
Abstract
Study design
retrospective review.
Objective
Enhanced Recovery After Surgery (ERAS) is a multidisciplinary set of evidence-based interventions to reduce morbidity and accelerate postoperative recovery. Complex spine surgery carries high risks of perioperative blood loss, blood transfusion, and suboptimal fluid states. This study evaluates the efficacy of a perioperative fluid and blood management component comprised of a restrictive transfusion policy, goal directed fluid management, number of tranexamic acid (TXA) utilization, and autologous blood transfusion within our ERAS protocol for complex spine surgery.
Methods
A retrospective review compared patients undergoing elective complex spine surgery prior to and following implementation of an ERAS protocol with intraoperative blood and fluid management. Outcomes included incidence of blood transfusion, estimated blood loss, intraoperative crystalloids administered, frequency of intraoperative TXA utilized, incidence of patients extubated within the operating room (OR), intensive care unit (ICU) admission, and hospital length of stay.
Results
Following implementation, the rate of blood transfusion decreased by 11.7%(P = .017) and average crystalloid infusion was reduced 680 mL per case(P < .001). Intraoperative blood loss decreased on average 342 mL per case(P = .001) and TXA use increased significantly by 25%(P < .001). Postoperative ICU admissions declined by 8.5%(P = .071); extubation within the OR increased by 13.3%(P = .005).
Conclusions
This protocol presents a unique perspective with the inclusion of an interdisciplinary and comprehensive blood and fluid management protocol as an integral part of our ERAS pathway for complex spine surgery. These results indicate that a standardized approach is associated with reduced rates of blood transfusion and optimized fluid states which was correlated with decreased postoperative ICU admissions.
Keywords
Introduction
Operations for spinal deformity and reconstruction are associated with increased levels of intraoperative blood loss, increased rates of blood transfusion, large fluid shifts, and increased intensive care unit (ICU) admissions compared to less complex spine surgeries1-3. ICU admissions after deformity operations are common and frequently attributed to fluid overload, postoperative anemia, and the need for postoperative vasopressor medications. High rates of perioperative blood transfusions are associated with increased postoperative risk of morbidity and mortality 4 . Glance et al showed patients undergoing general, vascular, or orthopedic surgery who received a blood transfusion have higher rates of pulmonary, septic, wound, and thromboembolic complications when compared to non-transfused patients 4 . For elective spine surgeries, even one unit of packed red blood cells (RBC) or whole blood was associated with longer hospital length of stay (LOS) and morbidity when controlling for preoperative hematocrit and comorbidities 5 . Similarly, this data has been corroborated in cardiac and gynecologic surgery where transfusion was found to carry a 16% increased hazard of infection, increased ischemic postoperative morbidity, mortality, cancer recurrence, hospital costs, and length of stay6-8.
Given the risks associated with blood transfusion and fluid imbalance, there is considerable interest in reducing the frequency of surgery-related transfusions and optimization of fluid management. Standardized perioperative Enhanced Recovery After Surgery (ERAS) protocols have demonstrated success across several specialties9-12. ERAS is an evidence-based protocol designed to improve post-operative outcomes while reducing perioperative morbidity and mortality. The ERAS protocol consists of multiple interdisciplinary interventions targeting high-risk populations and procedures designed to maximize patient outcomes through decreased length of stay, reduced postoperative complication rate, and optimized recovery. ERAS has been successfully adapted for spine surgery by multiple institutions with data demonstrating a reduction in ICU admissions, hospital length of stay (LOS), hospital costs, and intraoperative blood loss13-19. The implemented protocol aimed to unite key pillars of existing ERAS protocols for spine surgery such as pain management with a novel pillar comprised specifically of blood and fluid management.
