points.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The institution has recieved a research grant from Cerapedics, USA.