Utilization of ERAS as a paradigm for blood and fluid management in other specialties correlated with decreased rates of transfusion, blood loss, LOS, complications, readmissions, and hospital costs1,20. Goal directed fluid therapy has been shown to reduce LOS and post-operative complications without increasing mortality in major elective surgery. In orthopedic surgery, goal directed fluid therapy increased hemodynamic stability and improved postoperative gastrointestinal function 21 . Therefore, to decrease associated risks with perioperative blood transfusions and fluid imbalances, an evidence-based fluid and blood management pathway was adopted as part of the ERAS protocol for elective spine surgeries. The protocol consists of pre-operative optimization of patients with anemia, intraoperative goal directed fluid therapy, use of tranexamic acid, and a restrictive transfusion policy.
This study aims to analyze the impact of incorporation of a perioperative blood and fluid management protocol within ERAS for elective complex spine surgery.
Methods
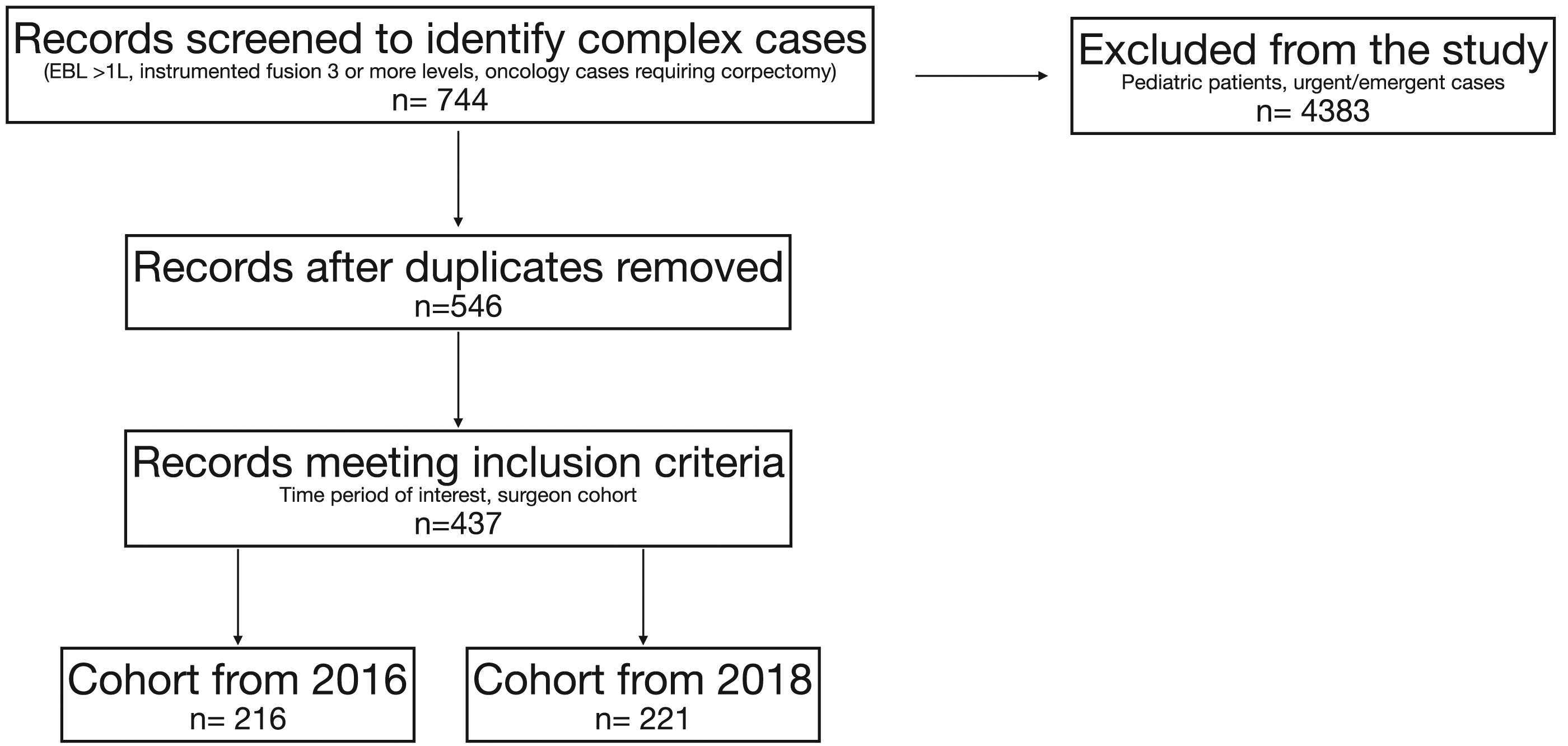
This is a retrospective cohort study of patients who underwent elective complex spine surgery from January 1, 2016 through December 31, 2018. These patients were identified by querying the electronic medical record (EMR) database for all surgical cases billed using a spine surgery Current Procedural Terminology (CPT) Code. The operative report for each case was reviewed and patients meeting the following criteria were included in final cohort: those with an expected blood loss >1000mL including pedicle subtraction osteotomy, oncology cases requiring corpectomy, and instrumented fusions of 3 or more levels (Figure 1). Cases performed by surgeons who were hired or retired during the period of interest were excluded from analysis. Additional exclusion criteria included pediatric cases (age < 18) and urgent/emergent cases (Figure 2). Each patient who met criteria was classified into one of two groups: (1) the “Before ERAS” group included patients that underwent surgery in the year prior to the initiation of our institutional ERAS protocol (January 1, 2016 through December 31, 2016), and (2) “After ERAS” group included patients that had surgery in the year following the initiation of our institutional ERAS protocol (January 1, 2018 through December 31, 2018). This study was deemed exempt from informed consent by institutional review board at the Cleveland Clinic Foundation (18-1030). Categories of spine surgeries based on complexity. Patient selection process.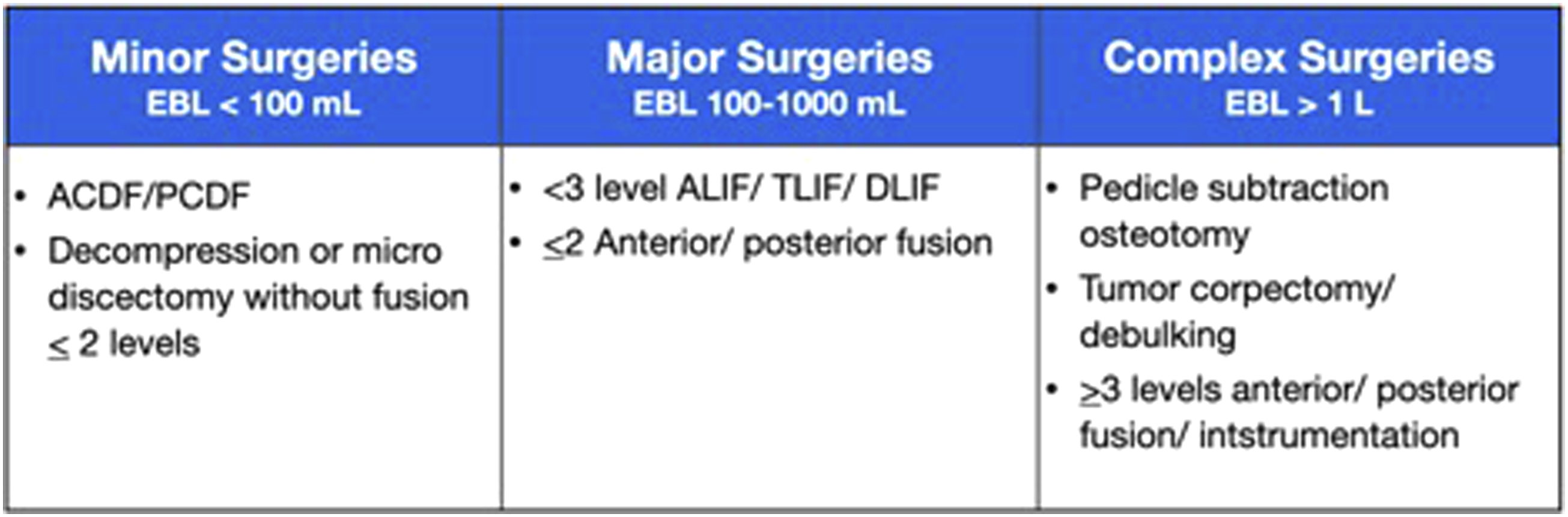
The primary outcome was defined as incidence of blood transfusion. Secondary outcomes included estimated blood loss, volume of intravenous crystalloids administered intraoperatively, incidence of intraoperative tranexamic acid (TXA) administration, incidence of patients extubated within the OR, ICU admission, hospital length of stay, and discharge disposition.
Additionally, a second analysis was performed of all patients undergoing spine surgery from 2016 to 2018. Outcomes analyzed included incidence of transfusion, utilization of cell saver, incidence of extubation within the OR, utilization of vasopressors, and incidence of ICU admission. This analysis was intended to trend all spine surgical cases from 2016 to 2018 (including both minor and major cases, Figure 1)
Patient Demographics
Patient age, sex, race, body mass index, medical comorbidities, location of surgery, and date of surgery were obtained by querying the EMR database. Manual chart review was performed to determine indications for surgery, type of surgery, levels of surgery, site of surgery (eg, cervical, thoracic, or lumbar), approach (eg, anterior vs posterior), and technique of fusion (eg, transforaminal interbody vs posterolateral etc.).
Statistical Analyses
Patient demographics and outcome variables were compared between the two groups using t-tests for independent samples and Mann-Whitney tests for normally and non-normally distributed variables, respectively. Categorical variables were compared using Pearson’s Chi-squared test. Study data were analyzed using R and R-Studio and the “tidyverse” package.
Protocol
The ERAS protocol for spine surgery was implemented in a phasic manner beginning in 2017 and fully adopted by 2018. The protocol focuses on preoperative optimization of risk factors such as smoking, diabetes, anemia, and BMI; intraoperative blood and fluid management, multimodal pain management and glycemic control; and postoperative early ambulation, pain management, and delirium prevention. Specifically, the multi-disciplinary blood and fluid management component consists of three main components: preoperative optimization, restrictive transfusion policy, and intraoperative goal directed fluid therapy (Figure 3). Blood and fluid management protocol.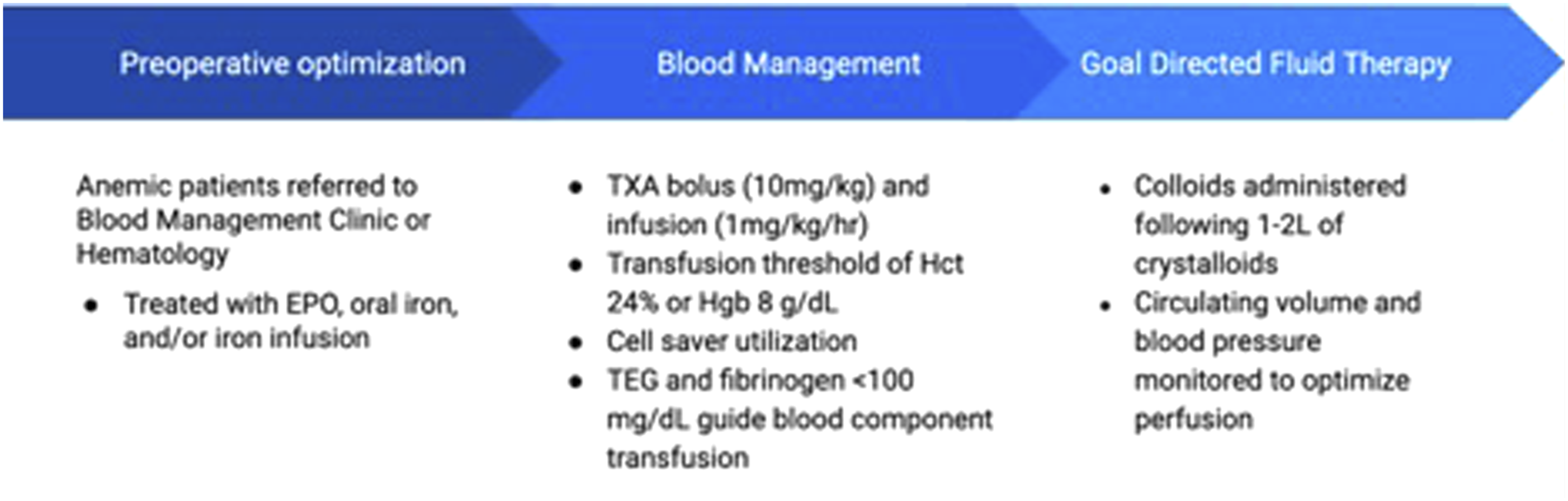
Preoperative
Preoperative optimization involves targeting high risk patients with anemia or hematopoietic deficiencies and providing early interventions in preparation for surgery. Patients scheduled to undergo major or complex elective spine surgery are screened and referred to the blood management clinic if they are found to be anemic. Available therapies target increasing the preoperative hemoglobin and hematocrit with a goal hemoglobin of 13g/dL. Patients are kept without food for at least 8 hours prior to surgery, however, are permitted to drink clear fluids until 2 hours prior to arrival at the hospital.
Blood Management Protocol
Tranexamic acid contraindications and complications.

The protocol follows a restrictive blood transfusion policy with a transfusion threshold for major and complex spine surgeries set at 24% hematocrit or 8g/dL hemoglobin. The use of cell salvage device is encouraged for all major and complex procedures, allowing blood loss to be centrifuged and transfused back to the patient (intraoperative autologous blood transfusion). Hemoglobin level from ABGs and thromboelastograph are utilized to guide transfusion of blood products.
Goal Directed Fluid Therapy
For complex cases, maintenance-balanced crystalloids are administered at a rate of 2-3 ml/kg/hr. Bolus amounts of crystalloids are utilized up to 2L. The use of colloids is encouraged, thereafter, to avoid soft tissue edema. Throughout the procedure, fluid administration is aimed to maintain hemodynamic stability, promoting adequate perfusion pressure (blood pressure within 10% of baseline). Pulse pressure variation (PPV) is utilized to predict fluid responsiveness during mechanical ventilation. A PPV threshold of 13% indicates the need to optimize the Frank Starling curve. This optimization of stroke volume is achieved by the administration of additional volume. If PPV is less than 13%, fluid resuscitation is avoided, and vasopressors are utilized to augment blood pressure. Maintaining hemodynamic stability offers an additional benchmark to decrease postoperative blood transfusions and ventilator-dependency. The decision to place a central venous catheter is determined by the staff anesthesiologist and was not a mandate in the ERAS protocol.
Results
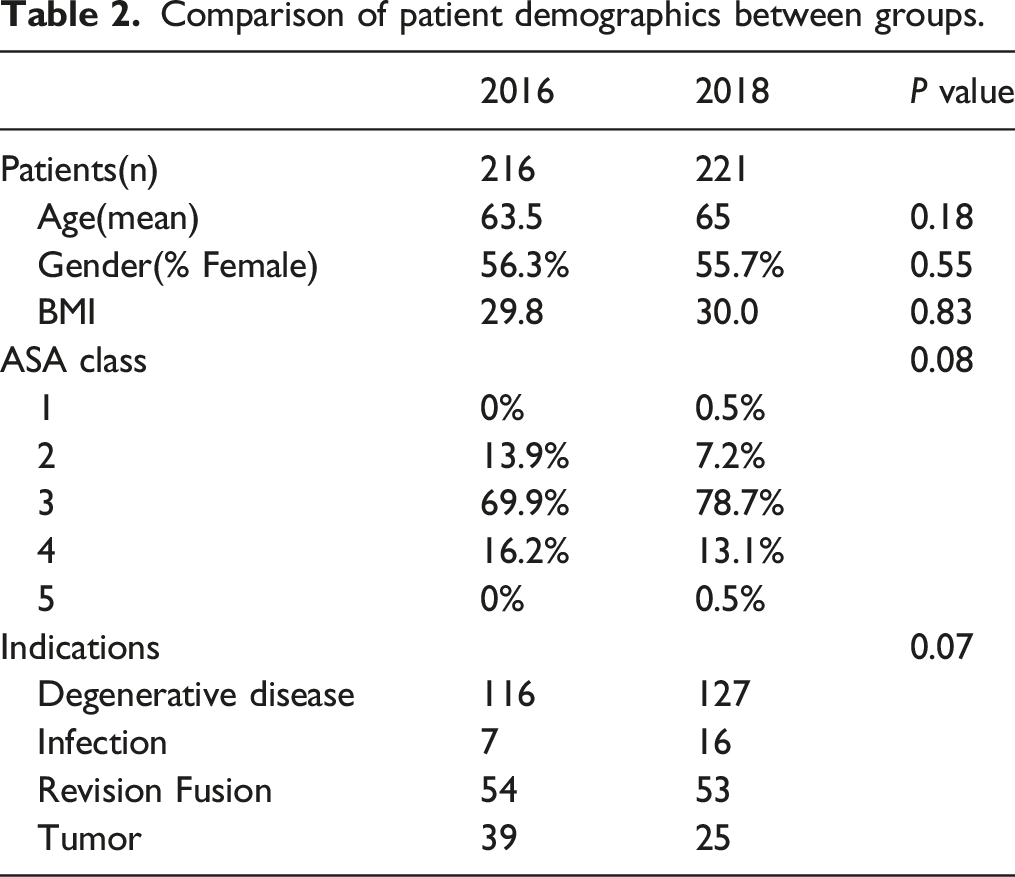
Comparison of patient demographics between groups.
Following implementation of ERAS protocol, elective complex spine surgeries demonstrated an 11.7% reduction in perioperative blood transfusions (34.1% vs 45.8%, P = .017) and on average 680 mL reduction in crystalloids infused (3278 mL vs 3958 mL, P < .001). Intraoperative blood loss decreased on average 342 mL per case (909 mL vs 1251mL, P = .001). TXA use increased significantly by 25% from 14.8 to 39.8% (P < .001). Additionally, ICU admissions declined by 8.5% following surgery (28.1% vs 36.6%, P = .071). Following ERAS, the number of patients extubated within the OR increased by 13.3% (84.4% vs 71.1%, P = .005). Of note, there was a statistically significant increase in median length of stay from 6 days to 7 days (P = .003) during this period.
Discussion
Standardized ERAS protocols have been shown to improve outcomes following surgery across a multitude of specialties. Benefits of ERAS protocols stem from incorporation of evidence-based practices spanning multiple aspects of perioperative care. Additionally, implementation of standardized protocols often acts as catalysts for improvement simply due to increased provider awareness and enhanced interdisciplinary collaboration. The implemented protocol was created via a collaboration between the Center for Spine Health and the Neuroanesthesia Department to integrate all aspects of perioperative care under one unified protocol.
Based on review of current ERAS protocols for spine surgery, this protocol uniquely emphasizes the role of comprehensive blood and goal directed fluid management. We believe this represents a unique pillar of perioperative care that is an essential aspect of the comprehensive care pathway. Existing ERAS protocols for spine surgery focus heavily on pain control, ambulation, nutrition, patient education, and surgical technique.13-17,26,27 Other institutions have adopted goal directed fluid management and/or the use of TXA within their protocol, but emphasizing the role intraoperative management has on postoperative care is imperative.13,14,17,26 These protocols proved clinically impactful with significant improvements in rates of complications, readmissions, cost, and length of stay among other factors. However, we believe that with greater focus on these key intraoperative metrics, further clinical impact can be derived.
TXA
Reducing intraoperative blood loss is key in avoiding the need for perioperative blood transfusions. One method for mitigating this risk is with intraoperative infusion of tranexamic acid. It has been studied extensively in orthopedic, cardiac, and complex spine surgery demonstrating reduced intraoperative blood loss and blood transfusion rates without increasing the incidence of venous thrombosis22,28-30. The use of TXA was included in the protocol to improve surgical hemostasis and avoid the need for blood transfusion. Following ERAS implementation, the average amount of intraoperative blood loss declined significantly by an average of 342 mL per case. Dagal et al similarly utilized intraoperative TXA in spine surgery demonstrating decreased intraoperative blood loss 17 .
Restrictive Transfusion
Perioperative blood transfusion is associated with a myriad of risks including postoperative infections and thromboembolic events which subsequently increase hospital costs and LOS
4
. To mitigate the aforementioned risks associated with transfusion, a restrictive transfusion policy with a transfusion threshold of hemoglobin
Goal Directed Fluid Therapy
Prior to implementation of a goal directed fluid protocol, there was significant variation of postoperative fluid states with some patients requiring additional resuscitation while others kept intubated due to postoperative oropharyngeal edema. Therefore, by monitoring central volume and blood pressure, administration of colloids was encouraged early in the procedure following the first 2 L of crystalloids administration. Colloids result in less loading of the interstitial space which in turn, minimizes soft tissue edema 21 . Although there is no clear consensus, the literature does suggest that colloid administration can lead to decreased postoperative complications when compared to crystalloids alone 31 . Similarly the utilization of hemodynamic parameters, such as stroke volume, mean arterial pressure, and cardiac index, to guide crystalloid and colloid infusion results in decreased incidence of pulmonary edema, acute kidney injury, respiratory distress, and postoperative infections as well as decreased ICU stays 32 . A proposed mechanism for this benefit postulates that improved perfusion minimizes the inflammatory response to surgical trauma. Maintaining euvolemia avoids tissue ischemia that results from dehydration or damage to the endothelial glycocalyx and interstitial edema as occurs in fluid overload states 32 . In the orthopedic literature a study by Peng et al showed targeted boluses of colloid prevents excess fluid administration thus reducing ischemia from tissue edema. This resulted in decreased GI intramural acidosis indicating improved perfusion and more expedient return of bowel function compared to conventional intraoperative fluid management 21 .
Ultimately, in our study implementing standardized guidelines for perioperative care resulted in decreased postoperative ventilator-dependent state. Increased extubation rate may reflect intraoperative optimization of hydration status with a subsequent reduction in postoperative fluid overload states. This result is especially clinically relevant in complex cases, lasting greater than 4 hours, where the risk of fluid migration and imbalance is most pronounced.
Trending towards significance, the postoperative ICU admission rate decreased, highlighting the impact of a multimodal approach to perioperative care. This trend has been observed at other institutions utilizing ERAS pathways for spine surgery which increases the likelihood that ERAS protocols are responsible for decreased ICU admissions16,17. Both blood transfusions and fluid imbalance states contribute to poor outcomes following high risk procedures. By mitigating these risk factors and minimizing the utilization of blood transfusions, the aim to decrease ICU admissions
Limitations
Due to the nature of analyzing bundled interventions, it is challenging to identify individual components of the protocol with the most profound impact or prove causation. There may be confounding factors responsible for the post-ERAS changes described above. It is possible that the improvement is due to the surgeons having 2 years of additional experience in 2018 as opposed to 2016. As seen in Figure 4 when analyzing all spine surgeries at our institution it seems the trend began prior to full implementation of ERAS, suggesting other factors may be contributing to our findings. However, this data is derived from all patients undergoing spine surgery and not limited to complex cases only as in our analysis. The changes observed could also stem from increased awareness of evidence-based practices presented to providers surrounding implementation of ERAS. ERAS compliance is another consideration when viewing trends following implementation. As with any new intervention there will be early and late adopters which makes analyzing temporal relationships challenging. Analysis of all spine surgeries performed at our institution from 2016 to 2018; from left to right: percentage of cases requiring blood transfusion, percentage of cases utilizing cell saver, percentage of patients remaining intubated after surgery, percentage of patients requiring vasopressors upon conclusion of surgery, percentage of cases which were admitted to the intensive care unit (ICU) postoperatively.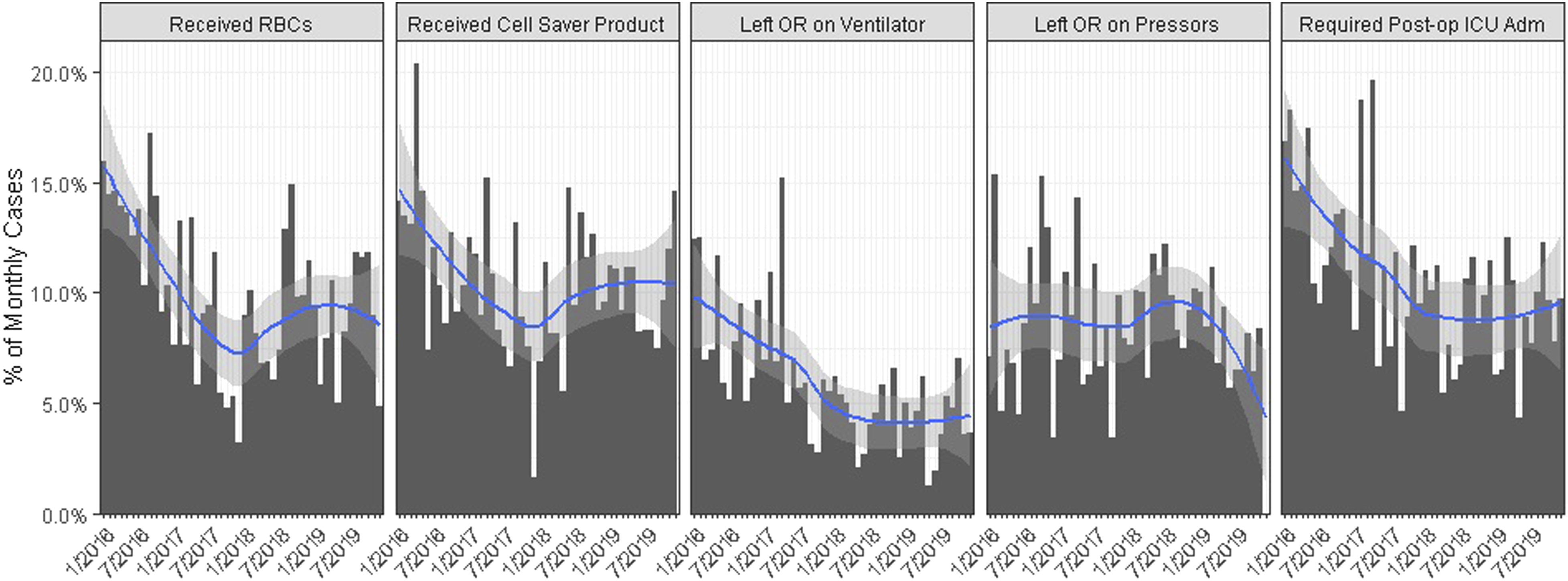
Interestingly, after implementation of ERAS there was a statistically significant increase in overall hospital LOS from 6 days to 7 days. It is difficult to speculate if this was related to ERAS as there are many factors influencing length of stay following complex spine surgeries. However, in 2018 there was a greater proportion of patients discharged home compared to skilled nursing facilities. Patients destined for home discharge often require additional optimization to ensure preparedness for independent care. Greater multi-disciplinary care occurs postoperatively, extending a patient's stay for reasons not directly related to their primary procedure. Although aiming to mitigate the effect of prior authorization and insurance length of stay requirements, this still may have contributed to the increased length of stay.
Conclusion
Enhanced recovery after surgery represents a paradigm shift in perioperative management through integration of evidence-based practices into a standardized algorithm for patient care. This study analyzed the effects of incorporating a novel, comprehensive intraoperative blood and fluid management protocol on postoperative outcomes for complex spine surgeries. These results indicate that a standardized interdisciplinary approach is associated with reduced rates of blood transfusion and optimized fluid states which may lead to reduced ICU admissions and accelerated recovery for all patients undergoing complex spine surgery.
Footnotes
Author’s Note
Support was provided solely from institutional and/or departmental sources
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.